



The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
Más datosPMS symptoms can include anxiety, quick temper, excessive strain on the breasts, increased or decreased appetite, nausea, vomiting, acne, low back pain, to faint. This study aimed to determine the effect of estrogen hormone in Adolescent Girls who experienced premenstrual syndrome at Darul Arqam, Makassar.
MethodsThe research design used the cross-sectional approach using the purposive sampling technique to get the samples of female teenagers who had PMS and another 25 samples of female teenagers who did not have PMS. The respondent who had experienced PMS filled in the daily diary sheets, did the blood taking of five ccs and underwent the examination of estrogen level using ELISA method. The study was conducted for three months, and the data were analyzed using the Mann–Whitney U test.
ResultThe research result indicated that the mean value of estrogen hormone in adolescent girls who experienced PMS was 148.32pg/ml higher than the female teenagers who did not experience PMS of 98.00pg/ml. The analysis result indicated that Ha was accepted, and H0 was rejected since the mean value in PMS teenagers was higher compared to the non-PMS teenagers with the value of p=0.000<α=0.05. This result showed a significant effect of estrogen hormone in adolescent girls who experienced PMS compared to those who did not experience PMS. The adolescent girls who experience mild PMS with the mean value of estrogen hormone were 130.73pg/dl, while those who experienced severe PMS of 162.14pg/ml.
ConclusionIt was found that the value of p=0.000<α=0.05, which indicated that there was a significant effect of the levels of estrogen hormone between the non-PMS, mild PMS, and severe PMS.
PMS symptoms could be indicated feeling excessive, irritable, late in the breasts, increased appetite, or vomiting, acne breakouts, back pain, and fainting. With some of these symptoms, it can be ascertained that PMS tends to reduce the productivity of adolescents in general.1 The impact of PMS includes reduced performance in the workplace. Depression can be subject to feelings of suicidal thoughts, even the desire to commit violence on oneself or others. Hence, there is also a condition where a person wakes up feeling angry, anxious, and/or sad in the morning. It is not uncommon for depression, anger, aggressive or excessive nature and has consequences for the person or the surrounding environment.2
In America, the incidence reaches 70–90%, Sweden around 61–85%, Morocco 51.2%, Australia 85, Japan reaches 95%, and Taiwan 73% who experience PMS. Knight, in 2004 announced that research at least 50% of women experience PMS. Likewise, symptoms of PMS have been reported to affect as many as 90% of women of reproductive age in the United States. The determination of a survey of 242 students at Jimma University, Ethiopia, with an average age of 20 years of respondents who found 99.6% of participants experiencing PMS. It was reported that 27% of the participants experienced premenstrual dysphoric disorder, 14% often missed classes, and 15% could not take exams because of their PMS.3
In Iran, it was found that around 98.2% of students experienced PMS with mild or moderate degrees; the overall evidence suggests that PMS is a common form of disorder experienced by teenagers in Asia. In Sri Lanka, PMS affects about 65.7% of young women (American College of Obstetricians and Gynecologists). In Indonesia, the incidence rate is around 70–90% (Ernawati, 2012). One of the causes of PMS is the factor of women's nutritional status. Other causes are due to hormonal imbalance, psychological factors, social problems, and serotonin dysfunction. The nutritional status of adolescent girls greatly affects the occurrence of menarche (first menstruation).4
PMS that occurs in adolescents can reduce productivity in carrying out daily activities. PMS symptoms in adolescents can affect their performance at A study conducted in 2011 with hsCRP levels <1.70% of women, as many as seven respondents experienced mild PMS. Meanwhile, for those with hs-CRP levels >1, 70% of respondents with severe PMS had a body mass index of eight waist circumference, 70% had severe PMS. The hs-CRP level is five times (IK: 2,155–204,614) is at risk for PMS. While the waist circumference is five times (CI: 1,039–28,533), there is a risk of STDs. Based on the previous, this study aims to respondents who had a normal BMI of 30% had severe PMS. Meanwhile, of the 15 respondents with obese BMI, 70% had severe PMS. Based on the waist circumference size of 6 respondents who had normal waist circumference, 30% had severe PMS. Meanwhile, of the 14 respondents with obesity, determine the effect of the hormone estrogen on adolescent girls who experience premenstrual syndrome.5
MethodsThis study used a cross-sectional where the Researcher demand to see the effect of estrogen levels on adolescent girls who experience premenstrual syndrome. The research location was carried out at the Ummul Mukminin Islamic Boarding School in Makassar. The research period was accomplished in March–May 2018. The population was all students at Darul Arqam Islamic Boarding School who experienced PMS. Therefore, the sample was part of the population to be studied or a part of the characteristics possessed by the population, namely young girls who experienced PMS at Darul Arqam Islamic Boarding School Makassar. The sample used is the formula of Stephen Issac and William B. Michael. The number of samples is determined based on Isaac and Michael's table with a significance level of 95% and based on the error rate of 1%, 5%, and 10%. The samples obtained with PMS were 25 people, and 25 people did not experience PMS, considering the inclusion and exclusion criteria.
