



Social vulnerability implies a higher risk of induced abortion (IA). Immigrant status could be an additional factor. The objective was to identify the patterns surrounding which women resort to IAs, and to study the relationship between socio-economic and health system factors. Another aim was to determine the relationship between the patterns identified and the immigrant's country.
MethodsA cross-sectional study was performed including all IAs notified during 2006 on women residing in three Spanish autonomous communities (the Balearic Islands, Catalonia and Comunitat Valenciana). We used sociodemographic, nationality and related variables, reproductive history and use of health services. A Categorical Principal Component Analysis was used to summarize the information and to identify profiles.
ResultsMore than a third of IAs were performed on non-Spanish women. Four dimensions have been determined that define the profile of women resorting to IAs: age, reproductive history and marital status; type of health services used; social level; and earlier or late IA and its repetitive use. Age and related factors were important determinants. Economic status and knowledge of the health system were related to access to contraception and IA information. Spanish, Western European and South American women had a higher social level than Romanian and African women. Late IA use and a lower recurrence characterised Asian, North African and Spanish women.
ConclusionDifferences on IA use between groups of different women seem to be related to vulnerability (economic, social, knowledge and use of healthcare services). There is a different situation among immigrants of differing nationalities.
La vulnerabilidad social representa un riesgo de interrupción voluntaria del embarazo (IVE). La inmigración puede ser un factor adicional. Se pretendía identificar patrones que caracterizaran a las mujeres que abortan y estudiar la relación con factores socioeconómicos y de atención sanitaria. Otro objetivo fue determinar la relación entre los patrones identificados y el origen de las inmigrantes.
MétodosSe realizó un estudio transversal incluyendo todas las IVE notificadas durante 2006 a tres registros de IVE de comunidades autónomas: Illes Balears, Catalunya y Comunitat Valenciana. Se utilizaron variables sociodemográficas, de nacionalidad y relacionadas, historia reproductiva y de utilización de servicios sanitarios. Se realizó un análisis de componentes principales categórico para resumir la información e identificar perfiles.
ResultadosLas inmigrantes representaron más de un tercio de las IVE. Cuatro dimensiones definieron el perfil de las mujeres que abortan: edad, historia reproductiva y estado civil; utilización de servicios públicos o privados; nivel social; IVE tardía o precoz y su recurrencia. Edad y factores relacionados fueron determinantes importantes. El nivel económico y el conocimiento del sistema sanitario estaban relacionados con el acceso a la anticoncepción y a la información sobre IVE. Españolas, europeas occidentales y latinoamericanas tenían mayor nivel social que rumanas y africanas. El uso tardío de la IVE y una menor recurrencia fue característico de españolas, norteafricanas y asiáticas.
ConclusiónLas diferencias en el recurso a la IVE entre grupos de mujeres parecen relacionarse con la vulnerabilidad (económica, social, de conocimiento y uso del sistema sanitario). La situación varía entre inmigrantes de diferentes nacionalidades.
In order to understand the induced abortion (IA) phenomenon, health service related factors as well as social factors need to be looked at. There are factors that strongly influence the probability of having an IA including age, the prospect of single parenthood and high parity, but there are also others such as the woman's housing situation, previous abortion history, attitudes towards abortion and occupational status.1 A low educational level, weak social networks, poverty, unemployment, and difficult access to the healthcare system are factors related to vulnerable social groups, and those women from these groups and low socio-economic status are exposed to a higher risk of IA.2
Immigration could be an additional factor for IA. Immigration, mainly of an economic nature, is an understudied factor in southern European countries with regard to IA because it is a recent phenomenon. For immigrant women, the risk would not necessarily be associated with cultural factors, but rather with their belonging to vulnerable groups.3 In some European countries4–7 the IA rates among immigrant women are higher than for autochthonous women, and it is also possible to distinguish differences depending on the nationality of the migrant.
In Spain, IA has been legal since 1985 in three cases (risk to the mother's health, risk of fetal malformation, and rape). Since then, there have been a small number of studies of IA, but most of them have emphasized the relevance of social factors8–10 and there are very few studies relating immigration to IA in Spain.11–13 The aim of this study is to identify the socio-economic and health-system related patterns surrounding which women resort to IAs in three Spanish autonomous communities and where immigration plays an important role. Finally, we want to determine the relationship between the patterns identified and the nationalities of the immigrants.
