



The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
More infoMoringa Oleifera leaves contain nutrients such as proteins, iron, and vitamin C that potentially prevent anemia more common in pregnant women. In the manufacture of cookies that are substituted Moringa Oleifera leaf flour substitution, 40% obtained Fe levels 22.68ppm so that it can be developed to prevent anemia. The purpose of this research is to know the effect of giving biscuits (cookies) Moringa Oleifera leaf flour to index erythrocytes (MCH, MCHC, MCV) of pregnant women with anemia.
MethodIt was a quasi-experiment research with design nonequivalent Control Group design. The research was conducted at Antang, Mamajang, and Batua Public Health Center in Makassar, examination of hematology analyzer in the Clinic Pathology Laboratory of Universitas Hasanuddin Hospital. Sampling techniques using purposive sampling. Samples were pregnant women with trimester I and III anemia amounted to 25 samples on the biscuit moringa group and 25 samples in the control group. Data were analyzed using test Paired T-Test, T-Test Independent, Wilcoxon, and Mann – U Withney.
ResultCharacteristics of age, gestational age, income, physical activity, education, and parity of both groups has been comparable before the treatment with the value p>0.05, with most of the samples aged 20–35 years having a pregnancy age of 4–8 weeks, income IDR 1 million – IDR. 2 million, activity score Baecke 6.00–7.25, Senior High School education, parity >1. A significant average increase in the value of MCH from 27.55 to 28.00 and MCV from 78.57 to 78.93 in the group provided biscuits (cookies) of Moringa Oleifera leaf flour with p-value <0.05, in the control group, occurred an average but insignificant increase with p-value >0.05. The MCHC Group control and biscuit moringa group had an average increase, but both were not statistically significant, p>0.05. There is a significant difference in increased MCH and MCV erythrocyte indices between the biscuit moringa and control groups with a p-value <0.05. As for the MCHC value, the two groups do not differ meaningfully with p-value=0.611, p>0.005.
ConclusionThere is the effect of giving biscuits (cookies) Moringa Oleifera leaf Flour Against the index of erythrocytes MCH and MCV in pregnant women with anemia. However, it has no effect on the MCHC value of pregnant women with anemia. It is recommended for pregnant women to utilize local plants, the Moringa Oleifera leaves to fulfill the intake of nutrients that can help pregnant women from anemia.
Anemia in pregnancy is public health, especially in developing countries, associated with various harmful events during pregnancy.1 According to the World Health Organization (WHO) the latest forecast for 2016 indicates that anemia affects 33% of women of reproductive age globally, about 613 million women between the ages of 15 and 49. The African region has countries with the lowest hemoglobin and the prevalence of the highest anemia.2 In Indonesia, the prevalence of anemia in pregnant women, according to the result of Basic Health Research year 2018 that is 48.9% higher than the year 2013 is 37.1%, and the year 2007 is 24.5%.3
The leading causes of anemia are inadequate nutrients (iron deficiency, folic acid, and vitamins), infectious diseases such as malaria, and untreated genetic hemoglobin abnormalities4 Anemia in pregnancy is generally regarded as a risk factor that can lead to complications that threaten maternal and fetal life.5
To reduce nutrition problems in Indonesia, developed an additional food delivery formula (AFD) in healthy biscuits that the manufacturing process is substituted for moringa leaf flour.6 Moringa is famous in Indonesia, especially in rural areas, but not fully used in life. In Indonesia, the Moringa tree is often planted as a living fence, planted along the edge of the field, functioning as a green crop. In addition, the Moringa plant is also known as a nutritious, medicinal plant by utilizing all parts of the moringa plants ranging from leaves, bark, seeds to roots.7 In addition, moringa leaves contain a multi-element of micronutrient substance that is needed by pregnant women, such as beta carotene, thiamin (B1), riboflavin (B2), niacin (B3), calcium, phosphorus, magnesium, zinc.8 The study conducted by Dewi in 2018 showed the influence of Moringa Oleifera leaf flour substitution (Moringa oleifera L.) on the manufacture of cookies on organoleptic properties, proximate and Fe levels. So that the moringa leaf flour can be developed for the prevention of anemia is substitution 40% Moringa leaf flour with Fe levels 22.68ppm.9
Materials and methodsMaterialsThe formulation of Moringa leaf flour biscuit has followed the research results conducted by Dewi (2018) with Fe content 22.68ppm. Moringa leaf flour biscuits made with wheat flour 150g, Moringa flour leaves 100 g (40%), margarine 175 g, milk powder 30mg, sugar powder 125 g, salt 2 g kitchen, and one chicken egg. Then processed into biscuits (cookies) with a weight of 17 g/chip that has a content of moringa leaf flour 2.8g/chip and total nutrient content based on the calculation of FICL (food ingredient composition list) 1 piece of biscuit (cookies) Moringa leaf flour has energy 78.3kcal, 1.68g protein, fat 4.63g, carbohydrate 8.17 g, and Iron 0.99mg.
