




The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
Más datosCurrently, stunting is seen as a serious public health problem. Although its prevalence has decreased, the stunting rate is a large number of cases in the world.
MethodsA literature search was conducted on electronic databases such as ProQuest, PubMed, ScienceDirect, and Google Scholar to identify relevant published articles from January 1, 2010, to July 1, 2020. Additional articles were identified from the reference lists and grey literature.
ResultThree main phases require the optimal mother roles to prevent stunting in children during the golden phase. These phases include the preconception phase, the prenatal phase, and the infant-toddlerhood phase. Various mother roles include fulfilling maternal, fetal, infant, and child nutrition, carrying out early breastfeeding initiation, exclusive breastfeeding, and appropriate complementary feeding, optimizing the environment for child development, optimizing family support, and avoiding various psychosocial factors that can be detrimental during growth, and child development.
ConclusionThe mother roles in the golden phase are crucial to preventing stunting in children. Although the conception period does not have a fetus, early strengthening of maternal nutrition must be done so that the mother's body is ready to undergo the prenatal phase for fetal development, which then continues in the infant phase - toddlerhood to adolescence.
Stunting is currently seen as a serious health problem in the community as the prevalence of children with stunting is more than 40%. Globally the world's stunting presentation is relatively high at 24%, in which the highest were Papua New Guinea and East Timor (50% each), followed by Pakistan (45%), Mozambique (43%), Zambia (40%), India (39%), Nepal (37%), Indonesia (36%), Myanmar (35%), and United Republic of Tanzania (35%), and based on continental coverage, south Asia ranked highest stunting presentation in the world at 37%, followed by sub-Saharan Africa (36%), eastern and southern Africa (36%), west, and central Africa (35%), and East Asia and Pacific (11%), and the lowest are Latin America, Caribbean, and Russian Federation (10%).1 The global prevalence of stunting in children under five is 141.3 million, and by 2025 WHO predicts that stunting incidence in children under five years old is 128.3 million, and it will decrease to 116.5 million by 2030. 2
Even though it has decreased, this number is still the largest number of cases globally, so efforts to prevent and minimize stunting must still be optimized because this cannot be separated from the short-term and long-term effects of stunting. Short-term consequences are impaired brain development, cognitive development, physical growth disorders, and metabolic disorders in the body. Long-term consequences are decreased cognitive abilities and learning achievement, a low immune system so that children are susceptible to disease, high risk for diabetes, obesity, heart and blood vessel function disorders, cancer, stroke, and disabilities in the old phase.3
These consequences are in line with stunting experienced in infancy and early childhood resulting in long-term harms such as increased morbidity, poor cognition and educational performance in childhood, an increased risk of perinatal death and premature death for women, lower productivity, reduced income in adults and if accompanied by excessive weight gain in childhood, resulting in an increased risk of chronic disease. 4 In other side, The prevalence rates of underweight and overweight among the children were 14.5% and 20.4%, respectively. Underweight was more prevalent in boys. Factors such as mother's level of education, having an underweight father, and playing outdoors on weekends for more than 2h were significantly associated with underweight children. By contrast, mothers with high levels of education, overweight parents, sleeping for less than 9h, and playing outdoors on weekends for less than 1h were significantly associated with overweight children. 5 Other study found that there was a significant relationship between food intake and nutritional status of children under five years. 6
The various roles of mothers are a key factor in preventing stunting. Mother is the only source of nutrition for a developing child during the critical 1000 days period, in the first six months of life when the breastfeeding period is exclusive.7 Mother plays a crucial role in shaping their children's food intake through their food intake and the food they provide for the child.8 Besides, the mother is also the primary person responsible for meal planning and food preparation, so it is evident that the mother's role is vital in fulfilling child nutrition to prevent stunting. 9 The long-term health impacts of malnutrition in childhood show that it is crucial to overcome its beginnings before a critical stage of childhood development is achieved that it is in desperate need of an early maternal role to prevent stunting. 10
However, a comprehensive review of the mother's role in preventing stunting does not yet exist. A review is needed to explore a mother's various roles as a key factor in stunting prevention. Therefore, this study aimed to provide a synthesis of evidence from the exploration of three important phases, called the golden phase, regarding the role of mother in child growth and development to prevent stunting.