MethodsDesign and study populationWith a cross-sectional study design, we include all IAs performed during 2006 on women residing in three Spanish autonomous communities: the Balearic Islands (IA=3,108), Catalonia (IA=20,058) and the Comunitat Valenciana (IA=10,024). These three regions cover 30% of the Spanish population (12,942,667 inhabitants; 2,842,057 women within reproductive age) and 42% of foreigners living in Spain in 2006.14
Source of informationThe IAs accounted for have been reported by authorized centres to the IA Registries (IA notification is mandatory in Spain) and data proceeding from the official form. Variables selected (categories of variables are shown in Tables 1 and 2) were: living in a couple (cohabitant), marital status, family planning attendance in the last two years (including the type of family planning centre: private, public or others), type of information centre about IA (private, public or other), age, education, work status, number of prior IAs, number of living children, years since their last delivery, gestational weeks, province of residence, nationality (country: grouped as Spain, Western Europe, Romania, Eastern Europe, North Africa, other African countries, Bolivia, Ecuador plus Colombia, other American countries, Asia plus Oceania, and «not available») and, when appropriate, the year of arrival in Spain. Nationalities were grouped by continents and, inside of them, by geographic regions or countries with regard to the number of women.
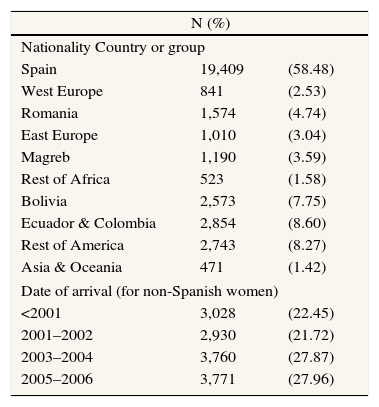
Number of women who resort to IA in Catalonia, the Balearic Islands and Comunitat Valenciana (Spain) by nationality and date of arrival
| N (%) | ||
| Nationality Country or group | ||
| Spain | 19,409 | (58.48) |
| West Europe | 841 | (2.53) |
| Romania | 1,574 | (4.74) |
| East Europe | 1,010 | (3.04) |
| Magreb | 1,190 | (3.59) |
| Rest of Africa | 523 | (1.58) |
| Bolivia | 2,573 | (7.75) |
| Ecuador & Colombia | 2,854 | (8.60) |
| Rest of America | 2,743 | (8.27) |
| Asia & Oceania | 471 | (1.42) |
| Date of arrival (for non-Spanish women) | ||
| <2001 | 3,028 | (22.45) |
| 2001–2002 | 2,930 | (21.72) |
| 2003–2004 | 3,760 | (27.87) |
| 2005–2006 | 3,771 | (27.96) |
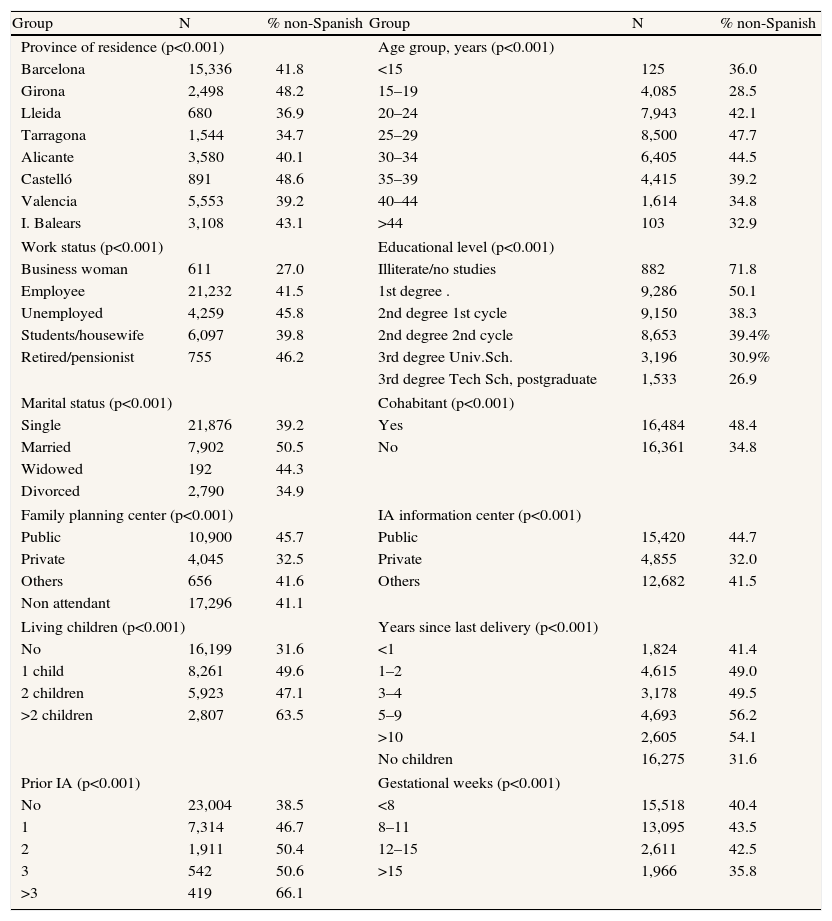
Number of IA (and percent in non-Spanish born women) in Catalonia, the Balearic Islands and Comunitat Valenciana (Spain) by category of variable (with p value)
| Group | N | % non-Spanish | Group | N | % non-Spanish |
| Province of residence (p<0.001) | Age group, years (p<0.001) | ||||
| Barcelona | 15,336 | 41.8 | <15 | 125 | 36.0 |
| Girona | 2,498 | 48.2 | 15–19 | 4,085 | 28.5 |
| Lleida | 680 | 36.9 | 20–24 | 7,943 | 42.1 |
| Tarragona | 1,544 | 34.7 | 25–29 | 8,500 | 47.7 |
| Alicante | 3,580 | 40.1 | 30–34 | 6,405 | 44.5 |
| Castelló | 891 | 48.6 | 35–39 | 4,415 | 39.2 |
| Valencia | 5,553 | 39.2 | 40–44 | 1,614 | 34.8 |
