



The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
More infoTeenagers are the second phase in life after the children's phase. The adolescent phase is called the transitional or transitional phase because in this phase it has not gained status as an adult but is no longer a childhood. The adolescent phase is called the critical period, a phase where there are many problems in growth and development, both physically, mentally, and in activities so that the need for food containing nutrients is large enough. Therefore, intervention efforts to improve adolescent nutrition are very necessary. The purpose of this study was to determine the effect of Moringa Oleifera leaf capsules on eating patterns in school drop-out adolescent girls aged 12–18 years in Polobangkeng sub-district, Takalar Regency, South Sulawesi Province.
MethodsThe study was a quasi experiment, the design used was Randomized Controlled Double-Blind Pre-Posttest. This research was conducted in Polobangkeng Utara Subdistrict, Takalar Regency, South Sulawesi on March 15, 2020 to May 23, 2020. The population in this study was all young women breaking up schools aged 12–18 years in Polobangkeng Utara District, Takalar Regency, South Sulawesi Province as many as 75 people. The sampling technique uses simple random sampling. Data were analyzed using the McNemar and Man Whitney tests.
ResultsMoringa leaf extract capsules of respondents who had a good diet before the intervention were 40% and less than 60% but after the intervention had a good diet as much as 100%. The Mc Nemar test p value was 0.004 which the p value α (0.05) which shows that there are differences in eating patterns before and after administration of Moringa capsule interventions. Whereas the TTD capsules of respondents who had a good diet before intervention were 26.6%. but changed to poor diet after intervention by 93.3%. Mc Nemar test p value is 0.125 which p value> α value (0.05) which shows that there is no difference in eating patterns before and after TTD capsule intervention.
ConclusionThere is an effect of giving Moringa leaf extract capsules to the diet seen from the average median value in the Moringa leaf extract capsule group is greater than 23 of the TTD capsule group which is 8 in teenage girls dropping out of school age 12–18 years in the North Polongbangkeng region Regency. Takalar, South Sulawesi.
Teenagers are the second phase in life after the children's phase. The adolescent phase is called the transitional or transitional phase because in this phase it has not gained status as an adult but is no longer a childhood. The adolescent phase is called the critical period, a phase where there are many problems in growth and development, both physically, mentally, and in activities so that the need for food containing nutrients is large enough. Increased need for nutrients that enter the body is used to increase body weight and height accompanied by an increase in the number and size of body tissue.1
Based on the Republic of Indonesia's Minister of Health Regulation No. 25 of 2014, adolescents are residents in the age range of 10–18 years. Where adolescence is a period of rapid growth and development both physically, psychologically, intellectually and requires a lot of intake of nutritional status.2 According to Asmani and Jamal (2012) at this time also became a period where adolescents learn and develop in identifying themselves and the surrounding environment, therefore the educational function is very important for adolescent development.3
Education can be obtained formally, nonformally and informally. School is a formal educational institution and in non-formal education is held for the community that functions as a substitute, supplementary or complementary formal education. Whereas informal education in the family is given by parents to teach and educate their children.4
Based on data from (Education Data Overview for Academic Year 2017/208, 2018) that the number of teenage girls dropping out of school for grade VI is 41.52%, SMP 35.30%, SMA 44.77% and SMK 34.53%. Meanwhile according to (Education Data and Statistics Center of FY 2017/2018, 2018) for South Sulawesi Province, teenage girls drop out of school for grade VI grade 27.5%, SMP 3.68%, SMA 4.24% and SMK 3.09%. Therefore, the development of the education sector needs serious attention from various parties, both students’ parents, the community and the government. For this reason, the government requires every Indonesian citizen to attend school for 12 years.5
Provision of proper nutrition for young women, in order to get a healthy and smart future generation. intervention efforts are needed to improve the nutrition of adolescents who will become prospective mothers and reduce fetal growth barriers that are right for developing countries if the acceleration is done before and during pregnancy, including the balance of protein energy, calcium and multimicro sufficiency.