MethodsThis study used a systematic review method with a narrative synthesis that discusses the mother's role in preventing stunting. This review is based on PRISMA guidelines on writing a systemic review report. 11 The process used to perform systemic reviews is for reviewers to search for several journal articles published through electronic databases. The electronic databases used include PubMed, ProQuest, ScienceDirect, and Google Scholar with a period of January 1, 2010, to July 1, 2020. The keywords included in the search terms were “stunting,” “role of maternal,” and “prevent stunting.”
The reviewed study selection process consisted of six steps shown in Figure 1, then further excluded, and in the end, the study that had been input will be synthesized. For this study, data extraction tools were designed to guide information from records according to study objectives. The data were extracted from each study that had inclusion criteria: author, year, country, population, and setting, study design, objectives, methods, instruments, and results (Table 1). This systemic review used guidelines to analyze the quality of literature among selected studies. The guideline used were the Critical Appraisal Skills Program tools (CASP) and Quality Assessment to assess the risk of bias from the selected study.12

Grid Synthesis Table.
| Grid synthesis | ||||||
|---|---|---|---|---|---|---|
| No | Author/Year | Country | Population | Types of study | Purpose of the study | Findings |
| 1 | Simanjuntak, Haya, Suryani, Khomsan, & Ahmad (2019) 13 | Indonesia | Mothers of children aged 12–59 months | Quantitative research with a cross-sectional approach | To know the relationship between mothers’ knowledge, attitudes, and traditional feeding practices in children under five with stunting and wasting among farming families in Central Bengkulu Regency. | There is a relationship between knowledge of traditional food nutrition and nutritional status of body weight for age (p-value = 0,031). There is a relationship between traditional food nutrition practices and the incidence of wasting (p-value = 0,012). Nutritional status, according to height index for age, is related to maternal knowledge about traditional food. In contrast, maternal nutrition practice with traditional food has a significant relationship with the weight index. |
| 2 | Stewart, Iannotti, Dewey, Michaelsen, Andy (2013) 14 | - | Nonspecified | Contextual review | To improve the practice of companion feeding or the nutritional quality of companion foods should take into account the contextual and proximal determinants of stunting. | Properly considered transdisciplinary action is required. Programs and policies tend to be concentrated in the middle of the framework on proximal causative factors, through infant and young child feeding (IYCF) directly and at lower rates of infection and other household and family factors. The conditions identified in this context and framework can ultimately be inhibition or support. The challenge identified is nutritionally sensitive development, which lies in designing the approach that best utilizes favorable contextual conditions or creatively avoids obstacles. |
| 3 | Abebe, Haki, & Baye, (2016)15 | Ethiopia | Mothers with at least one child aged 12 to 23 monthsand women's health counselors | Quantitative research with a cross-sectional approach | To evaluate mothers and health educators’ knowledge about key IYCF practices and investigate whether maternal knowledge and knowledge sharing effectiveness (KSE) were associated with stunting in young children (ages 12-23 months). | Stunting (50%), underweight (34%), and wasting (10%) are prevalent. Less than half (45%) of mothers have access to nutritional education through health counseling programs, but those with better knowledge of IYCF practices can lower stunting rates (P <0,001). However, the key practices of IYCF are not well understood by health extension workers (HEW), which affected their KSE. The gap in KSE is negatively associated with length-for-age Z-score (LAZ) (r = −.475, P <.001) and remains significant even after adjusting for maternal height, socioeconomic status, and maternal education (r = −.423, P = .002). |
| 4 | Young et al. (2018)16 | Vietnamese | Preconception Women | Randomized-controlled trial; a prospective cohort | To know the relationship between maternal nutritional status (PMNS) preconception and child growth during the first 1000 days | A third of preconception women have a height of <150cm or weight of <43kg. Women with preconception height <150cm or weight <43kg are at increased risk of having a stunted child at two years of age (IRR event risk ratio: 1.85, 95% CI 1.51–2.28; IRR 1.35, 95% % CI 1.10–1.65, respectively). While the traditional low BMI limit (<18.5kg / m2) is not significant, a lower BMI limit (<17.5kg / m2 or <18.0kg / m2) is significantly associated with a 1.3 times increased risk of stunting child. PMNS affects the linear growth of offspring and the risk of stunting during the first 1000 days. |
