




Studies of the prevalence of HIV in sentinel populations are one of the key strategies to monitor the HIV epidemic. We describe HIV prevalence trends and identify differences across time in the sociodemographic characteristics of HIV-infected women giving birth in Catalonia.
MethodsWe used dried blood specimens, residual to newborn screening, which have been collected in Catalonia every 2 months since 1994. The total number of samples obtained until 2009 and in 2013 represented half of yearly newborns. From 2010 to 2012, the total number of samples obtained represented a quarter of yearly newborns. We studied the prevalence by year and place of current residence (Barcelona-city, cities>200,000 inhabitants and cities ≤ 200,000 inhabitants) and by the mother's birth country. A total of 624,912 infants were tested for HIV antibodies from January 1994 to December 2013.
ResultsHIV prevalence trends among women giving birth in Catalonia decreased until 2007. Thereafter, there was a change to a steady trend until 2013. However, among foreign women giving birth and living in cities ≤ 200,000 inhabitants, the prevalence of HIV increased from 2007 to 2013.
ConclusionTo ensure early identification and treatment of HIV-infected mothers, it is essential to maintain HIV surveillance programs and pre- and post-natal screening programs, both in Barcelona and in cities with 200,000 inhabitants or less, especially in immigrant women.
Los estudios de prevalencia del VIH en poblaciones centinela son una de las estrategias clave para monitorizar la epidemia. Describimos tendencias de la prevalencia de VIH e identificamos diferencias en el tiempo y según las características socio-demográficas de las mujeres que dan a luz infectadas por el VIH en Cataluña.
MétodosUtilizamos muestras de sangre seca, residuales al cribado de recién nacidos que se recoge cada dos meses desde el año 1994. El total de muestras obtenidas hasta el 2009 y en 2013, representa la mitad de los recién nacidos anuales. En los años 2010 a 2012, el total de muestras obtenidas representa un cuarto de los recién nacidos anuales. Estudiamos la prevalencia por año y lugar de residencia (Barcelona-ciudad, ciudades de más de 200.000 habitantes y otras ciudades o pueblos de ≤ a 200.000 habitantes) y por lugar de nacimiento de la madre. Entre enero 1994 y diciembre 2013, fueron cribados de existencia de anticuerpos anti-VIH 624.912 recién nacidos.
ResultadosLa prevalencia de VIH en las mujeres que dan a luz en Cataluña decrece hasta el año 2007, estabilizándose en 2013. Sin embargo, entre las extranjeras que dieron a luz y que viven en ciudades de ≤ a 200.000 habitantes la prevalencia de VIH aumenta entre 2007 y 2013.
ConclusiónEs fundamental mantener la vigilancia del VIH y los programas pre y post natal en Barcelona ciudad y ciudades de ≤ a 200.000 habitantes, y especialmente en las mujeres extranjeras para asegurar un temprano abordaje de las infectadas por el VIH.
Studies in sentinel populations to estimate HIV prevalence are the key strategies to monitor the epidemic 1. Pregnant women are an important group to target for HIV prevention as early diagnosis and appropriate management reduces mother to child transmission. Monitoring HIV prevalence in this group has been done using different methods such as back projection from reported cases of AIDS due to perinatally acquired HIV infection 2 or unlinked anonymous surveillance 3–7 or testing programs in antenatal care or abortion clinics 8.
In Catalonia, estimations of pregnant women's HIV prevalence cannot be done from information collected in antenatal care or abortion clinics because the standard HIV surveillance questionnaire doesn’t ask about pregnancy status. Unlinked anonymous testing was introduced in the Integrated Surveillance System of HIV/AIDS/STI of the Health Department (Generalitat de Catalunya) in 1994, as a way to monitorize HIV prevalence with the minimum participation bias, in key populations. Originally, Intravenous Drug Users, Men who have Sex with Men and Female Sex Workers were chosen as high risk populations. Since the offering of an HIV test to all pregnant women was mandatory in the local protocol, and since a newborn metabolic screening program was in place with a very high coverage (99%), newborns were also included as a sentinel population to estimate HIV prevalence among pregnant women. The unlinked anonymous newborn survey has provided information on HIV prevalence by area of residence since 1994 and by country of origin since 2007 and now includes approximately 50% of live births in Catalonia. The survey includes women whose HIV infection has already been diagnosed as well as those unaware of their infection, giving a measure of overall HIV prevalence in pregnant women.
