



Since the nineteen seventies, high- and low-income countries have undergone a pattern of transnational economic and cultural integration known as globalization. The weight of the available evidence suggests that the effects of globalization on labor markets have increased economic inequality and various forms of economic insecurity that negatively affect workers’ health. Research on the relation between labor markets and health is hampered by the social invisibility of many of these health inequalities. Empirical evidence of the impact of employment relations on health inequalities is scarce for low-income countries, small firms, rural settings, and sectors of the economy in which "informality" is widespread. Information is also scarce on the effectiveness of labor market interventions in reducing health inequalities. This pattern is likely to continue in the future unless governments adopt active labor market policies. Such policies include creating jobs through state intervention, regulating the labor market to protect employment, supporting unions, and ensuring occupational safety and health standards.
A partir de los años 1970, los países de altos y bajos ingresos entraron en una fase de integración económica y cultural conocida como «globalización». La evidencia disponible muestra que los efectos de la globalización en los mercados de trabajo acarrea incrementos en desigualdades y varias formas de inseguridad económica que afectan negativamente a la salud de los trabajadores. La investigación sobre la relación entre los mercados laborales y salud se ve perjudicada por la invisibilidad social de estas desigualdades en salud. La evidencia empírica sobre las relaciones de empleo y su impacto en las desigualdades de salud es escasa en los países con ingresos bajos, las pequeñas empresas, los entornos rurales y los sectores de la economía donde la «informalidad» es generalizada. La información disponible es también escasa sobre la efectividad de las intervenciones en el mercado laboral para reducir las desigualdades en salud. Esta situación no parece que vaya a mejorar en un futuro cercano, a menos que los gobiernos adopten políticas de mercado laboral activas, incluyendo la creación de empleo, la regulación de los mercados laborales para proteger el empleo, la ayuda a los sindicatos, y aseguren el cumplimiento de las leyes de seguridad y salud laborales.
Over the past few decades, countries rich and poor alike have undergone «[a] pattern of transnational economic integration animated by the ideal of creating self-regulating global markets for goods, services, capital, technology, and skills»1, which we refer to as globalization. Globalization has resulted in gains for some; however, the weight of available evidence suggests that its effects on labour markets have led to increases in economic inequality and various forms of economic insecurity2, and is likely to continue to do so without decisive policy interventions.
Globalization was one of several macro-scale social processes considered by the World Health Organization’s Commission on Social Determinants of Health.3 In language highly unusual for a United Nations document, the Commission’s final report began with the observation that «social injustice is killing people on a grand scale.»3(p26) Evidence on this point was assembled by the Employment and Working Conditions Knowledge Network (EMCONET)4 one of several such networks that supported the work of the Commission. EMCONET developed a conceptual framework for understanding the mechanisms leading from globalization and related macro-scale social processes to health inequalities by way of employment conditions. In this article, we first provide an overview of this framework, which organizes the remainder of the text. We then summarize findings from a research program on the connection between labour market relations and welfare state regimes, and provide an historical perspective on those connections. The section that follows, still based on the framework, identifies generic policy entry points for efforts to reduce health inequalities by way of labour markets. The concluding section describes the ‘upstream’ political directions that will be needed if these policy entry points are to be utilized effectively.