A study by Lowell Fuglie, a French citizen who first examined the nutritional content of Moringa leaves showed that Moringa leaves did not contain any dangerous substances even though they contained substances that were bitter. In fresh Moringa leaves have high iron, protein, and vitamin C. This is what makes Moringa leaves as a raw material that has the potential to be used as functional food to overcome the problem of anemia. One of them, Moringa can be changed in the form of flour that can last for several months without cooling.6
Moringa oleivera or commonly known as Moringa leaf plant, is one source of nutrition that contains lots of vitamin A which is even 10 times better containing vitamin A even compared to carrots which are known to be rich in vitamin A one of the things what makes oleivera moringa become a worldwide concern and gives hope as a nutrient source plant that can save millions of humans from malnutrition, is moringa oleivera is rich and dense with nutrients and compounds that the body needs to be fit all parts of moringa oleivera can be used for healing, maintaining and improving the quality of human health and especially sources of family nutrition.7
Based on several studies and a series of explanations above, it is the background, so prospective researchers are interested in conducting research on the effect of giving Moringa leaf extract capsules on eating patterns in teenage girls who drop out of school.
Material and methodThis type of research is a Quasi experiment research. The design used was a randomized double-blind pretest–posttest controlled Double Blind meaning that the parties involved such as researchers, recipients did not know the difference between supplements and each package had a code on the label to ensure participants received the same preparation. This research was conducted in Polongbangkeng Subdistrict, Takalar Regency, South Sulawesi, from 15 March 2020 to 23 May 2020 after obtaining the Ethical Approval Recommendation issued by the Faculty of Public Health, Hasanuddin University, Makassar. The sample in this study was teenage girls dropping out of school aged 12–18 years in North Polongbangkeng Subdistrict, Kab. Takalar.total samples in this study were 30 people who were suitable based on inclusion criteria, then divided into two groups: 15 control group samples were given capsules (TTD) and 15 intervention group samples were given Moringa leaf extract capsules. After 60 days of intervention, dietary assessment, data processing and analysis are then performed.
Data collection techniqueData were obtained from Polobangkeng Utara sub-district, Takalar District, South Sulawesi Province and directly from respondents collected through questionnaire sheets, FFQ and 24-hour Food Recalls.
Data analysisThe data analysis test used Mc Nemar to see statistically significant changes in the two pairs of groups (before and after each group). Then Mann Whitney to see the statistical difference between the two unpaired groups (before and after between the intervention group and the control group).
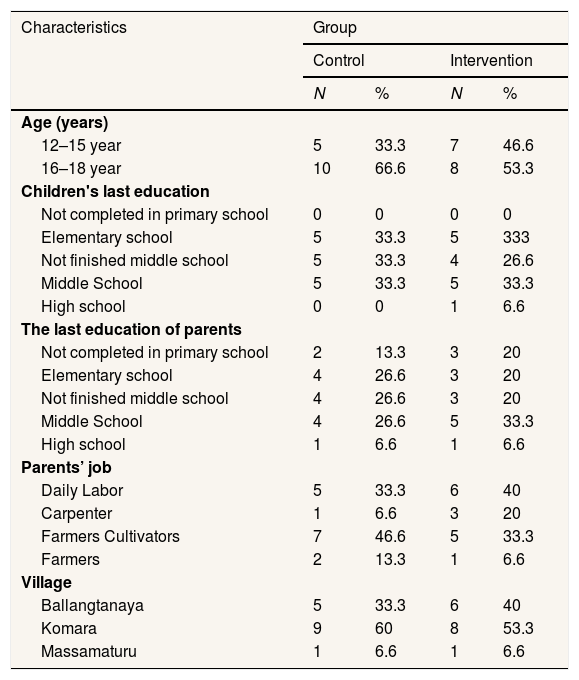
Research resultBased on Table 1, for the age group the majority of respondents in the control group were 12–15 years old or 33.3% while in the intervention group the majority were 16–18 years old or 53.3%. Then for the last education of respondents in the majority control group at the elementary level, not graduating from junior high and junior high as many as 5 people each with a percentage of 33.3% each, the intervention group also is the last education respondents are at the elementary and junior high school level of 5 people with a percentage of 33.3%. Furthermore, for the most recent education of parents in the control group, the majority were in the elementary stage, not completing junior and junior high school, each with 4% with a percentage of 26.6%, while for the majority of intervention groups for the final education of parents, namely 5 students or 33.3%. On the characteristics of the work of parents for the control group the majority have jobs as tiller farmers, as many as 7 people or 46.6% while for the intervention group the majority have jobs as daily laborers as many as 6 people or by 40%. Furthermore, for the village area where the sample/respondent is domiciled for the control group, the majority are in the Komara Village area as many as 9 people or as much as 60%, while for the intervention group the majority are in the Komara Village area as many as 8 people or as much as 53.3%.