| 5 | Martorell & Young, (2012) 17 | India | Children under five years of age and women 15–49 years | Quantitative study | To investigate the causes of stunting and wasting | In Indian children 0–5 months of age, wasting more than tripled, from 8% to 30%, leading to the highest prevalence of losing. Based on the national center for health statistics (NCHS) reference, the lowest and highest stunting prevalence among Indian children occurred in children 0–5 and 12–23 months. Besides, there is a relationship between household wealth and women's condition related to stunting and wasting. Risk factors causing high wasting levels in India include poor female status, “skinny-fat” infant phenotypes, chronic food shortages, low food quality, striking seasonal patterns, and poor sanitation rates. |
| 6 | Nugraha, Fatikhah, Wahyuni, & Saudah (2019)18 | Indonesia | Mothers with toddlers | Correlation analytics with cross-sectional | To analyze the influence of family social support on foster care patterns in preventing stunting | Family social support with a good frequency of 65 respondents (60,7%). Moreover, respondents with sufficient frequency were 67 respondents (62,6%). Linear regression test result with p of 0.00. This figure means a relationship between family social support and foster care patterns in preventing stunting in toddlers. The better the mother's family's social support, the better the toddlers’ parenting pattern to prevent stunting. |
| 7 | Makatita & Djuwita (2020) 19 | Indonesia | Toddlers | Quantitative study with a cross-sectional approach | To assess maternal parenting patterns in toddlers aged 12-36 months with stunting | Maternal parenting pattern is one of the contributing factors to the high prevalence of stunting in toddlers aged 12-36 months in Bogor Regency, Indonesia. Stunting prevention efforts are very important, one of which is based on the mother's parenting factors. Therefore, it is necessary to improve mothers-to-be education, especially young women, and increased knowledge of pregnant women who have low education about parenting patterns in toddlers under aspects of good and correct parenting patterns. |
| 8 | Fawzi, Andrews, Fink, Danaei, Mccoy, Sudfeld, Kaaya, et al., (2019)20 | Asian, American, African | Children 2 years old | A comparative risk assessment | To measure the burden of stunting in childhood in low/middle-income countries caused by psychosocial risk factors and estimates the associated lifetime economic costs. | Psychosocial factors cause approximately 7.2 million cases of stunting in low/middle-income countries. The main risk factor is maternal depression, with 3.2 million cases caused. Maternal depression also showed that the most significant economic losses were $14.5 billion, followed by low maternal education ($10.0 billion) and IPV ($8.5 billion). The combined cost of these risk factors is $29.3 billion per birth group. |
| 9 | Dewey (2016)21 | South Asia | Mothers and children | To discuss the challenges of meeting nutritional needs during the first 1000 days and strategies can increase nutrient intake in the target group. | Some strategies applied, both prenatal and post-natal, can positively impact a child's growth, but the results are mixed, and growth responses are not always observed. There is a risk of not producing the expected impact for nutritional interventions if the target population often experiences an infection, both clinically and subclinically. | |
| 10 | Sumiaty, Pont, & Sundari (2017)22 | Central Sulawesi, Indonesia | Household | Retrospective cohort | To know the effect of maternal factors and breastfeeding patterns on stunting | Stunting risk factors in maternal factors include the mother's height of <150cm, birth distance <3 years and no pregnancy screening and no early breastfeeding initiation. |
| 11 | Bukari et al. (2020) 23 | Tamale Metropolis | Mothers and children | Analytical cross-sectional study design | To assess maternal growth monitoring knowledge and its effect on stunting, wasting, and underweight in children 0-18 months | 87.6% of mothers have a good knowledge of growth monitoring. The prevalence of stunting, underweight, and wasting were 9.4%, 25.9%, and 17.9%, respectively. The bivariate analysis shows that there is no relationship between maternal growth monitoring knowledge with stunting (p=0.781), wasting (p=0.743), and underweight (p=0.529) in children aged 0-18 months in Tamale Metropolis. |
This study is a part of our original study that examine the role of maternal in preventing stunting. The study has been approved by the Ethical Committee for Medicine and Health Research of Hasanuddin University number 493/UN4.6.4.5.31/PP36/2020.