| I. Balears | 3,108 | 43.1 | >44 | 103 | 32.9 |
| Work status (p<0.001) | Educational level (p<0.001) | ||||
| Business woman | 611 | 27.0 | Illiterate/no studies | 882 | 71.8 |
| Employee | 21,232 | 41.5 | 1st degree . | 9,286 | 50.1 |
| Unemployed | 4,259 | 45.8 | 2nd degree 1st cycle | 9,150 | 38.3 |
| Students/housewife | 6,097 | 39.8 | 2nd degree 2nd cycle | 8,653 | 39.4% |
| Retired/pensionist | 755 | 46.2 | 3rd degree Univ.Sch. | 3,196 | 30.9% |
| 3rd degree Tech Sch, postgraduate | 1,533 | 26.9 | |||
| Marital status (p<0.001) | Cohabitant (p<0.001) | ||||
| Single | 21,876 | 39.2 | Yes | 16,484 | 48.4 |
| Married | 7,902 | 50.5 | No | 16,361 | 34.8 |
| Widowed | 192 | 44.3 | |||
| Divorced | 2,790 | 34.9 | |||
| Family planning center (p<0.001) | IA information center (p<0.001) | ||||
| Public | 10,900 | 45.7 | Public | 15,420 | 44.7 |
| Private | 4,045 | 32.5 | Private | 4,855 | 32.0 |
| Others | 656 | 41.6 | Others | 12,682 | 41.5 |
| Non attendant | 17,296 | 41.1 | |||
| Living children (p<0.001) | Years since last delivery (p<0.001) | ||||
| No | 16,199 | 31.6 | <1 | 1,824 | 41.4 |
| 1 child | 8,261 | 49.6 | 1–2 | 4,615 | 49.0 |
| 2 children | 5,923 | 47.1 | 3–4 | 3,178 | 49.5 |
| >2 children | 2,807 | 63.5 | 5–9 | 4,693 | 56.2 |
| >10 | 2,605 | 54.1 | |||
| No children | 16,275 | 31.6 | |||
| Prior IA (p<0.001) | Gestational weeks (p<0.001) | ||||
| No | 23,004 | 38.5 | <8 | 15,518 | 40.4 |
| 1 | 7,314 | 46.7 | 8–11 | 13,095 | 43.5 |
| 2 | 1,911 | 50.4 | 12–15 | 2,611 | 42.5 |
| 3 | 542 | 50.6 | >15 | 1,966 | 35.8 |
| >3 | 419 | 66.1 | |||
The data are complete for most of the cases, only 2.8% of IA notifications had any missing value.
Statistical analysisWe started with a bivariate analysis, performing a chi-square test to check the differences between all variables comparing Spanish and non-Spanish women
Categorical Principal Component Analysis (CATPCA)15 was used to summarize the information because of the categorical nature of variables. This technique provides an optimal quantification for each category of the variables analysed, giving them metric properties that will allow us to calculate distances between individuals or correlations between variables. The linear combinations of the quantified variables with the most explained variance were derived. The original categorical variables were summarised in several numerical variables, every one of them representing the patterns that best explain the variability.
We consider as relevant dimensions those with an eigenvalue (measure of explained variance) higher than 1 unit.16 This means retaining in the analysis those dimensions having an explanatory power greater than that of a variable uncorrelated with all the others included. To interpret every dimension, we only consider those variables with a contribution higher than 10% of the eigenvalue, the remaining variables being considered as not relevant.
