



The initial high level of compliance with the Chilean comprehensive national smoke-free law in 2013 is fading, particularly in the hospitality sector. This paper draws attention to how using a simple and low-cost surveillance inquiry may help focus on the use of scarce inspection resources to improve compliance with the law in the hospitality sector. We conducted a cross-sectional assessment of second-hand smoke exposure in night entertainment venues in Santiago, Chile, by measuring particulate matter of less than 2.5μm (PM2.5). Smoking where prohibited by law was observed in 36% of the venues visited. Venues where smoking was spotted at the time of the observation had a median PM2.5 concentration 13 times higher than background concentration on the street. The study shows that a targeted approach for inspection to find pockets of venues with suboptimal compliance is feasible and affordable.
El alto nivel inicial de cumplimiento de la Ley integral chilena de ambientes libres de humo de 2013 se está desvaneciendo, particularmente en el sector de la restauración. Este documento muestra cómo una encuesta de vigilancia simple y económica puede ayudar a mejorar el uso de recursos de inspección escasos para mejorar el cumplimiento de la ley en dicho sector. Se realizó una evaluación transversal de la exposición al humo de tabaco ajeno en locales de entretenimiento nocturno en Santiago, Chile, midiendo el nivel de partículas menores de 2,5μm (PM2.5). En el 36% de los locales visitados se fumaba donde lo prohíbe la ley. Los locales en los que se fumaba tenían una concentración mediana de PM2.5 13 veces mayor que la concentración en la calle. El estudio muestra que una vigilancia enfocada en la inspección de lugares con cumplimiento subóptimo es factible y asequible.
A national comprehensive smoke-free legislation came into force in Chile in 2013.1 It banned smoking in all enclosed and semi-enclosed areas of all workplaces and public places, including the hospitality sector.
The enforcement efforts during the year following the entry into force of the current smoke-free legislation led to a high compliance with the law, overall and in the hospitality sector,2 which was associated with a sudden and significant decline of myocardial infarction in 2014.3 These efforts included a surge of inspections in 17,406 of the approximately 40,000 existing venues in the hospitality sector in the country.4
Presently enforcement efforts in Chile are fading. By 2016, last year for which governmental enforcement information is available, smoke-free law inspections in hospitality venues were cut in half (8196) while the number of annual public health control activities was in that year similar to that of 2013.4 Moreover, the WHO reported that, compared to 2014, the compliance with the smoke-free law in the hospitality sector in 2018 remained substantial but had declined.5 These data raise questions about how enforcement of the Chilean smoke-free law can be improved. This paper draws attention to how using a simple and low-cost surveillance inquiry may help focus the use of scarce inspection resources to improve compliance with the law in the hospitality sector.
ApproachWe suspected that there remained significant pockets of noncompliant places in the hospitality sector, where venues are expected to be less compliant, based on previous international evidence.6 Within the hospitality sector, we assumed that the venues most likely to be non-compliant would be those catering to young adults and operating outside regular office hours in which inspectors are much less likely to conduct routine inspections.
We conducted a cross-sectional exposure assessment of night entertainment venues in two well-known areas of concentration of this commercial activity in the Greater Santiago, Chile, in November 2018. Eligible venues were establishments making their revenue mostly from the sale of beverages, including alcoholic drinks, although customers may also consume small dishes and appetizers. Venues included bars, pubs, cabarets, night-clubs, and discos, opened at least between 00:00 and 3:00 on Fridays, Saturdays, and Sundays.
To identify potential participating venues, a sampling frame of establishments was constructed, based on information provided by students of our university or available on the internet. We listed a total of 128 potential venues, of which we selected randomly 30. In each selected venue, we measured levels of respirable particles ≤2.5μm in diameter (PM2.5), a well-established marker of tobacco smoke.7 We used three TSI SidePak AM510 Personal Aerosol Monitors, hand-held optical instruments that monitor particle size and mass concentration in real-time. They were set to a one-second sampling interval. The three monitors were previously calibrated in an experiment with a gravimetric BAM-1020 instrument that measures and records airborne particulate concentration levels using the principle of beta-ray attenuation. The calibration factors derived from the experiments were 0.37, 0.39, and 0.39 for each of the monitors.
