



To examine trends in the prevalence of problematic cocaine use in a large city and describe the problems encountered when estimating these trends using capture-recapture techniques based on secondary data
MethodsWe used clinical data on accident and emergency department episodes at four university hospitals in Barcelona (Spain) between 1999 and 2008 (3 capture periods per year). Users were categorized into two subgroups depending on concomitant heroin use (cocaine plus heroin, cocaine without heroin).
ResultsThe mean age of users was 34 years and 25% were women (2008). The mean number of episodes per user differed between drug subgroups and over time. The estimated total number of cocaine users increased from 6,028 (95% confidence interval [95%CI]: 4,086-9,327) in 1999 to 22,640 (95%CI: 14,001-37,500) in 2006, but decreased thereafter. The prevalence of problematic use of cocaine plus heroin was stable throughout the study. Thus, trends in the prevalence of problematic cocaine use differed depending on concomitant heroin use.
ConclusionOur results are consistent with those provided by health surveys and treatment registries. They also highlight the pitfalls of applying the capture-recapture approach to secondary data, and the need for a better understanding of how information is collected and changes over time.
Explorar la tendencia de la prevalencia del consumo problemático de cocaína en una gran ciudad y describir los problemas encontrados cuando se estiman estas tendencias mediante técnicas de captura-recaptura utilizando datos secundarios.
MétodosSe utilizaron los datos de los servicios de urgencias de cuatro hospitales universitarios de Barcelona entre 1999 y 2008 (tres capturas por año). Las personas se clasificaron en dos subgrupos según el uso concomitante de heroína (cocaína junto con heroína, cocaína sin heroína).
ResultadosLa edad media fue de 34 años (2008) y el 25% eran mujeres. El número medio de episodios por paciente fue distinto según el subgrupo y el año. La estimación del número total de consumidores/as problemáticos/as de cocaína aumentó de 6028 (intervalo de confianza del 95% [IC95%]: 4086-9327) en 1999 a 22.640 (IC95%: 14.001-37.500) en 2006, y disminuyó a partir de entonces. La prevalencia del consumo problemático de cocaína más heroína se mantuvo estable durante el período. Por lo tanto, las tendencias de prevalencia diferían dependiendo del consumo de heroína concomitante.
ConclusiónLos resultados concuerdan con los de las encuestas de salud y con los registros de tratamiento. Los resultados también ponen de relieve ciertos peligros en la aplicación de la captura-recaptura para datos secundarios, y la necesidad de un conocimiento profundo de cómo se recopila la información y los posibles cambios en el tiempo.
The capture-recapture approach is an indirect method of generating prevalence estimates based on the degree of overlap (the appearance of a case/individual in more than one sample)1 between two or more distinct samples of the study population, and has been used to estimate prevalence in many epidemiological scenarios,2 including hard to reach populations3,4 such as illegal drug users.5 Surveys designed to estimate the prevalence of illegal drug use have the important limitation that illegal drug users are hard to detect because they are a small fraction of the population and often conceal themselves due to the illegal and highly stigmatized nature of drug-taking.6 Thus, the capture-recapture technique has been used in distinct geographical areas, including cities of different sizes, to estimate the prevalence of illegal drug use, mainly of opiates and cocaine.5,7–10While capture-recapture has proven to be adequate for estimating prevalence in incomplete epidemiological data,2,11 it involves certain assumptions: 1) the target population must be closed; 2) false-positive subjects should not be present on any list; 3) capture sources should be independent; and 4) each case in the population should be equally likely to be captured in each source.11 In addition to these assumptions,11 this approach has other limitations: the specific application of the method, especially when using secondary data that is susceptible to changes in the data collection protocol, as well as on professional criteria in identifying relevant characteristics.12
Cocaine is one of the most widely used illegal drugs in Europe, and Spain has one of the highest prevalence rates.13 To assess the consequent burden on health care services and the need for preventive interventions, it is important for public health officials to have a clear picture of the magnitude of problematic cocaine use and trends in consumption.
The aim of this study was to examine trends in the prevalence of problematic cocaine use in Barcelona (Spain) through the capture-recapture approach based on a secondary data source, namely visits to the city's four main emergency rooms (ER). We also describe problems encountered in applying this approach.