Frequency distribution of respondent characteristics.
| Characteristics | Group | |||
|---|---|---|---|---|
| Control | Intervention | |||
| N | % | N | % | |
| Age (years) | ||||
| 12–15 year | 5 | 33.3 | 7 | 46.6 |
| 16–18 year | 10 | 66.6 | 8 | 53.3 |
| Children's last education | ||||
| Not completed in primary school | 0 | 0 | 0 | 0 |
| Elementary school | 5 | 33.3 | 5 | 333 |
| Not finished middle school | 5 | 33.3 | 4 | 26.6 |
| Middle School | 5 | 33.3 | 5 | 33.3 |
| High school | 0 | 0 | 1 | 6.6 |
| The last education of parents | ||||
| Not completed in primary school | 2 | 13.3 | 3 | 20 |
| Elementary school | 4 | 26.6 | 3 | 20 |
| Not finished middle school | 4 | 26.6 | 3 | 20 |
| Middle School | 4 | 26.6 | 5 | 33.3 |
| High school | 1 | 6.6 | 1 | 6.6 |
| Parents’ job | ||||
| Daily Labor | 5 | 33.3 | 6 | 40 |
| Carpenter | 1 | 6.6 | 3 | 20 |
| Farmers Cultivators | 7 | 46.6 | 5 | 33.3 |
| Farmers | 2 | 13.3 | 1 | 6.6 |
| Village | ||||
| Ballangtanaya | 5 | 33.3 | 6 | 40 |
| Komara | 9 | 60 | 8 | 53.3 |
| Massamaturu | 1 | 6.6 | 1 | 6.6 |
Primary data source 2020.
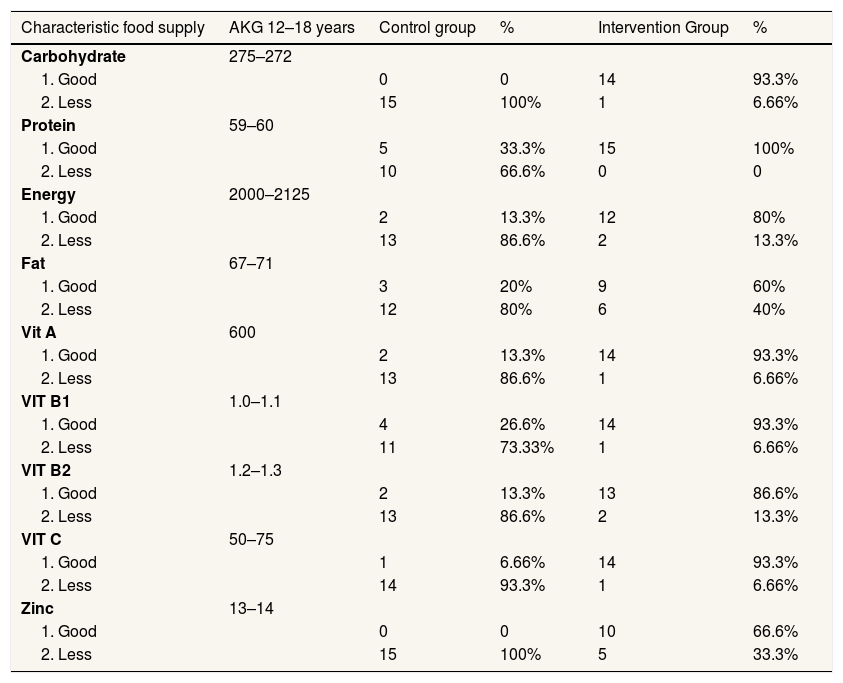
Based on Table 2 shows that after given intervention with Moringa leaf extract capsules in the control group and the intervention group. The intervention group had a good intake of carbohydrates as much as 93.3%, and the control group did not meet the intake criteria either. Whereas in protein intake, most respondents had a good intake of 33.3% in the control group and in the intervention group by 100%. The energy intake in the control group was good intake of 20% and 86.6% less while in the intervention group good intake as much as 80% and less as much as 13.3%. in the fat intake of the control group who had good intake as much as 20% and less as much as 80% in the intervention group of good intakes as much as 60% and less as much as 40%. 