



The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
More infoAtrial fibrillation (AF) is one of the most commonly occurring arrhythmias and a major modifiable risk factor of stroke, especially in women. The incidence of AF in Indonesia is not well-characterized yet. This is a community-based study to determine the prevalence and characteristics of AF in the Makassar city population.
MethodStandard ECG recording showing atrial fibrillation obtained between January 1, 2014 and September 31, 2018 from Telemedicine Study Center in Hasanuddin University Hospital were collected in form of portable document format (pdf) and were analyzed. ECG with incomplete interpretation and/or epidemiological data were excluded. ECG interpretation and analysis were performed by the first author as an electrophysiologist (MA). Epidemiological data, heart rate, P wave amplitude, QRS axis, QRS complex duration and configuration, QRS rate (ventricular response), corrected QT interval according to Bazzett's formula, presence of QRS complex abnormalities and ST-T changes were analyzed. Data analysis were performed using SPSS 20.0 for Windows.
ResultA total of 19.718 ECG data were obtained, taken from the Makassar Telemedicine study data center at Hasanuddin University Hospital which cover all Public Health Center and a private clinic in Makassar city. From this population, AF was found in 189 (0.96%) ECGs. 98 (51.9%) are males’ and 91 (48.1%) of which are females’. AF is increasingly prevalent with increasing ages. There was a significant difference on the QRS axis between male and female with a p value of <0.001. The duration of the QRS complex between men and women was significantly different (p=0.038). QTc value was also found to be significantly different between male and female (p=0.001). AF was accompanied by PVC in 9 males and 2 females.
ConclusionThe prevalence of AF in the Makassar population is 0.96%, more common in men and elderly.
Atrial fibrillation (AF) is a typical supraventricular tachyarrhythmia, with uncoordinated atrial activation resulting in deterioration of the mechanical function of the atrial. On an electrocardiogram (ECG), the characteristic of AF is the absence of consistency of P wave, which is replaced by vibrating wave (fibrillation) that vary in amplitude, shape, and duration. In normal atrioventricular node function, AF is usually followed by a ventricular response that is also irregular and often rapid.1 AF could occur with or without prior heart disease. Increasing age is closely associated with an increased incidence of these arrhythmias as well as an increased risk of their complications. AF is associated with almost all heart disease that causes a change in the myocardial atrial such as distension, inflammation, hypertrophy, ischemia, and infiltration.2
Atrial fibrillation is associated with an increased risk of stroke. Stroke might be the first clinical manifestation of AF and neurologists are sometimes the first entry point toward a diagnosis of AF. In 37% of AF patients less than 75 years of age, ischemic stroke was the first symptom. People with AF have five times the risk of stroke than people who do not have one.3 AF-related stroke increases the risk of long-term disability and death. The risk of stroke associated with AF was 1.5% among 50–59 years, whereas among 80–89 years, it increased to 23.5%.4
Atrial fibrillation is the most common type of arrhythmia in clinical practice. The increasing prevalence of AF is a growing community health problem around the world. Epidemiological descriptions of the AF to date have mostly come from North American and European populations, and there is a relatively limited data from Asian countries, including Indonesia. The Global Burden of Disease (GBD) Study estimated that the prevalence of AF in adults in the world in 2010 was around 0.5%, representing a total of 33.5 million individuals.5 Women generally have lower age-adjusted incidence and prevalence of AF.6 In Southeast Asia, community-based AF data are scarce. In Singapore, the prevalence of AF is reported to be 1.5%. In Thailand, the prevalence of AF ranges from 0.4 to 2.2%. In Malaysia, it is estimated around 0.5–0.7%.7
Sex difference in epidemiology and prognosis of AF have been outlined by several studies. The GBD study estimated in a prevalence of AF of 373.1/100,000 for women and 5962/100,000 for men. Women suffering from AF show a different prognosis, with a higher incidence of stroke and a higher mortality rate compared to men.8 In Indonesia, an observational study (MONICA, multinational MONItoring of trend and determinant in Cardiovascular disease) in the urban population in Jakarta obtained an AF incidence rate of 0.2% with a male to female ratio of 3:2.9
Telemedicine is a health service program utilizing information technology that enables electronic data transferred from one health service facility to another. This program has been developed at the primary health center in Makassar city, especially in the field of cardiology.10
To date, telemedicine has been a popular tool in overcoming geographical barriers and increasing access to healthcare services. This particularly benefits the rural and underserved populations in low- and middle-income countries-groups that traditionally suffer from lack of access to healthcare. Because of the shortage of cardiologists and evident demand for expertise in cardiovascular care, Makassar Cardiac Center initiated the first telemedicine project in Eastern Indonesia-transferring the electrocardiography (ECG) recording from primary care facilities to the center of expertise at Hasanuddin University Hospital. This project entailed decision support for general practitioners (GPs) in primary care when confronted with patients with symptoms of cardiovascular disease.11
In Indonesia, to date there has not been much data suggesting the characteristics and prevalence of AF. Therefore, it is important to describe the characteristics of AF in Indonesia. This is an epidemiological study aimed to determine the prevalence of atrial fibrillation inferred from the data obtained in the community health center and clinics in Makassar. The data was collected from the Makassar Telemedicine database.