Design researchThis research was conducted in the working area of Antang, Mamajang and Batua Public Health Center in Makassar and Clinical Pathology Laboratory of Hasanuddin University Hospital. The research took place in March 2020 to June 2020 after Ethical approval recommendation from the Medical Research Ethics Committee of the Faculty of Medicine of Hasanuddin University. The study used the quasi experiment research type, with the design of The Nonequaivalent control group Design in which the control and intervention groups were not randomly selected.10 The intervention Group is given the biscuit moringa leaves flour 2 pieces/day with a content of 2.8 grams of moringa leaf flour and a Fe tablet 2× 250mg and a control group given the tablet Fe 2× 250mg/day for 60 days. Sampling techniques with purposive sampling. Each group has 25 samples making it a total of 50 samples. The sample is a pregnant woman with anemia (Hb<11g/dl) in I and III trimester of a single fetus, does not have a history of diabetes, infection and genetic diseases and does not consume multivitamins and other minerals.
Data collection techniquesData obtained directly from the respondents collected through a questionnaire sheet physical activity Baecke Index and Food recall 24h and 3 cc blood intake through the red vein that is assisted by laboratory officers at the research site then conducted hematology examination by using Sysmex hematology Analyzer in Clinical Pathology Laboratory at Hasanuddin University Hospital to know the value of erythrocytes index in blood.
Data analysisTest Chi square to see the homogeneity of the respondents characteristics of both groups. Test data analysis of Paired Sample T-Test and Wilcoxon for a statistically significant average difference in two groups in pairs (average before and after each group). Then T-Test independent and Mann Whitney to see the statistically average difference between the two groups that are not paired (before and after between the biscuit moringa group and the control group).
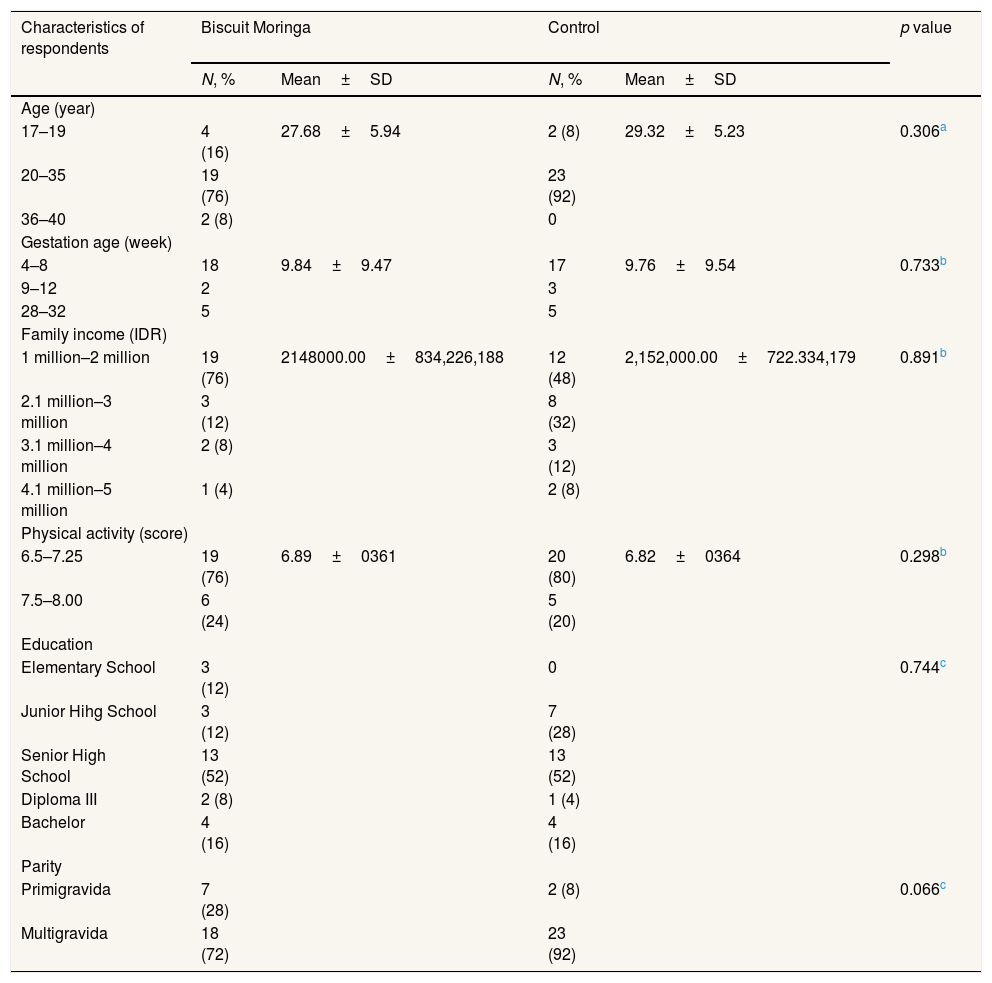
