



To analyse perceived visual health and health services use in a rural population in relation to socioeconomic characteristics and compared with the general population in Spain.
MethodCross-sectional study in a rural population using a structured questionnaire including questions comparable to the Spanish National Health Survey (2012). A descriptive analysis was carried out through the calculation of frequencies and prevalence, the χ2 test for independent variables, contrasts of proportions and logistic regression to obtain associations between the rural and general populations and socioeconomic variables.
ResultsFor the rural population studied, the prevalence of poor perceptions of visual health is 40.8% in men and 39.4% in women, and is strongly associated with age, employment situation, income and presence of chronic diseases (p ¿0.001). Compared with the general population, the rural population has a higher risk of presenting with serious difficulties related to farsightedness (OR: 2.56; 95% CI: 1.32-4.95) and make less use of optical correction (OR: 0.57; 95%CI: 0.44-0.74). The use of health services is not sufficient for adequate prevention, particularly in diabetics. For those affected by poor vision, the distance to travel to receive an eye exam, the belief that eyesight problems come with age and the cost of glasses are the principal reasons used to explain why eyesight problems are not resolved.
ConclusionsThe rural population presents worse visual health that is influenced by social and economic factors. Improving accessibility and reducing barriers is essential to tackle avoidable visual disability and reduce health inequities.
Analizar la salud visual y el uso de servicios de salud en una población rural periférica en relación a variables socioeconómicas y a la población general española.
MétodosEstudio transversal en población rural con administración de cuestionario estructurado incluyendo preguntas comparables a la Encuesta Nacional de Salud en España (2012). Se realizó un análisis descriptivo a través del cálculo de frecuencias y prevalencias, el uso de la prueba χ2 para la independencia de variables y el contraste de proporciones y regresión logística para obtener asociaciones entre variables en población rural y general.
ResultadosEn la población rural estudiada, la prevalencia de mala salud visual percibida es del 40,8% en los hombres y del 39,4% en las mujeres, y está fuertemente asociada a la edad, la situación laboral, el nivel de ingresos y la presencia de enfermedades crónicas (p ¿0,001). Presentan mayor riesgo de afrontar importantes dificultades en visión lejana (odds ratio [OR]: 2,56; intervalo de confianza del 95% [IC95%]: 1,32-4,95) y hacen un menor uso de corrección óptica (OR: 0,57; IC95%: 0.44-0.74) en comparación con la población general. El uso de los servicios de salud es insuficiente para una adecuada prevención, particularmente en las personas diabéticas. Aquellos/as con dificultades visuales señalaron la distancia al centro de salud, asociarlo a la edad y el precio de las gafas como principales barreras en el acceso a una solución.
ConclusionesLa población rural presenta peores indicadores de salud visual, influenciados por factores socioeconómicos. Se requieren acciones que aborden la discapacidad visual por causas evitables y reducir las inequidades en salud.
Visual disability affects negatively the autonomy and quality of life especially at advanced ages and is associated with worse mental health,1 greater cognitive deterioration2 and a greater risk of falls and injuries.3
Vision may be impaired due to multiple reasons being uncorrected refractive errors the most common cause worldwide. The prevalence of vision impairment and blindness is unequally distributed and strongly associated with socioeconomic factors and health services availability.4 Ageing, gender, socioeconomic status, ethnicity and place of residence are factors that determine inequalities in both visual health and use of eye health services. Prevalence of vision impairment, including blindness, is higher in women.5 Low-income populations and minority ethnic groups have less probability of access to preventive eye care services.6 Live in rural areas has been shown as a risk factor for certain common eye conditions such as cataracts or diabetic retinopathy compared to urban populations.7
During the last decade, the prevalence of visual impairment is growing in Spain and is unequally distributed among groups with an increased risk in lower-income regions.8 National surveys on the prevalence of blindness and visual disability in Spain show that these problems affect more than 900,000 people, of whom 69% are over age 65 and two thirds are women;9 life expectancy may contribute to this gap as in Spain is greater in women than in men, 86.2 years versus 80.4 years.10 Age and diabetes are considered principal risk factors, given the fact that age-related macular degeneration and diabetic retinopathy are the blinding conditions with the greatest increase in recent years.11 In Spain, patients searching medical eye care are referred by their family doctor and the average waiting time to receive specialized consultation is 68 days estimated by the NHS in 2015.12
For Spanish society, visual health is becoming more relevant as a public health concern, with an expected doubling of the population over age 65 by the year 2050, the greatest elderly population in Europe.13
There is a scarcity of research related to visual health status and the use of eye care services, particularly in rural areas. A regional survey carried out in Catalonia showed that the elderly and women with low incomes are particularly vulnerable to perceived poor vision14 and some rural populations have been identified at risk for ocular conditions such as diabetic retinopathy.15
The Spanish National Health Survey16 (NHS) addresses visual health in the population through five unique questions about the use of glasses or contact lenses and the capacity for near sight and far sight. In this study, we aim to analyze perceived visual health and health services use in a peripheral rural population in Madrid in relation to sociodemographic, socioeconomic and health characteristics. We also compared the use of optical correction and eyesight limitations between the rural population and the general population in Spain.
MethodStudy population, sample and data collectionThis study was carried out in the rural municipality of Cenicientos, located at the farthest site of the Southwest Sierra in the province of Madrid, reason for which was selected for the study. Cenicientos has a population of 2,073 inhabitants (50.7% women) and an ageing index −percentage of population over 65 years of age− of 27% compared to 19%, 17% and 18% in the area, province and country respectively.17 At the national level, 7.4% of the total population lives in municipalities with 2000 inhabitants or less and the average ageing index in these populations is 24%, similar to the studied rural municipality.