MethodLocationThis research was conducted at the Telemedicine Data Center at Hasanuddin University Hospital. This research was conducted in accordance with ethical principles and has received ethical clearance from Hasanuddin University ethical committee (No: 968/UN4.6.4.5.31/PP36/2019).
DesignThis study is a cross sectional epidemiological study. The population and sample in this study was the Mongoloid race of the Malay sub-race in Makassar city aged ≥17 years who had been subjected to standard electrocardiogram (ECG) examinations (12 leads, speed 25mm per second, amplitude 10mm per millivolt) by a trained physician and nurse at several community health centers and private clinics in Makassar. ECG was recorded using BTL-O8Sd machine with 12-lead recording format with the lowest filter of 0.05Hz, with 25mm/s and 10mm/mV calibration, with activated filter to reduce artifacts. A minimum of 5 beat were recorded from each lead. ECG calibration was performed at the beginning and the end of recording process. ECG recording from each center was sent to Telemedicine Study Center in Hasanuddin University Hospital. Standard ECG recording showing atrial fibrillation obtained between January 1, 2014 and September 31, 2018 from Telemedicine Study Center in Hasanuddin University Hospital were collected in form of portable document format (pdf) and analyzed. ECG with incomplete interpretation and/or epidemiological data were excluded. ECG interpretation and analysis were performed by the first author as an electrophysiologist (MA). Epidemiological data, heart rate, P wave amplitude, QRS axis, QRS complex duration and configuration, QRS rate (ventricular response), corrected QT interval according to Bazzett's formula, presence of QRS complex abnormalities and ST-T changes were analyzed. Data analysis was performed using SPSS 20.0 for Windows.
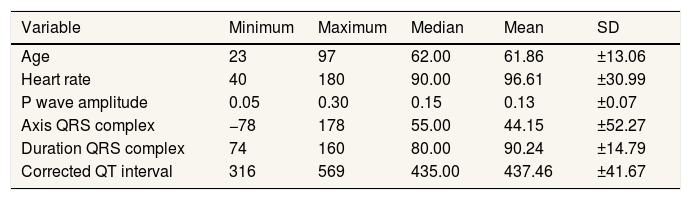
ResultA total of 19,718 ECG data were obtained, taken from the Makassar Telemedicine study data center at Hasanuddin University Hospital which cover all Public Health Center and a private clinic in Makassar city. From this population, AF was found in 189 (0.96%) ECGs. Numerical variable inferred from patients with AF is shown in Table 1.
Basic characteristic of patients with AF in the population (Numerical data).