Research resultsTable 1 showed that most of the biscuit moringa group and control group respondents had an age of 20–35 years, 76% in the biscuit moringa group and 92% in the control group. On the characteristics of gestation age most respondents had a pregnancy of 4–8 weeks (I trimester) in the biscuit moringa group of 72% and control group of 68%. On the family income characteristics most of the two groups have an income of IDR. 1 million – IDR. 2 million with an average income in biscuit moringa group IDR. 2,148,000 and control group IDR. 2,152,000. In most physical activity the two groups had a Baecke index score of 6.5–7.25 (light activity) with an average score on biscuit moringa group is 6.89 and 6.82 in control group. Last education most of the respondents were Senior High School (SHS), on the biscuit moringa group and control group equal to 52%. In the parity characteristics most of the respondents had a pregnancy history of >1 times, with 72% on biscuit moringa Group and the control group of 92%. The homogeneity test of the entire characteristics of the both groups is equal with p value >0.05.
Frequency distribution of respondents characteristics.
| Characteristics of respondents | Biscuit Moringa | Control | p value | ||
|---|---|---|---|---|---|
| N, % | Mean±SD | N, % | Mean±SD | ||
| Age (year) | |||||
| 17–19 | 4 (16) | 27.68±5.94 | 2 (8) | 29.32±5.23 | 0.306a |
| 20–35 | 19 (76) | 23 (92) | |||
| 36–40 | 2 (8) | 0 | |||
| Gestation age (week) | |||||
| 4–8 | 18 | 9.84±9.47 | 17 | 9.76±9.54 | 0.733b |
| 9–12 | 2 | 3 | |||
| 28–32 | 5 | 5 | |||
| Family income (IDR) | |||||
| 1 million–2 million | 19 (76) | 2148000.00±834,226,188 | 12 (48) | 2,152,000.00±722.334,179 | 0.891b |
| 2.1 million–3 million | 3 (12) | 8 (32) | |||
| 3.1 million–4 million | 2 (8) | 3 (12) | |||
| 4.1 million–5 million | 1 (4) | 2 (8) | |||
| Physical activity (score) | |||||
| 6.5–7.25 | 19 (76) | 6.89±0361 | 20 (80) | 6.82±0364 | 0.298b |
| 7.5–8.00 | 6 (24) | 5 (20) | |||
| Education | |||||
| Elementary School | 3 (12) | 0 | 0.744c | ||
| Junior Hihg School | 3 (12) | 7 (28) | |||
| Senior High School | 13 (52) | 13 (52) | |||
