



Obesity is currently a global public health problem. Obesity in early life increases the risk of long-term energy imbalance and adult obesity and its comorbidities, type 2 diabetes, and cardiovascular disease. Since infancy and childhood are critical periods for the adoption of food preferences and physical activity, prevention strategies must intervene in these early periods to promote healthy habits and reduce risk behaviors. Trends in the prevalence of childhood obesity and overweight in Spain have continuously increased in the last three decades. Obesity and overweight currently affect 15 and 20% of Spanish children, respectively, and these percentages are among the highest in Europe. Childhood obesity is determined by social and economic factors pertaining to sectors other than the health system, such as advertising, the built environment, education and the school environment, transportation and the food environment. Following the Health in All Policies (HiAP) approach, the authors identified a series of multisector policy changes that may help to prevent and control the current rising trend of childhood obesity in Spain. The HiAP approach acknowledges that social factors including socioeconomic status, gender differences and the work-life balance are important to develop effective policy changes in the prevention of childhood obesity. A key to success in the prevention of childhood obesity in Spain through policy changes will depend on the ability to establish a policy with the explicit and primary goal of improving health outcomes, despite the anticipated resistance from various sectors and stakeholders.
Actualmente, la obesidad es un problema de salud pública en todo el mundo. La obesidad temprana aumenta el riesgo de sufrir desequilibrio energético a largo plazo, así como de presentar obesidad en edad adulta o sus comorbilidades: diabetes tipo 2 y enfermedades cardiovasculares. Puesto que la infancia y la niñez son períodos cruciales para establecer las preferencias alimenticias y de actividad física, las estrategias de prevención deben iniciarse durante esta etapa para fomentar hábitos saludables y reducir los comportamientos de riesgo. La tendencia en la prevalencia de la obesidad y el sobrepeso infantil en España ha aumentado de forma continua en las tres últimas décadas. En la actualidad, la obesidad y el sobrepeso afectan a un 15 y a un 20% de los niños españoles, respectivamente, y estos porcentajes se encuentran entre los más elevados de Europa. La obesidad infantil viene determinada por factores sociales y económicos que son independientes del sistema sanitario, tales como la publicidad, el entorno, la educación y el ambiente escolar, el transporte y el entorno alimentario. Mediante el enfoque de la Unión Europea, Salud en Todas las Políticas, los autores identificaron una serie de cambios de política dirigidos a varios sectores y que podrían ayudar a prevenir y controlar la creciente tendencia actual de la obesidad infantil en España. Este enfoque reconoce que factores sociales como el nivel socioeconómico, las diferencias de género y el equilibrio entre la vida laboral y personal son importantes para la prevención de la obesidad infantil. El éxito de la prevención de la obesidad infantil en España dependerá en gran medida de la capacidad que tengamos para desarrollar políticas fuera del sector sanitario que tengan el objetivo explícito y primario de mejorar resultados en salud pese a la resistencia esperada de diferentes sectores económicos y partes interesadas.
Obesity has been recognized as a global public health problem1,2. Childhood obesity increases the risk of long-term energy imbalance and adult obesity and its comorbidities, type 2 diabetes, cardiovascular disease and other non communicable chronic diseases3.
The evidence from developmental psychology indicates that infancy and childhood are critical periods for the adoption of food preferences and other key behaviors associated with energy intake and physical activity. Thus, it is recognized that effective prevention strategies must intervene at these early periods, in order to promote healthy habits and reduce risk behaviors.
In the field of public health, it is important to acknowledge that childhood obesity is determined by social and economic factors situated in sectors other than the health system. Research in the field of obesity has shown that in the past three decades, population-wide changes are the main driving forces of the worldwide increase of childhood obesity. There is a consensus among obesity experts that changing the ‘‘obesogenic’’ environment is a critical step to advance in the prevention and control of obesity4. Reversing the current policies that lead to increased caloric consumption and reduced physical activity will require major changes in different sectors such as advertising, transportation, urban planning, education and the food environment1.
Key points
- •
Childhood obesity is an increasing public health problem, since around one third of our children already have excessive bodyweight. The number of overweight and obese children in Spain is among the highest observed in Europe.
- •
The current health of children relates directly to the health of our future population. Specifically cardiovascular health and primordial prevention focuses directly on the healthy habits that children might learn and carry on through their adult life.
- •
Childhood obesity is a multi-factorial disease where different social and economic sectors play a crucial role. Sectors other than the health system, closely related to childhood obesity include advertising, transportation, the built environment, education and the food environment. These sectors are amenable to be intervened through policies that take into account their possible impact on childhood obesity, such as the Health in All Policies framework.