At the time the study was carried out, the health center with ophthalmological specialty was located 70 kilometers away, connected by frequent public transportation. In Cenicientos, like other municipalities in Spain with a similar number of inhabitants, there are no existing specialized visual health services, nor any ophthalmologist or optometrist office, and the local health center does not include specific resources necessary for the identification of refractive errors or ocular pathologies.18
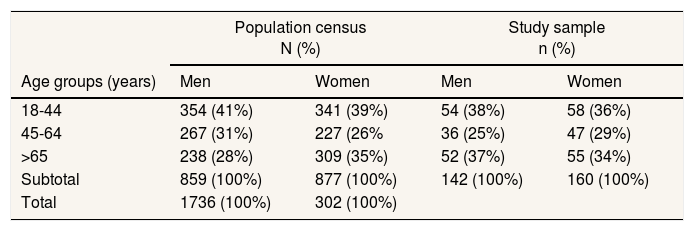
We conducted a cross-sectional study in a stratified random sampling of 302 individuals over age 18, representing 17.4% of the total population censed at rural municipality of Cenicientos (Table 1). The surveys were administered face-to-face in randomly selected households to complete the quotas stablished by age and sex. Data was collected during August of 2013 by local interviewers that received prior training. All of those approached accepted participation, with a response rate of 100%.
Total population and study sample in the rural municipality of Cenicientos.
| Population census N (%) | Study sample n (%) | |||
|---|---|---|---|---|
| Age groups (years) | Men | Women | Men | Women |
| 18-44 | 354 (41%) | 341 (39%) | 54 (38%) | 58 (36%) |
| 45-64 | 267 (31%) | 227 (26% | 36 (25%) | 47 (29%) |
| >65 | 238 (28%) | 309 (35%) | 52 (37%) | 55 (34%) |
| Subtotal | 859 (100%) | 877 (100%) | 142 (100%) | 160 (100%) |
| Total | 1736 (100%) | 302 (100%) | ||
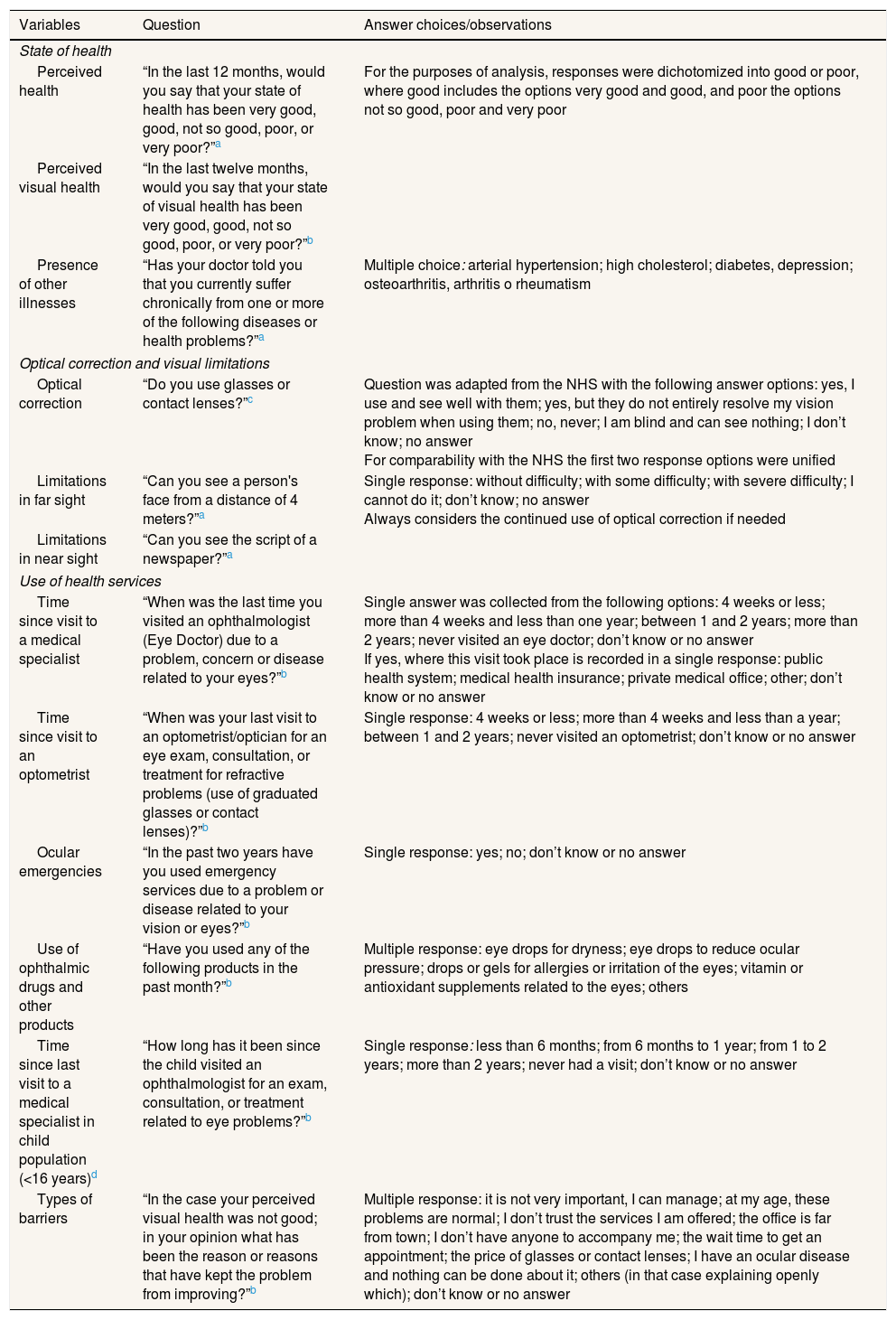
A questionnaire was developed to collect data based on questions comparable to the Spanish NHS (2012). After consulting other regional surveys in Spain19,20, the questionnaire was completed with ad-hoc questions in order to obtain information relevant to the study objectives (Table 2). Information regarding use of eye care services in the child population (<16 years old) was collected through the adults interviewed.