| Diploma III | 2 (8) | 1 (4) | |||
| Bachelor | 4 (16) | 4 (16) | |||
| Parity | |||||
| Primigravida | 7 (28) | 2 (8) | 0.066c | ||
| Multigravida | 18 (72) | 23 (92) | |||
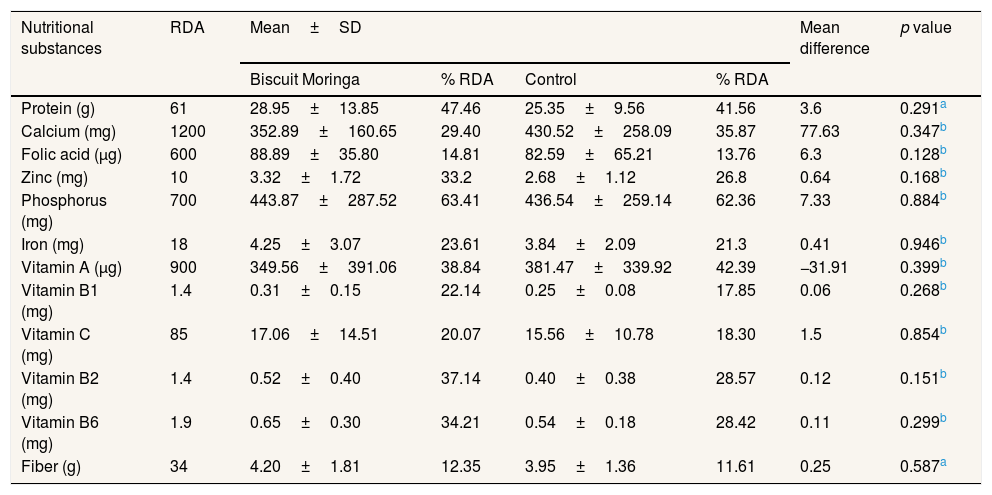
Table 2 shows both groups having nutritional adequacy protein, calcium, folic acid, zinc, phosphorus, iron, vitamin A, vitamin B1, vitamin C, vitamin B2, vitamin B6 and fiber are below 80% minimum of recommended dietary allowances (RDA) which should be said to be insufficient for nutritional needs each day. The analysis of the differences all nutrients between the both groups show have p>0.05 which means before treatment of interventional groups and control groups has comparable or equivalent nutritional intake.
Distribution of nutritional adequacy levels of macronutrients and micronutrients in the biscuit moringa group and control group before treatment.
| Nutritional substances | RDA | Mean±SD | Mean difference | p value | |||
|---|---|---|---|---|---|---|---|
| Biscuit Moringa | % RDA | Control | % RDA | ||||
| Protein (g) | 61 | 28.95±13.85 | 47.46 | 25.35±9.56 | 41.56 | 3.6 | 0.291a |
| Calcium (mg) | 1200 | 352.89±160.65 | 29.40 | 430.52±258.09 | 35.87 | 77.63 | 0.347b |
| Folic acid (μg) | 600 | 88.89±35.80 | 14.81 | 82.59±65.21 | 13.76 | 6.3 | 0.128b |
| Zinc (mg) | 10 | 3.32±1.72 | 33.2 | 2.68±1.12 | 26.8 | 0.64 | 0.168b |
| Phosphorus (mg) | 700 | 443.87±287.52 | 63.41 | 436.54±259.14 | 62.36 | 7.33 | 0.884b |
| Iron (mg) | 18 | 4.25±3.07 | 23.61 | 3.84±2.09 | 21.3 | 0.41 | 0.946b |
| Vitamin A (μg) | 900 | 349.56±391.06 | 38.84 | 381.47±339.92 | 42.39 | −31.91 | 0.399b |
| Vitamin B1 (mg) | 1.4 | 0.31±0.15 | 22.14 | 0.25±0.08 | 17.85 | 0.06 | 0.268b |
| Vitamin C (mg) | 85 | 17.06±14.51 | 20.07 | 15.56±10.78 | 18.30 | 1.5 | 0.854b |
| Vitamin B2 (mg) | 1.4 | 0.52±0.40 | 37.14 | 0.40±0.38 | 28.57 | 0.12 | 0.151b |
| Vitamin B6 (mg) | 1.9 | 0.65±0.30 | 34.21 | 0.54±0.18 | 28.42 | 0.11 | 0.299b |
| Fiber (g) | 34 | 4.20±1.81 | 12.35 | 3.95±1.36 | 11.61 | 0.25 | 0.587a |
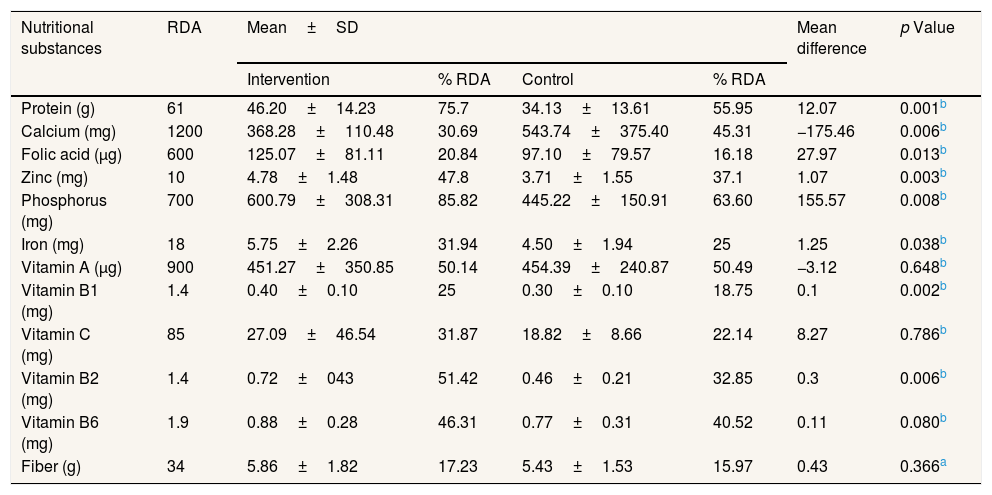