- •
Social determinants such as socioeconomic status, work-life balance and gender differences act as risk regulators of the proposed policies in relation to childhood obesity and therefore should be taken into account in the development of preventive interventions.
- •
Policy changes, recommendations and regulations in each of the analyzed sectors, with its subsequent evaluations, may help to prevent this important public health problem. The NAOS strategy and the PERSEO program have been important steps in this direction.
The increasing number of children affected, coupled with the difficulty, cost, and low yield of therapeutic approaches available, suggests that prevention should be the primary focus of our efforts to reduce and eliminate childhood obesity. Furthermore, once obesity is established, it is a protracted and difficult-to-treat condition; therefore, it makes sense to focus prevention efforts on the younger generations5.
The Health in All Policies (HiAP) European Initiative reinforces the idea of the potential impact in health outcomes of policy actions that lay in sectors other than health6. While the health sector´s curative activities are mainly planned and implemented through health outcomes, health promotion and prevention need to be planned from the social and economic determinant points of view. This approach showed to be very useful for decreasing the burden of cardiovascular disease in Finland, and is particularly relevant for the case of obesity7. This approach acknowledges the role of regulations and laws that may influence the different policies in relation to childhood obesity. We will follow the example of HiAP framework to identify the current policies affecting childhood obesity and are therefore amenable of change for the prevention of childhood obesity in Spain.
In this article we will first briefly review the current situation of childhood obesity in Spain within the context of other European countries. Next, we will identify and analyze a series of policies directly related to the sectors mentioned above. These policies affect different environments where children spend most of their time: physical environment8, school environment9 and home/family