Data collection was carried out with research preparation; (1) Preparation of menstrual cycle daily notes (LCH) (2) Arrangement of research permits for the principal of Madrasah Aliyah Pesantren Darul Arqam, research permit from the health research ethics committee, Hasanuddin University, RSPTN UH, RSP dr. Wahidin Sudirohusoda (Number: 72/H4-8.4.5.3.1/PP 36-KOMETIK/2018). Initial data collection was conducted to determine the population size and minimum sample size required in the study. This study, began with sample grouping according to inclusion and exclusion criteria. Then take blood samples, then was collected, processed, and analyzed. Furthermore, the conclusion is drawn according to the research results. After the data was collected, the data was managed with the help of Excel and SPSS version 21 computer programs. Analysis of the effect of the estrogen hormone using the ELISA kit on adolescent girls who experienced PMS was then performed data management using univariable, and bivariable analyzed using the Mann–Whitney U test.
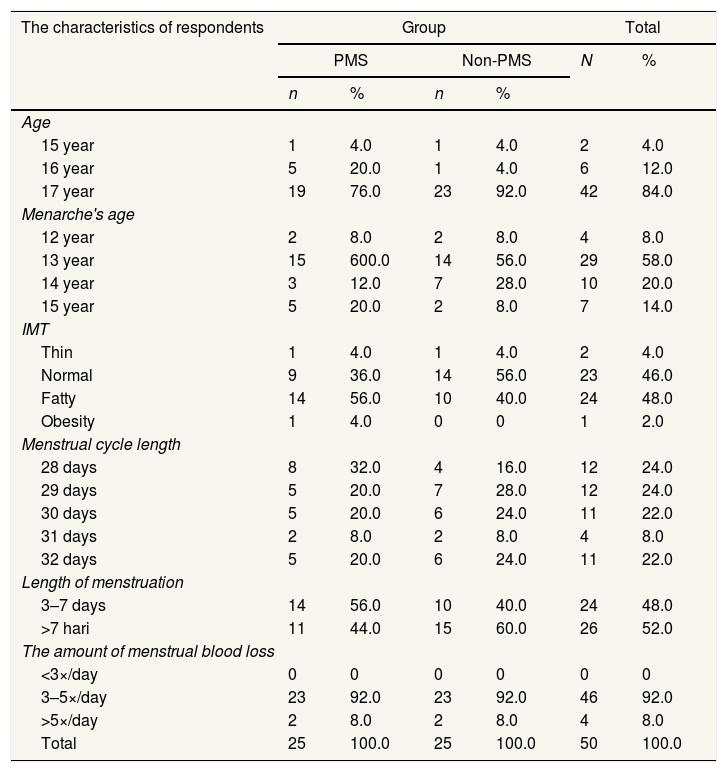
ResultUnivariate analysisFrom Table 1, it clearly shows that the 25 respondents with PMS the most age group was 17 years, namely 19 people (76%), the lowest was 15 years (4%), while of the 25 respondents who are not PMS the most age group was 23 people (92%). at 15 and 16 years, namely 1 person (4%), the most menarche age was 11 years old as many as 15 people (60%) and the lowest was 13 years old as many as 2 people (8%), while respondents who were not PMS had the most menarche age, namely 13 14 people (56%) and the lowest at 12 and 15 years were 2 people (8%).