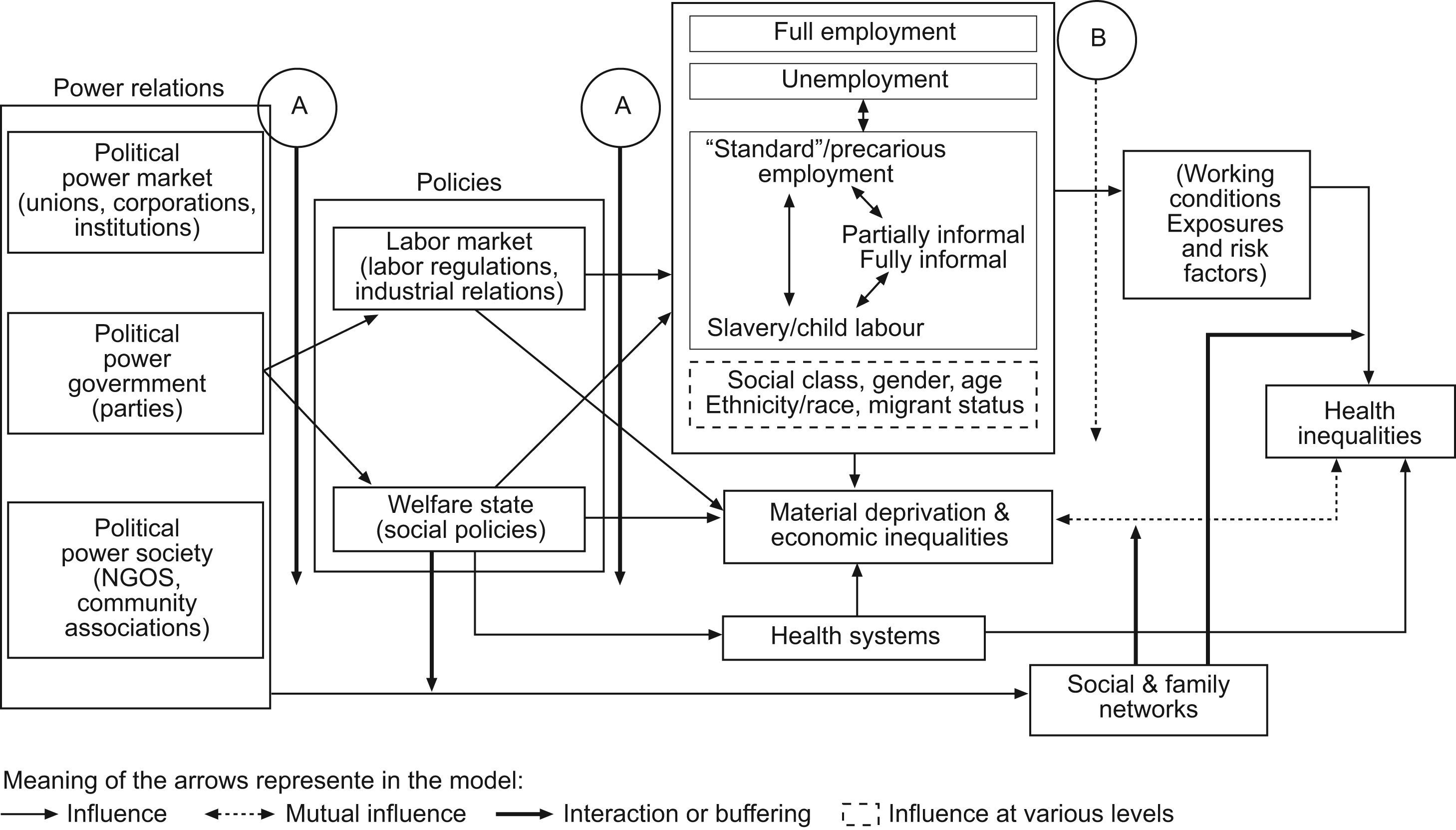
Employment relations frameworksFigures 1 and 2 provide flow charts that show the operation of the relevant causal pathways on two scales. The flow charts show both the origins and consequences of different employment relations and the connections among employment relations (the terms and conditions, including legal frameworks and extralegal forms of coercion that define the relations between employers and workers), economic and political factors, working conditions (including exposure to physical, chemical and biological hazards as well as psychosocial stress), and health inequalities.