Table 3 shows off the overall nutritional substance only phosphorus which has a nutritional adequacy percent which is more than minimum needs (80%) of RDA that is 85.82%. After the analysis of the differences between the both groups of some nutrients, namely protein, calcium, folic acid, zinc, phosphorus, iron, vitamin B1 and vitamin B2 get a p value<0.05 which means that some nutrients have a significant average difference between both group after treatment.
Distribution of nutritional adequacy levels of macronutrients and micronutrients in biscuit moringa group and control group after treatment.
| Nutritional substances | RDA | Mean±SD | Mean difference | p Value | |||
|---|---|---|---|---|---|---|---|
| Intervention | % RDA | Control | % RDA | ||||
| Protein (g) | 61 | 46.20±14.23 | 75.7 | 34.13±13.61 | 55.95 | 12.07 | 0.001b |
| Calcium (mg) | 1200 | 368.28±110.48 | 30.69 | 543.74±375.40 | 45.31 | −175.46 | 0.006b |
| Folic acid (μg) | 600 | 125.07±81.11 | 20.84 | 97.10±79.57 | 16.18 | 27.97 | 0.013b |
| Zinc (mg) | 10 | 4.78±1.48 | 47.8 | 3.71±1.55 | 37.1 | 1.07 | 0.003b |
| Phosphorus (mg) | 700 | 600.79±308.31 | 85.82 | 445.22±150.91 | 63.60 | 155.57 | 0.008b |
| Iron (mg) | 18 | 5.75±2.26 | 31.94 | 4.50±1.94 | 25 | 1.25 | 0.038b |
| Vitamin A (μg) | 900 | 451.27±350.85 | 50.14 | 454.39±240.87 | 50.49 | −3.12 | 0.648b |
| Vitamin B1 (mg) | 1.4 | 0.40±0.10 | 25 | 0.30±0.10 | 18.75 | 0.1 | 0.002b |
| Vitamin C (mg) | 85 | 27.09±46.54 | 31.87 | 18.82±8.66 | 22.14 | 8.27 | 0.786b |
| Vitamin B2 (mg) | 1.4 | 0.72±043 | 51.42 | 0.46±0.21 | 32.85 | 0.3 | 0.006b |
| Vitamin B6 (mg) | 1.9 | 0.88±0.28 | 46.31 | 0.77±0.31 | 40.52 | 0.11 | 0.080b |
| Fiber (g) | 34 | 5.86±1.82 | 17.23 | 5.43±1.53 | 15.97 | 0.43 | 0.366a |
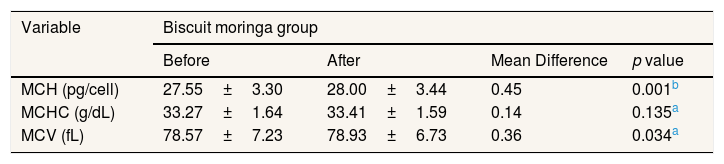
Based on Table 4 data occurred an increase in the average value of the index of MCH, MCHC and MCV erythrocytes. After testing the analysis obtained the index of erythrocytes MCH and MCV increases significantly with the p value<0.05, so there is a meaningful difference before and after the administration of the biscuit moringa leaves flour.