MethodsThe Barcelona Drug Information System (SIDB) created in 1987 collects information about ER at the city's four university hospitals that involved patients aged 15-54 years, and where the corresponding clinical record mentioned the use of illegal drugs. A previous study found that these emergency rooms covered about 95% of drug-related emergencies in Barcelona14. We selected visits between 1999 and 2008 involving Barcelona city residents who visited the ER at least once in the year in question, with a medical record mentioning cocaine. ER records do not always report consumed substances7, so we considered that all substances mentioned in the ER record(s) for each patient in a given year had been used by him/her throughout the year. Episodes for each individual were grouped using a confidential identification algorithm.
We collected data on age, gender, and drugs used. Data on drugs used were collected from clinical notes written by the physician. Individuals were categorized into two consumer profiles according to their concomitant use of opioids (mainly heroin) in any episode in a given year: either “cocaine plus heroin”, or “cocaine without heroin”. A single source capture-recapture technique was applied for each individual year 2,15 to estimate the prevalence of problematic cocaine use for the entire sample and separately for each consumer profile, cocaine with heroin and cocaine without heroin.
We assumed that the prevalence did not vary within a given calendar year. To assess possible sample dependences, the ER register for a full year was divided into three 4-month periods, and each period was considered to be a distinct sample.5,7,16 To estimate the unknown population, we fitted log-linear regression models for each year and each consumer profile. To adjust for possible dependencies between samples, we fitted models with all possible combinations of interactions (one, two or three interactions of two 4-month periods), and evaluated the best fit using the Bayesian Information Criterion (BIC).1,17 Models with a deviance of less than±2 degrees of freedom were considered well-fitted. When we found more than one model with a good fit, we computed the estimate for the unknown population by averaging BIC-weighted estimates from the adjusted models (the BIC-weighted estimates were calculated using NˆwIC=∑(Nˆi·e−(ICi/2))/∑e−(ICi/2), where ICi is the BIC information considered and Nˆi is the population estimate associated with each model i)18. When dependence between the three capture periods was not rejected, we fitted the saturated model to estimate the unknown population.11 Finally, 95% confidence intervals (95%CI) were calculated according to Cormack.15,19
All analyses were performed using STATA version 11 and R 2.8.
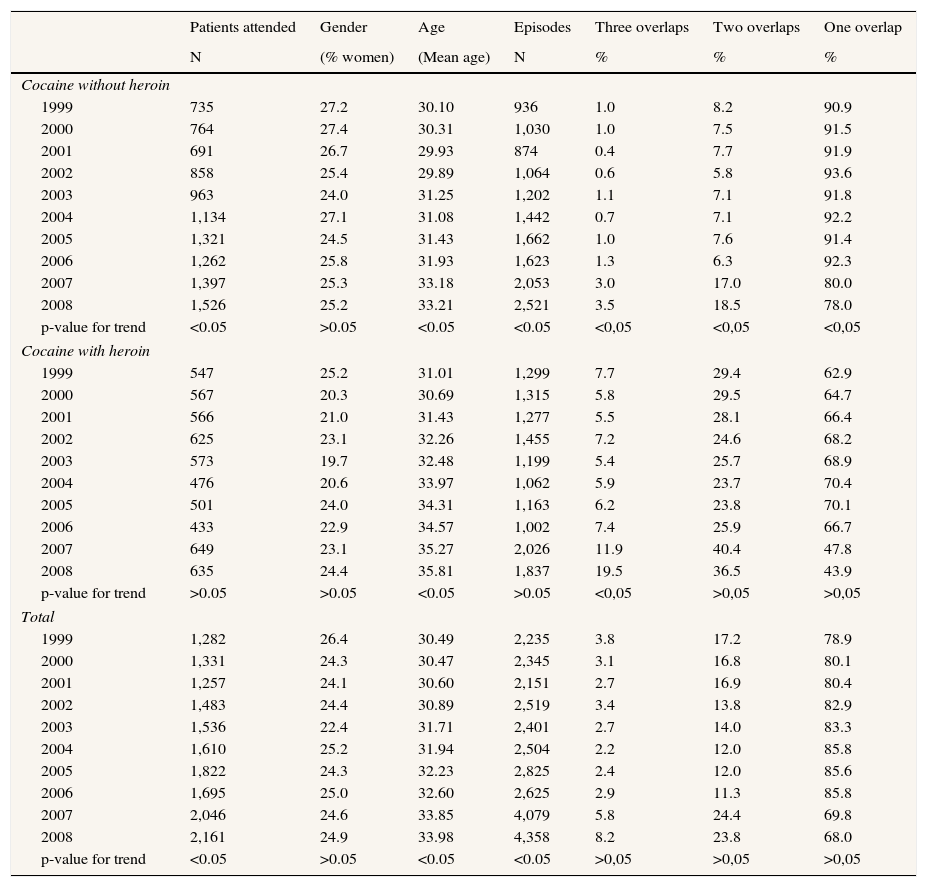
ResultsOver the period of this study, we observed an increase in the number of patients who received emergency treatment with a mention of cocaine in their medical record: from 1,282 in 1999 to 2,161 in 2008 (Table 1). This increase was statistically significant (p-value for trend <0.05) in patients who consumed cocaine without heroin, but not those who consumed cocaine with heroin. The number of emergency episodes also increased during this period, from 2,235 in 1999 to 4,358 in 2008. The number of overlaps (when an individual appears in more than one trimester) remained constant between 1999 and 2006, but increased in 2007 and 2008. The mean proportion of patients in the cocaine with heroin and cocaine without heroin groups who received emergency treatment once in a year was 67.3% and 92.0% between 1999 and 2006, respectively, and 45.8% and 79.0% in 2007-2008. The percentage of female patients remained constant at around 25%, while the average age of patients increased over time in both groups (cocaine with heroin and cocaine without heroin) (Table 1).