Six trained observers entered incognito each venue in pairs and sampled the air for at least 30minutes, moving discreetly around the public areas of the establishment, avoiding getting too close to active sources of particulate matter, such as people actively smoking or kitchen entrances if there were any. Observers recorded if there was any tobacco smoking at the time of the visit. The total number of smokers could not be recorded, given that many venues were very dimly lighted, and not all areas of the venues could be visited without being noticed or causing security concerns. Only the data from 25 of the 30 selected venues are reported because the data from four venues were not logged-in appropriately, and the data from one was discarded since the air was contaminated with stage fog, which raised the level of particulate matter spuriously. The air from streets surrounding each of the venues was also sampled concurrently for about 20minutes to set the background PM2.5 concentration for comparison purposes.
We used boxplots to describe medians (M) and interquartile ranges (IQR) of PM2.5 concentration (μg/m3) in the venues, overall and stratified by selected characteristics. We compared median PM2.5 concentration by these characteristics and with background levels using non-parametric Kruskall-Wallis and U-Mann Whitney tests, at a 5% significance level.
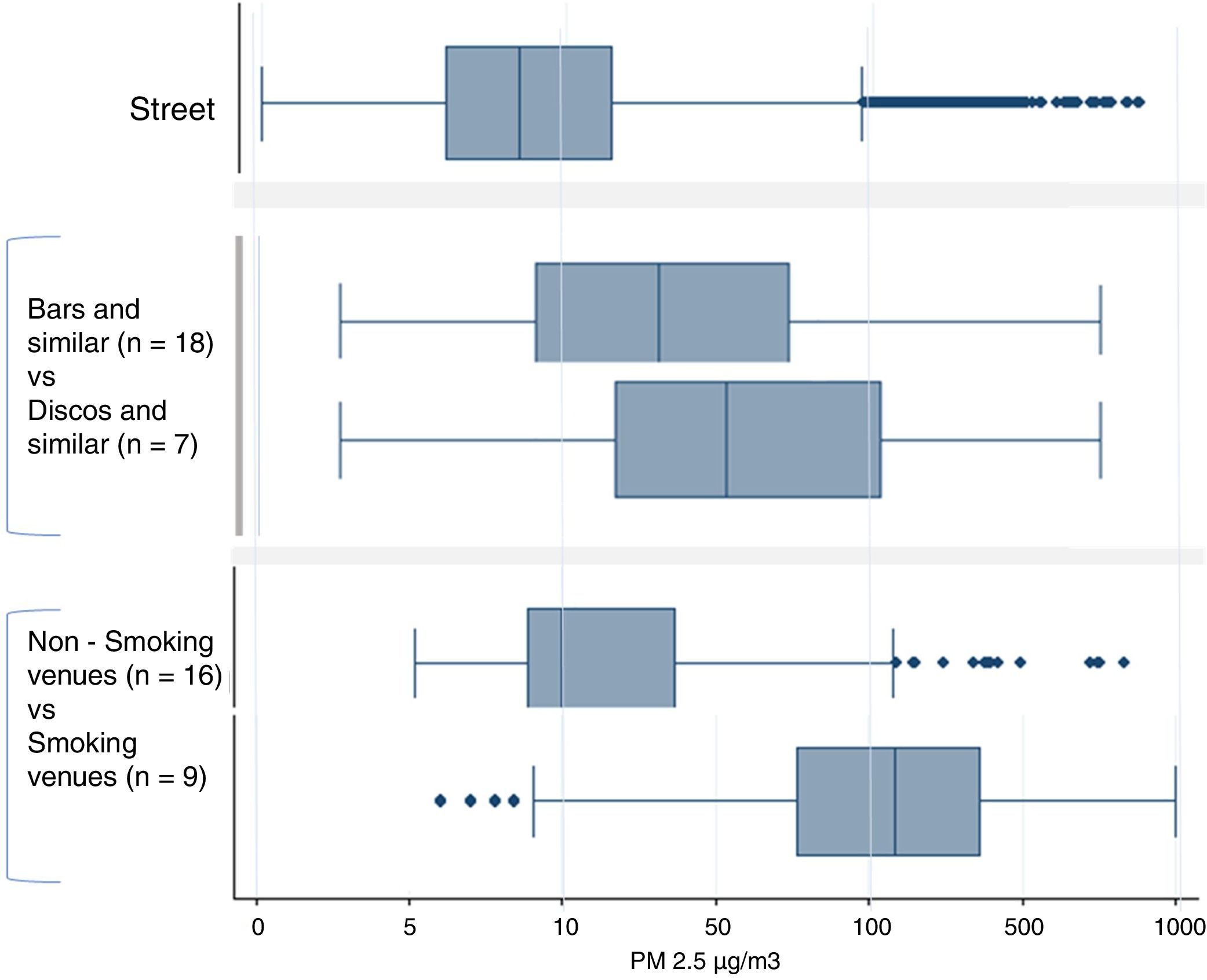
ResultsSmoking where prohibited by law was observed in 36% of the venues visited. Figure 1 presents the boxplots of PM2.5 concentration separately for venues where smoking was and was not observed, by type of venue (bars, pubs, and cabarets vs. discos and nightclubs) and on the street, which served as a reference benchmark. The median PM2.5 concentration on the street was 9μg/m3 (IQR: 5-22μg/m3). In non-smoking venues (those where smoking was not spotted at the time of the observation), the median PM2.5 concentration (M=13μg/m3; IQR: 7-26μg/m3) was 1.4 times higher than on the street. In smoking venues (those where smoking was witnessed at the time of the observation), the median PM2.5 was more than 13 times higher (M=122μg/m3; IQR: 58-230μg/m3) than on the street. Differences between median PM2.5 concentration in smoking and non-smoking venues were statistically significant.

We also compared the median PM2.5 concentration in venues where dancing is their signature activity, such as discotheques and nightclubs, with that in the rest of venues. Compared to the street, the median value of PM2.5 was three times higher in bars and similar venues (m=27μg/m3; IQR: 10-78μg/m3) and more than five times higher in disco and night club venues (m=47μg/m3; IQR: 19-165μg/m3) (all p values <0.001).
