




The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
More infoThis study aimed to determine the differences in midwives’ knowledge, attitudes, motivation and abilities regarding maternal health care after an intervention.
MethodsThis was an experimental research study with a quasi-experimental pretest–posttest design with a control group. The sample of this study was 66 midwives in Jeneponto Regency; 33 midwives comprised the control group, and 33 comprised the treatment groups. The sampling technique was purposive. This study was conducted at six primary health care in Jeneponto Regency.
ResultsThis study shows that there were differences between the midwives in the treatment and control groups in mean knowledge, motivation, attitude and ability regarding health care for pregnant women before and after health education (p<0.005); the increase in the service abilities of midwives after the Ammuntuli Bija intervention models indicates that the intervention is truly working. The components that showed significant changes (p<0.05) were knowledge (p=0.024), motivation (p=0.046) and ability (p=0.017).
ConclusionThe models and modules provided were capable of increasing the knowledge, motivation and ability of midwives in maternal health care. Comprehensive efforts, cross-sector support and supporting regulations are needed.
To achieve the target of the sustainable development goals (SDGs), joint efforts are needed between the distributors of limited resources, academics and policy makers. Health monitoring by policy makers can shift the focus more towards resources and implementation efforts by involving the community in providing health services to disadvantaged and marginalized populations. Achieving targets and accelerating progress in reducing maternal and newborn deaths requires an understanding of good services before and during pregnancy and after childbirth.1
A total of 287,000 mothers die every year throughout the world. Most maternal deaths are the result of direct obstetric causes.2 The mortality of Sub-Saharan African mothers is 510 per 100,000 live births, and the maternal death rate in South Asia is 90 per 100,000 live births. Previous research reported that only 42% of pregnant women gave birth in health service facilities, and only 34% of women received postnatal care from trained medical providers within 48h after giving birth.3
The World Health Organization (WHO) has identified several ways to reduce and prevent pregnancy-related morbidity and mortality, including implement the following: (1) access to antenatal care during pregnancy, (2) skilled midwives present during childbirth, and (3) postnatal care in the days and weeks after birth.4 Related efforts to prevent health problems have been made in various cases, including educating cooks about cardiovascular disease.5
Home visit programmes are recommended to improve maternal and child health services. Home visit programmes are conducted in Uganda, Bangladesh, India and Pakistan by community health cadres or village health teams. They are designed to address public health problems.6 However, it is also understood that in certain cases, natural conditions do not affect the incidence of an illness.7
Health workers are an important component of a system for reducing maternal and infant mortality. The health system will function properly if supported by qualified health personnel. To provide good service, health workers must have good motivation and attitudes. In low- and middle-income countries, the performance and behaviour of health workers, who are less frequently reported as contributing factors, reduce the quality of health services. One solution to the low level of service provided by health workers is to improve their performance and behaviour.8
Midwives play an important role in reducing maternal and infant morbidity and mortality6. Previous studies found that home visits can identify various problems that cause low-quality health care for pregnant women.9–11
The 2012 Indonesian Demographic and Health Survey showed that the maternal mortality rates (related to pregnancy, childbirth, and childbirth) amounted to 359 per 100,000 live births.12 Maternal mortality in South Sulawesi Province in 2014 was 138 people, or 93.20 per 100,000 live births. Jeneponto Regency (193/100,000 live births) had the fourth-highest mortality after Bone (240/100,000 live births), Gowa (240/100,000 live births), and Luwu (293/100,000 live births).13
The high maternal mortality rate in Jeneponto Regency is due to bleeding, eclampsia, infectious diseases, late referrals and low competence among midwives. This lack of competence can is evident in the fact that despite the large number of midwife services, the quality of health services in Jeneponto Regency is still low.14 The health service programme for pregnant women has not run optimally.15
The ability of a midwife is an important key to the success of health services, including the increased ability of midwives in the health services provided for pregnant women. The aim of this study was to determine the influence of biological models on the knowledge, attitudes, motivation and abilities of midwives in health services for pregnant women in Jeneponto Regency.
MethodsExperimental site and designThis study had a quasi-experimental pretest–posttest design with a control group. The study was conducted in Jeneponto Regency, Indonesia. The sample of this study was 66 midwives in Jeneponto Regency; 33 midwives comprised the control group, and 33 comprised the treatment group.
Data collection procedureData from this study were collected using questionnaires. The respondents were surveyed before (pretest) and after (posttest) the implementation of the Ammuntuli Bija intervention model.
Variable measuredThe main parameters measured in this study were the knowledge, attitude, motivation of the midwives in pregnancy care as well as the accessibility and capacity of midwives providing health services to pregnant women.
Statistical analysisSPSS was used for the statistical analysis. The Mann–Whitney statistical analysis was conducted to test the hypothesis.