«Nationality», «number of years since arriving in Spain» (for immigrants) and «province of residence» have been included in a secondary step as supplementary variables as we did not want these variables to determine the social pattern of women demanding IAs, but rather we wanted to see the relation of these variables with the patterns arising from the analysis. Thus, groups of women have been projected on the axis according to their nationalities, dates of arrival in Spain and provinces of residence in order to characterize the determinants of these groups.
ResultsMore than a third of the IAs in 2006 in the territory studied (Table 1) were performed on non-Spanish women (from 34.7% in Tarragona to 48.6% in Castelló). Differences between Spanish and non-Spanish women were statistically significant (p<0.01) for all the variables (Table 2).
Four dimensions yielded an eigenvalue higher than 1 unit. The percentage of variance explained by the four axes altogether is 64.39% (for each axis, respectively, 28.26%, 15.97%, 10.47%, and 9.69%). The dimensions extracted enable the profiling of women who undergo an IA.
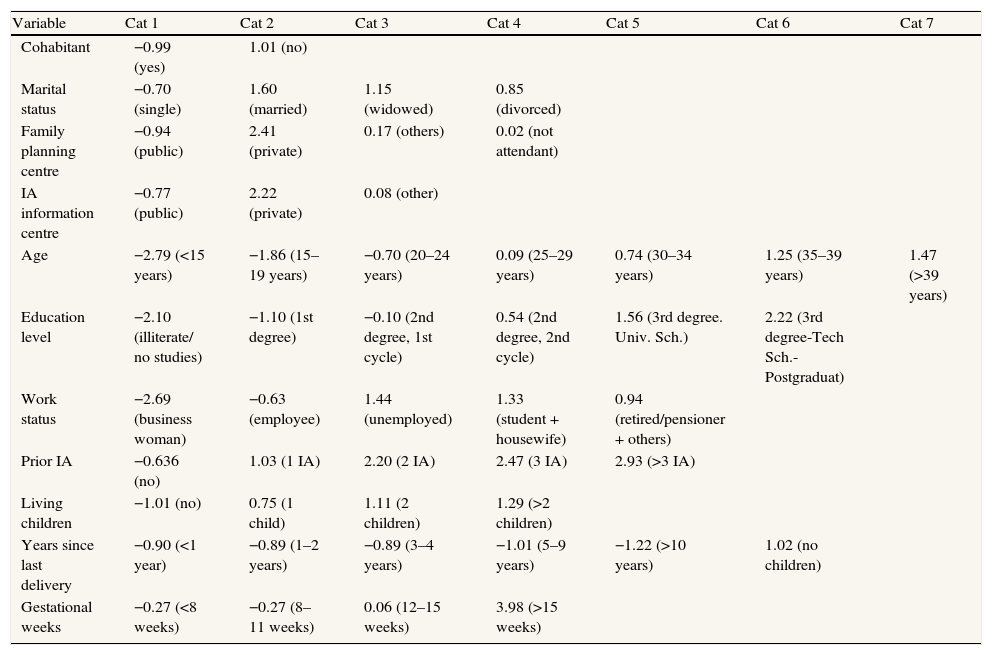
Table 3 shows the quantification for each category variable obtained by CATPCA. With regard to marital status, Table 3 indicates that singles show quite different behaviour from other categories. For «centre for family planning» and «information centre», we can see that public centres are clearly different from private, but other types of centres, or their absence, belong to less defined patterns. Regarding the variable «work status», there are qualitative differences between women with paid jobs and the other categories. Women without any previous children have different behaviour from the other women. Finally, women with more than 15 gestational weeks for IA have different characteristics than the rest.