Description of selected questions related to visual health outcomes included in the data collection instrument.
| Variables | Question | Answer choices/observations |
|---|---|---|
| State of health | ||
| Perceived health | “In the last 12 months, would you say that your state of health has been very good, good, not so good, poor, or very poor?”a | For the purposes of analysis, responses were dichotomized into good or poor, where good includes the options very good and good, and poor the options not so good, poor and very poor |
| Perceived visual health | “In the last twelve months, would you say that your state of visual health has been very good, good, not so good, poor, or very poor?”b | |
| Presence of other illnesses | “Has your doctor told you that you currently suffer chronically from one or more of the following diseases or health problems?”a | Multiple choice: arterial hypertension; high cholesterol; diabetes, depression; osteoarthritis, arthritis o rheumatism |
| Optical correction and visual limitations | ||
| Optical correction | “Do you use glasses or contact lenses?”c | Question was adapted from the NHS with the following answer options: yes, I use and see well with them; yes, but they do not entirely resolve my vision problem when using them; no, never; I am blind and can see nothing; I don’t know; no answer For comparability with the NHS the first two response options were unified |
| Limitations in far sight | “Can you see a person's face from a distance of 4 meters?”a | Single response: without difficulty; with some difficulty; with severe difficulty; I cannot do it; don’t know; no answer Always considers the continued use of optical correction if needed |
| Limitations in near sight | “Can you see the script of a newspaper?”a | |
| Use of health services | ||
| Time since visit to a medical specialist | “When was the last time you visited an ophthalmologist (Eye Doctor) due to a problem, concern or disease related to your eyes?”b | Single answer was collected from the following options: 4 weeks or less; more than 4 weeks and less than one year; between 1 and 2 years; more than 2 years; never visited an eye doctor; don’t know or no answer If yes, where this visit took place is recorded in a single response: public health system; medical health insurance; private medical office; other; don’t know or no answer |
| Time since visit to an optometrist | “When was your last visit to an optometrist/optician for an eye exam, consultation, or treatment for refractive problems (use of graduated glasses or contact lenses)?”b | Single response: 4 weeks or less; more than 4 weeks and less than a year; between 1 and 2 years; never visited an optometrist; don’t know or no answer |
| Ocular emergencies | “In the past two years have you used emergency services due to a problem or disease related to your vision or eyes?”b | Single response: yes; no; don’t know or no answer |
| Use of ophthalmic drugs and other products | “Have you used any of the following products in the past month?”b | Multiple response: eye drops for dryness; eye drops to reduce ocular pressure; drops or gels for allergies or irritation of the eyes; vitamin or antioxidant supplements related to the eyes; others |
| Time since last visit to a medical specialist in child population (<16 years)d | “How long has it been since the child visited an ophthalmologist for an exam, consultation, or treatment related to eye problems?”b | Single response: less than 6 months; from 6 months to 1 year; from 1 to 2 years; more than 2 years; never had a visit; don’t know or no answer |
| Types of barriers | “In the case your perceived visual health was not good; in your opinion what has been the reason or reasons that have kept the problem from improving?”b | Multiple response: it is not very important, I can manage; at my age, these problems are normal; I don’t trust the services I am offered; the office is far from town; I don’t have anyone to accompany me; the wait time to get an appointment; the price of glasses or contact lenses; I have an ocular disease and nothing can be done about it; others (in that case explaining openly which); don’t know or no answer |
The questionnaire was applied previously in a pilot sample of 15 people in order to explore applicability and data collection. The study was approved by the Ethics Committee of the University conducting the study and developed in cooperation with authorities of Cenicientos (Madrid) that provided human and logistical resources. All interviewees consented by signature to use anonymous data in this study.
VariablesSeveral outcomes were collected for the categories: state of health and visual health, use of optical correction, visual limitations at far and near sight, use of health services, and perceived barriers to improve visual health including options for multiple response and open answers.
The term visual health was explained to participants as the capacity to see well at any distance without discomfort and without ocular disease. The description of questions and outcomes related to visual health included in the data collection instrument is presented in Table 2.
The sociodemographic and socioeconomic variables collected at the study includes: age (ranges: 18-44, 45-64, <65 years), sex, marital status, education level (no studies/primary, secondary, university), employment situation (employed, self-employed, household, unemployed, student or retired), professional category of the current or last job (NHS 2012 classification later grouped into low, medium and high rank) and income level (combined contributions of all family members per month: less than 800 €, between 800 € and 1550 €, more than 1550 €).
Data analysisThe perceived health and perceived visual health of the rural population over the last 12 months was analyzed by sociodemographic, socioeconomic and health variables for both sexes. The answer options were grouped into good (very good and good) or poor (not so good, poor and very poor).