The «Macro Conceptual Framework» (fig. 1) situates employment relations in their larger institutional context, determined by social institutions and relations that ultimately respond to a global division of production and the situation of each country in the world-system.5 The world-system, in turn, influences and interacts with the main ecological, historical, and institutional characteristics of each society. This framework explains the effects of the distribution of political power (which we refer to as power relations) on health inequalities through intermediary forces. In the macro-structural framework, political power holders affect health inequalities in numerous ways. Their influence over the labour market is broad ranging, extending across labour standards and regulations, collective bargaining, and the power (or lack of power) of trade unions. Political power holders also have an impact on the life experience of different social groups through their influence on access to healthcare, social well-being, and exposure to hazards leading to disease.6 The next part of the framework concerns the balance between welfare state policy and labour market relations. The more protection people receive from welfare state policy, the higher the level of «decommodification»: the extent to which workers are able to maintain their livelihood when they find themselves outside of the labour market, or in other words, out of a job for one reason or another.7
For the past few decades, wealthy countries have experienced dynamic changes in labour markets: reduced social safety nets for the unemployed and disadvantaged; job losses in the public sector; growth in job insecurity and precarious employment; a weakening of regulatory protections; and the historical re-emergence of an informal economy, including home-based work and some forms of child labour. In poor countries, reliance on neo-liberal economic policy has resulted in a new model of economic development oriented toward export production for global markets. Globalization’s influence is evident in many ways, notably the need to maintain economic policies (including labour market policies) that will attract and retain direct investment and contract production. By the end of the 1970s, a well-established pattern emerged in which low-regulation export processing zones (EPZs) were used to provide an incentive to relocate labour-intensive production from industrialized countries.8 More recently, the World Bank noted that today’s «open production environment mercilessly weeds out those centers with below-par macroeconomic environments, services, and labor-market flexibility.»9
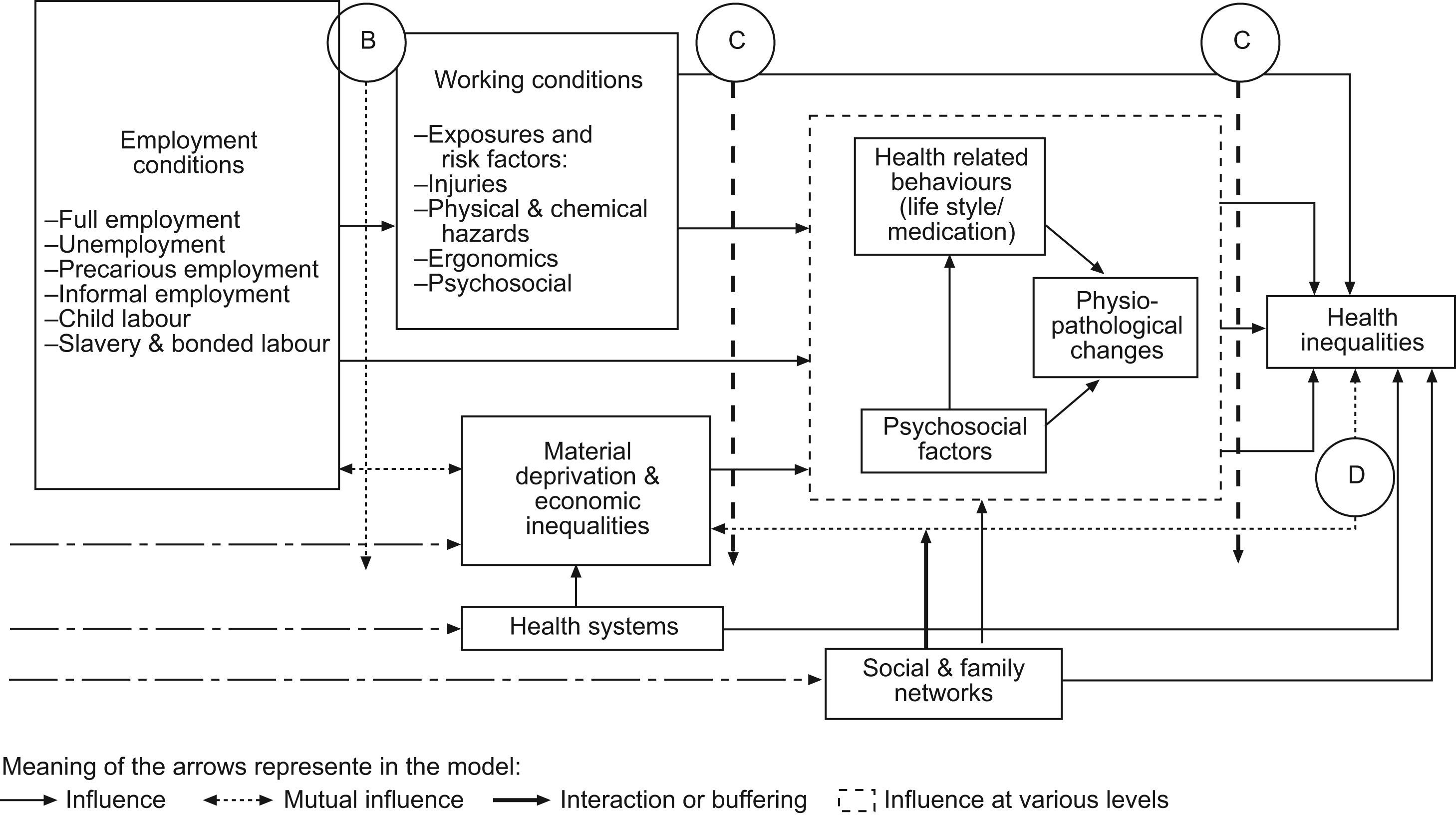
The «Micro Conceptual Framework» (fig. 2) identifies the links between employment conditions and health inequalities with reference to three different pathways: behavioural, psychosocial, and physio-pathological. Potential exposures and risk factors are classified into four main categories which are physical, chemical, ergonomic, and psychosocial. Each risk factor may lead to different health outcomes by a number of different means. The specific mechanisms of stratification according to (for example) class, gender, and ethnicity/race explain how workers are exposed to risk in different ways through different levels of exploitation, domination, and discrimination.10–12 The axes generating work-related health inequalities can influence disease even though the profile of risk factors may vary dramatically.13 Exposure to material deprivation and economic inequalities, which are closely related to employment conditions (e.g., nutrition, poverty, housing, income, etc.), have important effects not only on acute conditions but also on chronic diseases and mental health14,15. In the real world most of these processes are intertwined and ideally should be integrated into a comprehensive framework for purposes of research and policy.