DiscussionChile introduced a comprehensive smoke-free law when the smoking prevalence was still high (>35%) compared to when other countries introduced similar national or subnational laws that were almost self-enforcing. Countries with higher smoking prevalence, although having reasonable overall compliance with smoking bans, tend to have more compliance issues8 in some sectors or pockets of venues, particularly in the hospitality sector. Hence the importance of an effective enforcement infrastructure and effort.
The results of our approach show that finding pockets of venues with suboptimal compliance is possible. In the case of Chile, we were able to point out the night entertainment venues not only as a type of business with a significant proportion of noncompliant venues (36%), but also with harmful levels of PM2.5, 13 times above the background street levels. WHO Air Quality Guidelines consider that long-term breathing of air with PM2.5 concentration above 10μg/m3 (annual outdoor average) significantly increases the mortality of exposed persons.9
The same approach can be followed to find additional pockets of non-compliance. For example, anecdotal evidence points to the need for finding such pockets in higher education institutions and small-size workplaces, or among specific administrative subnational jurisdictions.
Until now, a massive effort to inspect all types of venues in the hospitality sector has had limited results in decreasing the self-reported proportion of exposure to second-hand smoke at workplaces.10 However, this study shows that a simple and affordable approach —the cost of this study, personnel expenses, and entry fees to venues, was approximately USD 700— targeting clusters of venues at high risk for violation of the smoke-free law may improve the use of scarce local inspection time and resources.
Editor in chargeCarlos Álvarez Dardet.
Authorship contributionsA. Peruga: conceptualization, investigation, formal analysis, and writing original draft preparation. M. Fu: methodology, resources, and writing, reviewing and editing. X. Molina: conceptualization, investigation, data curation, and writing, reviewing and editing. E. Fernández: methodology, resources, and writing, reviewing and editing.
FundingWHO, the University del Desarrollo, and the Catalan Institute of Oncology-WHO Collaborating Center for Tobacco Control all contributed with funds. The Tobacco Control Research Group (AP, MF, EF) is partially supported by the Ministry of Universities and Research, Government of Catalonia (2017SGR319), and EF is partially supported by the Instituto de Salud Carlos III, Government of Spain (INT16/00211 and INT17/00103), co-funded by the European Regional Development Fund (FEDER). The authors did not enter into an agreement with any of the funders that may have limited their ability to complete the research as planned. The authors had full control of all primary data.
Conflicts of interestNone.