Characteristics of patients visited in hospital emergency rooms with a mention of cocaine use on their medical record. Barcelona, 1999-2008.
| Patients attended | Gender | Age | Episodes | Three overlaps | Two overlaps | One overlap | |
|---|---|---|---|---|---|---|---|
| N | (% women) | (Mean age) | N | % | % | % | |
| Cocaine without heroin | |||||||
| 1999 | 735 | 27.2 | 30.10 | 936 | 1.0 | 8.2 | 90.9 |
| 2000 | 764 | 27.4 | 30.31 | 1,030 | 1.0 | 7.5 | 91.5 |
| 2001 | 691 | 26.7 | 29.93 | 874 | 0.4 | 7.7 | 91.9 |
| 2002 | 858 | 25.4 | 29.89 | 1,064 | 0.6 | 5.8 | 93.6 |
| 2003 | 963 | 24.0 | 31.25 | 1,202 | 1.1 | 7.1 | 91.8 |
| 2004 | 1,134 | 27.1 | 31.08 | 1,442 | 0.7 | 7.1 | 92.2 |
| 2005 | 1,321 | 24.5 | 31.43 | 1,662 | 1.0 | 7.6 | 91.4 |
| 2006 | 1,262 | 25.8 | 31.93 | 1,623 | 1.3 | 6.3 | 92.3 |
| 2007 | 1,397 | 25.3 | 33.18 | 2,053 | 3.0 | 17.0 | 80.0 |
| 2008 | 1,526 | 25.2 | 33.21 | 2,521 | 3.5 | 18.5 | 78.0 |
| p-value for trend | <0.05 | >0.05 | <0.05 | <0.05 | <0,05 | <0,05 | <0,05 |
| Cocaine with heroin | |||||||
| 1999 | 547 | 25.2 | 31.01 | 1,299 | 7.7 | 29.4 | 62.9 |
| 2000 | 567 | 20.3 | 30.69 | 1,315 | 5.8 | 29.5 | 64.7 |
| 2001 | 566 | 21.0 | 31.43 | 1,277 | 5.5 | 28.1 | 66.4 |
| 2002 | 625 | 23.1 | 32.26 | 1,455 | 7.2 | 24.6 | 68.2 |
| 2003 | 573 | 19.7 | 32.48 | 1,199 | 5.4 | 25.7 | 68.9 |
| 2004 | 476 | 20.6 | 33.97 | 1,062 | 5.9 | 23.7 | 70.4 |
| 2005 | 501 | 24.0 | 34.31 | 1,163 | 6.2 | 23.8 | 70.1 |
| 2006 | 433 | 22.9 | 34.57 | 1,002 | 7.4 | 25.9 | 66.7 |
| 2007 | 649 | 23.1 | 35.27 | 2,026 | 11.9 | 40.4 | 47.8 |