The distribution of respondents based on the characteristics of young women who have PMS and non-PMS in the Darul Arqam Islamic Boarding School in Makassar in 2018.
| The characteristics of respondents | Group | Total | ||||
|---|---|---|---|---|---|---|
| PMS | Non-PMS | N | % | |||
| n | % | n | % | |||
| Age | ||||||
| 15 year | 1 | 4.0 | 1 | 4.0 | 2 | 4.0 |
| 16 year | 5 | 20.0 | 1 | 4.0 | 6 | 12.0 |
| 17 year | 19 | 76.0 | 23 | 92.0 | 42 | 84.0 |
| Menarche's age | ||||||
| 12 year | 2 | 8.0 | 2 | 8.0 | 4 | 8.0 |
| 13 year | 15 | 600.0 | 14 | 56.0 | 29 | 58.0 |
| 14 year | 3 | 12.0 | 7 | 28.0 | 10 | 20.0 |
| 15 year | 5 | 20.0 | 2 | 8.0 | 7 | 14.0 |
| IMT | ||||||
| Thin | 1 | 4.0 | 1 | 4.0 | 2 | 4.0 |
| Normal | 9 | 36.0 | 14 | 56.0 | 23 | 46.0 |
| Fatty | 14 | 56.0 | 10 | 40.0 | 24 | 48.0 |
| Obesity | 1 | 4.0 | 0 | 0 | 1 | 2.0 |
| Menstrual cycle length | ||||||
| 28 days | 8 | 32.0 | 4 | 16.0 | 12 | 24.0 |
| 29 days | 5 | 20.0 | 7 | 28.0 | 12 | 24.0 |
| 30 days | 5 | 20.0 | 6 | 24.0 | 11 | 22.0 |
| 31 days | 2 | 8.0 | 2 | 8.0 | 4 | 8.0 |
| 32 days | 5 | 20.0 | 6 | 24.0 | 11 | 22.0 |
| Length of menstruation | ||||||
| 3–7 days | 14 | 56.0 | 10 | 40.0 | 24 | 48.0 |
| >7 hari | 11 | 44.0 | 15 | 60.0 | 26 | 52.0 |
| The amount of menstrual blood loss | ||||||
| <3×/day | 0 | 0 | 0 | 0 | 0 | 0 |
| 3–5×/day | 23 | 92.0 | 23 | 92.0 | 46 | 92.0 |
| >5×/day | 2 | 8.0 | 2 | 8.0 | 4 | 8.0 |
| Total | 25 | 100.0 | 25 | 100.0 | 50 | 100.0 |
The Mann–Whitney U test.
On the body mass index of respondents who have the most PMS in overweight BMI, namely 14 people (56%) and the lowest is 1 person (4%) while those who were not PMS mostly normal, 14 people (56%) and none are obese, 0 people (0%). For respondents whose length cycle was carried out on PMS, respondents were 28 days as many as 8 people (32%) and the day cycle was 2 people (8%). The respondent who were not PMS with a cycle of 29 days were 7 people (28%) while in the 31-day cycle there were 2 people (8%). For volunteers who came from STD respondents, there were at most 3–7 days as many as 14 people (56%) and >7 days as many as 11 people (44%), for those who did not have PMS consisting of menstruation >7 days as many as 15 people (60%) and 10 respondents with a menstrual duration of 3–7 days (40%). For PMS respondents with a blood count of 3–5 sanitary napkins per day, 23 people (92%) and 0 blood counts < 3 sanitary napkins or none had a blood count < 3 days, while 23 people without PMS (92%) who have a blood count of 3–5 pads per day and 0 (0%) people who have a menstrual blood count <3 sanitary napkins.
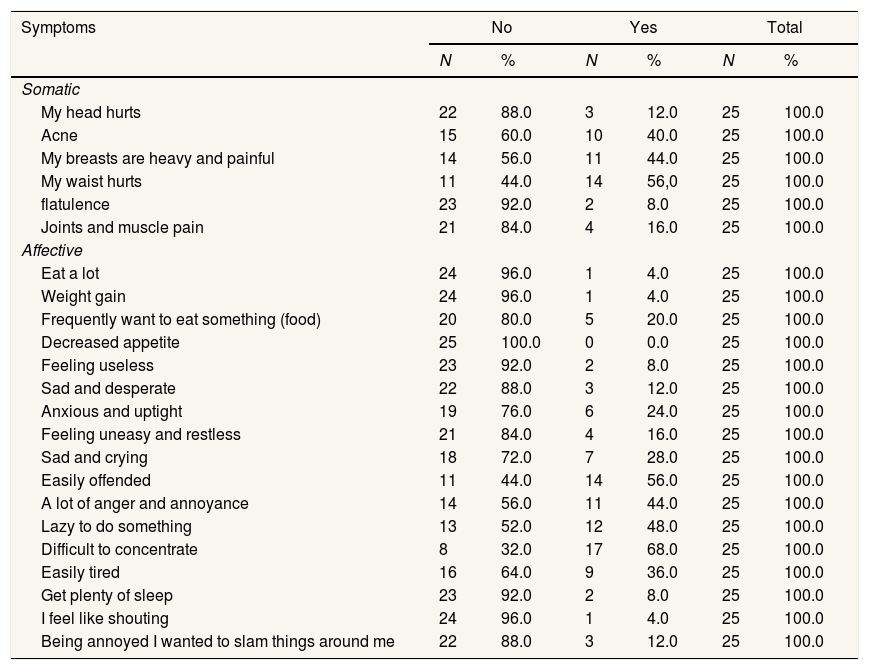
From Table 2, it was illustrated that 25 respondents based on the symptom group the most experienced affective symptoms were 17 people (68%) difficult to concentrate, while the most experienced somatic symptoms were the waist pain as many as 14 people (56.0%) and from affective symptoms, namely decreased appetite, none of the respondents experienced these symptoms and for somatic symptoms 1 respondent (4.0%) experienced symptoms of weight gain.
