



To determine the characteristics of users of a smoking cessation programme run by the Open University of Spain (Universidad Nacional de Educación a Distancia [UNED]).
MethodsWe examined the demographic, psychological and smoking characteristics of 23,763 smokers who participated in the on-line smoking cessation program of the UNED. The programme was open to any smoker, free of charge, and was fully automated and with direct access.
ResultsA total of 93.5% of the users were Spaniards, with an equal percentage of participation among men and women. The mean age was 39 years. Somewhat less than half were married and had a university education. The participants smoked a mean of 19.3 cigarettes per day, showing a mid-range level of nicotine dependence according to the Heaviness of Smoking Index. The results of the Anxiety and Depression subscales of the Symptom Checklist-90-Revised (SCL-90-R) and Perceived Stress Scale were not clinically significant. In a secondary analysis of the data, we found gender differences in all the variables measured.
ConclusionsThe results of this study confirm the digital divide, with lower participation among people with a lower educational level. No association was observed between stress, anxiety or depression and cigarette consumption.
Conocer las características de los participantes en el programa online para dejar de fumar de la Universidad Nacional de Educación a Distancia (UNED).
MétodoSe analizaron las características demográficas, psicológicas y de consumo de tabaco de 23.763 fumadores, participantes en un programa on-line para dejar de fumar de la UNED. El programa de libre acceso estaba abierto a cualquier fumador, sin coste alguno y totalmente automatizado.
ResultadosEl 93,5% de los usuarios eran españoles, con igual porcentaje de participación entre hombres y mujeres. La media de edad fue de 39 años, casados y con estudios universitarios. Fumaban una media de 19,3 cigarrillos al día, con un nivel de dependencia medio de acuerdo con el Heaviness of Smoking Index. Las puntuaciones en las subescalas de ansiedad y depresión del Symptom Checklist-90-Revised (SCL-90-R) y en la Perceived Stress Scale no tienen significado clínico. En un análisis secundario de los datos se encontraron diferencias entre hombres y mujeres en todas las variables medidas.
ConclusiónSe constata la denominada brecha digital, con un menor número de participantes con bajo nivel cultural. No se observa relación entre estrés, ansiedad o depresión con consumo de cigarrillos.
The World Health Organization (WHO)1 informs that tobacco consumption causes 6.4 million deaths by lung cancer, cardiopathy, and other diseases. Europe and Americas have a similar number of deaths due to tobacco that rise up to 833,000 to 874,000 respectively.1 According to the Environment, Public Health, and Food Safety Committee of the European Parliament,2 in the European Union, 650,000 people die each year due to tobacco consumption. Not only are these institutions aware of the harmful effects of tobacco consumption, but also smokers. 70% of them would like to quit smoking; one half tries to quit each year, mostly without professional help.3 Of them, between 3% and 4% successfully quit smoking.4
A problem of this magnitude requires both effective and accessible treatments, thereby preventing millions of deaths worldwide,5 especially when treatments for tobacco dependence are available only for 14% of the world population. Many smokers do not want to or cannot receive conventional treatment.6 Internet could be an effective, accessible, and efficient alternative in such cases.7,8
Most studies about Internet smoking cessation programs were performed with English-speaking population in developed countries. On-line smoking cessation programs attract people between 30 and 40 years old, more females than males, married, with higher education, employed, and with a daily consumption of 19.3 cigarettes.9,10 However, with the exception of Barrera et al.,9 there are no studies with Spanish-speaking population, while more than 333 million people worldwide speak Spanish as their first language, 88% of them living in Latin America.11 According to the WHO,1 tobacco consumption increases in poor or developing countries, where 80% of smokers are concentrated, whereas it decreases in rich countries. For example, in countries like Peru, the rate of male smokers is greater than 50%; in Chile, Cuba or El Salvador, over 40%; and in Bolivia, Honduras, Nicaragua or Uruguay, over 30%12 versus 21.5% in the United States.13
There is a lack of research about the use of smoking cessation programs for Spanish language population due to the poor information about the characteristics of Spanish speaking participants in online programs for tobacco cessation. To overcome this needs, the present paper aims to describe the users’ characteristics of an Internet smoking cessation program provided in Spanish language and the relations among demographic, psychological and smoking characteristics.
