



It is well known that sex differences in analgesic prescription are not merely the logical result of greater prevalence of pain in women, since this therapeutic variability is related to factors such as educational level or social class. This study aims to analyse the relationship between analgesic prescription and gender development in different regions of Spain.
MethodsCross-sectional study of sex-differences in analgesic prescription according to the gender development of the regions studied. Analgesic prescription, pain and demographic variables were obtained from the Spanish Health Interview Survey in 2006. Gender development was measured with the Gender Development Index (GDI). A logistic regression analysis was conducted to compare analgesic prescription by sex in regions with a GDI above or below the Spanish average.
ResultsOnce adjusted by pain, age and social class, women were more likely to be prescribed analgesics than men, odds ratio (OR) = 1.74 (1.59-1.91), as residents in regions with a lower GDI compared with those in region with a higher GDI: ORWomen = 1.26 (1.12-1.42), ORMen = 1.30 (1.13-1.50). Women experiencing pain in regions with a lower GDI were more likely than men to be treated by a general practitioner rather than by a specialist, OR = 1.32 (1.04-1.67), irrespective of age and social class.
ConclusionsGender bias may be one of the pathways by which inequalities in analgesic treatment adversely affect women's health. Moreover, research into the adequacy of analgesic treatment and the possible medicalisation of women should consider contextual factors, such as gender development.
Las diferencias por sexo en la prescripción de analgésicos no son simplemente el resultado lógico de una mayor prevalencia del dolor en las mujeres (ya que se relaciona con factores como la educación o la clase social). El objetivo de este estudio fue analizar la relación entre la prescripción de analgésicos y el desarrollo de género de las regiones de España.
MétodosEstudio transversal de las diferencias por sexo en la prescripción de analgésicos en función del desarrollo de género de las regiones. La prescripción de analgésicos, el dolor y las variables demográficas se obtuvieron de la Encuesta Nacional de Salud de 2006. El desarrollo de género se midió con el Índice de Desarrollo al Género (IDG). Se realizó un análisis de regresión logística para comparar la prescripción de analgésicos por sexo en las regiones con IDG mayor o menor que la media española.
ResultadosIndependientemente del dolor, la edad y la clase social, las mujeres tienen mayor probabilidad de prescripción de analgesia que los hombres, con una odds ratio (OR) = 1,74 (1,59-1,91), así como los residentes de las regiones con menor IDG en comparación con los de regiones con mayor IDG: ORMujeres = 1,26 (1,12-1,42), ORHombres = 1,30 (1,13-1,50). Las mujeres que padecen dolor en regiones de menor IDG tienen más probabilidades de ser tratadas por un médico y no por un especialista, con una OR = 1,32 (1,04-1,67).
ConclusionesEl sesgo de género puede ser una vía por la cual las desigualdades en el tratamiento analgésico afecta negativamente a la salud de las mujeres. La investigación sobre la conveniencia de la analgesia y la medicalización de las mujeres debería incluir factores de contexto, como el desarrollo de género.
Consistent with the greater prevalence of pain in women, epidemiological studies have shown that they report a significantly higher use of analgesics than men.1,2 Accordingly, pain should logically be the main reason for analgesic prescription. However, the literature indicates that given the same pain intensity, women are more likely to be prescribed analgesics.3 Furthermore, for the same intensity, men are prescribed more aggressive treatment (for example, opioid-analgesia for men versus non-opioid analgesia for women).4 It is important to determine whether this difference is explained by adequate drug use or whether women are unnecessarily exposed to a much greater risk of adverse effects and dependency as they are more frequently prescribed with analgesics.5
It was during the 1990s that empirical evidence began to emerge regarding the possibly inappropriate treatment of women as a result of gender bias, indicating differential management of men and women with the same health problem.6 Of particular note are the gender bias studies related to the treatment of cardiovascular disease.7 At that time, much of the gender bias in health care could be explained by insufficient knowledge of this issue. However, given the amount of evidence published in the literature today, lack of knowledge can no longer explain the persistence of this problem.7 Furthermore, women's lack of access to specialist services and the symptomatic treatment they receive imply that the cause of the problem is being overlooked.8,9
The therapeutic variability associated with the sex of patients experiencing pain is related not only to individual factors, such as marital status, educational level and lifestyle,1,10 but also to factors linked to social inequalities such as ethnic group and social class.11,12 A study conducted by Kawachi et al.13 highlights the importance of gender inequalities for the social determinants of health and demonstrates the association with social status for women and morbidity for both sexes, according to geographic region within the same country. More recently, the final report of Sen et al.14 for the WHO Commission on Social Determinants of Health indicates that gender inequality undermines the physical and mental health of millions of girls and women worldwide, as well as that of boys and men. Furthermore, the association between the empowerment of women and community health indicators has been demonstrated,15 based particularly on the woman's role as the primary caregiver within the family. Nevertheless, further research is necessary to determine which specific aspects of the empowerment of women effectively influence the health of the larger community.15
The Gender Development Index (GDI), created in 1995 by the United Nations, is the Human Development Index that differentiates the development of women and men as regards life expectancy at birth, as well as two important health determinants: education and income.16 Recent studies have shown that clear regional inequalities exist within Spain.17 Historically, northern regions have enjoyed greater economic and gender development18 which, according to the literature cited above, suggests that analgesic prescription may be subject to gender bias in southern regions of Spain. The existence of gender bias in analgesic treatment poses some additional problems since national health services were created to reduce inequalities and to provide free services to all citizens regardless of their ethnic group, social class or gender.19 In these equity-based systems, discrimination against over half the population — women— has more explicit political implications.
The literature on differential analgesic prescription for men and women has not focused to date on contextual determinants such as human development according to region of residence. Based on the Spanish National Health Survey 2006/2007, the aim of this study was to analyse factors associated with analgesic prescription according to levels of gender development in Spain, considering pain, age and social class.