The increase of immigration occurred in Spain and Catalonia within the last 20 years with a steady trend of migrants since the year 2009. The pattern of migration of women 15 to 64 years old is similar, both in big and small cities, increasing up to 2009 and stable after then. Percentages of migrant women are the highest in Barcelona, followed by 4 cities>200,000 (Badalona, Hospitalet de Llobregat, Terrassa and Sabadell) and cities ≤ 200,000 inhabitants.
According to these data, it is meaningful to study the HIV prevalence by mother's country of birth and place of current residence. Other researchers have studied serological markers of HIV and other infections in Spain 9,10. The study of the geographic distribution of HIV prevalence in women giving birth may be an additional tool to help targeting geographic areas for intervention. Although ecological studies are not conclusive 11, taking profit of data already available helps reducing costs and better targeting for further studies. The aim of this study was to describe HIV prevalence trends in women giving birth and identify differences on their socio-demographic characteristics by place of current residence in Catalonia during a 20 years period (1994 to 2013) as well as describe the potential role of immigration more specifically for the period 2007 to 2013.
MethodsCollection of samplesThe neonatal dried blood spot survey, residual to newborn screening 12, takes left over dried blood spots taken from newborn 3 days after birth and tests them for maternal HIV infection. These blood specimens are being collected, in order to avoid seasonality, every two months. The obtained sample size represents half of the yearly newborns up to the year 2009 and also for the year 2013. Samples from 2009 to 2012 represent only a quarter of the yearly new born 13 in Catalonia. All samples are irreversibly unlinked and anonymized prior to HIV testing. Anonymity was guaranteed by using a computer-aided coding process at the Neonatal Early Detection Program therefore, the results of HIV antibody testing can’t be linked with any patient identification number. Regional distribution of yearly samples within Catalonia is proportional to regional birth rate.
VariablesVariables collected in the study were: HIV results from testing new born as a surrogate of HIV status of the mother (100% completion), age (100% completion), mother's country or region of birth (from 2007) (>95% completion) and mother's place of current residence (99.6% completion). In order to allow comparisons we established three categories of mother's place of current residence: Barcelona city, cities >200,000 (Hospitalet de Llobregat, Terrassa, Sabadell and Badalona) and cities or towns ≤ 200,000 inhabitants.
Mother's country or region of birth was grouped into Latin America, Sub-Saharan Africa, Spain and rest of the world.
As background information, population data by country of birth were collected from the Annual statistical report of Catalonia. Catalan Institute of Statistics13 and classified according to populations’ origin (Spanish and foreign born) and grouped by categories used to study mother's place of current residence: Barcelona city (more than 1.5 million inhabitants), cities>200,000 and cities or towns ≤ 200,000 inhabitants.
Laboratory methodsTwo drops of blood were collected on filter paper discs (Schleicher and Schuell no. 903TM, Dassel, Germany) and stored at 4°C until used. HIV antibodies were determined using a modified Serodia IgG antibody-capture particle agglutination test for HIV-1 (Fujirebio Diagnostics) 14. Positive samples were sent to the Microbiological Service of the University Hospital Germans Trias I Pujol to confirm the results using an IgG antibody capture ELISA for HIV-1 and HIV-2. Until 2001 this was done using the GACELISA test (Murex, UK) 15. In 2002 up to 2006, this confirmatory test was replaced with the Pasteur HIV-1/2 GenElavia Mixt ELISA (BioRad, Spain) after checking that normal and external valid values were similar for both tests 16. From 2007 to 2009, the test used was BED-CEIA Assay (Calypte Biomedical Inc, Portland, OR, USA) and from 2010 until nowadays, Vitros HIV1+2 Reagent (Ortho Clinical Diagnostics Inc, Cardiff, Wales, UK) is the test used. The surveys are conducted in collaboration with the Catalan Neonatal Early Detection Programme, Service of Biochemistry and Molecular Genetics, Hospital Clinic, Faculty of Medicine, Barcelona, Spain, as well as with the Microbiology Laboratory of the Hospital Germans Trias i Pujol, where reactive samples are confirmed.
Statistical analysisThe annual HIV prevalence among women giving birth was computed as the number of HIV-positive samples divided by the total number of HIV-positive and HIV-negative samples tested each year. Confidence intervals for proportions were calculated by using the Clopper and Pearson method. The Cochran-Armitage test was used as a test for trends of proportions with a 0.05 significance level. Statistical comparisons of prevalence between country or region of birth were performed using chi-squared analysis and Fisher's exact test.