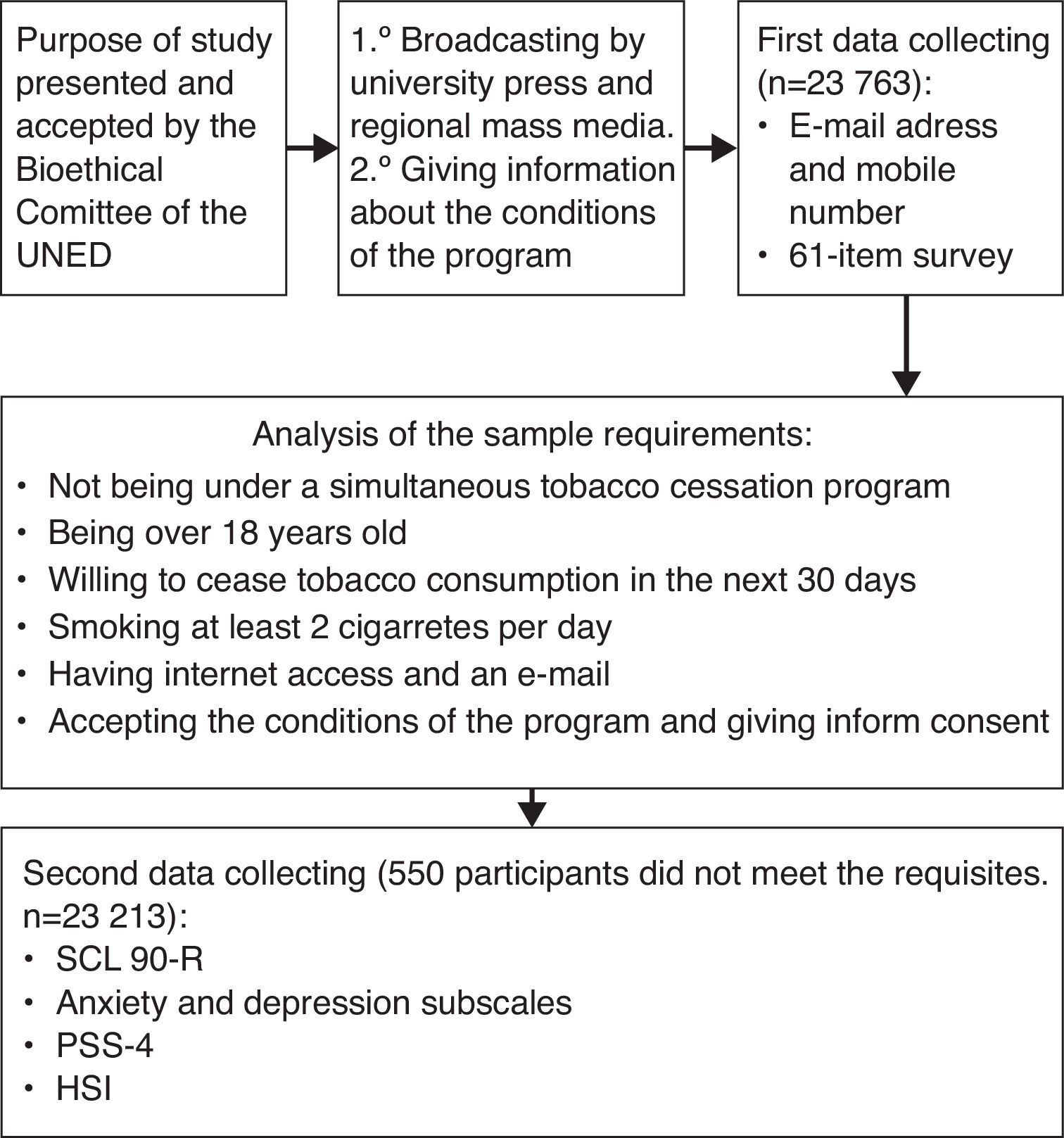
MethodsA descriptive non-experimental design was used to address the study aim. The program designed for the study is fully automated, free of charge, open, with direct access (as referral by a professional or health service was not required), and may be highly efficient in countries with few resources for smoking cessation. There were not economic incentives employed to participants and there was no direct contact with participants to confirm the data recorded.
The data analyzed in the study were obtained from the smoking cessation program website of the UNED (http://www.apsiol.uned.es/dejardefumar), from October 2009 until May 2010. In such a period of time, 23,763 users registered on the program, but only 23,213 people were considered in the final analysis because of the criteria established for the selection of the sample. To check if the participants meet the requirements, they underwent a 61-item survey about demographic, psychological and smoking variables, reporting information such as their age, gender, nationality, marital status, education and employment status. The entire process of data collecting and criteria is specified in the Figure 1.