MethodsDesign and source of dataWe used individualised secondary data collected during the Spanish National Health Survey carried out in 2006 and 200720 which was conducted by the Spanish Statistics Institute under the aegis of the Ministry of Health and Social Policy. The format of this survey was adapted to meet the requirements of the guidelines for the development and criteria for the adoption of Health Survey instruments proposed by the European Commission.21 The survey covered a representative sample of Spain's non-institutionalised population residing in main family dwellings (households) and, in order to meet its aim of being able to furnish estimates with a certain degree of reliability at national and regional levels, a sample of 29,478 households was selected. Study subjects were selected by means of probabilistic multistage sampling, in which the first-stage units were the census sections, and the second-stage units were main family dwellings. Information was collected in home-based personal interviews. The methodology is described elsewhere.20 A total of 29,478 adults (individuals aged at least 16 years old) of both sexes (14,459 men and 15,019 women) living in Spain were interviewed.
Using the data collected, this study presents a nationwide, descriptive, cross-sectional epidemiologic study of analgesic prescription.
VariablesThe dichotomous dependent variable chosen was the answer “yes” or “no” to the question “In the last two weeks, have you taken any pain medication prescribed to you by a doctor?”
The independent variables collected in the study were primary socio-demographic characteristics such as age (divided into three categories: 16-44, 45-64, ≥65 years), sex and occupational status, which was used as a proxy variable of social class (manual/non manual).22
The variable pain confirmed by a doctor was created based on the answers to questions about different types of pain: “has a doctor confirmed that you are experiencing neck pain, lumbar pain or frequent headaches/migraine in the last 12 months?” We considered the answer affirmative if the interviewee answered “yes” to having being diagnosed with at least one of these types of pain.
The independent variable medical consultation was classified as dichotomous: consulting a general practitioner (people who answered that they had visited a general practitioner once or more in the last four weeks, and who had not seen a specialist) and seeing a specialist (people who responded that they had consulted a specialist once or more). This variable was created from two questions: “how many times have you visited a general practitioner in the last 4 weeks due to a complaint or a disease?” and “how many times have you consulted a specialist?” Although it was not possible to establish whether pain was the reason for visiting the general practitioner or specialist, this variable was only calculated for those subjects with pain diagnosed by a doctor and prescribed an analgesic. No reason for medical consultation was excluded.
With the aim of identifying gender inequalities within a country, province or region, the UN proposed the GDI. The GDI has been used to measure gender inequalities in health, as it includes life expectancy by sex as well as two determinants of health: educational level and purchasing power parity.16
Gender development is measured by calculating GDI values (0: low gender development index – 1: high gender development index). The GDI is the average of three sub-indices: the equally distributed life expectancy index, the equally distributed education index and the equally distributed income index, measured by the gross domestic product per capita, expressed as equally distributed purchasing power parity in US dollars.23 For this study, we used a dichotomous classification of the 2005 GDI for the different regions in Spain: below national average in Spain (Andalusia, Asturias, the Canary Islands, Castile-La Mancha, Region of Valencia, Extremadura, Galicia, Murcia) or above (Aragon, the Balearic Islands, Cantabria, Castile and León, Catalonia, Madrid, Navarre, the Basque Country, La Rioja), based on previous work published in detail by our research team.18
This classification showed a north-south pattern whereby gender development in northern regions of Spain is above the national average whilst in the south it is lower.
In order to express the dimension and direction of the difference that exists between men and women in analgesic prescription, the gender gap was calculated as the difference between the percentage of analgesic prescription for women and men, and it was standardised by dividing this difference by the sum of both percentages.
Statistical analysisAnalgesic prescription patterns for women and men for the year 2006 were stratified by age, social class, the GDI for the area of residence in Spain, diagnosis of pain by a doctor and consultation with a general practitioner or a specialist. The χ2 test and a contrast of proportional equality were used to determine the significance of differences between men and women.
To estimate the independent effect of sex on analgesic prescription, a non-conditional logistic regression model was used. We calculated the odds ratio (OR) and confidence intervals of 95% (CI95%), adjusted for pain confirmed by a doctor, age and social class. We also calculated the association between analgesic prescription and sex for the different social classes (adjusted for age and pain) and for different age groups (adjusted for social class and pain). The same analysis was conducted for regions with a GDI above or below the Spanish average. Furthermore, the probability of analgesic prescription for men was calculated according to the GDI for their area of residence and for the different social classes and age groups, as it was for women.
In order to determine general practitioner and specialist consultation patterns according to sex for those individuals who responded in the affirmative to the question regarding pain confirmed by a doctor in the last 12 months, raw probability was calculated, together with probability adjusted for age and social class. The same analysis was conducted for regions with a GDI above or below the Spanish average.
The SPSS software package version 16 and EPIDAT were used for all calculations and statistical analyses.