A total of 624,912 infants were tested for HIV antibodies during the 20 years studied (1994-2013). We present the evolution of the population of women aged 15 to 64 years provided that the age range of women giving birth from whom blood samples were taken was 10 to 56 years old. The annual number of live births is also presented to help the interpretation of HIV prevalence.
Due to reductions in financial support, the number of HIV tests performed was reduced during the period 2008 to 2012, although the distribution of samples tested by the mother's place of current residence has been maintained overtime.
Data were analyzed using SAS v 9.3
ResultsDuring the twenty years of study, the number of live births in Catalonia has been rising up to 89,327 in the year 2008 17 and thereafter decreasing to 71,771 in 2013 18,19 In both, Spanish and foreign born mothers, the number of live births increased up to the year 2008 and decreased mainly in Spanish mothers18,19 up to 2010. From 2010 until 2013, there was a 5.9% and 1.7% reduction of foreign and autochthonous live births, respectively. Median age of mothers is 31 years (interquartile range: 28 to 34) being foreign mothers, slightly younger than autochthonous and no differences were found by mother's place of current residence.
Despite changes in population numbers overtime, there were no variations across the geographical categories of cities established by our study.
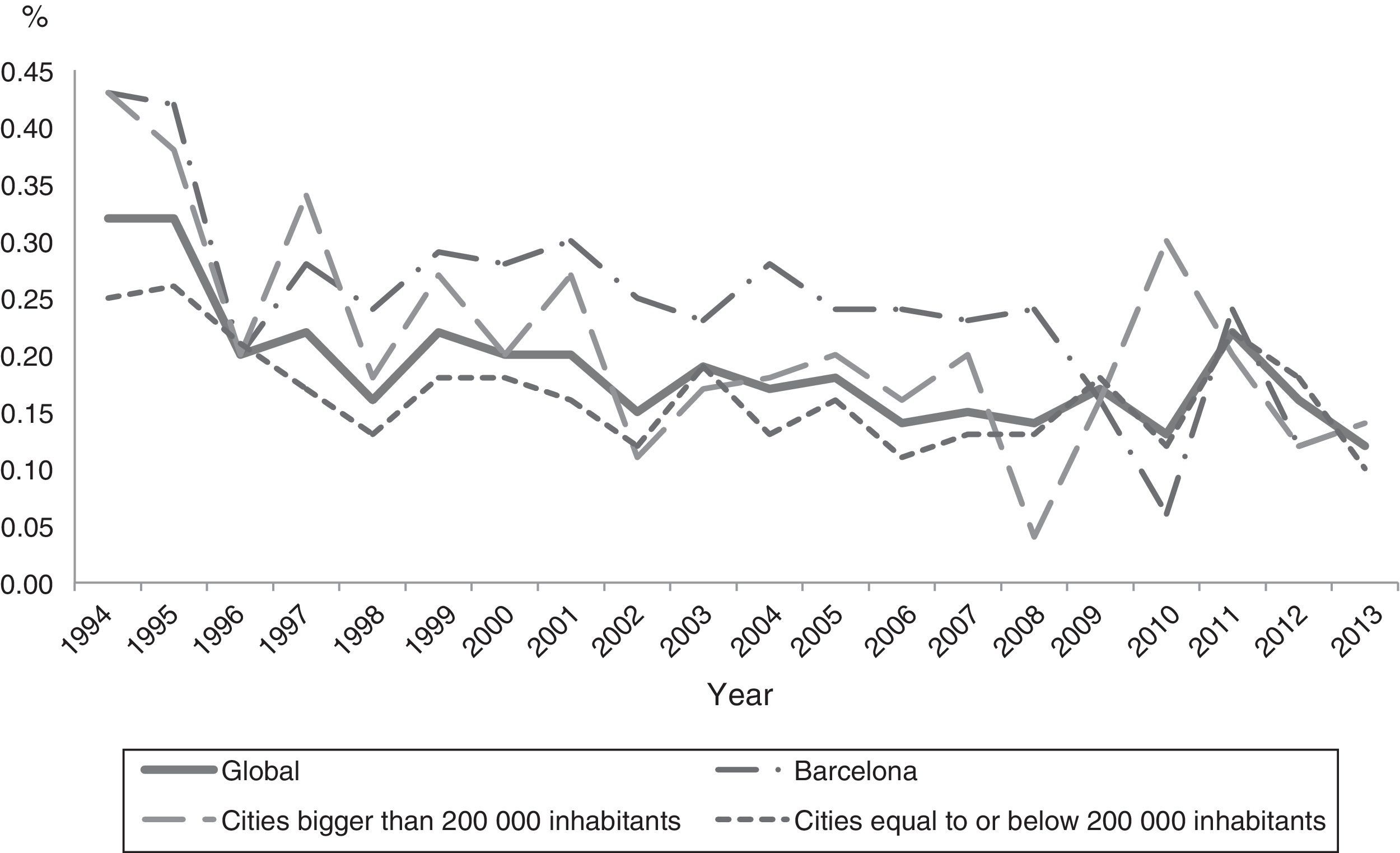
During 1994 to 2007, HIV prevalence trends among women giving birth in all Catalonia are decreasing from 0.32% (95%CI:0.25-0.40) to 0.15% (95%CI:0.12-0.20) (p<0.0001) (Figure 1). In Barcelona city trends are decreasing (p<0.05) from 0.43%(95%CI:0.27-0.64) to 0.23% (95%CI:0.14-0.37) as well as in cities>200,000 inhabitants (p<0.005), from 0.43% (95%CI:0.23-0.73) to 0.20%(95%CI:0.10-0.36) and in cities ≤ 200,000 inhabitants (p<0.0001), from 0.25% (95%CI:0.18-0.35) to 0.13%(95%CI:0.09-0.17), but from 2008 onwards the trend is steady in each geographical category.

In summary, for all the 20 years’ period, HIV prevalence of all women giving birth is higher in Barcelona city than the rest of the Catalan cities (Table 1).