Category quantifications
| Variable | Cat 1 | Cat 2 | Cat 3 | Cat 4 | Cat 5 | Cat 6 | Cat 7 |
| Cohabitant | −0.99 (yes) | 1.01 (no) | |||||
| Marital status | −0.70 (single) | 1.60 (married) | 1.15 (widowed) | 0.85 (divorced) | |||
| Family planning centre | −0.94 (public) | 2.41 (private) | 0.17 (others) | 0.02 (not attendant) | |||
| IA information centre | −0.77 (public) | 2.22 (private) | 0.08 (other) | ||||
| Age | −2.79 (<15 years) | −1.86 (15–19 years) | −0.70 (20–24 years) | 0.09 (25–29 years) | 0.74 (30–34 years) | 1.25 (35–39 years) | 1.47 (>39 years) |
| Education level | −2.10 (illiterate/ no studies) | −1.10 (1st degree) | −0.10 (2nd degree, 1st cycle) | 0.54 (2nd degree, 2nd cycle) | 1.56 (3rd degree. Univ. Sch.) | 2.22 (3rd degree-Tech Sch.-Postgraduat) | |
| Work status | −2.69 (business woman) | −0.63 (employee) | 1.44 (unemployed) | 1.33 (student + housewife) | 0.94 (retired/pensioner + others) | ||
| Prior IA | −0.636 (no) | 1.03 (1 IA) | 2.20 (2 IA) | 2.47 (3 IA) | 2.93 (>3 IA) | ||
| Living children | −1.01 (no) | 0.75 (1 child) | 1.11 (2 children) | 1.29 (>2 children) | |||
| Years since last delivery | −0.90 (<1 year) | −0.89 (1–2 years) | −0.89 (3–4 years) | −1.01 (5–9 years) | −1.22 (>10 years) | 1.02 (no children) | |
| Gestational weeks | −0.27 (<8 weeks) | −0.27 (8–11 weeks) | 0.06 (12–15 weeks) | 3.98 (>15 weeks) |
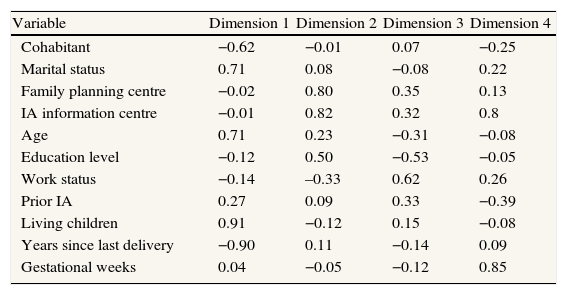
Table 4 shows the variable weights for each dimension according to the CATPCA. We represent in bold the values with a contribution higher than 10% of the total variability explained by each axis.
Variable weights for each dimension
| Variable | Dimension 1 | Dimension 2 | Dimension 3 | Dimension 4 |
| Cohabitant | −0.62 | −0.01 | 0.07 | −0.25 |
| Marital status | 0.71 | 0.08 | −0.08 | 0.22 |
| Family planning centre | −0.02 | 0.80 | 0.35 | 0.13 |
| IA information centre | −0.01 | 0.82 | 0.32 | 0.8 |
| Age | 0.71 | 0.23 | −0.31 | −0.08 |
| Education level | −0.12 | 0.50 | −0.53 | −0.05 |
| Work status | −0.14 | –0.33 | 0.62 | 0.26 |
| Prior IA | 0.27 | 0.09 | 0.33 | −0.39 |
| Living children | 0.91 | −0.12 | 0.15 | −0.08 |
| Years since last delivery | −0.90 | 0.11 | −0.14 | 0.09 |
| Gestational weeks | 0.04 | −0.05 | −0.12 | 0.85 |
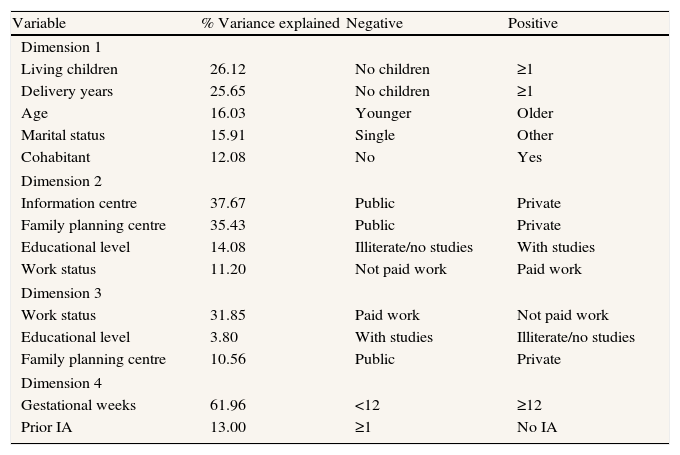
Table 5 provides, for each dimension, the relationship between the extremes of each axis with the variables that contribute most to it (those in bold in Table 4). The orientation of every variable in every dimension in Table 5 has been determined as the product of the quantifications of every variable by the weight of the corresponding dimension. Dimensions are ordered by their importance with regard to the variance that they explain, and variables for every dimension are ordered from higher to lower according to their contribution to the axis. At every dimension the percentage of variance explained for every variable is also shown in Table 5.