Psychological measurement instruments previously used on-line14,15 were selected to avoid uncontrolled effects due to their use via Internet.16 Psychological variables were assessed by the following questionnaires: Symptom Checklist-90-Revised (SCL 90-R),17 Anxiety (AN) and Depression (DEP) subscales, and the Perceived Stress Scale of 4 items (PSS-4).18 The SCL 90-R is an adequate questionnaire to evaluate psychopathology in substance use disorders19 (Bergly, Nordfjærn and Hagen, 2014). The Spanish adaptation of SCL 90-R denotes high reliability with Cronbach's alpha coefficients fluctuating between 0.81 and 0.90.20 The PSS-4 is a reduced version of the 14-item Perceived Stress Scale. It measures the degree to which the respondent has perceived stressful situations during the past month. Higher scores are correlated to more stress. Although the four item PSS (PSS-4) has a moderate loss in internal reliability compared to the 14-item scale (r=0.60 vs r=0.85),21 the brevity of this instrument lends itself well to settings in which assessment time is limited.
Smoking variables were assessed by the Heaviness of Smoking Index (HIS),22,23 onset of smoking, physician's advice on smoking cessation, motivation to quit smoking, living with smokers and expectations of treatment success.
The HSI is a reduced 2-item version of the Fagerstrom Tolerance Questionnaire (FTQ).24 Nicotine dependence is categorized into a three-category variable: low (0–1), medium (2–4) and high (5–6). The HSI is used when time and resources are scarce.25
An alpha level of 0.05 was used for the statistical tests. Pearson correlation coefficient was used to relate the quantitative variables, and chi square for the categorical variables. The relation between categorical and quantitative variables was calculated with Student's t-test. Given the large sample size, some irrelevant differences may be statistically significant, and therefore we calculated the strength of the association through Cohen's d index for t-test and Cramer's V for χ2, according to Cohen's criteria.26 For Cohen's d, the small, medium, and large effect sizes are respectively 0.20, 0.50, and 0.80. For Cramer's V the small, medium, and large effect sizes are calculated from w index.27 For Pearson correlation coefficient, small, medium, and large effect sizes are respectively 0.10, 0.30, and 0.50.
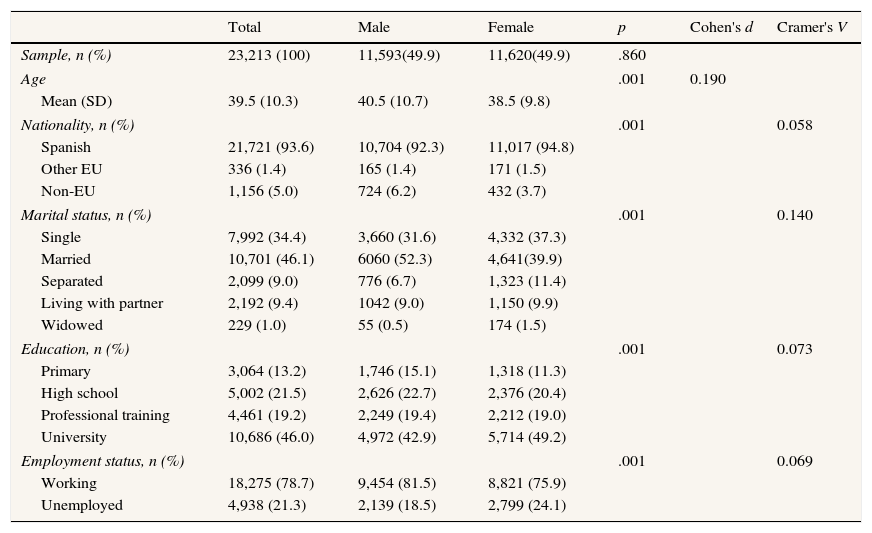
ResultsDemographic variables showed that more women registered for the treatment than men, 11,620 (50.1%) and 11,593 (49.9%) respectively, but this difference is not statistical significant, with a mean age of 39.5 years, most of them of medium economic level (64.6%), Spanish nationality (93.6%), married (46.1%), with university education (46%), and employed (78.7%). The percentage of non-European male participants was 1.7 times that of females, 6.2% and 3.7%, respectively (Table 1).