The prevalence of the use of optical correction and the presence of visual limitations in the studied rural municipality (n=302) was analyzed and compared to the general population in Spain, captured by the last available NHS (n=20,956).16
Given the relationship −established by prior research− between chronic diseases and vision impairment,4 we observed the use of optical correction and presence of visual limitations in individuals with informed diagnosis −given by the general practitioner− of hypertension, cholesterol, diabetes, and depression. For the purposes of the analysis, each health condition was considered separately and individuals with comorbidities were presented in each of the corresponding groups.
We analyzed the use of visual health services in the rural population considering visits to the ophthalmologist, health system use and reason for visit, ocular emergencies and visit to an optometrist. The use of ophthalmic drugs was described in the rural population and analyzed by sex.
A descriptive analysis of the population was carried out through the calculation of frequencies and prevalence. The χ2 test was used to determine whether statistically significant differences (p <0.05) exist among the sociodemographic and socioeconomic variables and perceived health and visual health variables. In order to measure the association between rural and general population, and use of optical correction and visual limitations, odds ratio (OR) and adjusted odds ratio by age (AOR) were calculated in a bivariate analysis with their respective 95% confidence interval which exposure is belonging to the rural population for each age group. The Mantel-Haenszel odds ratio was taken as AOR. Data analysis was performed using statistical packages Excel, SPSS 15.0 and Epidat 3.1.
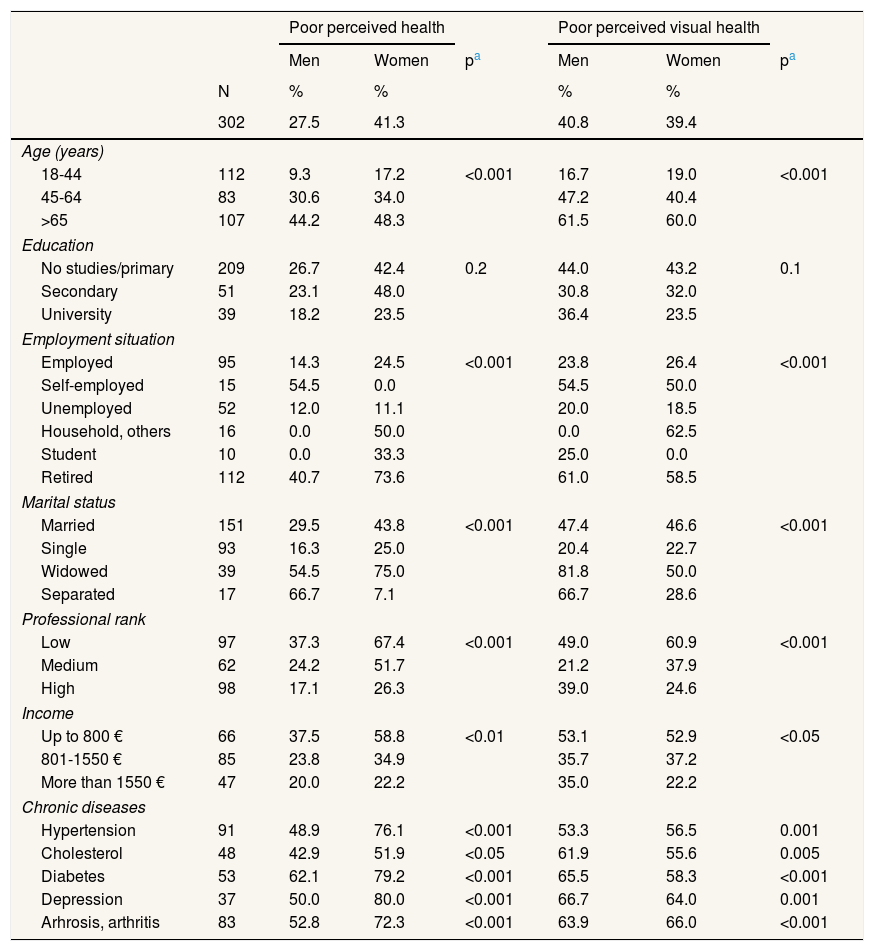
ResultsPerceived health and visual health in the rural population according to social factors and health variablesAs shown in Table 3, the prevalence of poor perceived health in the rural population was 27.5% in men and 41.3% in women, and the prevalence of poor perceived visual health was 40.8% in men and 39.4% in women. Age, marital status, employment situation, professional rank, income level and chronic diseases were associated with perceived health and perceived visual health (p <0.001).
Prevalence of poor perceived health and poor perceived visual health in the last 12 months by age, socioeconomic variables and diagnosed chronic diseases for both sexes of the rural municipality of Cenicientos.