Dimensions
| Variable | % Variance explained | Negative | Positive |
| Dimension 1 | |||
| Living children | 26.12 | No children | ≥1 |
| Delivery years | 25.65 | No children | ≥1 |
| Age | 16.03 | Younger | Older |
| Marital status | 15.91 | Single | Other |
| Cohabitant | 12.08 | No | Yes |
| Dimension 2 | |||
| Information centre | 37.67 | Public | Private |
| Family planning centre | 35.43 | Public | Private |
| Educational level | 14.08 | Illiterate/no studies | With studies |
| Work status | 11.20 | Not paid work | Paid work |
| Dimension 3 | |||
| Work status | 31.85 | Paid work | Not paid work |
| Educational level | 3.80 | With studies | Illiterate/no studies |
| Family planning centre | 10.56 | Public | Private |
| Dimension 4 | |||
| Gestational weeks | 61.96 | <12 | ≥12 |
| Prior IA | 13.00 | ≥1 | No IA |
For the first axis, on the negative-sign side are women who are younger, childless, single, and not cohabiting. At the positive sign side are women with opposite characteristics. The main characteristic of this axis is related to age, reproductive history and marital status. It can be labelled using «age» as a synthetic term.
In the second axis, on one side we see women who attend public centres for information about contraception, are illiterate and have paid work. At the other extreme are women who attend private health centres, have studied and without paid jobs. The variables contributing the most are «type of information centre» and «type of contraception centre» and it is possible to classify the women with regard to their use of public health facilities.
The third axis distinguishes educated women with paid work who use public centres for contraception as opposed to illiterate women without paid work who use private centres. Because the contribution of «type of centre» is lower, the main characteristic of this axis can be labelled as the social level.
Finally, in the fourth axis we can see on one side women with lower than twelve gestational weeks and with prior IAs, and on the other side women with opposite characteristics. Our interpretation is that the axis distinguishes women with earlier IA and occasional recourse to it from women with late IA and more repetitive use of it.
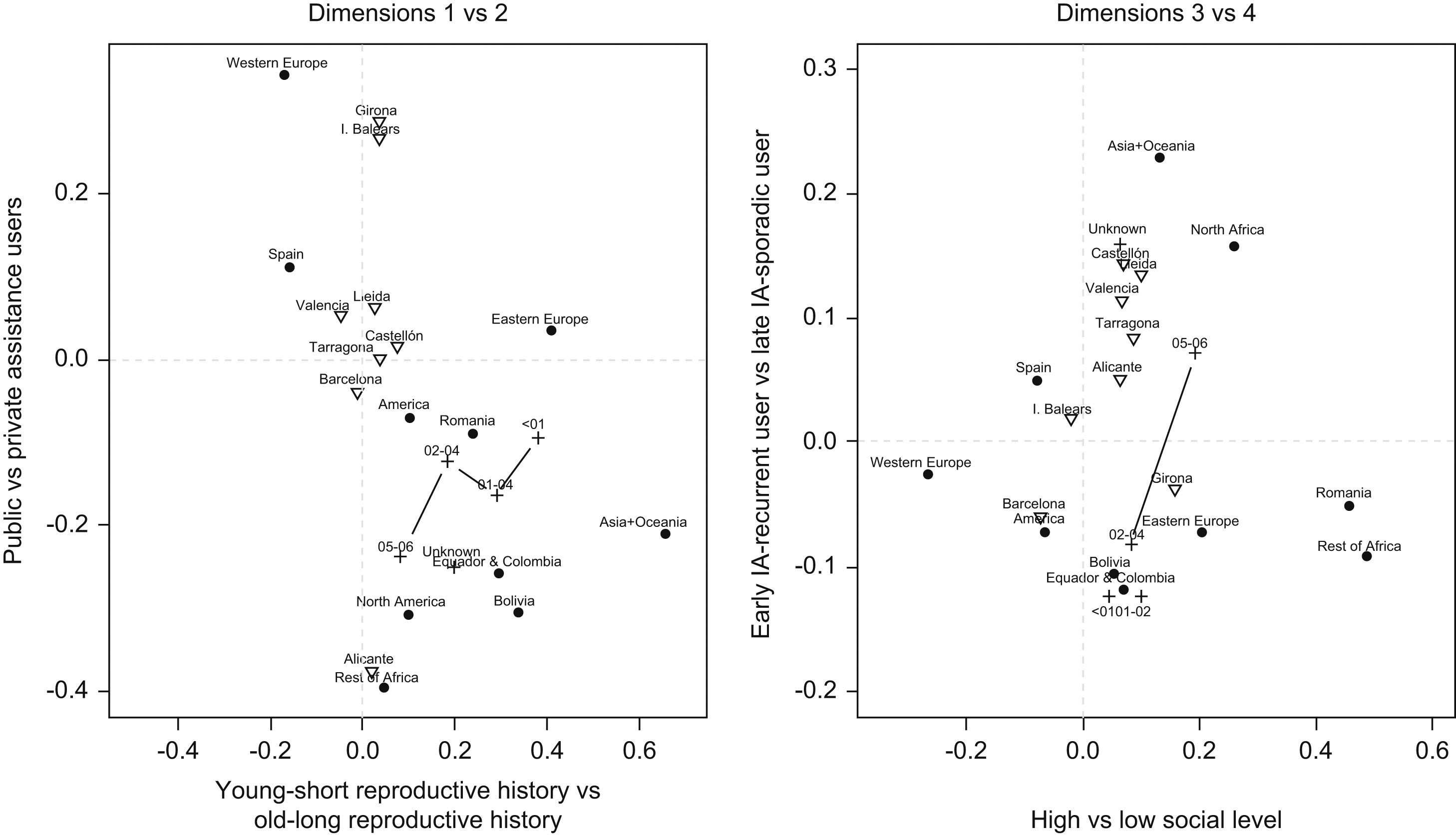
Regarding the supplementary variables (nationality, time since arrival and province of residence), Fig. 1 show how these categories are related to the four dimensions determined. A triangle indicates each province of residence, a circle is for each nationality group, and a cross shows the date of arrival in Spain. For this last variable, the categories of consecutive groups are linked to simplify the visualization.