13.3% of good intake and 86.6% of lack in the good intake intervention group of 93.3% and 6.66% less than the intake of Vit B1 in the control group that was well-fed as much as 26.6% and less as much as 73.33% while in the intervention group that was well fed as much as 93.3% and less as much as 6.66%. In the intake of Vit B2 in the control group that was well as many as 13.3% and less as much as 86.6%. whereas in the intervention group, each intake was 86.6% and less was 13.3%. In the intake of Vit C in the control group, both intake was 6.66% and less was 93.3%. whereas in the intervention group, both intake was 93.3% and 6.66% lacking. Zinc intake in the control group did not have a good intake and was less than 100%, whereas in the intervention group, both intake was 66.6% and less was 33.3%.
Frequency distribution of respondents in the control and intervention group of young women dropouts in Polongbangkeng Utara District, Takalar Regency, South Sulawesi.
| Characteristic food supply | AKG 12–18 years | Control group | % | Intervention Group | % |
|---|---|---|---|---|---|
| Carbohydrate | 275–272 | ||||
| 1. Good | 0 | 0 | 14 | 93.3% | |
| 2. Less | 15 | 100% | 1 | 6.66% | |
| Protein | 59–60 | ||||
| 1. Good | 5 | 33.3% | 15 | 100% | |
| 2. Less | 10 | 66.6% | 0 | 0 | |
| Energy | 2000–2125 | ||||
| 1. Good | 2 | 13.3% | 12 | 80% | |
| 2. Less | 13 | 86.6% | 2 | 13.3% | |
| Fat | 67–71 | ||||
| 1. Good | 3 | 20% | 9 | 60% | |
| 2. Less | 12 | 80% | 6 | 40% | |
| Vit A | 600 | ||||
| 1. Good | 2 | 13.3% | 14 | 93.3% | |
| 2. Less | 13 | 86.6% | 1 | 6.66% | |
| VIT B1 | 1.0–1.1 | ||||
| 1. Good | 4 | 26.6% | 14 | 93.3% | |
| 2. Less | 11 | 73.33% | 1 | 6.66% | |
| VIT B2 | 1.2–1.3 | ||||
| 1. Good | 2 | 13.3% | 13 | 86.6% | |
| 2. Less | 13 | 86.6% | 2 | 13.3% | |
| VIT C | 50–75 | ||||
| 1. Good | 1 | 6.66% | 14 | 93.3% | |
| 2. Less | 14 | 93.3% | 1 | 6.66% | |
| Zinc | 13–14 | ||||
| 1. Good | 0 | 0 | 10 | 66.6% | |
| 2. Less | 15 | 100% | 5 | 33.3% |
Primary data source 2020.