HIV prevalence in women giving birth in Catalonia, by place of current residence. 1994-2013.
| Place of current residence | HIV + | N test | HIV prevalence % | 95%CI |
|---|---|---|---|---|
| Barcelona city | 312 | 123177 | 0,25 | 0,23-0,28 |
| Cities >200,000 inhabitants | 162 | 79864 | 0,20 | 0,17-0,24 |
| Cities ≤ 200,000 inhabitants | 654 | 397842 | 0,16 | 0,15-0,17 |
Information about country of birth was only available from 2007 to 2013. During this period the number of women aged 15 to 64 years living in Catalonia increased by 2% as well as the number of foreign women of this age group.
In the city of Barcelona and other cities>200,000 inhabitants, the number of women aged 15 to 64 years decreased slightly, by 0.2% and 0.3%, respectively. While it increased by 4% in cities ≤ 200,000 inhabitants. The percentage of foreign women over the total number of women of this age group increased everywhere, by 2% in Barcelona city and by 3% in the other two categories of cities (> and ≤ to 200,000 inhabitants).
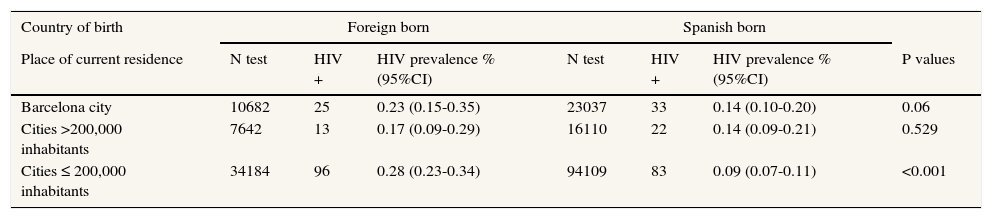
Over the years 2007-2013, foreign women giving birth and living in any of the geographical categories of cities established in our study, showed higher HIV prevalence (0.26%) than Spanish women (0.10%). The highest (0.28%) and lowest (0.09%) levels of HIV prevalence were found in cities ≤ 200,000 inhabitants among foreign and Spanish women giving birth, respectively (Table 2).
HIV prevalence in women giving birth in Catalonia, by country of birth and place of current residence. 2007-2013.
| Country of birth | Foreign born | Spanish born | |||||
|---|---|---|---|---|---|---|---|
| Place of current residence | N test | HIV + | HIV prevalence % (95%CI) | N test | HIV + | HIV prevalence % (95%CI) | P values |
| Barcelona city | 10682 | 25 | 0.23 (0.15-0.35) | 23037 | 33 | 0.14 (0.10-0.20) | 0.06 |
| Cities >200,000 inhabitants | 7642 | 13 | 0.17 (0.09-0.29) | 16110 | 22 | 0.14 (0.09-0.21) | 0.529 |
| Cities ≤ 200,000 inhabitants | 34184 | 96 | 0.28 (0.23-0.34) | 94109 | 83 | 0.09 (0.07-0.11) | <0.001 |
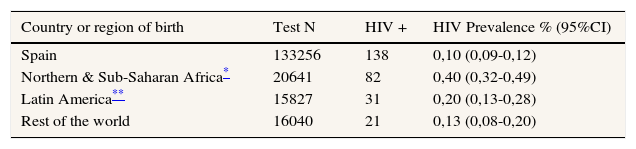
In all Catalonia, the 7 years period HIV prevalence was higher among women born in Sub-Saharan Africa (0.40%) followed by Latin Americans (0.20%) (Table 3).