| Poor perceived health | Poor perceived visual health | ||||||
|---|---|---|---|---|---|---|---|
| Men | Women | pa | Men | Women | pa | ||
| N | % | % | % | % | |||
| 302 | 27.5 | 41.3 | 40.8 | 39.4 | |||
| Age (years) | |||||||
| 18-44 | 112 | 9.3 | 17.2 | <0.001 | 16.7 | 19.0 | <0.001 |
| 45-64 | 83 | 30.6 | 34.0 | 47.2 | 40.4 | ||
| >65 | 107 | 44.2 | 48.3 | 61.5 | 60.0 | ||
| Education | |||||||
| No studies/primary | 209 | 26.7 | 42.4 | 0.2 | 44.0 | 43.2 | 0.1 |
| Secondary | 51 | 23.1 | 48.0 | 30.8 | 32.0 | ||
| University | 39 | 18.2 | 23.5 | 36.4 | 23.5 | ||
| Employment situation | |||||||
| Employed | 95 | 14.3 | 24.5 | <0.001 | 23.8 | 26.4 | <0.001 |
| Self-employed | 15 | 54.5 | 0.0 | 54.5 | 50.0 | ||
| Unemployed | 52 | 12.0 | 11.1 | 20.0 | 18.5 | ||
| Household, others | 16 | 0.0 | 50.0 | 0.0 | 62.5 | ||
| Student | 10 | 0.0 | 33.3 | 25.0 | 0.0 | ||
| Retired | 112 | 40.7 | 73.6 | 61.0 | 58.5 | ||
| Marital status | |||||||
| Married | 151 | 29.5 | 43.8 | <0.001 | 47.4 | 46.6 | <0.001 |
| Single | 93 | 16.3 | 25.0 | 20.4 | 22.7 | ||
| Widowed | 39 | 54.5 | 75.0 | 81.8 | 50.0 | ||
| Separated | 17 | 66.7 | 7.1 | 66.7 | 28.6 | ||
| Professional rank | |||||||
| Low | 97 | 37.3 | 67.4 | <0.001 | 49.0 | 60.9 | <0.001 |
| Medium | 62 | 24.2 | 51.7 | 21.2 | 37.9 | ||
| High | 98 | 17.1 | 26.3 | 39.0 | 24.6 | ||
| Income | |||||||
| Up to 800 € | 66 | 37.5 | 58.8 | <0.01 | 53.1 | 52.9 | <0.05 |
| 801-1550 € | 85 | 23.8 | 34.9 | 35.7 | 37.2 | ||
| More than 1550 € | 47 | 20.0 | 22.2 | 35.0 | 22.2 | ||
| Chronic diseases | |||||||
| Hypertension | 91 | 48.9 | 76.1 | <0.001 | 53.3 | 56.5 | 0.001 |
| Cholesterol | 48 | 42.9 | 51.9 | <0.05 | 61.9 | 55.6 | 0.005 |
| Diabetes | 53 | 62.1 | 79.2 | <0.001 | 65.5 | 58.3 | <0.001 |
| Depression | 37 | 50.0 | 80.0 | <0.001 | 66.7 | 64.0 | 0.001 |
| Arhrosis, arthritis | 83 | 52.8 | 72.3 | <0.001 | 63.9 | 66.0 | <0.001 |
The population over 65 years old showed worse visual health, as did those with low education, low-skilled workers, women in the household, retired people living in widowhood and individuals in low-income households. The population with chronic diseases showed high prevalence of poor visual health, particularly those with depression, arthrosis and diabetes (Table 3).