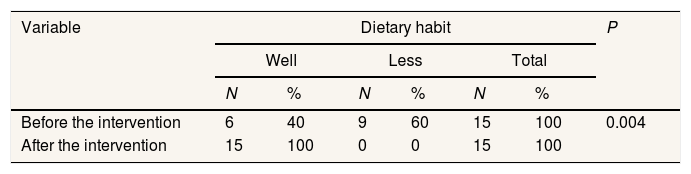
Based on Table 3 it can be seen that respondents who have a good diet before the intervention are 40% and less than 60% but after the intervention have a good diet as much as 100%. McNemar test p value is 0.004 which p value << α (0.05) which shows that there are differences in eating patterns before and after administration of Moringa extract capsule intervention.
Distribution of changes in respondents’ eating before and after in the extraction of kelor leaf capsules adolescent girls dropping out of school in Polongbangkeng Utara District, Takalar Regency, South Sulawesi.
| Variable | Dietary habit | P | |||||
|---|---|---|---|---|---|---|---|
| Well | Less | Total | |||||
| N | % | N | % | N | % | ||
| Before the intervention | 6 | 40 | 9 | 60 | 15 | 100 | 0.004 |
| After the intervention | 15 | 100 | 0 | 0 | 15 | 100 | |
Primary data source 2020.
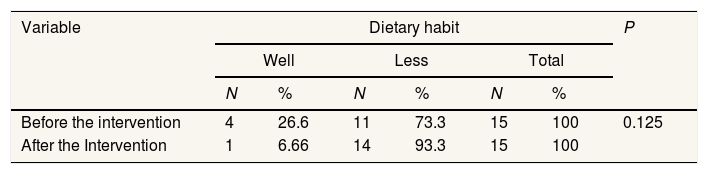
Based on Table 4 it can be seen that respondents who had a good diet before the intervention were 26.6%. but changed to poor diet after intervention by 93.3%. McNemar test p value is 0.125 which p value> α value (0.05) which shows that there is no difference in eating patterns before and after TTD capsule intervention.
Distribution of changes in respondents’ eating before and after in TTD capsules adolescent girls dropping out of school in Polongbangkeng Utara District, Takalar Regency, South Sulawesi.
| Variable | Dietary habit | P | |||||
|---|---|---|---|---|---|---|---|
| Well | Less | Total | |||||
| N | % | N | % | N | % | ||
| Before the intervention | 4 | 26.6 | 11 | 73.3 | 15 | 100 | 0.125 |
| After the Intervention | 1 | 6.66 | 14 | 93.3 | 15 | 100 | |
Primary data source 2020.
McNemar Test.
Note: TTD (tablets plus blood).
Table 5 shows that based on the Mann Whitney test on the tabell diet of the Moringa extract and TTD capsules group, the intervention group had an average Median value greater than the control, where the median intervention group was 23 while the control was only 8, so statistically more significantly between the intervention and control groups. which indicates that the administration of Moringa leaf extract capsules is better than (TTD capsules).
Distribution of differences in groups receiving Moringa leaf extract capsules and TTD capsules among female teenagers who dropped out of school in Polongbangkeng Utara District, Takalar Regency, South Sulawesi.
| Dietary habit | N | Mean rank | Sum of ranks | p Value |
|---|---|---|---|---|
| Intervention | 15 | 23.0 | 345.00 | 0.000 |
| Control | 15 | 8.00 | 120.00 | |
| Total | 30 |
Man Whitney Test.
Note: TTD (tablets plus blood).
Moringa leaves have a very good potential to complement the nutritional content in the body, increase energy and endurance of the body and to overcome complaints due to mineral deficiencies such as iron deficiency that causes anemia. The dried Moringa leaves have high levels of protein, iron, vitamin A and vitamin C, so it is very effective in treating iron deficiency anemia. In addition, this leaf does not contain harmful substances so it has no side effects. So far, no cases or poisonings have been found as a result of consuming Moringa leaves.