Similarly, the Macro and Micro Conceptual Frameworks must be viewed together, as depicting the operation of a particular set of social processes at different scales. For example, it has been conclusively demonstrated that insecure or precarious work is associated with increased probability of work-related illness and injury.16,17 The increase in such insecure employment must, in turn, be viewed in the context created by globalization and the associated shift of power from labour to capital.2,18
Employment relations and welfare statesA new research program has emerged at the intersection of health policy and social epidemiology that focuses on two political determinants of health.11,19–21 The first focus involves the labour market relations that give rise to social class. The second focus involves the welfare state policies that follow from social class conflict. In this model, employment relations are at the core of a country’s welfare regime.22,23 Notably, employment relations are a centrepiece of West European welfare states.7 They are the result of a social pact that cements the power relationship among organized labour (trade unions and collective bargaining), government, and business associations. Social democratic parties have historically played a prominent role in negotiating the social pact. The power of labour, usually measured by union density or collective bargaining coverage, varies consistently according to the type of welfare state regime24, providing an effective means of classifying the type of employment relations as well as suggesting a causal pathway that connects the power of labour with the characteristics of welfare state regimes.
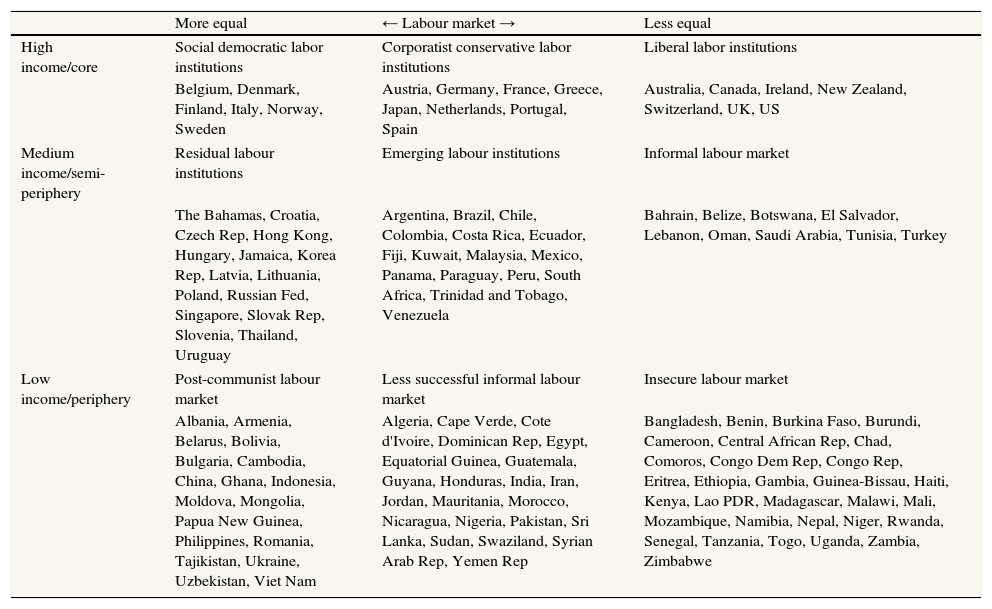
In other words, workers’ bargaining power, and its associated ability to push for a stronger welfare state and healthier working conditions, is key to understanding the impact of employment relations on workers’ health. To advance this idea, we constructed a typology of national labour markets and welfare state regimes using data from the World Bank25,26, the International Labour Office (ILO)27, and the World Health Organization (WHO)28. Specifically, we conducted a series of cluster analyses in an effort to understand the relation between labour market conditions and health in 88 peripheral and 49 semi-peripheral countries. For high income countries we used variations of Esping-Andersen’s typology of welfare state regimes as applied to the health field21. To highlight the interdependence of countries in the global context, we substituted the terminology of world-systems theory (core, semi-periphery, and periphery) for that of high, medium and low income (table 1). Countries marked in bold on table 1 are analysed in more detail in a forthcoming book.29
Typology of countries classified by national economic level and labour market indicators
| More equal | ← Labour market → | Less equal | |
| High income/core | Social democratic labor institutions | Corporatist conservative labor institutions | Liberal labor institutions |