| 2008 | 635 | 24.4 | 35.81 | 1,837 | 19.5 | 36.5 | 43.9 |
| p-value for trend | >0.05 | >0.05 | <0.05 | >0.05 | <0,05 | >0,05 | >0,05 |
| Total | |||||||
| 1999 | 1,282 | 26.4 | 30.49 | 2,235 | 3.8 | 17.2 | 78.9 |
| 2000 | 1,331 | 24.3 | 30.47 | 2,345 | 3.1 | 16.8 | 80.1 |
| 2001 | 1,257 | 24.1 | 30.60 | 2,151 | 2.7 | 16.9 | 80.4 |
| 2002 | 1,483 | 24.4 | 30.89 | 2,519 | 3.4 | 13.8 | 82.9 |
| 2003 | 1,536 | 22.4 | 31.71 | 2,401 | 2.7 | 14.0 | 83.3 |
| 2004 | 1,610 | 25.2 | 31.94 | 2,504 | 2.2 | 12.0 | 85.8 |
| 2005 | 1,822 | 24.3 | 32.23 | 2,825 | 2.4 | 12.0 | 85.6 |
| 2006 | 1,695 | 25.0 | 32.60 | 2,625 | 2.9 | 11.3 | 85.8 |
| 2007 | 2,046 | 24.6 | 33.85 | 4,079 | 5.8 | 24.4 | 69.8 |
| 2008 | 2,161 | 24.9 | 33.98 | 4,358 | 8.2 | 23.8 | 68.0 |
| p-value for trend | <0.05 | >0.05 | <0.05 | <0.05 | >0,05 | >0,05 | >0,05 |
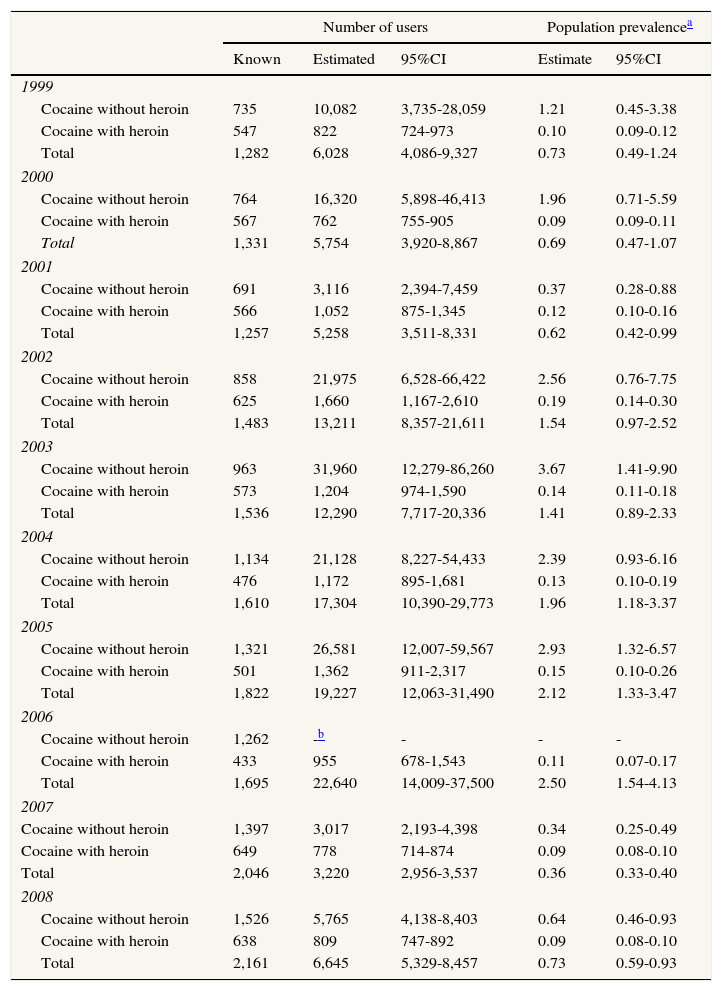
The estimated annual prevalence of problematic cocaine use is shown in Table 2. The estimated number of users in Barcelona increased from 6,028 (95%CI: 4,086-9,327) in 1999 to 22,640 (95%CI: 14,009-37,500) in 2006, and decreased to 6,645 by 2008 (95%CI: 5,329-8,457), comparable to the initial rate in 1999. The use of cocaine without heroin was the most common consumer profile, and its prevalence increased rapidly and then decreased during the study period (1.21% in 1999, 2.93% in 2005, and 0.64% in 2008). In contrast, the prevalence of cocaine use with heroin was lower and remained stable during the study period (0.10% in 1999, 0.15% in 2005 and 0.09% in 2008).