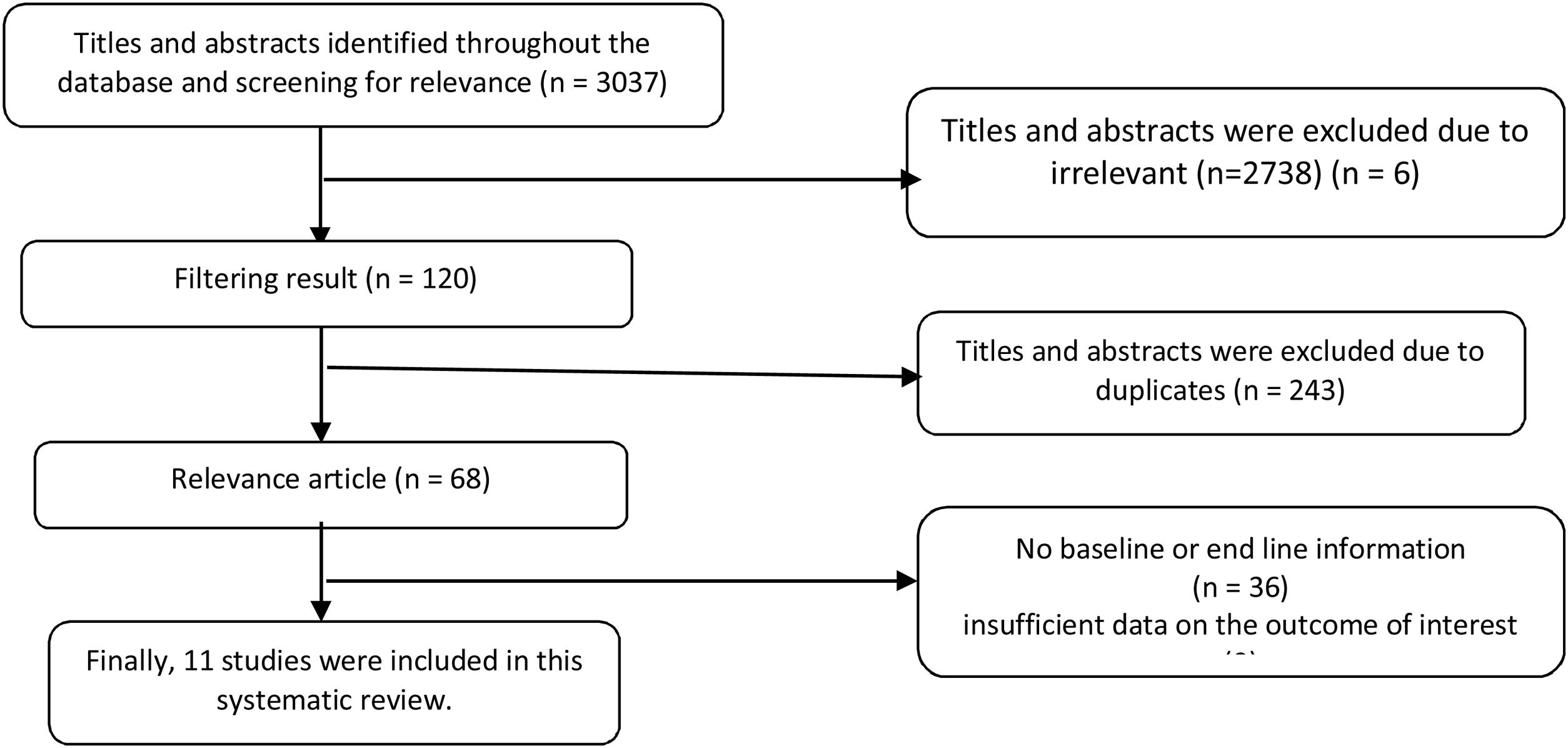
ResultsIdentification and selection of literatureAn initial search that combined all keywords results in 3037 article titles. Titles and abstracts were excluded because they were irrelevant (2738), similar (243), and the full texts were not available. Of the 243 papers filtered and assessed eligibility after removing duplicates (based on the author's name, article title, year of publication, and journal name) and articles that were not related to further papers were identified from the reference list and gray literature by 45. After the removal of untrustworthy studies, 11 papers were included in this review (Figure 2). In this way, the variety of mother's role was identified in the important phase of child growth to prevent stunting.
Description of the included studyThe studies targeted the population of mothers and children under the age of 5. Those studies were conducted in Asia, Africa, and America and analyzed and extrapolated various maternal roles in child growth phases. Some studies did not overall identify mother's roles in the three essential phases of child growth, so reviewers performed synthesis to identify the mother's overall role at each phase.
Based on the study results in the selected article, it is known that three important phases require the mother's role, referred to as the golden phase. In this golden phase, the mother's role is vital in the child's growth to prevent future stunting events.
Preconception phaseThe mother's role during preconceptions varies from optimal nutritional fulfillment to the mother's role. Most mothers with a high level of nutritional knowledge can practice how to provide their food to meet their nutritional needs.13 Periconception conditions, including the mother's nutritional status before pregnancy and the mother's energy and nutritional status intake, affect the initial process of growth and development. 24
In addition to nutrition, other maternal factors play a role in determining the growth of offspring, for which all of these factors are the mother's responsibility.14These maternal factors include infection, pregnancy in adolescence, short birth distance and hypertension during pregnancy and genetics, maternal infections associated with malaria, worms, HIV/AIDS, and other conditions that can cause IUGR and then inhibit growth in infants.25 Teenage pregnancy interferes with the availability of nutrients for fetuses due to maternal growth's constant competition demands. 26Hypertension during pregnancy can also lead to adverse nutritional outcomes for spring. 27
On genetic factors, this can be seen from the mother's early nutritional status reflecting her height in adulthood and the observed relationship between maternal height and hereditary growth and the risk of stunting reflecting the transmission of malnutrition between generations. 28 In addition to nutrition, the mother's genetic factors also connect to the incidence of stunting in the child. The mother's height is an indicator of preconception nutritional status that is most closely related to the child's linear growth. The mother's height is an important indicator that may reflect the combination of the mother's genetics and the nutritional and environmental factors she experienced during her childhood. Therefore, genetic factors and the mother's nutritional status during the first 1000 days are essential for her child's growth. 16 Although genetic factors cannot be changed, strengthening nutrition in children during the growth period can increase the child's growth.