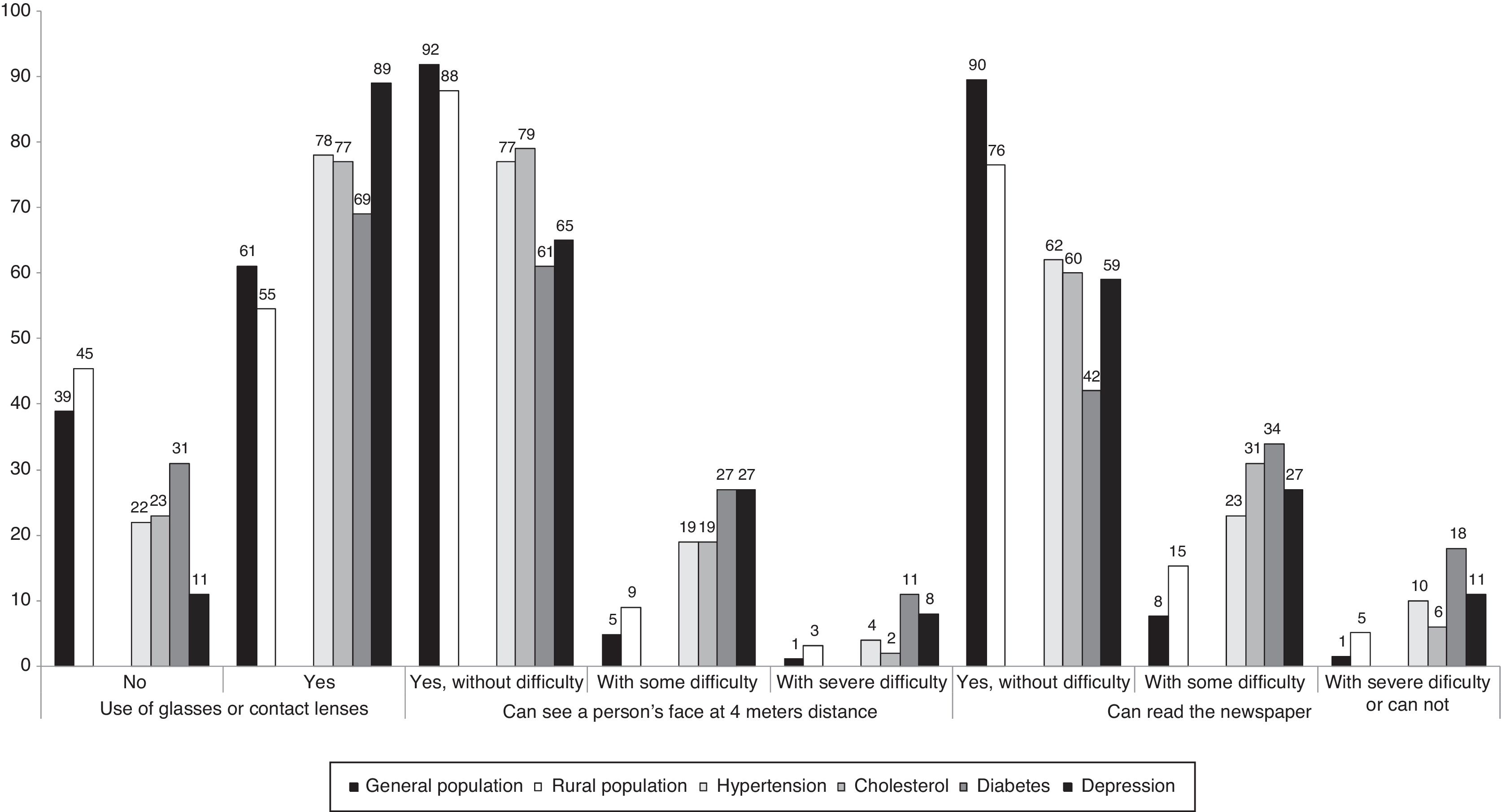
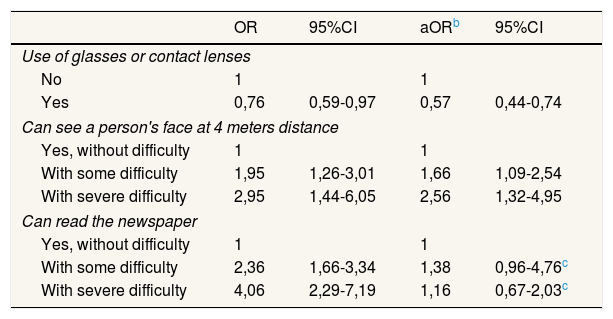
Use of optical correction and visual limitations in the rural and general populationsThe rural population in the studied municipality showed less use of eye glasses or contact lenses compared to the general population in Spain (AOR: 0.57; 95% confidence interval [95%CI]: 0.44-0.74) particularly in men where 54% declare not use these optical aids compared to 35% of women (Table 4). The risk of presenting difficulty in completing far sight tasks is greater among the rural population compared to general population (AOR: 2.56; 95%CI: 1.32-4.95). In both populations, women showed greater difficulty in face recognition at a four-meter distance than men, and this difference was more than double for women in the rural population (13%). Rural population is more likely to present near vision difficulties than general population, although these differences were not statistically significant when adjusted by age (AOR: 1.38; 95%CI: 0,96-4,76). In the rural population, prevalence of diabetics presenting difficulties in near vision was 34%, higher than the average of the municipality (15%), and the general population (8%) (Figure 1).
Use of optical correction and visual limitations in the Spanish general population and in the rural municipalitya.
| OR | 95%CI | aORb | 95%CI | |
|---|---|---|---|---|
| Use of glasses or contact lenses | ||||
| No | 1 | 1 | ||
| Yes | 0,76 | 0,59-0,97 | 0,57 | 0,44-0,74 |
| Can see a person's face at 4 meters distance | ||||
| Yes, without difficulty | 1 | 1 | ||
| With some difficulty | 1,95 | 1,26-3,01 | 1,66 | 1,09-2,54 |
| With severe difficulty | 2,95 | 1,44-6,05 | 2,56 | 1,32-4,95 |
| Can read the newspaper | ||||
| Yes, without difficulty | 1 | 1 | ||
| With some difficulty | 2,36 | 1,66-3,34 | 1,38 | 0,96-4,76c |
| With severe difficulty | 4,06 | 2,29-7,19 | 1,16 | 0,67-2,03c |
95%CI: 95% confidence interval; OR: odds ratio; aOR: adjusted odds ratio.

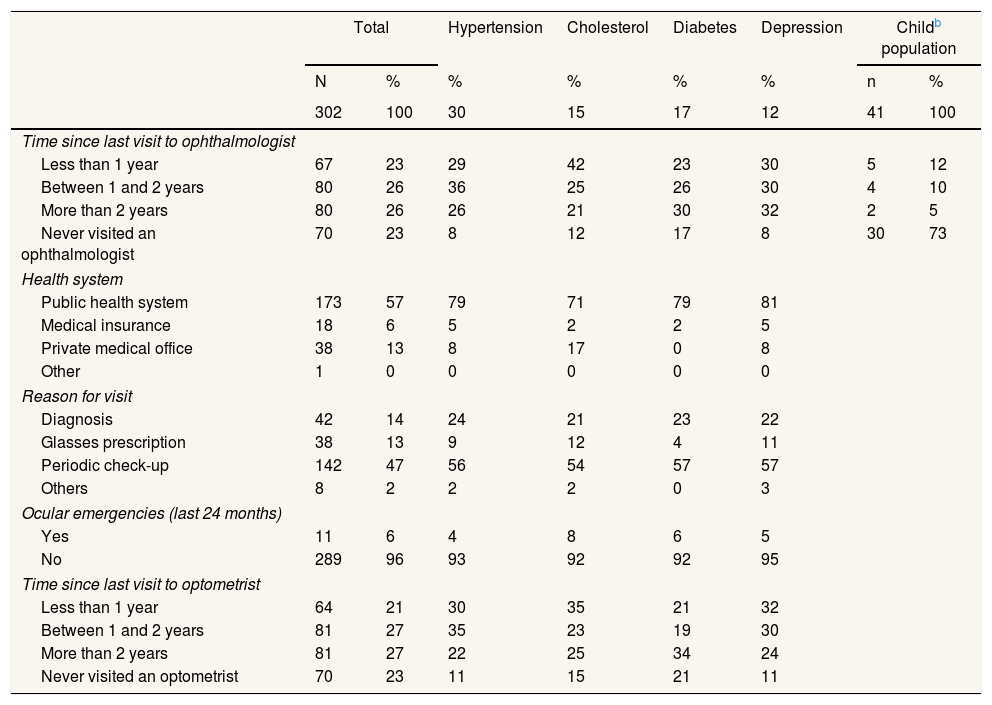
Table 5 shows that 49% of the studied rural population had visited the ophthalmologist in the last 24 months and 23% had never visited this type of specialist. In the child population (under age 16), 73.2% had never visited the ophthalmologist.