| Belgium, Denmark, Finland, Italy, Norway, Sweden | Austria, Germany, France, Greece, Japan, Netherlands, Portugal, Spain | Australia, Canada, Ireland, New Zealand, Switzerland, UK, US | |
| Medium income/semi-periphery | Residual labour institutions | Emerging labour institutions | Informal labour market |
| The Bahamas, Croatia, Czech Rep, Hong Kong, Hungary, Jamaica, Korea Rep, Latvia, Lithuania, Poland, Russian Fed, Singapore, Slovak Rep, Slovenia, Thailand, Uruguay | Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, Fiji, Kuwait, Malaysia, Mexico, Panama, Paraguay, Peru, South Africa, Trinidad and Tobago, Venezuela | Bahrain, Belize, Botswana, El Salvador, Lebanon, Oman, Saudi Arabia, Tunisia, Turkey | |
| Low income/periphery | Post-communist labour market | Less successful informal labour market | Insecure labour market |
| Albania, Armenia, Belarus, Bolivia, Bulgaria, Cambodia, China, Ghana, Indonesia, Moldova, Mongolia, Papua New Guinea, Philippines, Romania, Tajikistan, Ukraine, Uzbekistan, Viet Nam | Algeria, Cape Verde, Cote d'Ivoire, Dominican Rep, Egypt, Equatorial Guinea, Guatemala, Guyana, Honduras, India, Iran, Jordan, Mauritania, Morocco, Nicaragua, Nigeria, Pakistan, Sri Lanka, Sudan, Swaziland, Syrian Arab Rep, Yemen Rep | Bangladesh, Benin, Burkina Faso, Burundi, Cameroon, Central African Rep, Chad, Comoros, Congo Dem Rep, Congo Rep, Eritrea, Ethiopia, Gambia, Guinea-Bissau, Haiti, Kenya, Lao PDR, Madagascar, Malawi, Mali, Mozambique, Namibia, Nepal, Niger, Rwanda, Senegal, Tanzania, Togo, Uganda, Zambia, Zimbabwe | |
The empirical categorisation of countries reveals two very important distinctions. First, it highlights the connection between labour institutions and informal labour markets. Labour institutions are closely related to the strength of the welfare state30: they are the ways in which the state regulates the labour market (e.g., provisions for collective bargaining). Labour institutions, measured through union density and collective bargaining coverage, correlate closely with welfare state regime type in wealthy countries.20,21 Informal labour markets emerge in the absence of state regulation.31 They both serve to bring order to an otherwise chaotic marketplace yet the results are very different. A second conclusion pertains to the labour markets in semi-peripheral countries, where union density and coverage are still important - some countries have emergent or residual welfare states (e.g., Eastern Block) but their effects could not be analysed due to the small sample size.
An historical perspective on labour marketsWe propose an historical perspective on labour markets in rich, medium income, and poor countries. Although it is difficult to capture a period of rapid structural change with a single sentence, it is widely held that the apogee of certain forms of industrial production (Taylorism-Fordism), social provision (welfare states), and public economic intervention (Keynesianism) moulded the socio-economic order of the so called "Golden Age of Welfare Capitalism" in the second half of the 20th century. However, there are notable international differences between wealthy and low income countries.