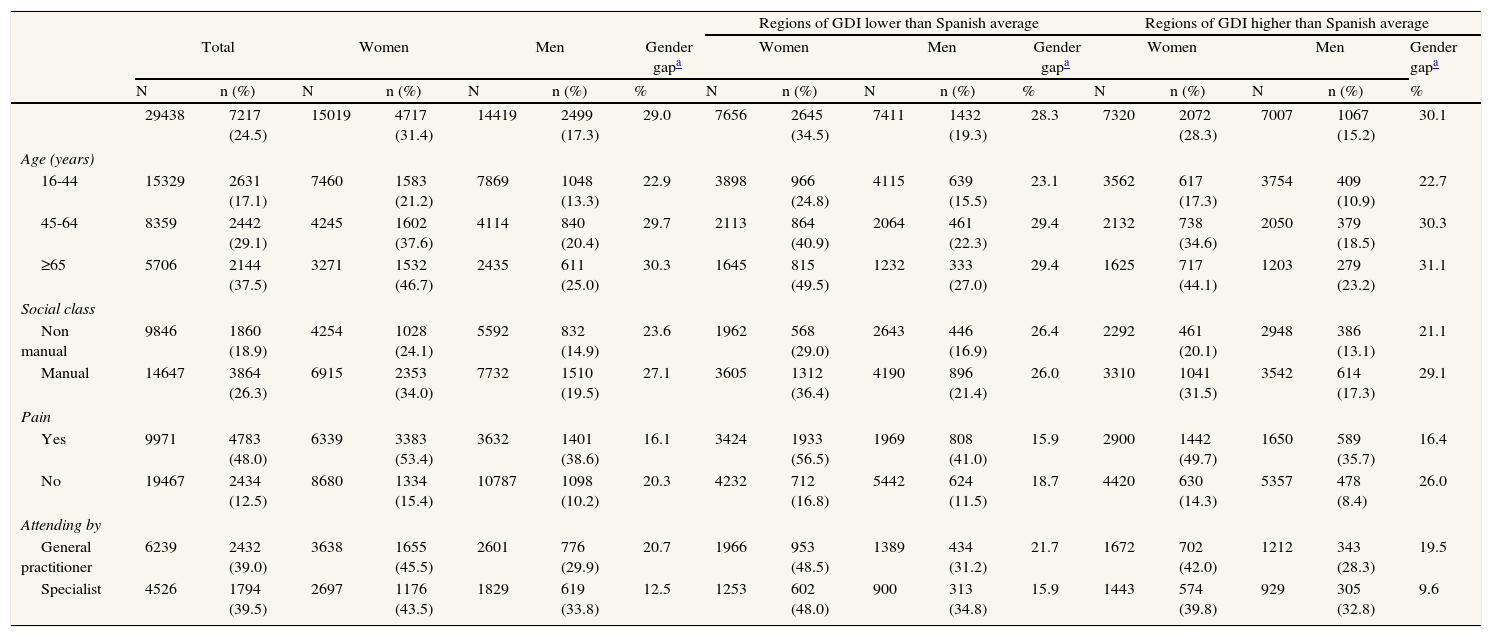
ResultsAccording to the 2006 Spanish HIS, a significantly higher proportion of women than men were prescribed analgesics by a doctor in the two weeks prior to the survey (gender gap 29%), with a 42.1% (6,324) prevalence of pain confirmed by a doctor in women and 25.1% (3,632) in men. Moreover, Table 1 shows that more women than men who had been prescribed analgesics suffered pain (gender gap 16.1%). The same sex-difference trends in analgesic prescription were observed for all age groups (increasing with age), social classes (higher in manual workers), regional levels of gender development (higher in regions with a lower GDI) (p <0.001) and according to the type of health care provision (higher for general practitioners than specialists) (p <0.001).
Comparing analgesic prescription by sex and GDI of area of residence in Spain; according to age, social class and type of medical attention.
| Regions of GDI lower than Spanish average | Regions of GDI higher than Spanish average | ||||||||||||||||
| Total | Women | Men | Gender gapa | Women | Men | Gender gapa | Women | Men | Gender gapa | ||||||||
| N | n (%) | N | n (%) | N | n (%) | % | N | n (%) | N | n (%) | % | N | n (%) | N | n (%) | % | |
| 29438 | 7217 (24.5) | 15019 | 4717 (31.4) | 14419 | 2499 (17.3) | 29.0 | 7656 | 2645 (34.5) | 7411 | 1432 (19.3) | 28.3 | 7320 | 2072 (28.3) | 7007 | 1067 (15.2) | 30.1 | |
| Age (years) | |||||||||||||||||
| 16-44 | 15329 | 2631 (17.1) | 7460 | 1583 (21.2) | 7869 | 1048 (13.3) | 22.9 | 3898 | 966 (24.8) | 4115 | 639 (15.5) | 23.1 | 3562 | 617 (17.3) | 3754 | 409 (10.9) | 22.7 |
| 45-64 | 8359 | 2442 (29.1) | 4245 | 1602 (37.6) | 4114 | 840 (20.4) | 29.7 | 2113 | 864 (40.9) | 2064 | 461 (22.3) | 29.4 | 2132 | 738 (34.6) | 2050 | 379 (18.5) | 30.3 |
| ≥65 | 5706 | 2144 (37.5) | 3271 | 1532 (46.7) | 2435 | 611 (25.0) | 30.3 | 1645 | 815 (49.5) | 1232 | 333 (27.0) | 29.4 | 1625 | 717 (44.1) | 1203 | 279 (23.2) | 31.1 |
| Social class | |||||||||||||||||
| Non manual | 9846 | 1860 (18.9) | 4254 | 1028 (24.1) | 5592 | 832 (14.9) | 23.6 | 1962 | 568 (29.0) | 2643 | 446 (16.9) | 26.4 | 2292 | 461 (20.1) | 2948 | 386 (13.1) | 21.1 |
| Manual | 14647 | 3864 (26.3) | 6915 | 2353 (34.0) | 7732 | 1510 (19.5) | 27.1 | 3605 | 1312 (36.4) | 4190 | 896 (21.4) | 26.0 | 3310 | 1041 (31.5) | 3542 | 614 (17.3) | 29.1 |
| Pain | |||||||||||||||||
| Yes | 9971 | 4783 (48.0) | 6339 | 3383 (53.4) | 3632 | 1401 (38.6) | 16.1 | 3424 | 1933 (56.5) | 1969 | 808 (41.0) | 15.9 | 2900 | 1442 (49.7) | 1650 | 589 (35.7) | 16.4 |
| No | 19467 | 2434 (12.5) | 8680 | 1334 (15.4) | 10787 | 1098 (10.2) | 20.3 | 4232 | 712 (16.8) | 5442 | 624 (11.5) | 18.7 | 4420 | 630 (14.3) | 5357 | 478 (8.4) | 26.0 |
| Attending by | |||||||||||||||||
| General practitioner | 6239 | 2432 (39.0) | 3638 | 1655 (45.5) | 2601 | 776 (29.9) | 20.7 | 1966 | 953 (48.5) | 1389 | 434 (31.2) | 21.7 | 1672 | 702 (42.0) | 1212 | 343 (28.3) | 19.5 |
| Specialist | 4526 | 1794 (39.5) | 2697 | 1176 (43.5) | 1829 | 619 (33.8) | 12.5 | 1253 | 602 (48.0) | 900 | 313 (34.8) | 15.9 | 1443 | 574 (39.8) | 929 | 305 (32.8) | 9.6 |
Source of information: Spanish National Health Interview Survey 2006.