Use of visual health services in the rural municipality and disaggregated by groupsa.
| Total | Hypertension | Cholesterol | Diabetes | Depression | Childb population | |||
|---|---|---|---|---|---|---|---|---|
| N | % | % | % | % | % | n | % | |
| 302 | 100 | 30 | 15 | 17 | 12 | 41 | 100 | |
| Time since last visit to ophthalmologist | ||||||||
| Less than 1 year | 67 | 23 | 29 | 42 | 23 | 30 | 5 | 12 |
| Between 1 and 2 years | 80 | 26 | 36 | 25 | 26 | 30 | 4 | 10 |
| More than 2 years | 80 | 26 | 26 | 21 | 30 | 32 | 2 | 5 |
| Never visited an ophthalmologist | 70 | 23 | 8 | 12 | 17 | 8 | 30 | 73 |
| Health system | ||||||||
| Public health system | 173 | 57 | 79 | 71 | 79 | 81 | ||
| Medical insurance | 18 | 6 | 5 | 2 | 2 | 5 | ||
| Private medical office | 38 | 13 | 8 | 17 | 0 | 8 | ||
| Other | 1 | 0 | 0 | 0 | 0 | 0 | ||
| Reason for visit | ||||||||
| Diagnosis | 42 | 14 | 24 | 21 | 23 | 22 | ||
| Glasses prescription | 38 | 13 | 9 | 12 | 4 | 11 | ||
| Periodic check-up | 142 | 47 | 56 | 54 | 57 | 57 | ||
| Others | 8 | 2 | 2 | 2 | 0 | 3 | ||
| Ocular emergencies (last 24 months) | ||||||||
| Yes | 11 | 6 | 4 | 8 | 6 | 5 | ||
| No | 289 | 96 | 93 | 92 | 92 | 95 | ||
| Time since last visit to optometrist | ||||||||
| Less than 1 year | 64 | 21 | 30 | 35 | 21 | 32 | ||
| Between 1 and 2 years | 81 | 27 | 35 | 23 | 19 | 30 | ||
| More than 2 years | 81 | 27 | 22 | 25 | 34 | 24 | ||
| Never visited an optometrist | 70 | 23 | 11 | 15 | 21 | 11 | ||
With respect to groups with chronic diseases, 30% of diabetics indicated not having had an ophthalmologist visit in the past two years, and 17% had never been to an ophthalmologist.
Fifty-seven percent of the rural population uses eye health services from the public health system while 13% uses private medical services for this purpose (Table 5). The main reason for visiting the ophthalmologist was to conduct a periodic check-up (47%), while 13% made a visit to obtain a prescription for eye glasses. Results regarding ocular emergencies in the rural population show that 6% made use of such services in the last two years. Forty-eight percent of the rural population declared having been to an optometrist in the past 2 years (Table 5).
Additional results concerning the use of ophthalmic drugs within the past month showed that 23.9% of men and 30.6% of women used them. Artificial tears were used by 15.5% of men and 22.5% of women. Eye drops or gels for allergies and minor eye irritations were used by 9.2% of men and 6.9% of women. Use of eye drops for the treatment of glaucoma was declared by 2.8% of men and 3.6% of women during this period.
Perceived barriers to resolution of vision problems in the rural populationThe reasons for lack of treatment signaled by people with poor vision included the distance to the doctor's office (50%), associating vision loss with age (37%), the price of eye glasses or contact lenses (23%), low perceived quality of available services (10%), having adapted to the situation and not seeking health services (8%), the time on a wait list for a visit (5%), the belief that there was no possibility of improvement (4%) or others −lack of time− (<4%).
DiscussionThe results of this study show that up to 40% of the rural population presents poor perceived visual health and that poor perceived visual health is strongly associated with aging and widowhood, disadvantaged socioeconomic status and facing chronic diseases. The rural population is more likely to have visual difficulties and make less use of optical correction. The use of eye health services may not be sufficient particularly in children and diabetics.
Perceived visual health is a useful public health variable that has been previously associated with eye problems,21 depression,22 functional state and wellbeing for both middle-aged and the elderly.23 Although perceived vision loss may not always be related to a clinical diagnosis of an eye disorder, it is worth mentioning that in the elderly population vision problems are more frequent than patients might believe. The elderly may over-estimate their capacity for functional vision, given their understanding of their vision capacities as related to their age and the belief that a solution is not required nor exists.24 The association between widowed and poor perceived visual health could be conditioned by the advanced age of these persons.
Our results show that the socioeconomic profile of the rural population with visual limitations is low in terms of education, income and labor qualifications, as has been shown in other studies.25,26 Our findings also show that rural population with far sight difficulties is not receiving appropriate diagnosis and treatment, while near sight problems are apparently resolved without seeking an eye examination by using non-personally prescribed glasses.