The expression «mid-century compromise» has been used to describe the socio-economic order that took place in Europe from the implementation of the Marshall Plan after WWII (late 1940s-early 1950s) until the oil crises of the 1970s. Workers profited from abundant and stable jobs with acceptable wages and social benefits for a large portion of the labour force, including low-skilled workers.32 The oil crises from 1972–1974 and 1978–1979 sparked a period of economic adjustment that realigned dominant economical-political interests. With an increase in unemployment and a slowdown in productivity during the 1980s, a strong neo-liberal ideological offensive challenged previous wisdom. Acceptance by elites and middle classes of the overriding need for flexible labour markets as a key to creating employment in competitive contexts legitimated the use of part-time jobs, temporary work, and self-employment. In addition, part-time workers were considered a better means of tying paid time to work time, shorter shifts being seen as the solution to unproductive time on the job.33,34 Furthermore, self-employment became a pragmatic option for the unemployed when changes in the labour market prompted mass unemployment.35 Soon enough, serious doubts were raised about the positive effects of this kind of job creation on both income levels and well-being.
While most Western economies achieved economic prosperity, the rest of the world, trying to catch up on economic development, was confronted with two antagonistic development paradigms: modernisation and dependency. To provide a stylized description, modernisation theory prescribes emulating the path of developed countries (e.g., first focus on economic growth). According to the dependency model, the periphery of this world system36 is exploited and kept in a state of backwardness by a core of dominant countries that profit from poor countries’ lack of sufficient skilled labour and industries to process raw materials locally. The oil crisis in 1972–74 greatly affected the poorest oil-importing countries which were heavily dependent on oil imports and external aid. Total long-term debt service increased on average by 29.4 per cent.37 In recent decades, some trends might suggest that developing and poor economies have been catching up in terms of economic growth (mostly due to China and India, the world’s most populous nations). For example, East Asia has seen its share of exports grow significantly (representing 4 per cent of total exports in 1990 and 11 per cent in 2004). However, other world regions have hardly increased their export participation, and poverty and unemployment remain widespread. The situation in sub-Saharan Africa and South Asia is particularly alarming, with 89 per cent of the employed population earning less than US $2 per day. Agricultural areas have a high prevalence of informal economic activity: 50 per cent of GDP and about 47 per cent of the workforce. The notion of an informal economy connotes a uniform, para-legal «underground» economy with appalling working conditions and no social security. Child labour is a serious matter of further concern (e.g., Togo, Niger, Guinea-Bissau, Cameron, Central African Republic, and Chad), given that in some sub-Saharan countries more than 50 per cent of children (5 to 14 years old) are workers. In addition, there are obvious limits to the ability to implement labour standards such as collective bargaining coverage rates38 in economies where «informalization» is widespread.
Employment-related policies on health inequalitiesThe theoretical frameworks already described (figs. 1 and 2) suggest effective entry points for future policies to reduce health inequalities by way of employment conditions. For each of the four main points identified, there is the need to identify the most effective level (international, national/regional, and local), type of employment dimension, and actor involved.
A. Refers to any change in power relations, especially related to labour market conditions and social policies, among the main political and economic actors in society.
International regulatory agencies should influence governments to put more emphasis on full-time permanent employment (for example, see 39,40) and the adoption of fair employment policies. For example, the United Nations, ILO, and other international agencies should actively seek to influence the adoption of fair employment practices among member countries. This agenda should include legislation, effective enforcement of beneficiaries of slavery and bonded labour as well as the development of international campaigns to raise awareness about sex traffic victims. Furthermore, the role and participation of unions, social movements, and grassroots community groups is crucial. Unions can generalize collectively negotiated protections (nationally and internationally) and, as evidence from poor countries attests, community actions can act as an important impetus to government measures that provide incentives for unionisation and collective bargaining and that support the collective organization of informal workers.
B. Refers to modifications of employment conditions that reduce exposures and vulnerability to health-damaging factors.
Public capacity for regulation and control of employment conditions should be strengthened. Full employment policies should be promoted to reduce the health inequalities associated with unemployment, precarious employment, and informal work. Employment creation often represents an afterthought in economic development policy; it should instead be a central objective, as it frequently was before the ascendancy of neo-liberalism. Government-led national industrial policies devoted to full employment, enforcement of fair employment standards, and universal education are necessary to eliminate child labour. In addition to the enforcement of prohibitions on slavery and human trafficking, supporting land reform in poor countries can also reduce slavery which is more common in rural areas with conflicts over land.
C. Relates to actions to modify working conditions such as health-related workplace material hazards, behaviour changes, and psychosocial factors.
Governments and firms must provide workers with the tools to participate in the analysis, evaluation, and modification of health-damaging work exposures. Unions play a fundamental role in reducing employment and work-related health inequalities through collectively negotiated international or national protections. Social movements and grassroots community activities can act as an impetus to government measures (e.g., living wage campaigns in US cities).