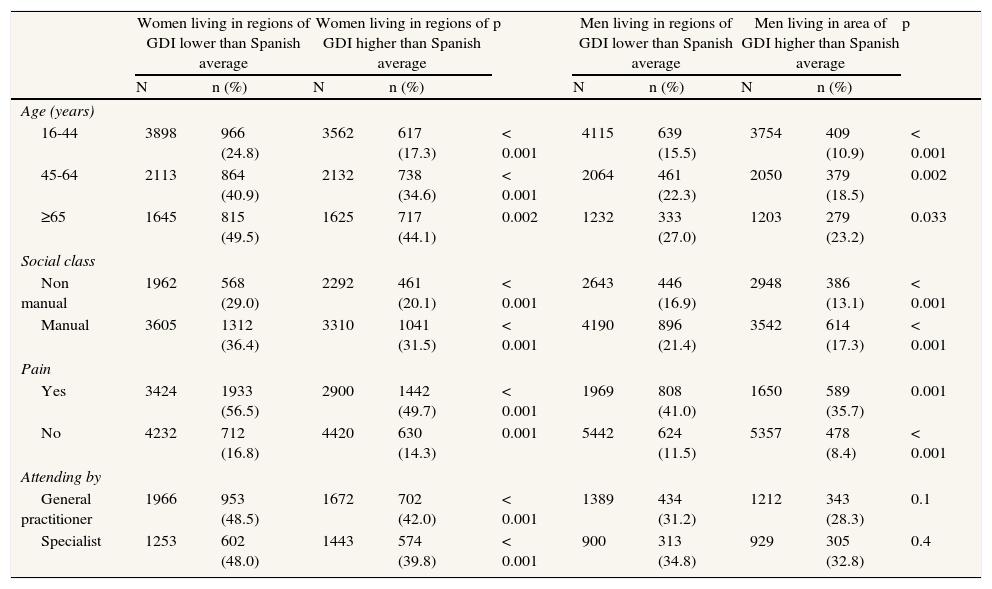
The prevalence of pain experienced by women in the 12 months prior to the survey is higher than in men in regions with an above average gender development index (39.6% of women and 23.5% of men), and also in regions with a below average gender development index (44.7% of women and 26.6% of men). In Table 1, analgesic prescription data are broken down and presented according to the GDI of the autonomous regions of residence. The same sex-difference can be observed for analgesic prescription according to age, social class and type of health care provision (general practitioner or specialist) (p < 0,001).
In regions with a GDI below the Spanish average, pain was more prevalent (35.8%) than in those regions with a higher GDI (31%). Women living in lower GDI regions were prescribed analgesics at a greater rate than those living in regions with a higher GDI, according to age and social class. The same trend was also observed for men. It was only in the case of women that differences were detected in relation to health care provision by a general practitioner or specialist, since those who lived in lower GDI regions were more frequently attended by a general practitioner than women living in higher GDI regions (p <0.001) (Table 2).
Comparing analgesic prescription by gender development of the area of residence in Spain in women and men; according to age, social class and type of medical attention.
| Women living in regions of GDI lower than Spanish average | Women living in regions of GDI higher than Spanish average | p | Men living in regions of GDI lower than Spanish average | Men living in area of GDI higher than Spanish average | p | |||||
| N | n (%) | N | n (%) | N | n (%) | N | n (%) | |||
| Age (years) | ||||||||||
| 16-44 | 3898 | 966 (24.8) | 3562 | 617 (17.3) | < 0.001 | 4115 | 639 (15.5) | 3754 | 409 (10.9) | < 0.001 |
| 45-64 | 2113 | 864 (40.9) | 2132 | 738 (34.6) | < 0.001 | 2064 | 461 (22.3) | 2050 | 379 (18.5) | 0.002 |
| ≥65 | 1645 | 815 (49.5) | 1625 | 717 (44.1) | 0.002 | 1232 | 333 (27.0) | 1203 | 279 (23.2) | 0.033 |
| Social class | ||||||||||
| Non manual | 1962 | 568 (29.0) | 2292 | 461 (20.1) | < 0.001 | 2643 | 446 (16.9) | 2948 | 386 (13.1) | < 0.001 |
| Manual | 3605 | 1312 (36.4) | 3310 | 1041 (31.5) | < 0.001 | 4190 | 896 (21.4) | 3542 | 614 (17.3) | < 0.001 |
| Pain | ||||||||||
| Yes | 3424 | 1933 (56.5) | 2900 | 1442 (49.7) | < 0.001 | 1969 | 808 (41.0) | 1650 | 589 (35.7) | 0.001 |
| No | 4232 | 712 (16.8) | 4420 | 630 (14.3) | 0.001 | 5442 | 624 (11.5) | 5357 | 478 (8.4) | < 0.001 |
| Attending by | ||||||||||
| General practitioner | 1966 | 953 (48.5) | 1672 | 702 (42.0) | < 0.001 | 1389 | 434 (31.2) | 1212 | 343 (28.3) | 0.1 |
| Specialist | 1253 | 602 (48.0) | 1443 | 574 (39.8) | < 0.001 | 900 | 313 (34.8) | 929 | 305 (32.8) | 0.4 |
Source of information: Spanish National Health Interview Survey 2006.