environment10. We also paid special attention to social factors such as gender differences, work-life balance and socio-economic status, that act as risk regulators11 for the different policies in relation to childhood obesity. We will subsequently describe several policy changes aimed at preventing and controlling the current childhood obesity epidemic in Spain.
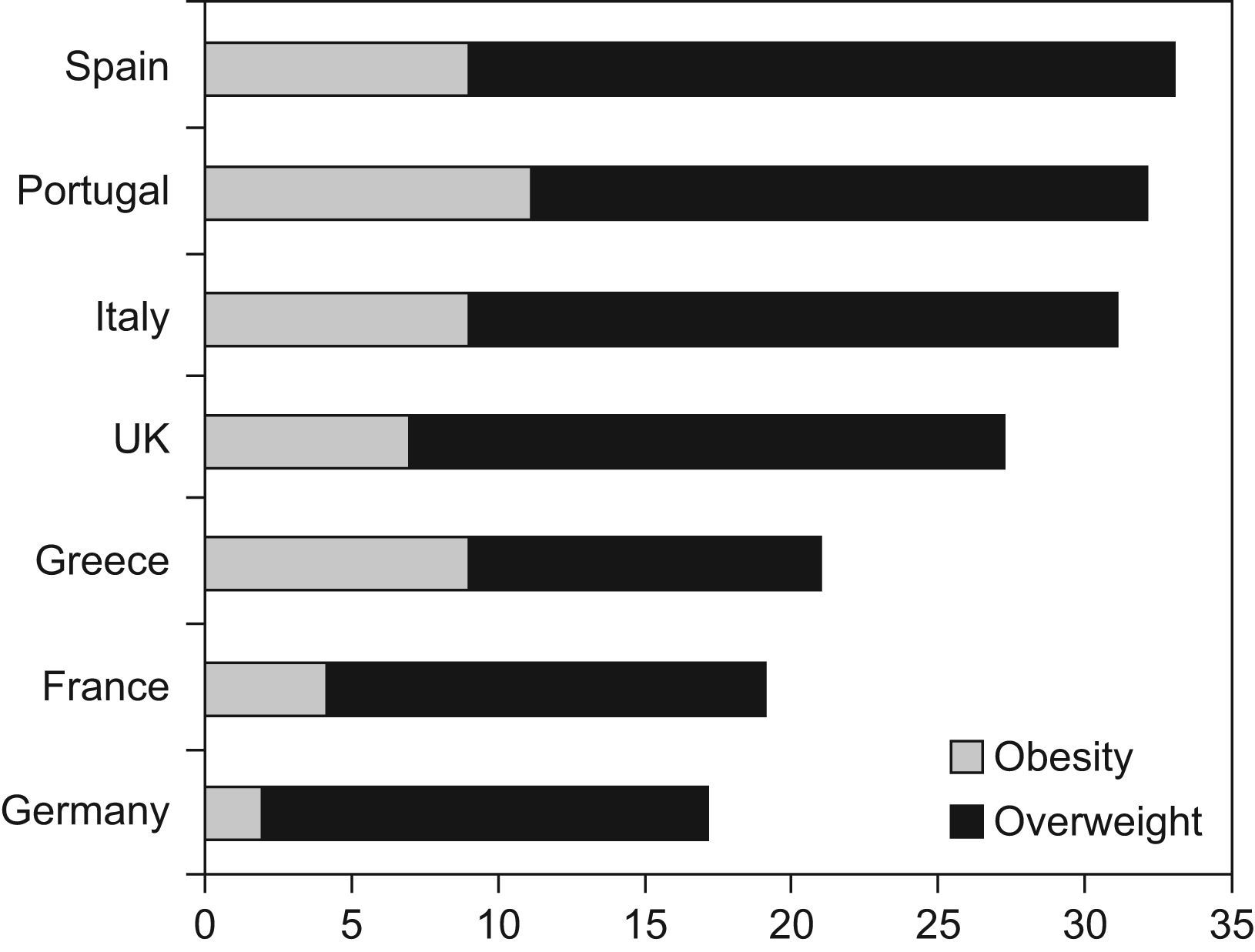
Current situation of childhood obesity in Spain and other European countriesThe prevalence of childhood obesity in Spain is among the highest of European countries, as shown by data gathered by the expert group on childhood obesity of the International Obesity Taskforce (IOTF) (fig. 1)12. The criteria used to define 'childhood obesity' and 'overweight' has been debated extensively13. To facilitate comparison across different studies, all the data presented in the review use the definitions corresponding to the IOTF criteria14.

Prevalence of obesity and overweight in schoolchildren aged 7-11 from Spain, Portugal, Italy, UK, Greece, France and Germany. Source: EU Platform on Diet, Physical Activity and Health, 200512.
It is noteworthy that the southern European countries in the Mediterranean region, along with the UK, are those showing the highest figures of childhood obesity and overweight12.
Greece presents childhood obesity statistics as high as Spain15,16. Greek studies have also shown that the principal factor underlying instance of being overweight among 10–12 years old in Athens was extended physical inactivity15. Furthermore, a study conducted in rural Greece confirmed the association between high blood pressure and increased BMI in children aged 4 to 1016.
On the other hand, not only Mediterranean countries present high levels of childhood excess weight in Europe as exemplified by the UK12. Studies conducted in Scotland17 and England18 showed a clear socioeconomic gradient with higher prevalence of being overweight and obese in low socioeconomic strata.
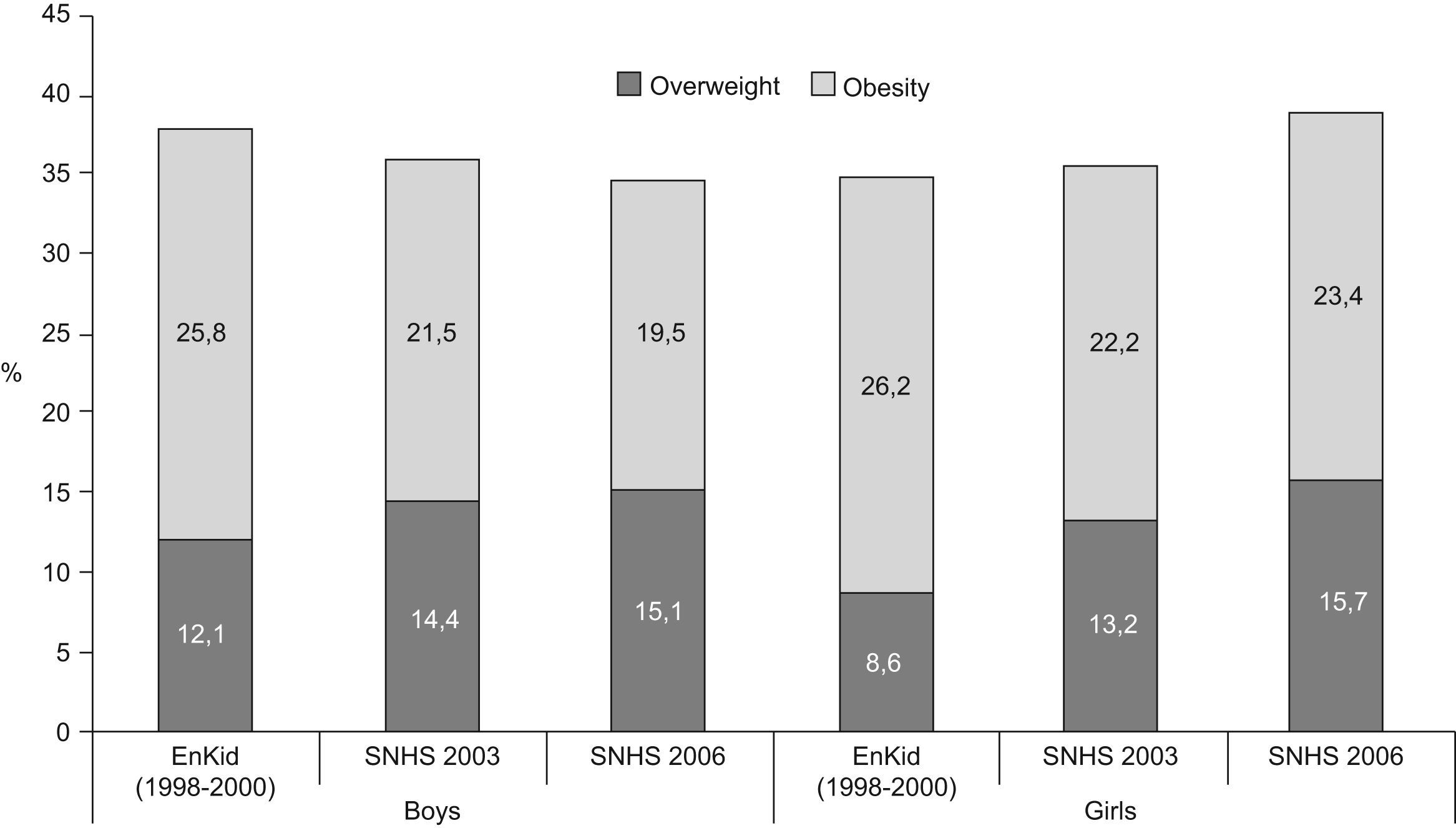