The left side of Fig. 1 shows that on the negative sign side (younger and with less reproductive history) are Spanish and Western European women. There are few differences with regard to the province of residence. As for the arrival date for immigrants, it indicates that recently arrived women are closer to the centre of the axis and a time change gradient can be seen (more time in Spain equals older and with more reproductive history).
On the second axis of the left side of Fig. 1, it can be seen that women who attend private centres for contraception are mainly Spanish or Western European, but also Eastern European. Women residents in the province of Alicante make the most use of public services for contraception and IA information and women from other provinces such as Girona and the Balearic Islands use the private services. Immigrant women basically attend public health services for contraception and IA information but there is a time evolution and the use of public services is more frequent among recent immigrants.
For the third dimension (right side of Fig. 1), the first axis in the former chart shows that Western European women, followed by Spanish and South American women, have a higher social status. Romanians and African women resorting to IAs have a lower social status. Women residents in Barcelona and the Balearic Islands have better social indicators, while women from Girona have the worst social indicators. There is a time evolution for immigrants: for women with a recent arrival date the social status is lower than for women with more years in Spain, although immigrant women always have a lower social status than the average population.
With respect to the fourth dimension: the IA of women from Asia, Oceania, North Africa and Spain is later and they are less recurrent users of IAs than the remaining nationalities who are more likely to be early and recurrent users. Moreover, immigrant women with more time in Spain, those arriving before 2005, are more likely to show an early and recurrent pattern than women with a more recent arrival. Women arriving before 2005 show similar early and recurrent patterns regardless of the specific date of immigration. The provinces of Barcelona and Girona were the ones where the IA early and recurrent pattern was more present.
DiscussionAge and related factors (living children, marital status, cohabitant, years since last delivery) emerge as important determinants for IA. This fact has been previously stressed17 with regard to the different phases of a woman's life cycle. The completion of studies and the beginning of work are frequent reasons for undergoing an IA for younger women. The desire to stop childbearing, family reasons and the work situation are motivations for older women. Differences can be observed in relation to the women's adopted country: in Barcelona,10 few women go ahead with their pregnancy in the absence of a «stable» partnership, which is in contrast to those who go to Northern European countries. Studies in France and Italy17–19 show that the association between educational level and the abortion decision depends on age and partner cohabitation.
The utilization of the health system for contraception and IA information is not the same in Spain for women of different nationalities. Private clinics are used by Spanish and Western European women (17.3% of these women vs. 10.7% of the women from other origins). Immigrant women use the public services (50.6% of these women vs 44.3% of the women from Spain and Western Europe). This fact indicates the existence of a dual access to information related to economic status and knowledge of health system and its context. In other countries,18 the woman's social and demographic profile influences the choice of the first type of professional contacted and depending on this first choice, the conditions of IA access can be different. In Denmark20 immigrant women felt that they were insufficiently informed about contraception and this fact was associated with an increased risk for requesting an IA.