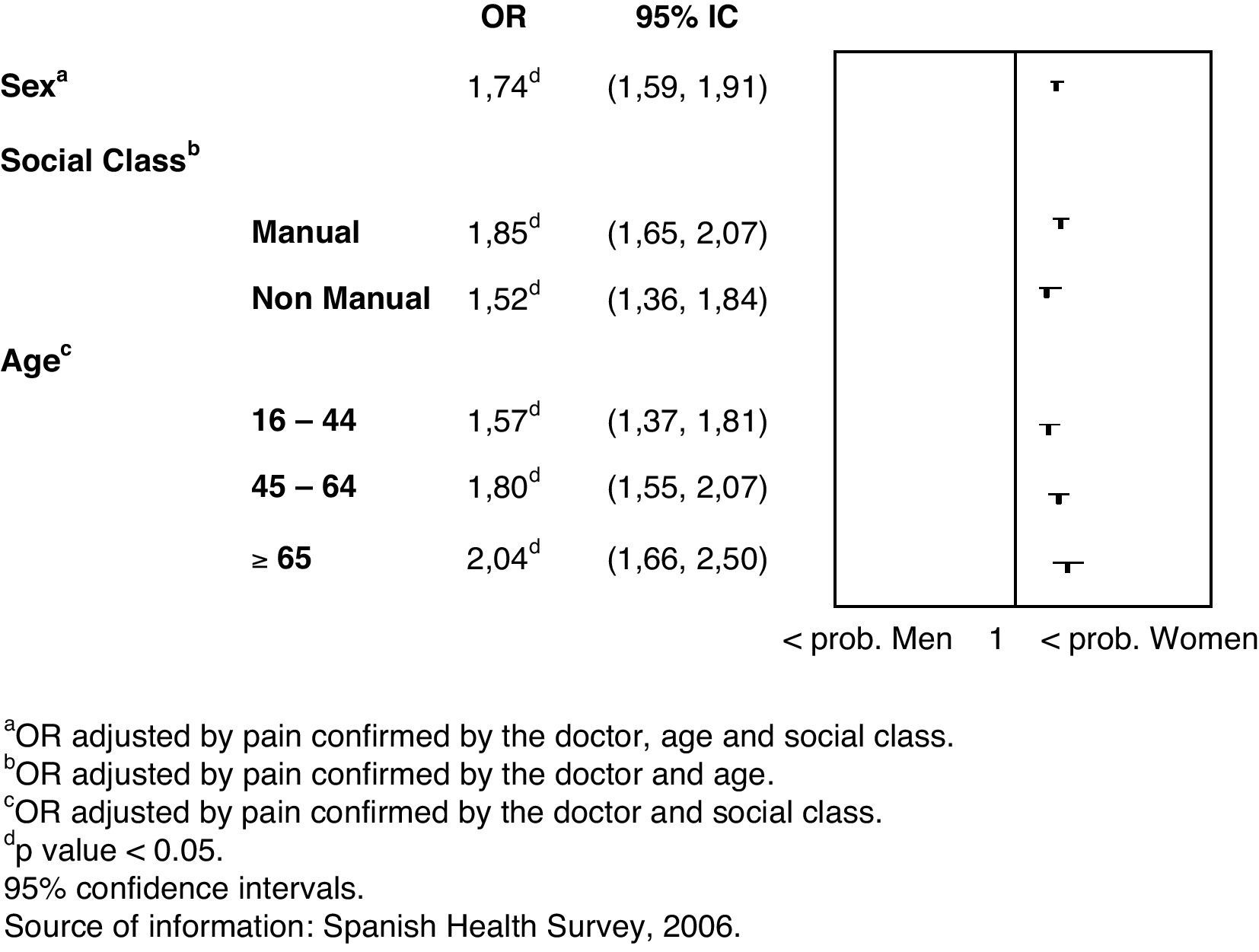
When adjusting for pain confirmed by a doctor, age and social class (Fig. 1), there was still a greater probability of analgesic prescription for women than for men, OR = 1.74 (CI95%: 1.59-1.91). Specifically, this was the case among individuals belonging to the manual class and for all age groups (Fig. 1). In particular, the probability of analgesic prescription for women over 65 was twice as high as for men.