Users of the Internet smoking cessation program, 2009-2010. Demographic variables and sex differences.
| Total | Male | Female | p | Cohen's d | Cramer's V | |
|---|---|---|---|---|---|---|
| Sample, n (%) | 23,213 (100) | 11,593(49.9) | 11,620(49.9) | .860 | ||
| Age | .001 | 0.190 | ||||
| Mean (SD) | 39.5 (10.3) | 40.5 (10.7) | 38.5 (9.8) | |||
| Nationality, n (%) | .001 | 0.058 | ||||
| Spanish | 21,721 (93.6) | 10,704 (92.3) | 11,017 (94.8) | |||
| Other EU | 336 (1.4) | 165 (1.4) | 171 (1.5) | |||
| Non-EU | 1,156 (5.0) | 724 (6.2) | 432 (3.7) | |||
| Marital status, n (%) | .001 | 0.140 | ||||
| Single | 7,992 (34.4) | 3,660 (31.6) | 4,332 (37.3) | |||
| Married | 10,701 (46.1) | 6060 (52.3) | 4,641(39.9) | |||
| Separated | 2,099 (9.0) | 776 (6.7) | 1,323 (11.4) | |||
| Living with partner | 2,192 (9.4) | 1042 (9.0) | 1,150 (9.9) | |||
| Widowed | 229 (1.0) | 55 (0.5) | 174 (1.5) | |||
| Education, n (%) | .001 | 0.073 | ||||
| Primary | 3,064 (13.2) | 1,746 (15.1) | 1,318 (11.3) | |||
| High school | 5,002 (21.5) | 2,626 (22.7) | 2,376 (20.4) | |||
| Professional training | 4,461 (19.2) | 2,249 (19.4) | 2,212 (19.0) | |||
| University | 10,686 (46.0) | 4,972 (42.9) | 5,714 (49.2) | |||
| Employment status, n (%) | .001 | 0.069 | ||||
| Working | 18,275 (78.7) | 9,454 (81.5) | 8,821 (75.9) | |||
| Unemployed | 4,938 (21.3) | 2,139 (18.5) | 2,799 (24.1) | |||
EU: European Union; F: females; M: males.
In a secondary analysis of the demographic data we found sex differences: the females were younger, mean age 38.5 years versus 40.5 years in males, t(22,961)=14.37, p <0.001, Cohen's d=0.19. In the categorical variables, the greatest sex difference was observed in marital status, χ2(4, N=23,213)=454.35, p <0.001, Cramer's V=0.140, p <0.001. There were more married men (52.3%) than women (39.9%) and fewer separated men (6.7%) than women (11.4%). There were more women (49.2%) with university education than men (42.9%), in contrast to primary education (11.3% vs. 15.1% for women and men, respectively), χ2(3, N=23,213)=124.08, p <0.001, Cramer's V=0.073. Job situation revealed the third largest difference: There were more employed men than women (81.5% vs. 75.9% for men and women, respectively), χ2(1, N=23.213)=110.11, p <0.001, Cramer's V=0.069 (Table 1).
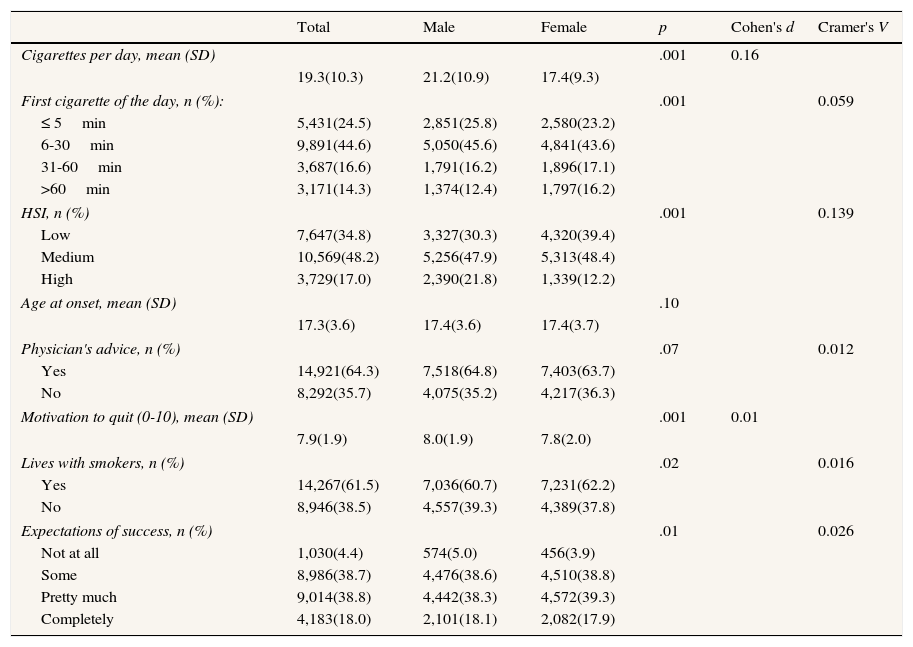
The second part of the analysis of the results, focused on smoking variables revealing the program users’ mean daily tobacco consumption was 19.3 cigarettes. Most participants smoked within the first half hour upon waking up. According to the HIS18 nicotine dependence was medium in 48.2% of participants and low in 34.8%. Age at onset of consumption was 17 years. Of the participants, 64.3% had received medical advice to quit smoking —almost twice as many as the 35.7% of those who had not. Level of motivation for abstinence was high, and expectations of success were positive (Table 2).