To date, the only nationally-representative survey on childhood obesity in Spain with direct measurements of height and weight is the enKid study, conducted in 1998–2000 in a random sample of 2–24 year-old children and young adults19,20. In 6–9 year-old children, the study reported prevalence of being overweight and obese of 25.8% and 12.1% in boys, and of 26.2% and 8.6% in girls, respectively (fig. 2). In the 10–13 year-old age group, obesity and overweight prevalence were reported as 6.6% and 23.8% in boys and 2.6% and 18.4% in girls, respectively. The Spanish National Health Survey (SNHS) included parental self-reported height and weight of 5–9 year-old children. Both boys and girls from 5–9 years have increased their prevalence of obesity, whereas instance of being overweight has stayed unchanged or slightly declined. The total combined prevalence of obesity and being overweight is, according to the last SNHS in 2006, 39% for girls and 35% for boys (fig. 2)21.

A number of local studies have also been carried out in Spain in the last 3 decades. Among these, the Cuenca study was able to directly measure height in 9–10 year-old children from that city in 1992, 1996, 1998 and 2004. The prevalence of obesity increased from 4.4% in 1992 to 10.1% in 2004 among boys and from 2.9% to 7.8% among girls22. Together with the data from the enKid study and the Spanish National Survey, these are highly concerning statistics.
Several determinants of childhood obesity in Spain have been reported in existing scientific literature. The enKid study found that sex, age group, place of residence, mother’s level of education and family income were significant predictors for obesity in children under 14 years19. A case-control study conducted in children from Navarra found that low levels of physical activity, an existing family history of obesity, long hours of watching television, and sugar-sweetened beverage consumption were important predictive variables for childhood obesity23.
All these factors were individual characteristics of the children and their parents. It is important to underline the lack of studies aiming to understand the possible relation of contextual characteristics and policies associated with childhood obesity in Spain. Nevertheless, important geographical differences were found in the enKid study pointing out possible group level determinants of childhood obesity20.