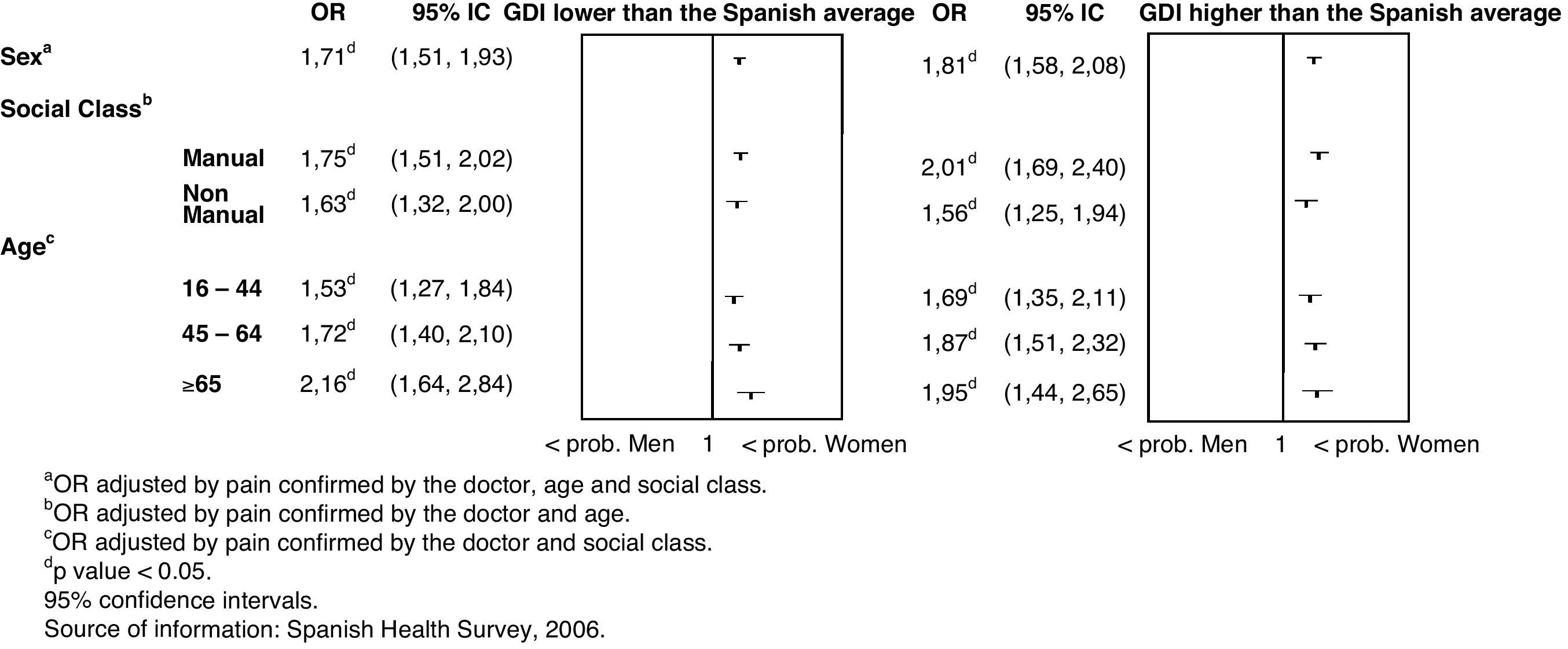
In Figure 2, these results are broken down and presented according to the level of gender development in the area of residence. After adjusting for social class, age and pain, the probability of analgesic prescription was higher for women than for men in autonomous regions with a GDI above (OR = 1.71 [CI95%: 1.51-1.93]) and below the Spanish average (OR = 1.81 [CI95%: 1.58-2.08]). This difference can be observed in all social classes and age groups.

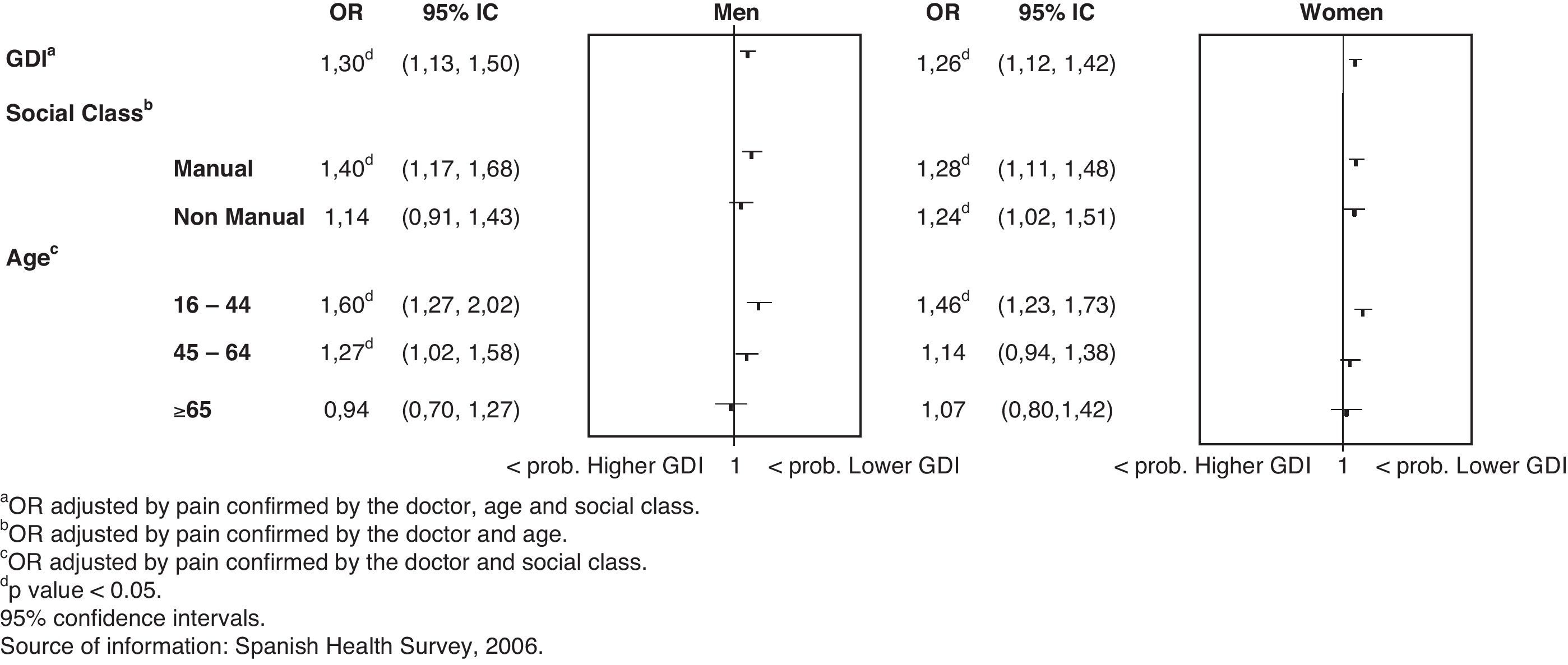
It can be seen in Figure 3 that, once adjusted for pain, social class and age, women living in regions with a lower level of gender development were more likely to be prescribed analgesics than those living in more gender-developed regions OR = 1.26 (CI95%: 1.12-1.42). The same pattern can be observed for social class after adjusting for pain and age. There was also a higher probability of analgesic prescription among men living in regions with a lower level of gender development OR = 1.30 (CI95%: 1.13-1.50), and among those from the manual social class.