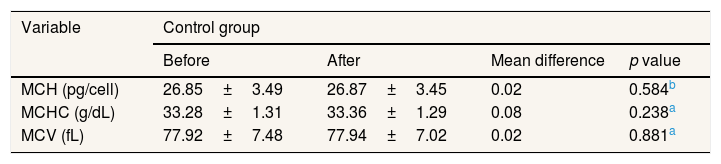
Table 5 shows an increase in the average value of MCH, MCHC and MCV erythrocytes. However, after the analysis has been tested the value erythrocytes of the MCH, MCHC and MCV are not significantly increased with p value >0.05, so there is no meaningful difference before and after the treatment in the control group.
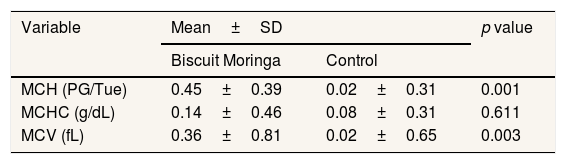
Table 6 shows from all three erythrocyte indexes that have significant differences between the groups are MCH and MCV with a value of p<0.05 which means the administration of the moringa leaf flour effectively increases the value of MCH and MCV.
DiscussionThe effect of giving biscuit moringa leaf flour to the index value of erythrocytes Mean corpuscular Hemoglobin (MCH)Based on the results of the Wilcoxon test found the result that there is an average difference before and after the treatment of the group given biscuit moringa leaf flour from 27.55 to 28.00 with a mean difference value of 0.45 and p value=0.001, p<0.05 indicates that there is a difference in the value of MCH between before and after administration of the biscuit moringa leaf flour. The occurrence of increased MCH value in the biscuit moringa group makes the average value entered in the normal category than previously less than normal. In the control group the average change before and after treatment is from 26.85 to 26.87 with mean difference 0.02 and p value=0.584, p>0.05 means there is no significant difference before and after treatment in the control group.
The results of this study in line with the results of the research before by Idohou-Dossou et al., 2011 was found that a significant increase in the value of MCH in Moringa Oleifera group and control group, only different in the results of this research that control group increased but did not differ significantly from before and after treatment. This can occur due to the difference in the duration of administration and given dosage. In the study of Idohou-Dossou et al., 2011 Administration was conducted for 3 months and a given dosage of 100g of moringa leaves flour each week has consumed 3 times a day mixed in sauces or on slurries before they ate.11
Furthermore, the average intake of nutrients in the control group in the study is also still smaller than the intervention group and there is a meaningful difference in some nutrients such as protein, folic acid, zinc, iron, vitamin B1 and vitamin B2 which play an important role in the improvement of the indicator of anemia. However, it is not all nutrients that are fulfilled sufficiency needs each day, this can be caused most of the respondents have gestational age that is still in the I trimester because an estimated increase in Human Chorionic Gonadotropin (HCG) that occurs in the I trimester that leads to an increase in estrogen production is the cause of the emergence of nausea and vomiting symptoms that are very often encountered in about more than 70% of pregnant women.12 This is often what makes the pregnant women nutritional inadequate in I trimester.
Table 6 shows a significant difference in the mean difference value between the biscuit moringa group and the control group after The Mann Whitney analysis tested with p value=0.001, p<0.05. Moringa leaves contain a number of nutrients such as proteins, iron and vitamin C that could potentially prevent anemia more common in pregnant women.13 According to the conclusion of the results of the study conducted by Suzana et al., 2017 on the effect of Moringa leaf extract on hematology and biochemical values of patients with iron deficiency anemia that the water leaf extract supplementation of moringa as a natural supplement in addition to iron sulfate may help cope with iron deficiency anemia where the leaf extract of the moringa as an additional therapy provides an increase in the value of Hematocrit, MCH and MCHC.14
The effect of giving biscuit moringa leaf flour to the index value of erythrocytes Mean corpuscular Hemoglobin Concentration (MCHC)Based on the results of the test Paired T-Test found that there was no meaningful influence from before and after treatment in the biscuit moringa group and control group. However, both groups are both experiencing average value changes, seen in Table 4 in the biscuit moringa group occur the average value change from 33.27 to 33.41 with a difference of mean 0.14 and on Table 5 of the control group occur the average change from 33.28 to 33.36 with the mean difference of 0.08.