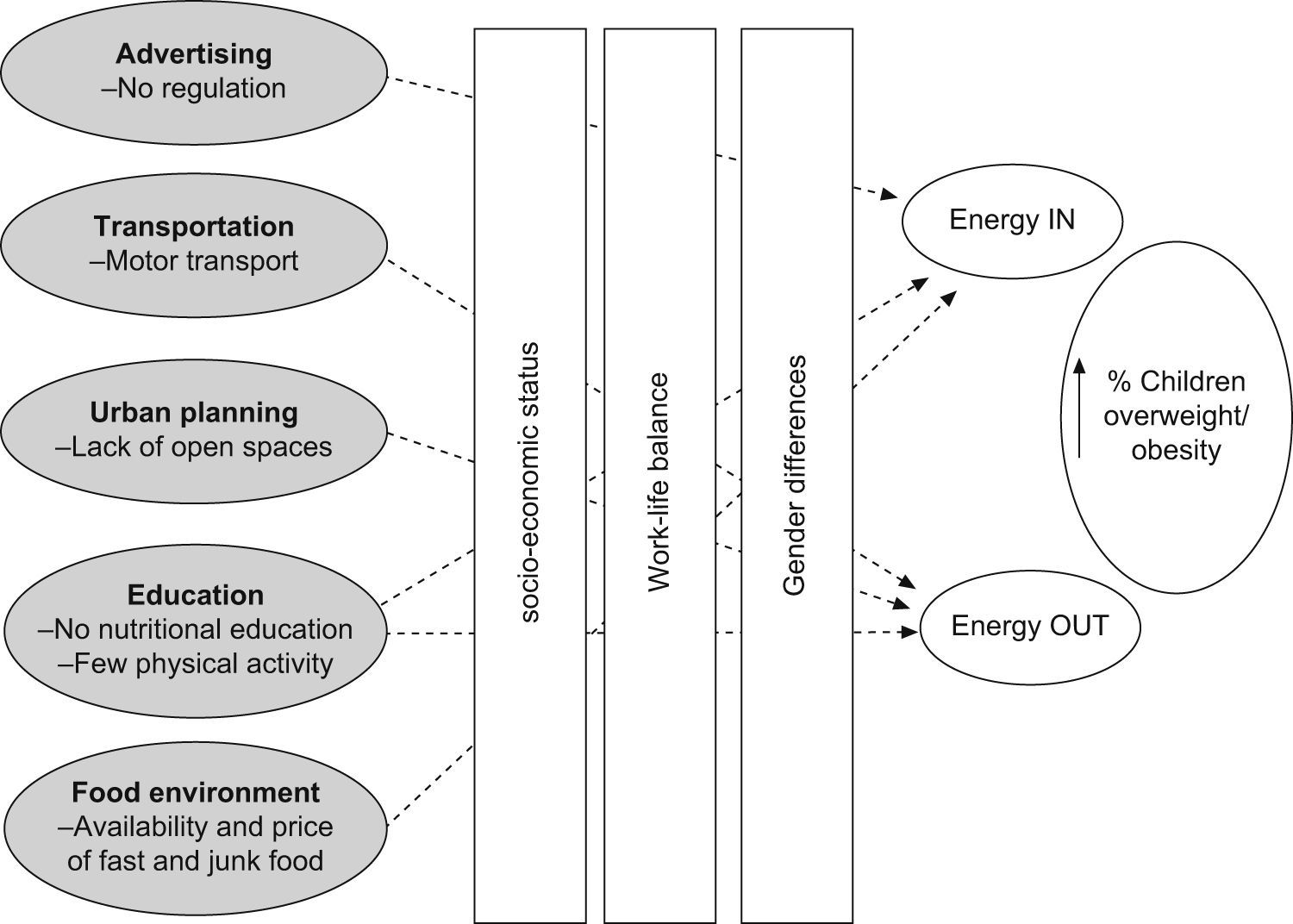
Policy determinants of childhood obesityNext, we will review the literature pointing out policies outside the health sector related with childhood obesity. After reviewing the current international literature, we identified several different sectors that relate to obesity. For their relevance for preventive actions, we decided to focus on advertising, transportation, the built environment, education and the food environment. Thus, we propose the following framework (fig. 3).

Advertising: Advertising is currently an extremely important sector of market economies. Television and tie-in ad campaigns have been shown to be very effective in modifying food preferences in children and adolescents. Unfortunately, most of these campaigns promote low-nutrient density, high-energy foods and beverages24. The fierce competition among food manufacturers results in extensive ad campaigns that use children’s educational programs, iconic characters such as movie stars, cartoons and sports celebrities to promote their products. This is a widespread phenomenon described not just in the US25 but also in Spain26. The relevance of advertising runs parallel to the fact that 90% of Spanish children watch TV every day and 20% persist for at least 2h27. TV advertising of foods of low nutritional value adds to the well-known burden of sedentarism associated with TV watching28, which has already been associated with obesity in Spanish children20,29.
Transportation: This topic has acquired relevance due to the difficulty of modern societies to expend sufficient daily calories to match energy intake. Certain forms of transportation provide a useful outlet to increase daily energy expenditure: walking, bicycling, even use of public transportation instead of personal car. The association of the type of transportation with physical activity levels has been explored in Spain30 and other countries, including China31. A secondary burden associated with sedentary transportation (personal car) is the ever expanding need for highways and parking lots, usually at the expense of open spaces, which could be used for physical activity. The car-centred culture also promotes the creation of large shopping complexes, reducing further the need for walking to fulfil daily purchasing needs.