| Variable | Minimum | Maximum | Median | Mean | SD |
|---|---|---|---|---|---|
| Age | 23 | 97 | 62.00 | 61.86 | ±13.06 |
| Heart rate | 40 | 180 | 90.00 | 96.61 | ±30.99 |
| P wave amplitude | 0.05 | 0.30 | 0.15 | 0.13 | ±0.07 |
| Axis QRS complex | −78 | 178 | 55.00 | 44.15 | ±52.27 |
| Duration QRS complex | 74 | 160 | 80.00 | 90.24 | ±14.79 |
| Corrected QT interval | 316 | 569 | 435.00 | 437.46 | ±41.67 |
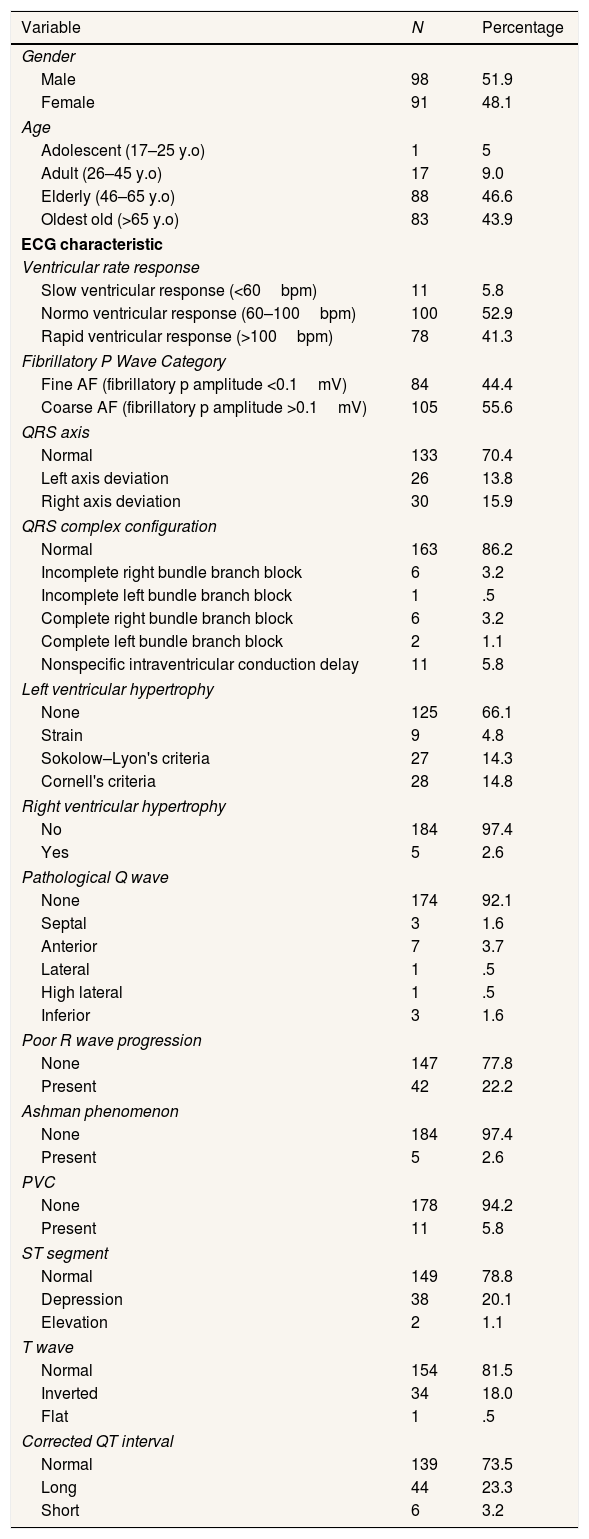
From 189 ECGs, 98 (51.9%) are males’ and 91 (48.1%) of which are females’. AF with a normal ventricular response was found in 100 (52.9%), a fast ventricular rate response of 78 (41.3%), and a slow ventricular response of 11 (5.8%). QRS axis was mostly normoaxis (70.4%), left axis deviation was found in 13.8%, and right axis deviation was found in 15.9%. Ashman phenomenon was only found in 5 ECGs (2.6%) and 11 PVCs (5.8%). ECGs with AF enrolled this study was found to generally have a normal QTc interval, long QTc intervals were found in 44, and short QTc intervals were found in 6 ECGs. Categorical data inferred from patients with AF is shown in Table 2.