The distribution of respondents based on symptoms experienced by adolescents with PMS at Darul Arqam Islamic Boarding School in Makassar Year 2018.
| Symptoms | No | Yes | Total | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Somatic | ||||||
| My head hurts | 22 | 88.0 | 3 | 12.0 | 25 | 100.0 |
| Acne | 15 | 60.0 | 10 | 40.0 | 25 | 100.0 |
| My breasts are heavy and painful | 14 | 56.0 | 11 | 44.0 | 25 | 100.0 |
| My waist hurts | 11 | 44.0 | 14 | 56,0 | 25 | 100.0 |
| flatulence | 23 | 92.0 | 2 | 8.0 | 25 | 100.0 |
| Joints and muscle pain | 21 | 84.0 | 4 | 16.0 | 25 | 100.0 |
| Affective | ||||||
| Eat a lot | 24 | 96.0 | 1 | 4.0 | 25 | 100.0 |
| Weight gain | 24 | 96.0 | 1 | 4.0 | 25 | 100.0 |
| Frequently want to eat something (food) | 20 | 80.0 | 5 | 20.0 | 25 | 100.0 |
| Decreased appetite | 25 | 100.0 | 0 | 0.0 | 25 | 100.0 |
| Feeling useless | 23 | 92.0 | 2 | 8.0 | 25 | 100.0 |
| Sad and desperate | 22 | 88.0 | 3 | 12.0 | 25 | 100.0 |
| Anxious and uptight | 19 | 76.0 | 6 | 24.0 | 25 | 100.0 |
| Feeling uneasy and restless | 21 | 84.0 | 4 | 16.0 | 25 | 100.0 |
| Sad and crying | 18 | 72.0 | 7 | 28.0 | 25 | 100.0 |
| Easily offended | 11 | 44.0 | 14 | 56.0 | 25 | 100.0 |
| A lot of anger and annoyance | 14 | 56.0 | 11 | 44.0 | 25 | 100.0 |
| Lazy to do something | 13 | 52.0 | 12 | 48.0 | 25 | 100.0 |
| Difficult to concentrate | 8 | 32.0 | 17 | 68.0 | 25 | 100.0 |
| Easily tired | 16 | 64.0 | 9 | 36.0 | 25 | 100.0 |
| Get plenty of sleep | 23 | 92.0 | 2 | 8.0 | 25 | 100.0 |
| I feel like shouting | 24 | 96.0 | 1 | 4.0 | 25 | 100.0 |
| Being annoyed I wanted to slam things around me | 22 | 88.0 | 3 | 12.0 | 25 | 100.0 |
The Mann–Whitney U test.
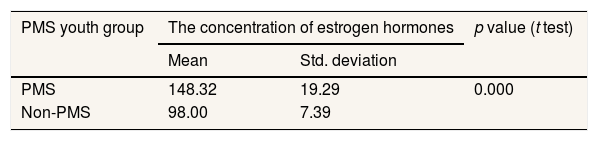
From Table 3, it is found that of the 50 respondents, 25 who are PMS and 25 who are not PMS, the average value of respondents who have estrogen levels is that the respondents with PMS the average estrogen value is 148.32pg/ml higher than those who are not PMS amounting to 98.00pg/ml. After checking the concentration of estrogen and the data processed using Mann–Whitney U, it was found that Ha was accepted and Ho was rejected, where the mean value of PMS adolescents was higher than those without PMS with p=0.000<α=0.05. This means that there is a significant difference in the increase in estrogen for people with PMS and those who do not have PMS.