Users of the Internet smoking cessation program, 2009-2010. Smoking variables and sex differences.
| Total | Male | Female | p | Cohen's d | Cramer's V | |
|---|---|---|---|---|---|---|
| Cigarettes per day, mean (SD) | .001 | 0.16 | ||||
| 19.3(10.3) | 21.2(10.9) | 17.4(9.3) | ||||
| First cigarette of the day, n (%): | .001 | 0.059 | ||||
| ≤ 5min | 5,431(24.5) | 2,851(25.8) | 2,580(23.2) | |||
| 6-30min | 9,891(44.6) | 5,050(45.6) | 4,841(43.6) | |||
| 31-60min | 3,687(16.6) | 1,791(16.2) | 1,896(17.1) | |||
| >60min | 3,171(14.3) | 1,374(12.4) | 1,797(16.2) | |||
| HSI, n (%) | .001 | 0.139 | ||||
| Low | 7,647(34.8) | 3,327(30.3) | 4,320(39.4) | |||
| Medium | 10,569(48.2) | 5,256(47.9) | 5,313(48.4) | |||
| High | 3,729(17.0) | 2,390(21.8) | 1,339(12.2) | |||
| Age at onset, mean (SD) | .10 | |||||
| 17.3(3.6) | 17.4(3.6) | 17.4(3.7) | ||||
| Physician's advice, n (%) | .07 | 0.012 | ||||
| Yes | 14,921(64.3) | 7,518(64.8) | 7,403(63.7) | |||
| No | 8,292(35.7) | 4,075(35.2) | 4,217(36.3) | |||
| Motivation to quit (0-10), mean (SD) | .001 | 0.01 | ||||
| 7.9(1.9) | 8.0(1.9) | 7.8(2.0) | ||||
| Lives with smokers, n (%) | .02 | 0.016 | ||||
| Yes | 14,267(61.5) | 7,036(60.7) | 7,231(62.2) | |||
| No | 8,946(38.5) | 4,557(39.3) | 4,389(37.8) | |||
| Expectations of success, n (%) | .01 | 0.026 | ||||
| Not at all | 1,030(4.4) | 574(5.0) | 456(3.9) | |||
| Some | 8,986(38.7) | 4,476(38.6) | 4,510(38.8) | |||
| Pretty much | 9,014(38.8) | 4,442(38.3) | 4,572(39.3) | |||
| Completely | 4,183(18.0) | 2,101(18.1) | 2,082(17.9) | |||
F: females; HIS: Heaviness of Smoking Index; M: males.
In subsequent analysis, significant sex differences in cigarette consumption were observed: men smoked 3.8 more cigarettes per day (95%CI: 3.5-4.1), they smoked their first cigarette of the day sooner (noticeable in higher percentages of men smoking within the first 30minutes after waking up and women tending to do it 30 to 60minutes later), and their level of physical dependence on nicotine was higher. More women were living with other smokers, and their expectations of success were higher (Table 2).