HIV prevalence in women giving birth in Catalonia, by country or region of birth. 2007-2013.
| Country or region of birth | Test N | HIV + | HIV Prevalence % (95%CI) |
|---|---|---|---|
| Spain | 133256 | 138 | 0,10 (0,09-0,12) |
| Northern & Sub-Saharan Africa* | 20641 | 82 | 0,40 (0,32-0,49) |
| Latin America** | 15827 | 31 | 0,20 (0,13-0,28) |
| Rest of the world | 16040 | 21 | 0,13 (0,08-0,20) |
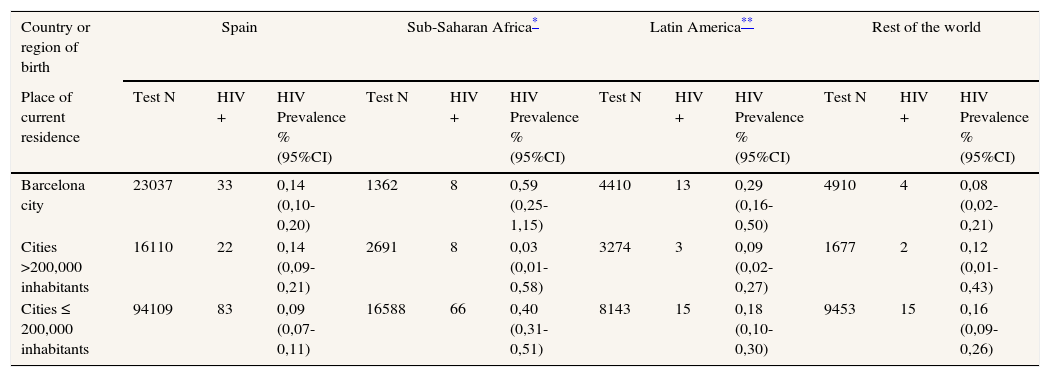
When looking at the current place of residence, the highest HIV prevalence was found in women from Sub-Saharan Africa (0.59%) (p<0.001) and living in Barcelona city or in cities ≤ 200,000 inhabitants, (0.40%), (p<0.0001) followed by those from Latin America and living in Barcelona city (0.29%) (p<0.001) (Table 4).
HIV prevalence in women giving birth in Catalonia by country or region of birth and place of current residence. 2007-2013.
| Country or region of birth | Spain | Sub-Saharan Africa* | Latin America** | Rest of the world | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Place of current residence | Test N | HIV + | HIV Prevalence % (95%CI) | Test N | HIV + | HIV Prevalence % (95%CI) | Test N | HIV + | HIV Prevalence % (95%CI) | Test N | HIV + | HIV Prevalence % (95%CI) |
| Barcelona city | 23037 | 33 | 0,14 (0,10-0,20) | 1362 | 8 | 0,59 (0,25-1,15) | 4410 | 13 | 0,29 (0,16-0,50) | 4910 | 4 | 0,08 (0,02-0,21) |
| Cities >200,000 inhabitants | 16110 | 22 | 0,14 (0,09-0,21) | 2691 | 8 | 0,03 (0,01-0,58) | 3274 | 3 | 0,09 (0,02-0,27) | 1677 | 2 | 0,12 (0,01-0,43) |
| Cities ≤ 200,000 inhabitants | 94109 | 83 | 0,09 (0,07-0,11) | 16588 | 66 | 0,40 (0,31-0,51) | 8143 | 15 | 0,18 (0,10-0,30) | 9453 | 15 | 0,16 (0,09-0,26) |
HIV prevalence among women giving birth in Catalonia is currently low (0.12% in 2013), although a significant difference was found on comparing Spanish and foreign born women from HIV endemic areas. As stated by a recent ECDC report 20, between 2007 and 2011 migrant populations in Europe are disproportionally affected by HIV, although there might be significant variations between countries.