D. Relates to different types of interventions that may reduce the unequal consequences of ill-health and psycho-pathological change.
Governments and firms must provide workers with the tools to reduce the impact of ill-health. These interventions comprise universal access to health care, established information centres or networks for workers, adequate compensation systems regardless of their employment conditions (access, quality, compensation, and rehabilitation), and medical and legal support services for injured workers. Devising appropriate policies and implementation strategies in economies characterized by a high proportion of informal employment obviously presents special challenges.
In addition, primary health care, currently a major focus of the World Health Organization3, has the capacity and a responsibility to reach these sectors with preventive and curative interventions and with support for reinsertion into work. It is now widely recognized that universal health care coverage is a precondition for making use of that capacity, as for health equity more generally.
Political directionsWhile interventions on employment conditions need to be conducted at the organisational and job level, ‘upstream’ action on employment and working conditions (especially through labour market regulations, social policies and workplace standards) is expected to be more effective in reducing health inequalities and should be the key priority focus for action. Continuing to treat the health consequences of employment conditions as an afterthought or ‘downstream’ consideration in trade, business practices, or public health interventions will perpetuate existing health inequalities caused by unfair employment and lack of decent working conditions. General strategies combining policies at different entry points (power relations, employment, working conditions, and ill-health workers) need to be specified and contextualised for each territory (international, country/region, urban/rural local areas), condition, and population.
To achieve better employment and working conditions, economic, social, and health policies and interventions require the implementation of inter-sectoral actions and programs in which policymakers, government, workers, and community organisations, need to be actively engaged. Efforts to reduce social inequalities in health should be understood, in general, as a part of global and local integrated economic and social policies and, in particular, of specific public health and occupational programmes and interventions. Examples of interventions include universal access to public education, legislation on living wage, income redistribution through progressive tax system and social services, the avoidance of wage gender, racial and ethnic gaps, and other forms of discrimination, and the protection of the right to organize and bargain collectively.
The health sector should assume an important role in the achievement of health equity for workers and their families. It can do so by insisting that discussions about economic development models, labour market policies, or regulations on employment and working conditions take into account evidence of their impact on the health of workers and their families. The health sector can also reinforce efforts to expand the participation of workers and unions, as well as collaborating with social movements representing disadvantaged populations such as the working class, women, racialized populations, and migrants.
Research on the relations between labour markets and health is made more difficult by the social invisibility of many of the health inequalities in question. Empirical evidence concerning the impact of employment relations on health inequalities is particularly scarce for poor countries, small size firms, rural settings, and sectors of the economy in which informalization is widespread. Information is also relatively scarce on the effectiveness of labour market interventions in the reducing of health inequalities. Therefore, it is crucial to search for ‘best practices’ at each of the points of intervention identified in this paper, across a range of countries and economic sectors. In order to improve the evidence base, government agencies, international organizations, and civil society must all expand their capacity for policy and program evaluation. To achieve this, it is necessary to establish adequate information and surveillance systems. These systems must gather health data associated with employment conditions, focusing on production chains rather than individual workplaces or narrow categories of economic activity in order to reveal the role of transnational corporations as well as the adequacy or inadequacy of public health and social protection coverage. For adequate analyses of equity impacts, studies of employment and health should be stratified by class (notably but not exclusively with regard to the nature of the employment relationship), gender, age, race/ethnicity, and migration status because of the special vulnerability of undocumented workers (for example, see 41,42). Training and education on the links between employment relations and health inequalities are urgently needed, not only for public health professionals who often receive minimal training in this area but also for workers. Finally, a strong need exists for communication and dissemination campaigns for the lay population identifying employment and working conditions as key social determinants of health inequalities.
Key points- •
Understanding the mechanisms leading from globalization to health inequalities requires integrating employment relations and welfare state regimes into conceptual frameworks.
- •
Employment relations can be viewed at both macro and micro levels, respectively, through macro-social, socio-psychological, behavioural and physio-pathological pathways.
- •
The causal pathway between workers’ bargaining power and welfare state policies can also be used to explore the health effects of labour market conditions.
- •
‘Upstream’ political interventions on labour market regulation, social policies, and workplace standards are effective directions to reduce health inequalities.
There are no conflicts of interest.
The authors thank the members of the Employment Conditions Network of the WHO CSDOH for their contributions to some of the ideas presented in this paper.