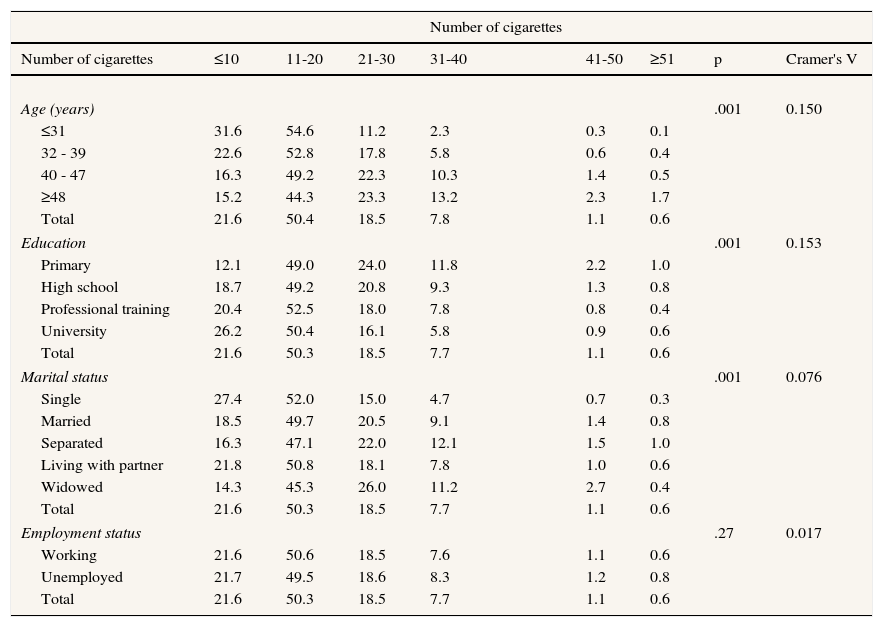
We verified that consumption increases with age, lower educational level, and in the case of separated people and widowers (Table 3), with medium effect sizes for age and education, and a small one for marital status. Results in Table 3 are consistent with results in Table 2, revealing in both cases a mean of cigarettes per day between 11 to 20 in all of the groups considered.
Users of the Internet smoking cessation program, 2009-2010. Percentage of users according to number of cigarettes smoked and demographic variables.
| Number of cigarettes | ||||||||
|---|---|---|---|---|---|---|---|---|
| Number of cigarettes | ≤10 | 11-20 | 21-30 | 31-40 | 41-50 | ≥51 | p | Cramer's V |
| Age (years) | .001 | 0.150 | ||||||
| ≤31 | 31.6 | 54.6 | 11.2 | 2.3 | 0.3 | 0.1 | ||
| 32 - 39 | 22.6 | 52.8 | 17.8 | 5.8 | 0.6 | 0.4 | ||
| 40 - 47 | 16.3 | 49.2 | 22.3 | 10.3 | 1.4 | 0.5 | ||
| ≥48 | 15.2 | 44.3 | 23.3 | 13.2 | 2.3 | 1.7 | ||
| Total | 21.6 | 50.4 | 18.5 | 7.8 | 1.1 | 0.6 | ||
| Education | .001 | 0.153 | ||||||
| Primary | 12.1 | 49.0 | 24.0 | 11.8 | 2.2 | 1.0 | ||
| High school | 18.7 | 49.2 | 20.8 | 9.3 | 1.3 | 0.8 | ||
| Professional training | 20.4 | 52.5 | 18.0 | 7.8 | 0.8 | 0.4 | ||
| University | 26.2 | 50.4 | 16.1 | 5.8 | 0.9 | 0.6 | ||
| Total | 21.6 | 50.3 | 18.5 | 7.7 | 1.1 | 0.6 | ||
| Marital status | .001 | 0.076 | ||||||
| Single | 27.4 | 52.0 | 15.0 | 4.7 | 0.7 | 0.3 | ||
| Married | 18.5 | 49.7 | 20.5 | 9.1 | 1.4 | 0.8 | ||
| Separated | 16.3 | 47.1 | 22.0 | 12.1 | 1.5 | 1.0 | ||
| Living with partner | 21.8 | 50.8 | 18.1 | 7.8 | 1.0 | 0.6 | ||
| Widowed | 14.3 | 45.3 | 26.0 | 11.2 | 2.7 | 0.4 | ||
| Total | 21.6 | 50.3 | 18.5 | 7.7 | 1.1 | 0.6 | ||
| Employment status | .27 | 0.017 | ||||||
| Working | 21.6 | 50.6 | 18.5 | 7.6 | 1.1 | 0.6 | ||
| Unemployed | 21.7 | 49.5 | 18.6 | 8.3 | 1.2 | 0.8 | ||
| Total | 21.6 | 50.3 | 18.5 | 7.7 | 1.1 | 0.6 | ||
Last phase of the analysis of the results considered the psychological variables: mean scores in anxiety, depression and stress were not clinically significant. In a secondary analysis of the data, women scored significantly higher than men on all the scales. As for anxiety, women obtained a mean of 0.67 (SD=0.65) versus 0.50 (SD=0.54) in men (95%CI: 0.16-0.19), t(22,961)=-14.37, p <0.001, Cohen's d=0.30. Regarding depression, the mean of women was 0.87 (SD=0.78) versus 0.66 (SD=0.67) in men (95%CI: 0.19- 0.23), t(23,211)=-22.34, p <0.001, Cohen's d=0.29. About stress, women had a mean score of 9.46 (SD=2.96) versus 9.11 (SD=2.86) in men (95%CI: 0.28- 0.43), t(22,961)=-9.19, p <0.001, Cohen's d=0.12.