Estimated prevalence of problematic cocaine use by subgroup and year. Barcelona, 1999-2008.
| Number of users | Population prevalencea | ||||
|---|---|---|---|---|---|
| Known | Estimated | 95%CI | Estimate | 95%CI | |
| 1999 | |||||
| Cocaine without heroin | 735 | 10,082 | 3,735-28,059 | 1.21 | 0.45-3.38 |
| Cocaine with heroin | 547 | 822 | 724-973 | 0.10 | 0.09-0.12 |
| Total | 1,282 | 6,028 | 4,086-9,327 | 0.73 | 0.49-1.24 |
| 2000 | |||||
| Cocaine without heroin | 764 | 16,320 | 5,898-46,413 | 1.96 | 0.71-5.59 |
| Cocaine with heroin | 567 | 762 | 755-905 | 0.09 | 0.09-0.11 |
| Total | 1,331 | 5,754 | 3,920-8,867 | 0.69 | 0.47-1.07 |
| 2001 | |||||
| Cocaine without heroin | 691 | 3,116 | 2,394-7,459 | 0.37 | 0.28-0.88 |
| Cocaine with heroin | 566 | 1,052 | 875-1,345 | 0.12 | 0.10-0.16 |
| Total | 1,257 | 5,258 | 3,511-8,331 | 0.62 | 0.42-0.99 |
| 2002 | |||||
| Cocaine without heroin | 858 | 21,975 | 6,528-66,422 | 2.56 | 0.76-7.75 |
| Cocaine with heroin | 625 | 1,660 | 1,167-2,610 | 0.19 | 0.14-0.30 |
| Total | 1,483 | 13,211 | 8,357-21,611 | 1.54 | 0.97-2.52 |
| 2003 | |||||
| Cocaine without heroin | 963 | 31,960 | 12,279-86,260 | 3.67 | 1.41-9.90 |
| Cocaine with heroin | 573 | 1,204 | 974-1,590 | 0.14 | 0.11-0.18 |
| Total | 1,536 | 12,290 | 7,717-20,336 | 1.41 | 0.89-2.33 |
| 2004 | |||||
| Cocaine without heroin | 1,134 | 21,128 | 8,227-54,433 | 2.39 | 0.93-6.16 |
| Cocaine with heroin | 476 | 1,172 | 895-1,681 | 0.13 | 0.10-0.19 |
| Total | 1,610 | 17,304 | 10,390-29,773 | 1.96 | 1.18-3.37 |
| 2005 | |||||
| Cocaine without heroin | 1,321 | 26,581 | 12,007-59,567 | 2.93 | 1.32-6.57 |
| Cocaine with heroin | 501 | 1,362 | 911-2,317 | 0.15 | 0.10-0.26 |
| Total | 1,822 | 19,227 | 12,063-31,490 | 2.12 | 1.33-3.47 |
| 2006 | |||||
| Cocaine without heroin | 1,262 | -b | - | - | - |
| Cocaine with heroin | 433 | 955 | 678-1,543 | 0.11 | 0.07-0.17 |
| Total | 1,695 | 22,640 | 14,009-37,500 | 2.50 | 1.54-4.13 |
| 2007 | |||||
| Cocaine without heroin | 1,397 | 3,017 | 2,193-4,398 | 0.34 | 0.25-0.49 |
| Cocaine with heroin | 649 | 778 | 714-874 | 0.09 | 0.08-0.10 |
| Total | 2,046 | 3,220 | 2,956-3,537 | 0.36 | 0.33-0.40 |
| 2008 | |||||
| Cocaine without heroin | 1,526 | 5,765 | 4,138-8,403 | 0.64 | 0.46-0.93 |
| Cocaine with heroin | 638 | 809 | 747-892 | 0.09 | 0.08-0.10 |
| Total | 2,161 | 6,645 | 5,329-8,457 | 0.73 | 0.59-0.93 |
95%CI: 95% confidence interval.
The prevalence of problematic cocaine use in the city of Barcelona increased between 1999 and 2006, and decreased rapidly in the following two years; in contrast, the number of emergency room visits involving cocaine use increased continuously during this period. This prevalence trend differed between the two consumer profiles analyzed, remaining stable in the cocaine plus heroin group, and following the overall trends described above in the cocaine without heroin.