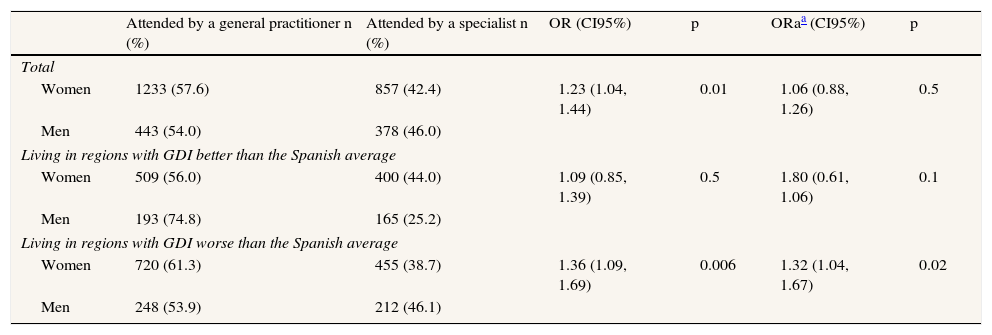
Table 3 shows that in regions with a lower level of gender development, health care (general practitioner, or general practitioner and/or specialist) for people experiencing pain varied according to sex. Regardless of age or social class, women suffering pain are more likely than men to be seen by a general practitioner and not by a specialist (OR = 1.32 [CI95%: 1.04-1.67]).
Likelihood of being attended by general practitioner versus specialist according to GDI of the area of residence in population with pain and analgesic prescription.
| Attended by a general practitioner n (%) | Attended by a specialist n (%) | OR (CI95%) | p | ORaa (CI95%) | p | |
| Total | ||||||
| Women | 1233 (57.6) | 857 (42.4) | 1.23 (1.04, 1.44) | 0.01 | 1.06 (0.88, 1.26) | 0.5 |
| Men | 443 (54.0) | 378 (46.0) | ||||
| Living in regions with GDI better than the Spanish average | ||||||
| Women | 509 (56.0) | 400 (44.0) | 1.09 (0.85, 1.39) | 0.5 | 1.80 (0.61, 1.06) | 0.1 |
| Men | 193 (74.8) | 165 (25.2) | ||||
| Living in regions with GDI worse than the Spanish average | ||||||
| Women | 720 (61.3) | 455 (38.7) | 1.36 (1.09, 1.69) | 0.006 | 1.32 (1.04, 1.67) | 0.02 |
| Men | 248 (53.9) | 212 (46.1) | ||||
Source of information: Spanish National Health Interview Survey 2006.
OR: odds ratio; CI95%: confidence interval of 95%.
Our results show that in Spain, analgesic prescription for men is frequent (17.3%), but much more so for women (31.4%). Being a woman and living in regions with a gender development index below the Spanish average are two factors that increase the probability of analgesic prescription. Our results suggest that women do not receive adequate care or attention for their symptoms and health needs; instead, their symptoms are treated with analgesics, and the potential health conditions causing the pain are dismissed or overlooked, preventing them from being referred to a specialist and/or receiving the correct treatment. The other significant finding was that, in these regions, women with pain who received analgesic prescription were more likely to be seen by a general practitioner alone, whereas men had a greater chance of being seen by a specialist. Thus, the main contribution of this study is the analysis of trends regarding analgesic prescription in Spain from a gender perspective.
The limitations of this study include the fact that since the Spanish Health Survey was based on self-reports of pain, it is possible that gender differences as regards reporting behaviour may explain some of the sex differences observed in the prevalence of pain, since women usually report pain with more frequency than men and also express quality of pain differently.24 Pain was measured using the questions in the Spanish Health Survey about migraine and chronic pain located in the back and neck. However, other regions of pain, such as joints, were not included. Nevertheless, the results of the European Pain Survey about location of pain indicate that the regions referred to in our study are among the most common.25
Given that the questions specifically referred to the two weeks prior to our survey, there was less probability of memory bias regarding analgesic prescription, although self-reporting bias remained a possibility. Nevertheless, the frequency of analgesic prescription would have been even higher if the question had referred to the previous 12 months, as in the case of pain.26 When interpreting the results, we did not consider the interval between the questions regarding analgesic prescription and pain diagnosed by a doctor, and thus can only assume that the prescription was in fact related to the pain diagnosed 12 months previously, as these questions enquired about chronic pain. A similar situation arises as regards consultation with a general practitioner or a specialist, as we do not know whether or not said consultation was related to pain or analgesia. In addition, we only analysed prescribed analgesics. However, although it might be thought that men are perhaps more likely to self-medicate, a recent study using data from the Spanish National Health Survey has shown that men do not in fact use analgesics without a prescription more frequently than women.27 Despite these limitations, the Spanish National Health Survey has proven to be a valid and widely used tool for estimating drug prescription patterns. Nevertheless, these findings require confirmation by longitudinal studies using methods which explore potential causal factors.
According to the Spanish Health Survey of 2006, more women than men reported pain confirmed by a doctor. This finding is consistent with other studies and is the main factor which determines analgesic prescription.28 It is important to draw attention to this fact since it has been observed that analgesic administration is less influenced by the discomfort of the person experiencing pain than by the doctor's preconceptions about the person in question.3,29 In practice, more women are prescribed analgesics than men,29 even after adjusting for pain and age. This also remains the case after adjusting for social class, which several studies have shown to be associated with pain and prescription.4,11 This finding may indicate that analgesic prescription is not merely the logical result of greater prevalence of pain.