Built environment: A large number of studies have looked at the specific features of the built environment in relation to obesity. Papas et al. conducted a systematic review and found a consistent positive association between some aspect of the built environment and obesity32. In the specific case of Spain, it is important to acknowledge that more than 90% of the population lives in residential urban areas (an urban area is defined as more than 2000 inhabitants)33. Therefore it is important to acknowledge that open spaces (parks and recreational facilities), specifically designed for children and facilitating physical activity, are far from being the norm in the Spanish urban environment.
Education and the school environment: Through the different levels and components of the childhood education process it is important to include the concepts of healthy habits in relation to diet and physical activity. These concepts go beyond the school and include parents and other stakeholders such as local and national government. Regarding the school environment and its association with childhood obesity, we find several relevant aspects:
- 1.
Lack of clear and national regulation over school menus in terms of quantitative and qualitative nutritional adequacy. This is a very complex topic. Currently in Spain there is a national effort to come to a nation-wide agreement on school lunch menus.
- 2.
The amount of physical activity that children perform in their schools as part of their curriculum and in their free time at schools has been decreasing in the last 3 decades29. Relevant to this topic, is the physical environment available within schools that include green spaces, safe parks and most importantly sport and recreational facilities, which provide opportunities for children to be physically active. It is important to distinguish between the hours and possibilities of physical education offered to all the children in a given school in comparison to sports offered only to some children enrolled in «varsity teams».
- 3.
The availability of vending machines offering low nutritional value products to children is also a topic of great discussion. In the case of Spain, vending machines are by law only available in High Schools.
Food environment: Research based in the US suggests that neighbourhood residents who have lower availability of healthy food options have a lower quality diet34. This might not be a problem in Spain but research is definitely needed in this area. The price of healthy options is an important feature of the food environment. In Spain two different studies so far have proved that healthier and recommended diets are more expensive than low quality diets35,36. This fact will most probably affect the acquisition of healthy foods for parents and schools with low budgets. The food environment in the areas surrounding schools, parks and other areas dedicated to children is important since they tend to offer low nutritional value foods. The food environment is currently changing in all countries and the consumption of foods away from home is becoming more prevalent. As societies urbanize, the fraction of daily caloric intake (>50% in the US) increases. The quality and quantity of food consumed inside or outside the home is strikingly different even within individual families. Shopping malls, which have become popular recreational places for some children in Spain, are relevant participants in the influence of food quality in children and adolescents. This raises interesting questions given the large availability of low nutritional value food in these malls.
Social factors as mediators of policies related to childhood obesitySocial factors such as socioeconomic status, work-life balance and gender differences act as risk regulators11 regarding childhood obesity. Next, we describe these factors and use some examples for clarification.
Socio-economic status (SES): Currently several studies have described a gradient in which children of low SES or living in poor neighbourhoods present higher risk of becoming overweight and obese37. In Spain, the prevalence of childhood obesity is higher among low socio-economic status (SES) families20, where the mechanisms involved in this association are several and of different kinds. Family level SES have been related to the type of food the families buy and consume38, and may also relate to the amount of free time for parents to cook and the amount of leisure time to spend with their children. Additionally, low SES families have a lower educational level, and may be less concerned about the relevance of healthy diets and physical activity17. Low SES families usually live in neighbourhoods characterized by poor access to safe open-air areas to practice physical activity and a food environment characterized by cheap, low nutritional value options39. SES also determines another relevant social factor, i.e. the work-life balance.
Work-life balance: In most of developed countries, maternal employment has increased during the last 3 decades. These changes in labor patterns have translated into lifestyle changes of the family members. Some studies suggest that the probability of a child becoming overweight is related to the number of hours worked by the mother and not necessarily by the father40–42. Reasons for this association could be that working women may have less time to acquire and prepare fresh foods; a larger portion of prepared foods may be consumed in the households of working mothers; children of working mothers may eat more low nutritional value foods, spend less time being physically active and instead spend more time watching TV43. Social policies aimed to achieve a work-life balance could help promote healthy lifestyle habits for the family members.
Gender differences: Gender is a social factor affecting several aspects relating to eating habits, physical activity and body weight. Large gender differences are observed in different countries in terms of childhood obesity, where in the case of Spain, boys present higher prevalence of obesity than girls20,22.
First, we find that there are different perceptions between what is considered excess weight for boys compared to girls. Excess weight is perceived earlier in girls, while families maybe more tolerant with excess weight in boys for longer periods of time44.
In relation to advertising, stereotypes linked to gender greatly influence the marketing campaigns of toys. Female toys are more static, supportive of a 'thinner' body form and less «physical» than toys directed at males. This fact is also directly related to gender differences in the choice of sports and therefore the level of physical activity.