We may hypothesize that due to the economical crisis starting in 2008, economically and socially deprived populations (foreign and autochthonous) living in big cities may have moved to smaller cities where living conditions are easier and less expensive, consequently increasing the social needs in these areas.
Also, to be considered is the reduction of the number of births in Catalonia, starting in 2009, from 89,327 new born in 2008 to 81,137 in 2011. Major reductions are among births in the foreign population: from the year 2010 to 2011 there was a 5.9% and 1.7% reduction of, foreign and autochthonous births, respectively. Nevertheless, these reductions don’t seem to affect the HIV prevalence estimations.
In any case, the fact that highest HIV prevalence is found among Sub-Saharan Africa and Latin-America women giving birth and living in Barcelona or in towns and cities ≤ 200,000 inhabitants, indicates that HIV surveillance, antenatal and mother's care have to be maintained and enhanced in both Catalan geographical areas, with special attention to address cultural and language barriers, in order to ensure proper identification and timely treatment of HIV infected mothers.
In Catalonia, differently to UK 21, it is unknown whether foreign born citizens living with HIV are less likely to access healthcare, mainly due to social isolation or insecure immigration status 22. This situation, although improbable because of the universal access to healthcare, may impact on diagnosis and access to HIV treatment. The number of HIV infected women reported as pregnant can only be estimated from unlinked anonymous testing and there is no institutionally established surveillance system to monitor mother to child transmission although data are annually retrieved from a clinicians’ managed data base of a cohort of mother and child pairs.
This study has some limitations such as: birth rates by mother's country of birth (foreign and autochthonous) and place of current residence could not be retrieved. Had this information been available it would have helped to better explain our findings.
More accurate estimates of HIV prevalence at district level and not only at town or city level may allow better targeting of resources in bigger cities. This information was not available from the data collected until nowadays, although some changes have been proposed from the year 2014 onwards.
In conclusion, this study reports on the only Catalan population-based HIV prevalence data currently available for women giving birth that has been carried out for two decades; these data have been a valuable tool for monitoring trends, targeting resources and evaluating programs and policies.
HIV prevalence in women giving birth in Catalonia continue to occur predominantly in women born abroad coming from countries with high HIV prevalence (ie: Sub-Saharan Africa) mirroring the situation of their country of origin.
The new Spanish legislation 23 denying health assistance to migrants without residence permit may reduce accessibility of vulnerable women to care aggravating the situation of coming years. Further studies should be developed to ascertain entrance and retention to care of these HIV infected women giving birth.
This paper, as well as other studies4, underlines the value of studying populations’ origins in monitoring HIV prevalence in diverse populations as well as the need to ensure reaching these populations on time.
HIV unlinked anonymous testing of neonatal dried blood spots taken for metabolic screening is simple, cheap and has the added advantage of providing unbiased prevalence rates. From 1994 to 2007 there has been a declining trend of HIV prevalence among women giving birth in Catalonia.
What does this study add to the literature?From 2008 onwards highest HIV prevalence rates were among women born in Sub-Saharan Africa or Latin America and living in Barcelona City and cities ≤ 200,000 inhabitants. Therefore, antenatal and postnatal care should be maintained and strengthened with special attention to ascertain entrance and retention to care, addressing cultural and language barriers of these HIV infected women giving birth.
Pere Godoy.
Authorship contributionsConceived and designed the studyDolors Carnicer-Pont, Alexandra Montoliu, Jose Luis Marin and Jordi Casabona
Performed the studyJose Luis Marin, Carmen Martinez, Victoria Gonzalez and Rafael Muñoz
Analysed dataDolors Carnicer-Pont and Alexandra Montoliu
Wrote and commented the manuscriptDolors Carnicer-Pont, wrote the article and Mireia Jane and Jesus Almeda gave critical inputs and a valuable intellectual contribution. The remaining authors also commented on the manuscript.
FundingNo external funding
Conflicts of interestNone of the authors has a conflict of interest.
We acknowledge the contributions of: Dr. Antonio Maya and Dr. Joan Massip that have been part of the HIV working group until the year 2007 and 2008, respectively.
Agència de Salut Pública de Catalunya, ASPCAT (A Mateu); Servei de Microbiologia, Hospital Universitari Germans Trias I Pujol, Badalona (V Ausina, L Matas, E Martró, D Sánchez); Unitat de Cribratge Perinatal. LCE.CDB. Corporació Sanitària Clínic, Barcelona.