Basic characteristic of patients with AF in the population (categoric data).
| Variable | N | Percentage |
|---|---|---|
| Gender | ||
| Male | 98 | 51.9 |
| Female | 91 | 48.1 |
| Age | ||
| Adolescent (17–25 y.o) | 1 | 5 |
| Adult (26–45 y.o) | 17 | 9.0 |
| Elderly (46–65 y.o) | 88 | 46.6 |
| Oldest old (>65 y.o) | 83 | 43.9 |
| ECG characteristic | ||
| Ventricular rate response | ||
| Slow ventricular response (<60bpm) | 11 | 5.8 |
| Normo ventricular response (60–100bpm) | 100 | 52.9 |
| Rapid ventricular response (>100bpm) | 78 | 41.3 |
| Fibrillatory P Wave Category | ||
| Fine AF (fibrillatory p amplitude <0.1mV) | 84 | 44.4 |
| Coarse AF (fibrillatory p amplitude >0.1mV) | 105 | 55.6 |
| QRS axis | ||
| Normal | 133 | 70.4 |
| Left axis deviation | 26 | 13.8 |
| Right axis deviation | 30 | 15.9 |
| QRS complex configuration | ||
| Normal | 163 | 86.2 |
| Incomplete right bundle branch block | 6 | 3.2 |
| Incomplete left bundle branch block | 1 | .5 |
| Complete right bundle branch block | 6 | 3.2 |
| Complete left bundle branch block | 2 | 1.1 |
| Nonspecific intraventricular conduction delay | 11 | 5.8 |
| Left ventricular hypertrophy | ||
| None | 125 | 66.1 |
| Strain | 9 | 4.8 |
| Sokolow–Lyon's criteria | 27 | 14.3 |
| Cornell's criteria | 28 | 14.8 |
| Right ventricular hypertrophy | ||
| No | 184 | 97.4 |
| Yes | 5 | 2.6 |
| Pathological Q wave | ||
| None | 174 | 92.1 |
| Septal | 3 | 1.6 |
| Anterior | 7 | 3.7 |
| Lateral | 1 | .5 |
| High lateral | 1 | .5 |
| Inferior | 3 | 1.6 |
| Poor R wave progression | ||
| None | 147 | 77.8 |
| Present | 42 | 22.2 |
| Ashman phenomenon | ||
| None | 184 | 97.4 |
| Present | 5 | 2.6 |
| PVC | ||
| None | 178 | 94.2 |
| Present | 11 | 5.8 |
| ST segment | ||
| Normal | 149 | 78.8 |
| Depression | 38 | 20.1 |
| Elevation | 2 | 1.1 |
| T wave | ||
| Normal | 154 | 81.5 |
| Inverted | 34 | 18.0 |
| Flat | 1 | .5 |
| Corrected QT interval | ||
| Normal | 139 | 73.5 |
| Long | 44 | 23.3 |
| Short | 6 | 3.2 |
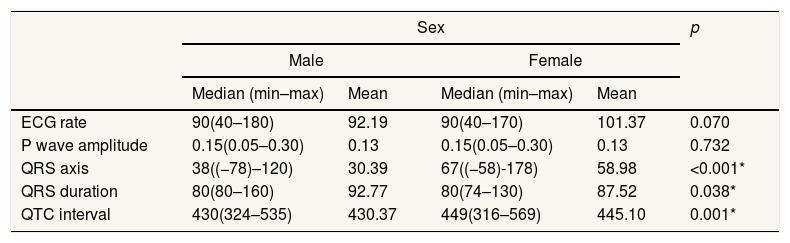
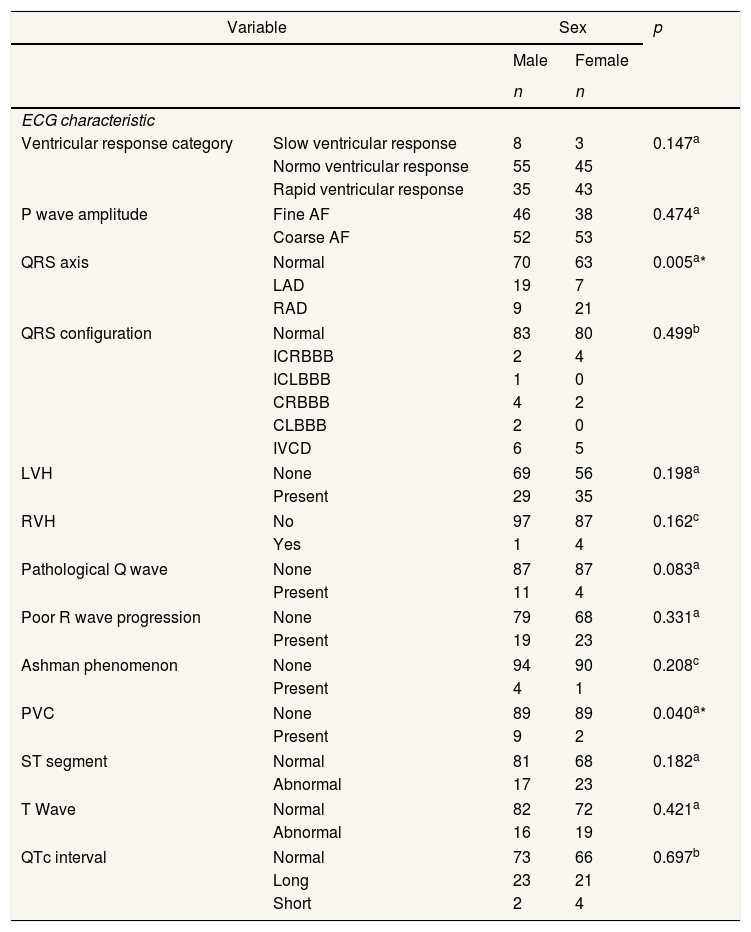
There was a significant difference on the QRS axis between male and female with a p value of <0.001 (Table 3). The duration of the QRS complex between men and women was also found to be significantly different (p=0.038). QTc value was also found to be significantly different between male and female (p=0.001). AF was accompanied by PVC in 9 males and 2 females (Table 4).
Basic characteristic of patients with AF in the population stratified by sex (numerical data).
| Sex | p | ||||
|---|---|---|---|---|---|
| Male | Female | ||||
| Median (min–max) | Mean | Median (min–max) | Mean | ||
| ECG rate | 90(40–180) | 92.19 | 90(40–170) | 101.37 | 0.070 |
| P wave amplitude | 0.15(0.05–0.30) | 0.13 | 0.15(0.05–0.30) | 0.13 | 0.732 |
| QRS axis | 38((−78)–120) | 30.39 | 67((−58)-178) | 58.98 | <0.001* |
| QRS duration | 80(80–160) | 92.77 | 80(74–130) | 87.52 | 0.038* |
| QTC interval | 430(324–535) | 430.37 | 449(316–569) | 445.10 | 0.001* |
Basic characteristic of patients with AF in the population stratified by sex (categorical data).