Prenatal phaseThe mother's role in the prenatal phase is vital in preventing stunting events in the child. Maternal nutrition plays a key role in fetal growth, infant health and survival, and long-term child health and development. 29 During the first half of a critical 1000 days period (conception up to 6 months), the mother is the only source of nutrition for a developing child; first in the womb and then during the first six months of life when exclusive breastfeeding is recommended.30
The European Foundation for the care of newborn infants states that the first 1000 days of life, the period between conception and a child's 2nd birthday, are opportunities to support a child's development and long-term health.31
This critical period has a substantial short and long-term impact on the health and well-being of unborn babies, infants, and young children, as well as on pregnant and lactating women.3232 Environmental and nutritional factors for 1000 days can have a positive effect on infant growth, brain development, gastrointestinal tract, metabolism, and immune system. For this reason, a balanced diet with optimal amounts of essential nutrients during the early life period plays a vital role in future programming health so that the child's growth can be optimal and prevent future stunting events.31
The mother is responsible for the fulfillment of fetal nutrition during the prenatal period; critical nutrients that are very important for mothers to pay attention to during the prenatal period are omega-3 fatty acids, iron, iodine, calcium, zinc, magnesium, and vitamins (folic acid/folate, vitaminS A, B6, B12, C, D, E).33 Therefore, the mother's responsibility during the prenatal period lies not only in the fulfillment of optimal nutrition for the fetus but also provides a conducive environment that can increase maternal factors so that the mother is ready for fetal development until the delivery period so that the optimal growing fetus can be spared stunting.
Infant and toddlerhood phase: 6-24 monthsThe role of mothers in toddlerhood ranges from early breastfeeding initiation, exclusive breastfeeding, and providing proper breast milk companion food. This role is essential because inappropriate feeding of infants and young children is one of the leading causes of stunting. 34 Key recommendations for infant and young child feeding practices include the minimum duration of continued breastfeeding, minimum diversity of food, and minimum acceptable food.15Babies who do not initiate early breastfeeding are associated with future stunting events.10 Proper feeding of infants and young children is very much related to the mother's knowledge. Research proves that mothers who have a better knowledge of infant and young child feeding practices can lower stunting incidence (P <0,001).15
Proper companion foods (i.e., solid foods and fluids other than breast milk or formula milk) should begin before the beginning of the 5th month (17 weeks) and not after the beginning of the 7th month (26 weeks) - while continuing to breastfeed as long as the mother and baby desire.35 However, all babies develop at different speeds, so parents should pay attention to signs of development to know when the baby is ready for solid food.31
Stunting caused by chronic malnutrition occurs in about 25% of toddlers. Research roves that the height-for-age index (HAZ) is influenced by nutritional knowledge (p-value=0.031), and maternal nutrition practices are related to the weight-for-age index (WAZ) (p-value=0.012). This finding reinforces the evidence that mother's r is vital in terms of child nutrition fulfillment. It is also supported by evidence that In Indian children aged 0–5 months, wasting more than tripled, from 8% to 30%, leading to the highest prevalence of wasting. 13 Based on the NCHS reference, the lowest and highest stunting prevalence among Indian children occurs in children 0–5 and 12–23 months. Besides, there is a relationship between household wealth and women's conditions associated with stunting and wasting; risk factors causing high wasting rates in India including poor female status, “skinny-fat” infant phenotypes, chronic food shortages, poor food quality, striking seasonal patterns, and poor sanitation levels so that in addition to nutritional factors, it is also important to pay attention to internal and external environmental factors along with family support.36
There is a relationship between family social support and foster care patterns preventing stunting in toddlers (p=0.00). The better the mother's family's social support, the better the toddlers’ parenting pattern to prevent stunting.18 Other evidence also shows that maternal parenting patterns contribute to the high prevalence of stunting in toddlers aged 12-36 months in Bogor Regency, Indonesia so stunting prevention efforts are very important is based on the maternal parenting pattern factor.19
In addition to parenting and social/family support patterns, psychotic factors should also be considered to prevent stunting. Results. Psychosocial factors cause approximately 7.2 million cases of stunting in low/middle-income countries. The main risk factor is maternal depression, with 3.2 million cases caused. Maternal depression also showed that the most significant economic losses were $14.5 billion, followed by low maternal education ($10.0 billion) and IPV ($8.5 billion). The combined cost of these risk factors is $29.3 billion per birth group.