The consumption of Moringa oleifera leaves is one alternative to overcome cases of malnutrition in Indonesia. The results of modern scientific research prove that Moringa leaves are one of the sources of plant foods which are rich in nutritional content. Balbir S. Mathur's analysis results show that Moringa leaves have nutritional content that is very important to protect various diseases.
Based on the smear mc test in the intervention group it can be seen that respondents who had a good diet before the intervention were 40% and less than 60% but after the intervention had a good diet as much as 100%. McNemar test p value is 0.004 which p value value < α value (0.05) which indicates that there are differences in eating patterns before and after administration of Moringa capsule interventions.
This study is in line with other research studies, namely Yulianti (2016), Moringa leaves contain vitamins A, C, B, calcium, potassium, iron and protein in very high amounts that are easily digested and assimilated by the human body.8 Moringa leaves are the leaves of Moringa trees which contain various macro and micro nutrients as well as active ingredients that are as antioxidants containing important nutrients such as iron (Fe) 28.2mg, calcium (Ca) 2003.0mg and vitamins A 16, 3mg is rich in β-carotene, protein, vitamins A, C, D, E, K and B (thiamine, riboflavin, niacin, pantothenic acid, biotin, vitamins B6, B12 and folate).
Every part of M. oleifera is an important storehouse of nutrients and antinutrients. The leaves of M. oleifera are rich in minerals such as calcium, potassium, zinc, magnesium, andcopper iron. Vitamins like beta-carotene vitamin A, vitamin B such as folic acid, pyridoxine and nicotinic acid, vitamins C, D and E are also present in M. oleifera. Phytochemics such as tannins, sterols, terpenoids, flavonoids, saponins, anthraquinones, alkaloids and reducing sugars are present with anti-cancer agents such as glucosinolates, isothiocyanates, gly-coside compounds and glycerol-1-9-octadecanoate. Moringa leaves also have a low calorific value and can be used in those diets that are obese.9
Vitamins are organic substances that act as coenzymes or regulators of metabolic processes and are very important for many vital bodily functions. Moringa contains Vitamins: A (Alpha & Beta-carotene), B, B1, B2, B3, B5, B6, B12, C, D, E, K, Folic Acid, Biotin.9
Because it has been proven by several studies of substances contained in Moringa leaf extract capsules it has been proven to have an influence to improve diet (frequency and increased portion of food) after intervention. Besides resting and eating healthy foods such as vegetables and fruits is a factor additional.
The effect of TTD capsules on teenage girls dropping out of school before and after the interventionIron (Fe) is needed in the body for growth, helps the work of various enzymes in the body, tackling infections, helping the intestines neutralize toxins and most important for the formation of hemoglobin.10
Based on the McNemar test in the control group it can be seen that respondents who had a good diet before the intervention were 26.6%, but changed to poor diet after intervention by 93.3%. McNemar test p value is 0.125 which p value > α value (0.05) which indicates that there is no difference in eating patterns before and after TTD capsule intervention.
Iron has properties that cannot be produced by the body, so we must meet the needs of iron from food. In the body, iron has a function related to the transportation, storage and utilization of oxygen and is in the form of hemoglobin, myoglibin or cytochrome. To meet the needs for the formation of hemoglobin, most of the iron derived from the breakdown of red blood cells will be utilized again, then the deficiencies must be met and obtained from food. The level of iron nutrition for a person is strongly influenced by the amount of consumption through food, the part that is absorbed through the digestive tract, iron reserves in the tissue of excretion and body needs.11
Arini Research Results (2018) about the effect of Moringa oleifera leaf flour on the increase in hemoglobin (Hb) levels in anemic female adolescents in Tamalate Sub-District, Jeneponto District, the results of the study showed that in the intervention group were 24 respondents and 24 control groups respondents, the intervention group Moringa leaf flour consumed at a dose of 2×2 capsules in the morning and evening. Changes in Hb levels in the control group of 14 people (58.3%) with an increase in Hb levels of 0.3–3.5 g/dl which were not given Moringa leaf flour, while in the intervention group changes in Hb levels by 22 people (91.7%) with an increase in Hb levels of 1.5–2.2g/dl after Moringa leaf flour is given.