Among the classic factors associated with undergoing an IA2 are a low educational level, unemployment and low income. In Spain, our results show a clear social difference between Spanish-born, Western European and South American women compared to Romanian and African women resorting to IAs. That fact again emphasizes the need to consider social inequality as one of the main factors influencing reproductive health.21
Gestational weeks and repeated IAs is mainly related with Asian, North African and Spanish women. In countries such as Switzerland,4 it is known that foreign nationality is a significant risk for repeating IAs and that Romanian women are the most frequent repeaters. According to our data, Romanians are in the more frequent group for recurrent IAs, but not more so than women from other parts of Western Europe or Africa, for example. Differences in knowledge about and use of contraception, or the consideration of IAs as a contraception method by some nationalities could be an explanation. Immigrant women with more years in Spain are in the group with earlier use and more repeated IAs. This could indicate a persistent social vulnerability related to IA use and the contraception situation and not simply the lack of prospects for personal, family and economic stability. Another fact to mention is that the probability of a recurrent IA for non-Spanish-born women increases with the duration of residency (it grows from 27.5% for those women arriving in Spain before 2001 to 42.8% for those women arriving between 2005 and 2006).
In the province of residence analysis, all the women are included both Spanish-born and foreigners, so both can influence the results. There are no differences with regard to age by province of residence, but there are differences in other axes. Women resident in the province of Alicante mainly use the public system for obtaining IA information (the province with the highest percentage, having 76.3% of the IAs). Women from the province of Girona use the private system for IA information (the province with the highest percentage, with 26.5% of the IAs), have lower social status and there are frequent repeated IAs and they are earlier (the province with the highest percentage of recurrent and early IAs, 37.4%). In the Balearic Islands women also use the private system for IA information (the province with the lowest use of public centres, 31.3%) and their social status is higher. For women resident in the province of Barcelona social status is higher, and repeated IAs are frequent with fewer gestational weeks, showing the highest percentage of IAs with less than 8 gestational weeks, 52.24%. The remaining provinces are all at similar levels with respect to the four dimensions determined, with the exception of Castelló, Lleida and Valencia as regards the dimension of gestational weeks and repeated IAs, as in these provinces recurrence and early IAs are less frequent than in other provinces.
A barrier for IA in immigrant women, and a source of inequality, could be the differences between regions for the economic access to IA (some regions have established partial or total financing for IA in private centres). The bureaucratic problems and the complexity of the process (different between regions) seem to be one of the causes11 of a different accessibility.
The source of data used in the study has some known limitations18,22 such as that of under-notification. An information bias can affect the results but only if the lack of notification is different with respect to the type of women or the type of centre, which could imply a modification of the socio-demographic profile. Most of the notification problems affect public centres and so it is possible that there is an under-representation of women who attend such centres. However, the proportion of women who undergo an IA in public centres is relatively low, and so the problem is minor.
A strength of the study is that the population analysed is wide and includes different health systems, varying demographic and socio-economic characteristics, and uses IA registries that have been working adequately for more than 20 years.
Four dimensions have been determined that define the profile of women resorting to IAs in our study. Depending on the place in which the women are located in the dimensions determined, each woman can be characterized as younger or older (and other related reproductive and marital status factors), a public health service user or private health service user, of a lower social level or higher social level, or a sporadic or recurrent IA demander. It is possible to distinguish differences between non-Spanish women depending on their nationality, date of arrival and province of residence. Immigration seems to increase the vulnerability (related to social support, educational and economic level, knowledge and use of health system), specifically for some groups of non-Spanish women, and influences the probability of having an IA.
The study results indicate that more effort is needed towards promoting adequate contraception use, making access to the family planning healthcare system easier and, especially, directing such efforts towards specific immigrant populations.
Some groups of immigrants need to access effective and qualified family planning care and a health promotion system for reproductive health. Frequently, for vulnerable groups, social and labour barriers make it difficult. The implementation of social policies addressed to specific immigrants groups could help to remove these obstacles. More research in this field is needed to contribute to making the vulnerability problem more visible and to minimize its effects.
Conflict of interestThe authors declare that they have no conflict of interest.
FundingThis work was performed within the authors’ institutions and received no external funding.
Author contributionsO. Zurriaga designed the study, supervised all aspects of its performance and wrote the article. M.A. Martínez-Beneito performed the statistical analysis and contributed to the drafting and critical review of the manuscript. A. Galmés Truyols participated in data acquisition, in interpretation of the results and contributed to the drafting and critical review of the manuscript. M.M. Torne performed the statistical analysis and contributed to the drafting and critical review of the manuscript. S. Bosch participated in data acquisition and in interpretation of the results. R. Bosser participated in data acquisition, in interpretation of the results and contributed to the drafting and critical review of the manuscript. M. Portell Arbona participated in data acquisition and in interpretation of the results. All the authors contributed ideas and reviewed the drafts of the manuscript. All the authors approved the final version.