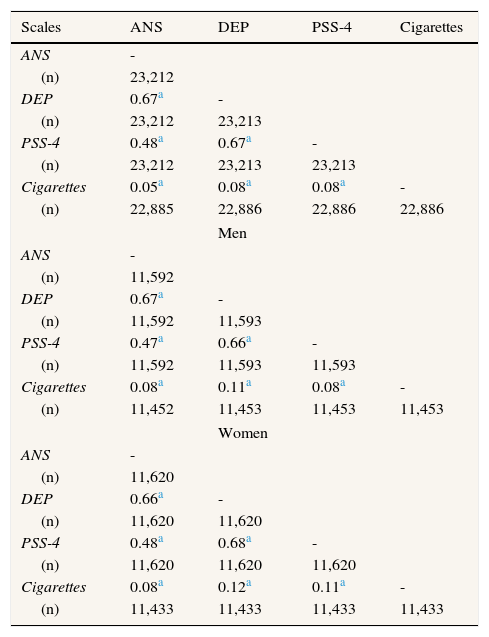
The relation between cigarette consumption and the psychological variables was statistically significant, but with an insignificant effect size. By sex, small effect sizes were observed in men in the DEP subscale, and insignificant ones in the rest of the scales. In women, small effect sizes were observed in the DEP subscale and the PSS-4, and insignificant ones in the ANS subscale (Table 4).
Users of the Internet smoking cessation program, 2009-2010. Pearson correlations (general and by sex) between psychological variables and number of cigarettes smoked.
| Scales | ANS | DEP | PSS-4 | Cigarettes |
|---|---|---|---|---|
| ANS | - | |||
| (n) | 23,212 | |||
| DEP | 0.67a | - | ||
| (n) | 23,212 | 23,213 | ||
| PSS-4 | 0.48a | 0.67a | - | |
| (n) | 23,212 | 23,213 | 23,213 | |
| Cigarettes | 0.05a | 0.08a | 0.08a | - |
| (n) | 22,885 | 22,886 | 22,886 | 22,886 |
| Men | ||||
| ANS | - | |||
| (n) | 11,592 | |||
| DEP | 0.67a | - | ||
| (n) | 11,592 | 11,593 | ||
| PSS-4 | 0.47a | 0.66a | - | |
| (n) | 11,592 | 11,593 | 11,593 | |
| Cigarettes | 0.08a | 0.11a | 0.08a | - |
| (n) | 11,452 | 11,453 | 11,453 | 11,453 |
| Women | ||||
| ANS | - | |||
| (n) | 11,620 | |||
| DEP | 0.66a | - | ||
| (n) | 11,620 | 11,620 | ||
| PSS-4 | 0.48a | 0.68a | - | |
| (n) | 11,620 | 11,620 | 11,620 | |
| Cigarettes | 0.08a | 0.12a | 0.11a | - |
| (n) | 11,433 | 11,433 | 11,433 | 11,433 |
ANS: Anxiety subscale of the SCL-90-R; DEP: Depression subscale of the SCL-90-R; PSS-4=4-item Perceived Stress Scale.
This study shows the main characteristics of the Spanish smoker who want to quit smoking. A medium nicotine dependence, a mean of 19.3 cigarettes and small differences in other variables. Another aspect of interest, is the lack of clinical significance of the emotional measures: anxiety, depression or stress perception. Finally, there is not relationship between the tobacco consumption and anxiety, depression or stress. This aspect has a special importance because there is a general belief about the tobacco as anxiety reduction or as a way to coping with emotional negative states.