Because it has been proven by several studies and based on the results of tests on the control group (TTD capsules) found no effect of giving TTd capsules on diet before and after the intervention.
Difference in changes in the group receiving Moringa leaf extract capsules with TTD capsules against teenage girls dropping out of school before and after the interventionFrom the results of the above study, we can see that after the intervention of Moringa extract capsules and TTD capsules in teenage girls dropping out of school age 12–18 years old, North Sumatra gets results that there are differences in the administration of Moringa extract capsules to young women before and after the intervention.
Showed that based on the Mann Whitney test on the table diet of the Moringa extract and TTD capsules group, the intervention group had an average Median value greater than the control, where the median intervention group was 23 while the control was only 8, so that it was statistically more significant between the intervention and control groups. which indicates that the administration of Moringa leaf extract capsules is better than (TTD capsules).
A good eating pattern that is meeting the intake, frequency and type of food can affect a person's nutritional status, because a balanced pattern of feeding that is in accordance with the needs accompanied by the selection of the right food ingredients will give birth to a good nutritional status. Basically, a person's nutritional status is determined based on nutritional consumption and the body's ability to use these nutrients. Normal nutritional status indicates that the quality and quantity of food that has fulfilled the body's needs.
The intake of nutrients (energy, protein, fat and carbohydrates) in the food consumed daily has a huge impact on a person's nutritional status because it will affect the energy balance which has an impact on the occurrence of nutritional problems. Someone needs a number of nutrients to be able to live healthy and be able to maintain their health. Nutrients obtained through food consumption must be suitable and sufficient for the body's needs.
Research conducted by Srikanth et al. (2014), Nutritional intervention with moringa leaf powder (Moringa oleifera) showed significant weight gain among children and adolescents with protein energy malnutrition. Moringa leaf powder can be effectively used for the treatment of malnutrition by spreading awareness about the nutritional value of Moringa oleifera leaves to mothers, children and adolescents.
According to research Yulianti (2016), Moringa leaves contain vitamins A, C, B, calcium, potassium, iron and protein in very high amounts that are easily digested and assimilated by the human body.8 Moringa leaves are the leaves of Moringa trees which contain various macro and micro nutrients as well as active ingredients that are as antioxidants containing important nutrients such as iron (Fe) 28.2mg, calcium (Ca) 2003.0mg and vitamins A 16, 3mg is rich in β-carotene, protein, vitamins A, c, D, e, K and B (thiamine, riboflavin, niacin, pantothenic acid, biotin, vitamins B6, B12 and folate). Various types of antioxidant compounds such as ascorbate acid, flavonoids, phenolics and carotenoids.
In the process of giving Moringa leaf extract capsules to young women, education is first given about the benefits of Moringa leaves themselves so that young women understand and are willing to consume extract capsules. After being educated, we conduct partnerships with local village officials or cadres to monitor the compliance of capsule consumption once a week and also we monitor by phone or whatsApp group every night with 2×1 consumption rules for 60 days at a dose of 1000mg per day.
By giving 2×1 moringa leaf extract capsules at a dose of 1000mg per day for 2 months or 60 days is considered to have a significant effect. Thus, proving that the content of Vit C, Vit B1, Vit B2 V B6, Zinc, carbohydrates, proteins and energy in Moringa leaf extract capsules can affect diet.
Conclusion- 1.
Giving Moringa leaf extract capsules affect to improve diet after 2 months of intervention.
- 2.
Giving Moringa leaf extract capsules greater effect to improve diet compared to administration of capsules (TTD).
The authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