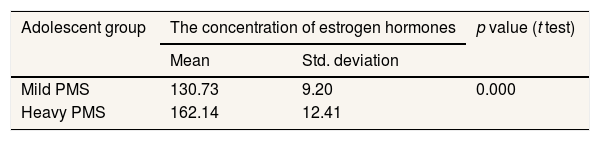
From Table 4, it is established that the average value of estrogen with mild PMS is 130.72pg/ml and those who experience severe PMS, the average value of estrogen is 162.14pg/ml, p=0.000<α=0.05, this means that there is a significant difference in the mean value between no PMS, mild PMS, and severe PMS.
The analysis of differences in average levels of estrogen in adolescents with mild PMS and severe PMS in Darul Arqam Islamic Boarding School Makassar.
| Adolescent group | The concentration of estrogen hormones | p value (t test) | |
|---|---|---|---|
| Mean | Std. deviation | ||
| Mild PMS | 130.73 | 9.20 | 0.000 |
| Heavy PMS | 162.14 | 12.41 | |
The Mann–Whitney U test.
The results of this study illustrate that there are differences in age levels. The PMS group who became respondents were from the age of 15, 16 years and 17 years, as well as the group that was not PMS. In the 17 year age group the most experienced PMS was 19 people (76.0%). Adolescence is a period of transitional development between childhood and adulthood which includes changes in the biological, cognitive, socio-emotional, adolescent age range 12–21 years.
Referring to the results of the study, 15 girls who experienced PMS experienced menarche at the age of 13 years (15%) where menarche was a sign of sexual organ maturity which was marked by the arrival of their first menstruation.6 From the results of research on the number of adolescent girls who experience PMS with overweight BMI as many as 14 people (56.0%) the more distribution of fat in the body causes fat levels which are a source of estrogen production which is the cause of PMS. The length of the menstrual cycle was 28 days in young women who experienced PMS as many as 8 people (32%), the length of menstruation was 3–7 days for 14 people with PMS while the characteristics of the number of menstrual blood 3–5 pads/day were 23 people (92%) and the length of menstruation for 8–10 days among young women with PMS was 15 people (60%).
Based on the results of research conducted on young women experiencing PMS as many as 17 people (68%) apperceived difficulty concentrating, this was an effective symptom, while the most somatic symptoms were a pain in the waist as many as 14 people (56%). Premenstrual syndrome (PMS) is a complaint that usually starts one week to several days before the onset of menstruation, and disappears after menstruation comes, although sometimes it continues until menstruation stops. Premenstrual syndrome (PMS) is a complaint that feels like; anxiety, depression, unstable mood, fatigue, weight gain, swelling, breast pain, spasms, and back pain that can occur about 7–10 days before the onset of menstruation and peaks at the time menstruation occurs.3 PMS is a collection of physical, psychological, and emotional symptoms associated with a woman's menstrual cycle. About 80–95% of women at childbirth experience premenstrual symptoms that can interfere with several aspects of their lives.7
The results of the study of 50 respondents, where 25 people with an average value of 148.32pg/ml who experienced PMS and 25 people with an average value of 98.00pg/ml who did not experience PMS, after examining their estrogen hormone levels and the data processed by Mann-Whitney U, it is found that the mean value of PMS adolescents is greater than those who are not PMS with a value of p=0.000<α=0.05. This means that there is a significant difference in the average level of estrogen in adolescent girls who experience PMS and do not experience PMS.