A strength of the study is the fact that the prevalence of problematic cocaine use was estimated in a large sample from a well-defined geographical area over a period of several years, and using the same capture-recapture approach with the same source of information. Overall trends (including confidence intervals) for the period 1999-2006 are consistent with those reported by other studies using indirect indicators (treatment demand data and mortality) in Barcelona,20,21 and with others in Spain and other European countries.13,22 However, the decrease observed after 2006 was unexpected, especially given the increase in the number of emergency episodes in which cocaine was mentioned in the medical record. In considering the possible reasons for this decrease, we observed that the magnitude and confidence intervals of the estimates were affected by an increase in the mean number of episodes per person in 2007-2008. Capture-recapture is very sensitive to changes in the number of overlaps, which may cause over- and underestimation.1 In epidemiological studies these changes may derive from data collection patterns. While we were not able to test the influence of contextual changes that occurred during the study period on trends in problematic cocaine use, our results could be partly due to increased access to emergency rooms or changes in how the patients are registered. In our case, the increasing mean number of episodes per person, and thus of overlaps, is probably due to changes in physicians’ awareness of cocaine use in emergency situations and its report. The increasing mean number of episodes per person is especially relevant when few overlaps are present.
Furthermore, stratifying the analysis into two consumer profile subgroups, the trend among users of both heroin and cocaine mirrored the stable pattern of heroin use in the city, whereas the estimated prevalence of consumers of cocaine without heroin had wide confidence intervals and an unexpected trend over time. Estimates for the cocaine with heroin group are stable because of the high number of overlaps during the study period (more than 40% of the sample); the increase in the number of episodes was probably prompted by their physical problems and stigma.12,23 The low proportion of repeated episodes in the cocaine without heroin group (<10% of overlaps before 2007, and 20% thereafter) resulted in unstable estimates, and prevented us from generating an estimate for one of the study years (2006). The observed increase in the number of overlaps could also be an artifact related to changes either in some aspects of the population (e.g., health status, patterns of use) or in health services available, although they seem unlikely to be important, according to published information on the city's health services.
Another possible limitation is users’ tendency to underreport cocaine use when attending the ER,12,24–26 and we attempted to minimize this bias by considering all substances mentioned by individuals in a given year. While this underreporting might differentially affect the two consumer profile subgroups studied, probably with a greater impact in the cocaine without heroin subgroup, the epidemiological curve would not be greatly affected if underreporting remained constant over time. In addition, considering only ER data is another possible cause of underreporting, as reported previously.5 Other possible limitations include assumptions of the capture-recapture approach, as reported in other studies11, and to the fact that we cannot account for various confounding variables (e.g., socioeconomic variables) that could influence the prevalence trend. Further studies should focus on this topic. Finally, it was only possible to analyze data from 1999 to 2008 because more recent data were not available. However, the 10-year trend observed was relevant per se, as discussed above.
Trends in the prevalence of cocaine use may differ depending on whether or not other drugs were used concomitantly (e.g., heroin in the present study). Our results also highlight some of the dangers involved in applying the capture-recapture approach to secondary data, in that a considerable number of samples’ overlaps is needed, and contextual changes may lead to significant variation in the type of information gathered in clinical records. Relying on secondary data to assess basic epidemiological indicators requires a thorough understanding of how this information is collected and of changes in the data collection procedure over time.
Capture-recapture is a widely used method to estimate prevalence of hidden populations. In Spain, the cocaine use epidemic followed a large epidemic of heroin use and, in fact, its increase overlapped with a decrease in the heroin use epidemic.
What does this study add to the literature?The prevalence of problematic cocaine use increased steadily up to 2006, after which it appeared to decline. Cocaine prevalence trends may differ depending on concomitant drug use. Contextual changes may lead to relevant variations in the information gathered in clinical records, affecting prevalence estimates. In capture-recapture, a certain amount of overlap between samples is needed to avoid results being inconsistent.
Alberto Ruano-Ravina.
Transparency DeclarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
FundingAddictive Disorders Network (RTA-RD12 / 0028/0018) contributed to the accomplishment of this work.
Authorship contributionsA. Espelt, A. Domingo-Salvany, A. Sanchez-Niubó and MT Brugal were involved in the conception and design of the work. A. Espelt, A. Sánchez-Niubó and M. Mari-Dell’Olmo carried out the analysis and interpretation of data. The first version of the manuscript was written by A. Espelt and was subsequently improved by all authors, with important intellectual contributions. All authors have approved the final version and are jointly responsible for adequate revision and discussion of all aspects included in the manuscript
Conflicts of interestNone.