Proposed policy changes in Spain towards the prevention of childhood obesityIn 2004, the World Health Assembly approved the Global Strategy on Diet, Physical Activity and Health with the aim of reducing the risk factors of non communicable chronic diseases related to unhealthy diets and physical inactivity45,46. It is noteworthy that in Spain, subsequently to the WHO initiative, the Ministry of Health began implementing the Strategy for Nutrition, Physical Activity and the Prevention of Obesity (NAOS Strategy) in 200547. The Reference Pilot School-based Program against Obesity (PERSEO) is included in the NAOS Strategy and is aimed to promote healthy habits in the children of 67 schools around the country. To reach its target, The PERSEO program promotes fruit consumption and physical activity in and outside the schools with a special interest in the family/home environment.
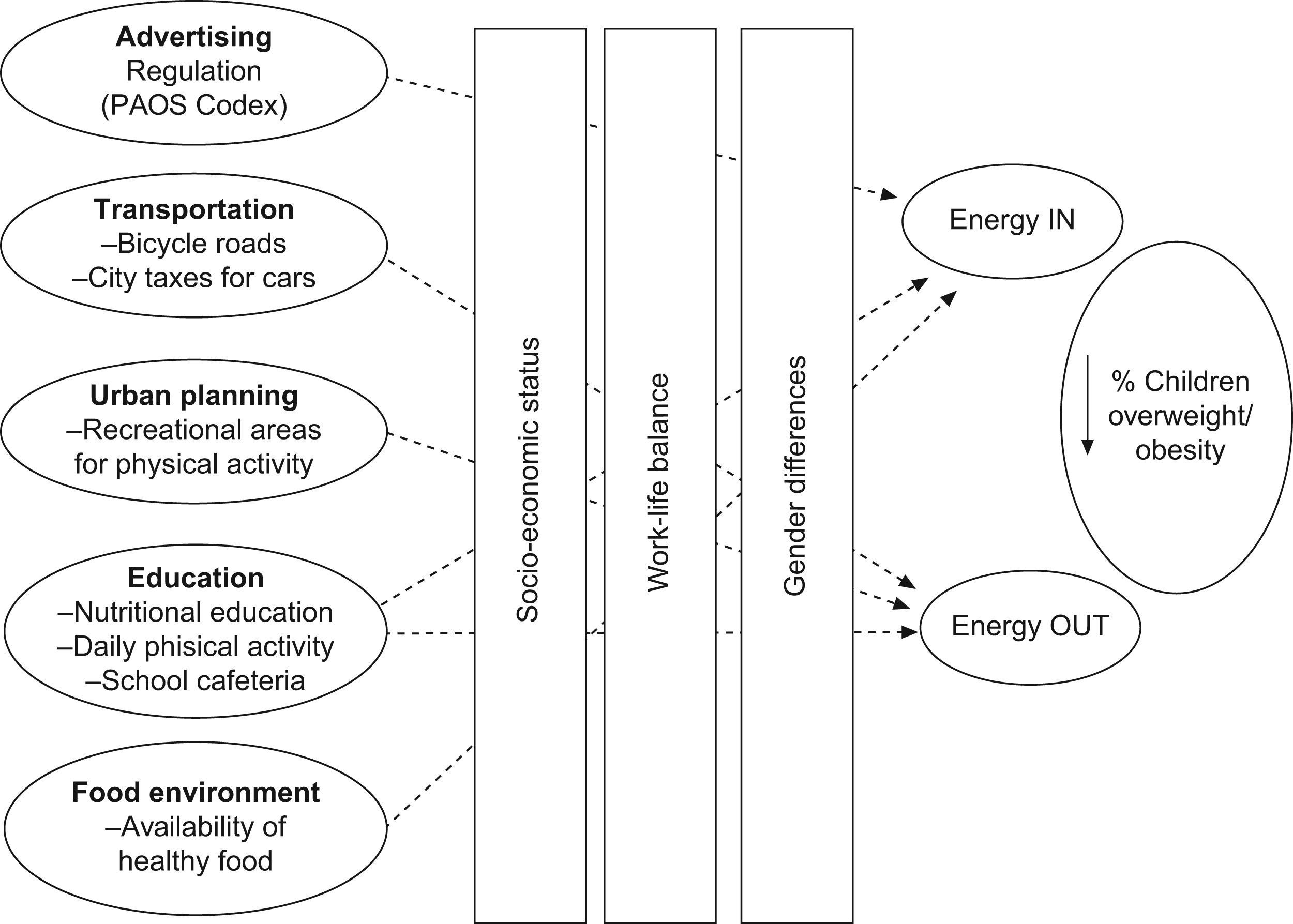
In this review, we critically analyzed the five social and economic sectors explained above and propose a number of policy changes that may help to prevent excessive energy intake and increase energy expenditure in Spanish children (fig. 4).