The UNED on-line smoking cessation program was fully automated, free of charge, and directly accessible to any smoker who wanted to quit smoking within the next 30 days after initiating treatment. The high number of enrollment shows that, in Spain, Internet smoking cessation programs are accessible to a large number of smokers, especially compared with conventional programs. The results of the UNED on-line smoking cessation program has been published elsewhere.28
The demographic and smoking characteristics obtained in this study are similar to those reported in other Internet smoking cessation programs9,10 except for sex; in the UNED program, the number of males and females was not significantly different, whereas in most other studies, females are majority. This may be due to the fact that in the mentioned studies, the sample and their sizes are different, ranging from 351 to 17,159 subjects.9 With larger samples, as in the case of Barrera et al.,9 the percentages of men and women are almost the same (49.3% men versus 50.7% women). The only difference found in the sample related to sex distribution, refers to non–European users, where men's participation was almost twice that of women's. We can assume that non-Europeans users (1,156) are mainly people from Latin American countries living in Spain, since the program was provided only in Spanish language and announced through national and regional mass media. Except for Spaniards, we did not register the nationality of each user, but just European or non- European nationality was reported. Despite the fact that there has been an increase in female tobacco consumption in recent years, the proportion of male smokers triples or quadruples that of women in countries such as Ecuador, El Salvador, Guatemala, Honduras, Mexico, Nicaragua, Paraguay, or Peru.12
There are no main differences between sex and smoking variables in studies based on general population. In such cases, women and men are equally likely to quit smoking successfully.29
The percentage of users with university education versus other categories is noteworthy, confirming the existence of digital divide also in the specific field of e-health. In Spain, the percentage of people with higher education in 2009 was 16.29% versus 20.22% with primary education. However, that same year, the percentage of Internet users with higher education was 28.34% versus 7.85% with primary education.30 Therefore, we confirm that smoking cessation programs are similar to other e-health programs in this aspect: subjects with less digital literacy, who are normally those with a lower educational level, are under-represented.31 Moreover, a higher ability to understand, organize, and analyze written information is required for the use of on-line programs compared to the traditional face-to-face intervention. All of this has a dissuasive effect on subjects with a lower educational level. It has also been suggested that the excessive length of the written material employed in self-help formats can hinder their use, especially in smokers who are not accustomed to dealing with this type of information.32
In this study, we confirmed significant sex differences in cigarette consumption. Women consume fewer cigarettes, smoke the first cigarette of the day later, and are less dependent on nicotine. Since a high level of nicotine dependence impairs abstinence, women can be expected to obtain better results than men in smoking cessation programs. Paradoxically, till now, the evidence indicated the opposite.33 It has been suggested that perception of the risks of smoking cessation, such as weight increase, negative mood, or a strong desire to smoke may affect women undergoing treatment more than men,34 and as a consequence, women achieve worse results.
Concerning psychological scale scores, the results do not differ from those obtained in other studies, both in general population14,20 and smoking population.35 In spite of the fact that cigarette consumption has been associated with higher levels of anxiety, depression and stress,36 in this study, the correlation was no significant or small, with a larger effect in women. The subjects studied are not a clinical sample, in terms of psychological or physical health, but they receive in a high percentage (64.3%) the physician advice to quit smoking, lower than the obtained in overweight or obese smokers without diabetes (72.8%),37 considered as groups at high risk.
The woman has higher scores in anxiety and depression than men. In spite of this scores are normal and it does not show any clinical interest, this outcome is consistent with other research that shows a relationship between emotional disorders in women and tobacco consumption.38
The poor participation of the subjects with lower educational level suggests the need to develop a more accessible and user-friendly format in the smoking program, which might help to motivate to this group of subjects and to reduce the digital divide.
One of the limitations of the study refers to the data registered by the website program users, the information obtained was not confirmed by other means as reports of significant people close to the participant or chemical measures of smoking. In addition, Spanish smokers were over-represented in the sample, so the results are not fully generalizable to other Spanish-speaking countries, but there is a representation of other Spanish speaking countries that makes it possible to establish a comparison.
The main strength of this study is the number of participants. 23,700 people wide distributed, are more than a sample. People, who are looking for an aid to quit smoking, visit this Web which does not have any monetary, advertising, cultural or political interest. The university prestige guarantee the data obtained and the results discussed above. This argument encourages Internet interventions related to health (prevention and treatment) from public institutions. Public health should be allied with internet and related technologies to provide everybody an opportunity to improve their health.
Most studies about Internet smoking cessation programs were performed with English-speaking population in developed countries. There is a lack of research about the use of smoking cessation programs for Spanish language population.
What does this study add to the literature?There are an equal percentage of participation in men and women. A mean age 39 years. They smoked a mean of 19.3 cigarettes per day, showing mid-range level of nicotine dependence. No relation of stress, anxiety or depression wit cigarette consumption was observed.
Mª José López.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsG. Mañanes and M.A. Vallejo designed the study. Both authors were involved in data analysis and interpretation. L. Vallejo-Slocker carried out the statistical analysis, conducted the literature searches and wrote the first draft of the manuscript. All results were discussed among the authors. All authors contributed to and have approved the final manuscript.
FundingThis research was supported by a grant of the Spanish Ministry of Science and Technology (grant ID# I+D+I SEJ2004-03392/PSI).
Conflicts of interestNone.