| Variable | Sex | p | ||
|---|---|---|---|---|
| Male | Female | |||
| n | n | |||
| ECG characteristic | ||||
| Ventricular response category | Slow ventricular response | 8 | 3 | 0.147a |
| Normo ventricular response | 55 | 45 | ||
| Rapid ventricular response | 35 | 43 | ||
| P wave amplitude | Fine AF | 46 | 38 | 0.474a |
| Coarse AF | 52 | 53 | ||
| QRS axis | Normal | 70 | 63 | 0.005a* |
| LAD | 19 | 7 | ||
| RAD | 9 | 21 | ||
| QRS configuration | Normal | 83 | 80 | 0.499b |
| ICRBBB | 2 | 4 | ||
| ICLBBB | 1 | 0 | ||
| CRBBB | 4 | 2 | ||
| CLBBB | 2 | 0 | ||
| IVCD | 6 | 5 | ||
| LVH | None | 69 | 56 | 0.198a |
| Present | 29 | 35 | ||
| RVH | No | 97 | 87 | 0.162c |
| Yes | 1 | 4 | ||
| Pathological Q wave | None | 87 | 87 | 0.083a |
| Present | 11 | 4 | ||
| Poor R wave progression | None | 79 | 68 | 0.331a |
| Present | 19 | 23 | ||
| Ashman phenomenon | None | 94 | 90 | 0.208c |
| Present | 4 | 1 | ||
| PVC | None | 89 | 89 | 0.040a* |
| Present | 9 | 2 | ||
| ST segment | Normal | 81 | 68 | 0.182a |
| Abnormal | 17 | 23 | ||
| T Wave | Normal | 82 | 72 | 0.421a |
| Abnormal | 16 | 19 | ||
| QTc interval | Normal | 73 | 66 | 0.697b |
| Long | 23 | 21 | ||
| Short | 2 | 4 | ||
In this study, we found the prevalence of AF in the population of Makassar city was 0.96%, where the prevalence in men was 51.9% more than in women 48.1%. The results of this study are in line with several studies in Asian countries where the reported prevalence of AF varies from 0.1% in India to 2.2% in Thailand. In various studies from other Asian countries such as Japan, the prevalence of AF was consistent, ranging from 0.6% to 0.9%, and a similar prevalence was reported in Taiwan (1.1%). Likewise, from a community-based cohort studies in China, the AF prevalence was 0.8% and in Thailand, it ranged from 0.4% to 2.2%. Men are more prone to developing AF. However, because women live longer than men, the cumulative lifetime-risk of AF is similar in men and women, about 30%. On average, women experience AF 10 years later than men. Differences in the effective refractory period (ERP) have been reported in men and women. The degree of atrial ERP shortening was significantly less in premenopausal women compared to postmenopausal women and age-appropriate men, suggesting a protective role for estrogen. In addition, non-pulmonary vein triggers are more common in women than in men. Recent evidence points to genetic differences in ion channel expression between men and women. Gender differences in the control of the autonomic nervous system of the cardiovascular system are also well known. The sympathetic-mediated response was predominant in men, while women had higher levels of parasympathetic activation, and this has been associated with an increased likelihood of developing AF.12 Morphologically, significant gender-based differences in AF-related atrial remodeling were observed. Left atrial fibrotic remodeling causes electrical dissociation of atrial cells which contributes to a higher incidence and recurrence rate of AF.13 Analyzed tissue samples from men and women with long-lasting persistent AF and showed that women had significantly higher rates of fibrotic remodeling compared with men.12