Despite being one of the groups with greatest exposure to vision loss, nearly half of the diabetics in our study have not received an eye exam from specialized services –an ophthalmologist or optometrist's office− in the last 2 years. In people with diabetes, the existence of diabetic retinopathy is associated with poor glucose management, hypertension and lipids in the blood, and especially with the time elapsed since the initiation of the disease. It is for this reason that accepted clinical guidelines recommend an exam with observation of the back of the eye every 1 to 2 years for diabetics, even without known eye problems.27 In the case of children, the lack of pediatric eye exams observed contrasts with scientific evidence that highlights the need to prevent irreversible vision loss as caused by amblyopia, which is a treatable condition during childhood.28
Regarding factors that influence the use of health services, the population in the rural municipality indicated barriers such as the distance to the office, the price of optical treatments, and the lack of awareness for seeking possible solutions –associating vision problems with age−. Prior studies show that geographic distance to the health center and attitudes and beliefs often associated with rural life –such as lack of knowledge of health risks and a sense of self-sufficiency– generate greater resistance to seeking health care for patients with chronic diseases in rural communities.29
In similar studies in the British population, the lack of knowledge of certain diseases, the cost of treatment or services, the lack of coordination among first and second level health centers, and seeking an eye exam at an advanced stage of the disease, have also been identified as barriers to reducing vision loss.30 In this sense, protocols for primary care and referral have been proposed for rural environments in countries such Ireland that include optometry professionals, which promotes better care for complex cases by ophthalmologists and contribute to reduce health inequities.31
Considering the social, mental and functional implications of vision problems, national health surveys tend to include relevant information regarding visual health, which permits more efficient action towards reducing inequalities.32,33 However, in the case of Spain there is a lack of information on the use of specialized eye care services, as this information is not collected by national statistics. In a scenario of projected high population growth among the elderly population, it is significant that Ophthalmology was the specialty with the greatest number of waitlisted patients, ahead of traumatology, dermatology or cardiology.12
The global action plan for universal eye health promoted by the World Health Organization urges to member countries to create national plans and coordinate efforts for the prevention of blindness and visual disability.34 In Spain, although some regional eye-care policy models have been proposed35 and remarkable care is provided to people with visual disability and blindness through the National Organization for the Blind, there is no current national plan to address the increasing needs of the population for avoidable vision loss.
This study is subject to certain limitations. The cross-sectional study design does not permit establishing causality in the observed relationships. When comparing two samples of such a disparate size, the uncertainty of the smaller sample is greater, consequently these differences should be assumed with statistical caution. The comparison of results for the rural population and the general population is limited to the variables contained in the NHS concerning the use of eye glasses or contact lenses and the perceived limitations in near sight and far sight. The inclusion of new questions in the questionnaire used in this study may not be comparable a priori with other surveys. Nevertheless, there are few studies that include aspects related to visual health, population groups at risk, and the use of health services in the rural environment in Spain to justify pertinence of such approach. In our study, as in the National Health Survey, we do not capture the time elapsed since diagnosis in the case of chronic diseases as diabetes, which limits the possibilities to better estimate risk or plan future demand for services.
Against the benefits of promoting access to eye care services and treatments for the prevention of avoidable vision impairment, evidence exists that these interventions may fail to reduce risk of preventing falls and fractures in frail older people.36 As showed by recent review studies, there is a need for more clinical trials to analyze effectiveness, benefits and implications of visual health screening in the adult population.37
ConclusionsThe rural population presents worse visual health indicators, more visual limitations and less use of optical correction. Poor visual health is influenced by age, social factors such as disadvantaged socioeconomic status, and the presence of chronic diseases. The use of health services may not be sufficient to prevent irreversible vision loss, such as that caused by diabetic retinopathy or amblyopia.
In light of the results of this study, it should be questioned whether the current system for prevention of visual disability in Spain sufficiently contributes to reducing inequalities in visual health and addressing the estimated increase in future demand for services. Actions to increase awareness and access to health services for an early diagnosis, treatment and better follow-up of eyesight disorders in the rural population may improve health outcomes and reduce inequities.
Editor in chargeMercedes Carrasco Portiño.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
During the last decade, the prevalence of visual impairment is growing in Spain and is unequally distributed among groups with an increased risk in lower-income regions. There is a scarcity of research in Spain related inequities in visual health and the use of eye care services, particularly with respect to those living in rural areas.
What does this study add to the literature?The rural population presents worse visual health indicators and these results are influenced by age, gender, socioeconomic status, and the presence of chronic illnesses. The use of health services is not sufficient to prevent irreversible vision loss for those at risk. Actions are needed to prevent inequities.
S. Latorre-Arteaga designed the study, planned the data collection, analyzed and interpreted the results, and wrote the first draft of the manuscript. J. Fernández-Sáez carried out the statistical analysis and interpretation of data. D. Gil-González made contributions to conception and design of the study, the analysis and interpretation of data, and contribute to writing the first draft. All authors approved the final version of the manuscript.
FundingThe study was supported by Entretodos Foundation-Global Health Vision (Spain), a nonprofit organization, and by the authorities of Cenicientos (Madrid, Spain).
Conflicts of interestNone.
We thank Maria del Mar Seguí Crespo and Ángel García Muñoz from University of Alicante for their support of the survey design, and Ignacio Gregorio Sánchez Mezquita for his support to implement the study.