The need for red blood cells will increase because of the increase in physiological needs in the development of mothers and her baby. The mechanism of production of red blood cells is very complex and involves hormonal mediators such as erythropoietin, human placentals lactogen, estrogen and also progesterone. Although red blood cells are increased during pregnancy, the value of improvement differs from the increase in this plasma volume resulting in a rigid physiological anemia in pregnancy.15 so that after treatment the both groups have MCHC values persist in the normal state and increase but not significantly. Furthermore, the content of moringa leaves that have a multi-ingredient micronutrient substance that is needed by pregnant women such as: beta carotene, thiamin (B1), Riboflavin (B2), niacin (B3), calcium, phosphorus, magnesium, zinc those who maintain MCHC score have even fewer increase in biscuit moringa group.8
Difference with the research results of Suzana et al., 2017 where the study gained a significant increase in the MCHC value for the group that received Moringa Oleifera but decreased in the control group. Nutritional intake affects the results of this research. In research conducted by Hadju et al. (2015) for the administration of moringa leaf extract results in the erythrocyte value of both groups that also experienced an increase before and after administration but not significantly, and also no increase in differences between the two groups but able to increase hemoglobin levels significantly so that moringa leaves extract proved to prevent anemia in pregnant women.13
The effect of giving biscuit moringa leaf flour to the index value of erythrocytes Mean corpuscular Volume (MCV)Based on the data on Table 4 occurs an average increase and differs significantly from before and after administration on the biscuit moringa group from 78.57 to 78.93 with a difference of mean 0.36 and p value=0.034, p<0.05. In the control group also experienced an average increase from 77.92 to 77.94 with a difference of mean 0.02 and p value=0.881, p>0.05 that means did not differ significantly from before to after treatment. This results in line with the research conducted Adegbite et al. (2016) where there was a significant increase in the MCV value after given food with the addition of moringa leaf flour. This can happen because Moringa Oleifera has been found to contain alkaloids, flavonoids, phytosterols and saponins that are known to have hematopoietic properties. In addition to this bioactive substance in the leaves of Moringa Oleifera, it is also said to be A source of vitamins A, B, C, minerals such as iron and proteins that all contribute to the formation of erythrocytes especially in the formation of hemoglobin in the blood.16 In addition, due to the high level of sensitive MCV erythrocytes to the change of erythrocytes to determine the likelihood of iron deficiency affects these differences are supported also by the difference in iron intake among the biscuits moringa group and control group.14
Based on the data in Table 6 test results the difference of the mean biscuit moringa group and control group get the value p=0.003, p<0.05 which means there is a significant difference to the increase in MCV between the both groups. This can be due to the iron content of the 22.68ppm moringa biscuit tested proximate on the research by Dewi (2018) which is known to be used in preventing anemia in pregnant women.9 In addition, a meaningful mean difference in protein nutrient intake, folic acid, iron, vitamin B1 and vitamin B2 between the biscuit moringa group and the control group supports this to occur. According to the research results many mention the high content of protein, vitamin B, vitamin C and iron in the moringa leaves. The iron on the leaves of the dried moringa or in the form of moringa leaf flour is equivalent to 25 times higher than that of spinach and also used as alternative to prevent anemia in pregnant women naturally.17 This proved by the feeding of extra biscuits (cookies) moringa leaf flour able to improve the value of the MCV erythrocytes in pregnant women with anemia.
ConclusionThere is the effect of giving biscuits (cookies) Moringa leaf flour to the index of erythrocytes MCH and MCV in pregnant women with anemia. However, it has no effect on the MCHC value of pregnant women with anemia. It is recommended for pregnant women to utilize local plants moringa leaves to fulfill the intake of nutrients that can prevent pregnant women from anemia.
Conflicts of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