Based on this, it is known that the role of mothers in infancy and toddlerhood includes strengthening nutrition through exclusive breastfeeding, quality breast milk companion food for infants as well as quality food in the child and also paying attention to the environment and family support for optimization of child growth and development to prevent stunting events.
DiscussionThe mother's role in child development is vital, starting from the preconception phase, prenatal phase, and baby-toddler phase. This role is important because failure to grow up can affect the life of the baby in adulthood. Besides, nutritional status is a factor in the child's development that is influenced by eating habits.13 Healthy eating habits are mandatory for children who need to grow up and address acute dietary problems in children.37 In a cohorts study examining five prospective birth groups (Brazil, Guatemala, India, the Philippines, and South Africa), short women (<150.1cm) were three times more likely to have dwarf children26 by the age of 2.16
Optimization of the mother's role can be realized from strengthening aspects of maternal knowledge and skills. This aspect is strengthened by a study that proves that the attitude score and understanding of the mother's diet is positively related to the diet scores of toddlers38 and mothers with good nutritional knowledge prefer to prepare food for their family in comparison to buying finished foods that cannot be certain of their nutritional content and hygiene.13 This contributes significantly to efforts to prevent stunting in children through optimal nutritional fulfillment. This effort is in line with what is stated, many mothers who have higher levels of nutritional practice have average-weight children.38
The pattern of foster care is also a contributor to stunting events in children.18,19 Therefore, it is necessary to improve education for mothers-to-be, especially young women, and increased knowledge of pregnant women who have low education about parenting patterns in toddlers following aspects of good and correct parenting patterns.19 The quality of baby growth at critical times is influenced both by genetic and environmental factors. One environmental factor is the role of the mother, who optimizes the innate potential of a child through care giving and stimulation, the effectiveness of mother empowerment in the care of babies through the provision of health education with a modeling approach showed an increase in baby anthropometric status.33. Mother's level of education was significantly associated with underweight children.8 For that reason, it is necessary to increase knowledge about positive parenting patterns for toddlers targeted by pregnant women through regular socialization conducted with village midwives and community health cadres. This effort is expected to improve the optimal parenting pattern in toddlers from before birth to later life, not to experience stunting.19
Strengthening the economic aspect must also be done, which is the mother and the family's responsibility. Research in India shows that children from low-income groups have high levels of difficulty buying food. This finding suggests that poverty is not the only contributing factor to malnutrition, but lack of food intake, poor hygienic habits, and low environmental and educational levels can also contribute to child malnutrition in low-income groups. 27 However, optimizing the local food which is more accessible and cheaper as local-food based complementary could be affordable for family.39
Some strategies applied, both prenatal and post-natal, can positively impact a child's growth, but the results are mixed, and growth responses are not always observed. There is no risk of producing the expected impact on nutritional interventions if the target population is frequently infected clinically and subclinically.21 The role of health workers to degrade and prevent stunting is also needed, growing evidence that improving the accessibility and quality of nutritional education through health services can improve maternal knowledge and child food intake, both of which can lower the prevalence of stunting. 40
ConclusionThe mother's important role in preventing stunting in the child lies in three phases: the preconception phase, prenatal phase, and baby phase – toddlerhood. The mother's role in these three phases becomes a key factor in preventing stunting events in the child. Although the conception period is not yet a fetus, maternal nutrition's early strengthening must be done. The mother's body is ready in the prenatal phase for fetal development, continuing in the baby phase – toddlerhood until adolescence.
RecommendationConsidering the mother's role as a key factor in the effort to combat stunting, it is vital to be involved in health workers and family support to empower mothers in strengthening aspects of knowledge and skills in self-management to prepare for pregnancy and child development.
Conflicts of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