In women who experience premenstrual syndrome, there is an imbalance of the hormones estrogen and progesterone, where estrogen levels increase, resulting in a decrease8 serotonin synthesis which affects mood and behavior changes. This decrease in serotonin synthesis is emotional symptoms that affect his appetite. The influence of appetite will have an impact on their eating behavior.2
Excess estrogen can increase prolactin, which can cause breast pain and increase aldosterone which contributes to increased sodium levels and water retention which results in breast tension. In one study 63% of women had a 25% increase in the number of inflammatory or acne lesions associated with the premenstrual disease. Hormonal changes can cause the sebaceous glands to produce more sebum. This oily substance can clog pores and cause acne lesions. Women who experience PMS have high levels of leptin during the menstrual cycle. They tend to eat foods that are high in fat, high in sugar, and low in protein. Changes in neurotransmitters and their interactions with hormones can lead to overweight and obesity.9
Changes in levels of the hormone estrogen affect the centrally acting neurotransmitter, serotonin. Lack of serotonergic neurotransmission results in depressed mood, irritability, aggression, poor implant control. An increase in the ratio of estrogen and progesterone is associated with a decrease in endorphins in the brain, causing changes in mood.8
The corpus luteum will regress if pregnancy does not occur. This will result in a decrease in progesterone levels and result in lysosomal membrane labilization so that it is easily split and releases the enzyme A2 phospholipase. Phospholipase A2 will hydrolyze the phospholipid compounds present in the endometrial cell membrane and produce arachidonic acid. Arachidonic acid together with endometrial damage will stimulate the arachidonic acid cascade and produce prostaglandins PGE2 and PGF2 alpha. Women with primary dysmenorrhoea have elevated blood levels of PGE and PGF2 alpha, which stimulate the myometrium. As a result, there is an increase in uterine contractions and dysrhythmias, resulting in decreased blood flow to the uterus and resulting in ischemia. Prostaglandins cause sensitization, further decreasing the pain threshold at the pelvic afferent nerve endings against physical and chemical stimuli.10
The theory suggests that the cause of PMS is the result of excess estrogen, pyridoxine deficiency, and changes in glucose metabolism and electrolyte imbalance. However, recent research suggests that PMS is greatly affected by sex hormones, including metabolites and their interactions with the neurotransmitter and neurohormonal systems such as serotonin, GABA, cholecystokinin, and aldosterone renin-angiotensin.11
According to the ACOG, at least 85% of women experience PMS. They experience PMS symptoms ranging from mild, which does not require treatment to more severe than PMS called PMDD (Premenstrual Dysphoric Disorder). PMDD is a condition accompanied by severe emotional and physical problems related to the sexual cycle.12 PMDD is a severe form of PMS and affects about 5% of menstruating women. PMDD is a form of the disorder that is more severe than PMS which affects about 3–8% of reproductive women. PMDD symptoms may differ from cloud to cloud. In the measurement of estrogen and progesterone, there was no difference between PMDD and PMS. The fluctuation of circulating estrogens and progesterone can cause effects on neurotransmitters in the brain, especially the serotonergic, noradrenergic, and dopaminergic pathways.8
These premenstrual symptoms cause them to feel exactly sad, irritable, or depressed. The women even feel out of control, and this affects their relationships with partners, colleagues, children, and friends. This is what is called Premenstrual Dysphoric Disorder (PMDD). PMDD is a condition accompanied by serious emotional and physical problems related to the menstrual cycle. The syndrome occurs after the middle of the menstrual cycle and ends when menstruation begins. PMDD and PMS both have the same symptoms including depression, anxiety, tension, irritability, and irritability, which differ in the degree of severity.13
ConclusionAdolescence is a period of transition from childhood to adulthood. In this transition period, there are so many changes, both physically and psychologically for children. Menstruation is one of the signs that a girl has gone through puberty. Menstruation is a regular discharge of blood that comes from the uterine wall out into the vagina. This indicates that the female reproductive organs have worked. Menstruation is influenced by the interaction of hormones released by the hypothalamus, anterior pituitary, and ovaries. Cycles in women have different cycle variations. During menstruation, women have various kinds of symptoms and menstruation during menstruation. Discomfort or symptoms that can occur can be felt physically and psychologically. Starting from complaints of abdominal pain, breast pain, dizziness, nausea, insomnia, irritability/irritability. This symptom is called premenstrual syndrome (PMS), where these symptoms are mild to severe and require medical treatment.
PMS has a huge impact on student activities and achievement. From research conducted at the Darul Arqam Islamic Boarding School, high-fat levels in the body of young women are a source of estrogen production which causes PMS to be more common in overweight women. During adolescent girls experiencing PMS on average the most symptoms, they will feel are difficulty concentrating, and the most frequent somatic symptom is a pain in the hip area. Estrogen levels in young women who experience PMS are 148.32 and not PMS 98.00pg/ml. PMS occurs due to a hormonal imbalance between estrogen and progesterone, where levels of the hormone estrogen increase, resulting in a decrease in serotonin synthesis which affects mood and behavior. Excess estrogen can increase prolactin which can cause breast pain and increase aldosterone which plays a role in increasing sodium levels and air retention which causes tension in the breasts.
Conflicts of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