This study found that AF prevalence increases with age. Advanced age is known as the most prominent risk factor for AF. An aging heart, characterized by myocardial fibrosis and atrial dilatation, provides the ideal conditions and substrate for AF to develop. AF induces electrical and structural remodeling in the atria by affecting the effective refractory period (increasing dispersion), suppressing intra-atrial conduction, and decreasing its contractile function.14 The majority of elderly people live with one or more comorbidities. The atrial myocardium undergoes electrical and structural remodeling with age, both of which play an important role in inducing and/or perpetuating AF. The longer time in which the atrial myocardium is exposed to the effects of external stressors and risk factors explains the relationship between age and FA.15
The duration of the QRS complex between male and female was also found to be significantly different. Research conducted by Ghani et al. on sex-based differences in cardiac arrhythmias, found that in female the QRS complex is narrower and the QRS amplitude is lower than that of male. This may be due to a smaller heart size in female, but it is still found after correcting heart mass and body weight. Even with cardiac abnormalities such as ventricular hypertrophy, female have relatively lower QRS duration compared to male.16
Another significant finding was that PVC is found more frequently in males than females, namely 9 vs 2 with a p=0.04. Most studies showed a higher prevalence of PVC in male, as in a study conducted by Ban J. et al. which examined 127 patients with PVC, found 61% of whom were male.17 Likewise a study conducted by Blaye-Felice et al. which examined 168 patients with PVC, 104 (62%) of whom were male.
Another significant difference was the QTc interval using Hodges formula, male vs female 430ms (324–535ms) vs 449ms (316 vs 569ms), p value 0.001. There is no consensus on the best method for correction of the QT interval in atrial fibrillation. Research conducted by Tooley J et al. found that there was a significant difference in QTc between atrial fibrillation and sinus rhythm in all tested correction formulas, but the use of the Hodges formula resulted in the smallest difference in QTc. Gender differences in QTc intervals have been noted since Bazett's initial description during the 1920s, where the QTc interval of female was 24ms greater than that of male. Sex hormones such as estrogen, progesterone, and testosterone have been shown to affect the QTc interval. Testosterone tends to shorten the QT interval whereas estrogen tends to lengthen the QT interval.18
ConclusionIn this study, the prevalence of AF in Makassar city population was 0.96%. AF is more common in male and elderly age group. AF in males has a wider mean QRS duration than the one in female, and is more often accompanied by PVC. Whereas in female the QTc interval is longer than in male.
Conflicts of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