Advertising: For the time being, the launch of the PAOS regulatory code has not reached the expected impact in terms of quantity and quality of food advertising targeting children26. Thus, larger efforts are warranted in this area. As a possible first step, advertising regulation policies should be established, both in television and other mass media and public events (sports, cultural, etc.)48.
Transportation: Within the framework of public health practice, current means of transportation must be evaluated and modified to continuously encourage more healthy options, such as walking and bicycling49. Tools such as the PEP project (Transport Health and Environment Pan-European Programme)50, studying the effects of transportation in children, identifies the following interventions: creation of adequate infrastructure for safer bicycling, creation of connected slow-traffic areas that encourage walking, and traffic control through appropriate regulations. Several local initiatives in Spain currently aim to organize a network of schools and parents to increase the number of children that walk to school. These initiatives have not translated yet into research articles.
Built environment: A process of urban planning where health (and childhood obesity in our case) is considered, is another point in which authorities should take action and join efforts towards a healthy built environment51. This is especially important for children, since they usually depend on their parents to participate in physical activity and play sports. Recreational areas are specifically needed in order to give children the opportunity to play sports and be physically active. Although the authors did not find published evidence in Spain, the positive relationship between recreational areas and physical activity has been well established52–54.
Education and the school environment: Since children spend a significant amount of time within the school environment, policy changes to education will have a great impact on child behaviour and encourage a healthier lifestyle. Necessary changes in the educational sector are:
- 1.
Modify the school curriculum to take into account aspects relating nutrition and health55.
- 2.
Adapt the school cafeteria menus to offer a healthier and high quality diet to children. In addition, we should not only pay attention to maintaining an energetic balance, but comply with other nutritional requirements determined by the Recommended Dietary Allowance (RDA) of each nutrient and food category56–58. In regards to this, the Spanish Ministry of Health (MSPS) has just launched an important set of recommendations for school lunch menus and the school food environment. These recommendations follow two main objectives: firstly, to promote the consumption of healthy foods and beverages within school menus, which will establish an adequate consumption of a variety of healthy food groups; and secondly, to limit the availability of low nutritional value food items in schools.59
- 3.
Dedicate more teaching and free time to physical activity and psychomotricity. Doing exercise on a regular basis at school may promote a more active attitude back at home.
Food environment: Residents of communities with poor access to healthy foods present a higher risk of following poor quality diets34. Food environment, policy, multilevel strategies for improving diet and obesity control are recommended based on a rapidly growing body of research.8 Developing policies related to the food environment in order to improve the availability of healthy options in food stores at reasonable prices60 is a field of necessary research and evaluation. Currently in the US, the idea of taxing sugar-sweetened beverages is being considered61. This is also now being considered in countries including Mexico and Colombia, in an attempt to influence children not to buy this unhealthy beverage.
ConclusionsChildhood obesity is of growing concern given the associated risk of a decreasing level of health in the future adult population. Childhood obesity in Spain is among the highest in Europe. From a prevention perspective, childhood offers the greatest opportunity to learn and establish healthy habits within nutrition and physical activity. Childhood obesity is a multi-factorial disease where social and environmental factors play a crucial role. These factors are located in different sectors of our societies and are amenable to be intervened through policies that take into account their possible impact on childhood obesity. The HiAP framework offers a valid perspective towards the case of childhood obesity7. We identified several sectors (advertising, transportation, the built environment, education and the food environment) that are directly related to childhood obesity, where policy changes may help preventing and controlling the current situation in Spain. It is important to acknowledge that these policies will only be fully efficient if they take into account social determinants of childhood obesity as SES, gender differences and work-life balance.
In Spain, the Ministry of Health developed a national strategy for the prevention and control of obesity that included the PERSEO program. Both, the PERSEO and the NAOS Strategy extend far beyond the health sector, by combining actions in different sectors. Importantly, the NAOS strategy includes informative campaigns, agreements with public and private institutions, voluntary working agreements, educational programs and supporting health promotion initiatives47. The comprehensive evaluation of the NAOS and PERSEO programs strategy will offer a great opportunity in facilitating the prevention and control of childhood obesity. Since the PERSEO program is a school based initiative, the sectors including the built environment, transportation and the food environment have received less attention and regulation.
A key success will be the ability to set a policy with the explicit and primary goal of achieving advances in the prevention and control of childhood obesity despite the possible resistance from different sectors and stakeholders.