Doctors interpret symptoms differently, depending on whether these are presented by men or women.30 Pain is a symptom related to a variety of illnesses and can be interpreted differently, including according to sex, which can lead to different therapeutic approaches.31 There are several gender differences with regard to aetiology, selected clinical characteristics and association of symptoms and signs with coronary heart disease in patients presenting chest pain in a primary care setting.32 This may translate into reduced awareness of the severity of an acute myocardial infarction, characterised by precordial pain which appears to be related to lower diagnosis rates of the condition before arrival at the hospital.33 Therefore, doctors’ different interpretations of pain in women may lead to inadequate treatment of their symptoms and an unsatisfactory response to their health needs.
The reasons given in the literature for higher levels of analgesic prescriptions to women than men include assertions that women are more sensitive to pain, are less tolerant of pain and have a greater need to report it.5 Perceiving and expressing pain more than men may lead to more prescriptions among women, and with greater frequency for low level pain, as occurs with other symptomatic medicines. However, several studies have demonstrated that this might depend on factors related to the doctor, who is more prone to offer drugs to female patients than to males with the same symptoms, regardless of gendered preconceptions.24 Consequently, it is important to consider whether this difference implies a negative effect for women's health in terms of medicalisation or whether it is negative for men in terms of insufficient treatment. Although the adequacy of analgesic prescription was not assessed in this study, the difference between women and men was not explained by differences in prevalence of pain, since our results were adjusted for pain.
The other main contribution of this study concerns those factors that influence analgesic prescription in relation to the level of gender development in the regions of residence. This finding has emerged irrespective of our results regarding individual patient factors such as sex, social class and age. Thus, in regions with the lowest GDI in the country, higher rates of analgesic prescription were found for both sexes. This finding may be explained by the greater prevalence of pain in these regions, coinciding with one of the few publications which has explored the relationship between gender development and health –the study Health Behaviour in School-Aged Children– which demonstrated that women living in countries with a lower gender development report experiencing certain complaints, such as headaches or abdominal pain, with more frequency.34 However, the prevalence of pain does not entirely explain analgesic prescription since, once its effect has been eliminated, it remains the case that the lower the level of gender development, the higher the level of analgesic prescription, and that this is even more pronounced among women.
As regards an explanation for the higher levels of analgesic prescription for women than for men, especially among those women living in regions with a lower level of gender development, an argument which has been suggested in other studies may be pertinent here, namely, that it is due to a vicious circle of repeated visits at the same level of health care, with associated lack of access to specialist services and restriction to non-specific, symptomatic treatment (analgesics).35
The results of this study can be associated with the body of research which has attempted to demonstrate that illness and treatment trends reflect the economic and political characteristics of each society and the various forms of social inequality. Gender inequality affects health and gender inequalities in health.36 In this respect, it has been demonstrated that the empowerment of women and their participation in political, economic and social life is associated with lower mortality rates among both women and men, and with infant well-being.15 Furthermore, it has been shown that women can experience problems related to the equality and quality of health care as regards access to specialist services,33,37one of the consequences of which is an increase in the prescription of symptomatic treatment. In relation to symptomatic treatment such as analgesics, a study in Spain (Catalonia) has shown that in a population with pain, women were attended more frequently by a general practitioner whereas men were referred more frequently to hospital.38 This effect has already been reported for other health problems such as tuberculosis39 or myocardial infarction.33 These differences in referral are important, as our review of the literature suggests that specialists are more knowledgeable about specific medical conditions, use more resources and may achieve better clinical outcomes.40 Moreover, a Spanish study found that agreement between general practitioners and specialists regarding diagnosis of pathologies with less diagnostic criteria was moderate or low.41
This study makes a further contribution to knowledge in this field, specifically that women may be exposed to a double gender bias, the first deriving from the condition of being a woman and the second from the context of lower regional levels of gender development, the latter of which also affects men. This study is therefore important as it adds a contextual factor that conditions the treatment of pain, namely, the level of gender development in the area of residence. These findings need to be confirmed by longitudinal studies using methods which explore potential causal factors. Gender bias may be one of the pathways by which inequalities in analgesic treatment adversely affect women's health. Moreover, research into the suitability of analgesic treatment and the possible medicalisation of women should consider contextual factors, such as gender development, since these could involve a high price for women's health as well as inflated pharmaceutical costs in these times of economic crisis. In order to prevent gender bias amongst health professionals when treating pain, this issue should form part of medical school curricula.
It is well known that sex differences in analgesic prescription are not merely the logical result of greater prevalence of pain in women (since this therapeutic variability is related to factors as educational level or social class).
What this study adds to what was known?This study adds a contextual factor conditioning treatment of pain: being a woman and living in areas with lower gender development are two independent determining factors which increase the likelihood of a physician deciding to prescribe analgesia. In these areas, women experiencing pain are less likely to be treated by specialists than men. Institutions conducting clinical practice guidelines and scientific societies should take steps to inform physicians about gender inequalities in analgesic prescription; and to place it in guidelines of medical practice.
E. Chilet Rosell contributed to conception and design, acquisition and interpretation of data, drafting the article, revising it critically for important intellectual content and final approval of the version to be published. M.T. Ruiz Cantero contributed to conception and design, acquisition and interpretation of data, drafting the article, revising it critically for important intellectual content and final approval of the version to be published. J. Fernández contributed to conception and design, acquision analysis and interpretation of data, revising it critically for important intellectual content and final approval of the version to be published. C. Alvárez-Dardet contributed to conception and design, interpretation of data, revising it critically for important intellectual content and final approval of the version to be published.
FundingThis work has been partially financed by CIBER of Epidemiology and Public Health (CIBERESP), Spain.
Conflicts of interestOne of the authors (C. Álvarez-Dardet) is a member of the editorial board of the journal but has not taken part in the editorial process of the manuscript.
Thank you to Maica Rodríguez Sanz for her helpful comments.