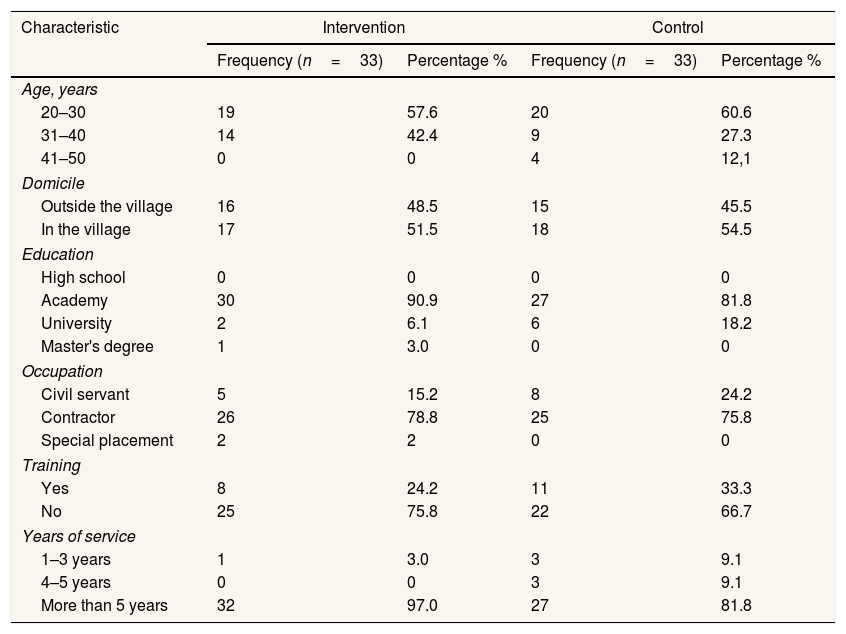
ResultTable 1 shows that in the intervention group, the largest age group was the 20–30 years group, with 19 people (57.6%). A total of 17 participants lived in the village (51.5%); the highest education level was D-III, with a total of 30 people (90.9%); and the most common job title was PTT, with a total of 26 people (78.8%). Respondents who had more than 5 years of work experience comprised 32 people (97.0%); the majority had never had any training (25 people; 75.8%).
Characteristics of the respondents in Jeneponto Regency.
| Characteristic | Intervention | Control | ||
|---|---|---|---|---|
| Frequency (n=33) | Percentage % | Frequency (n=33) | Percentage % | |
| Age, years | ||||
| 20–30 | 19 | 57.6 | 20 | 60.6 |
| 31–40 | 14 | 42.4 | 9 | 27.3 |
| 41–50 | 0 | 0 | 4 | 12,1 |
| Domicile | ||||
| Outside the village | 16 | 48.5 | 15 | 45.5 |
| In the village | 17 | 51.5 | 18 | 54.5 |
| Education | ||||
| High school | 0 | 0 | 0 | 0 |
| Academy | 30 | 90.9 | 27 | 81.8 |
| University | 2 | 6.1 | 6 | 18.2 |
| Master's degree | 1 | 3.0 | 0 | 0 |
| Occupation | ||||
| Civil servant | 5 | 15.2 | 8 | 24.2 |
| Contractor | 26 | 78.8 | 25 | 75.8 |
| Special placement | 2 | 2 | 0 | 0 |
| Training | ||||
| Yes | 8 | 24.2 | 11 | 33.3 |
| No | 25 | 75.8 | 22 | 66.7 |
| Years of service | ||||
| 1–3 years | 1 | 3.0 | 3 | 9.1 |
| 4–5 years | 0 | 0 | 3 | 9.1 |
| More than 5 years | 32 | 97.0 | 27 | 81.8 |
In the control group showed that the most age group was the 20–30 age group with 20 people (60.6%), 18 people living in the village (54.5%) with the highest education level were D III with 27 people (81.8%), the most work was PTT with the number 25 people (75.8%), and respondents who had a service period of more than 5 years were 32 people (97.0%) who had never attended training, with 27 people (81.8%).
Table 2 shows that there were differences in the knowledge, motivation and ability between the treatment group and the control group after the implementation of the intervention. The variables knowledge, motivation and ability showed significant differences (p<0.05); however, there was no difference in attitudes or access to the workplace between the treatment group and the control group after the intervention.
Differences in knowledge, motivation, attitude, access and ability between the treatment group and the control group after intervention in Jeneponto Regency.
| Variable | Group | Mean rank | Elementary school | p |
|---|---|---|---|---|
| Knowledge | Treatment (Model+Module) | 38.64 | 1,264 | 0.024* |
| Control (Module) | 28.36 | |||
| Motivation | Treatment (Model+Module) | 38.17 | 2,671 | 0.046* |
| Control (Module) | 28.83 | |||
| Attitude | Treatment (Model+Module) | 32.61 | 4,000 | 0.704 |
| Control (Module) | 34.39 | |||
| Access | Treatment (Model+Module) | 33.50 | 0,000 | 1.000 |
| Control (Module) | 33.50 | |||
| Ability | Perla kuan (Model+Module) | 39.09 | 5,105 | 0.017* |
| Control (Module) | 27.91 |
* Mann–Whitney test.
Organizational determinants play an important role, especially in providing adequate resources to support teamwork, human resource management and leadership. As suggested by policy makers, the government must encourage the scope and utilization of the workforce by updating policies, for example, by implementing a programme to increase staff and facilities in environments with a persistent lack of midwives and facilities.15
In terms of respondent characteristics such as age, domicile, occupation, education, training funds, most of the respondents were aged 21–30 years (57.6%), lived in the village (51.5%) had a diploma-level education (90.9%), and worked as contract health professionals (78.8%); a total of 32 respondents had served for more than 5 years (97%). The majority of the participants, 25 (75.8%), had never attended training. In the control group, the largest age group was 21–30 years, with a total of 20 people (60.6%). Eighteen people lived in the village (54.5%); the highest education level was D-III, with 27 people (81.8%); and the largest job category was non-permanent employees, with 25 people (75.8%). Thirty-two respondents (97.0%) had a service period of more than 5 years, and the majority had never attended training (27 people; 81.8%).
In this study, the most favourable characteristics were found in the youngest age group (21–30 years). This greatly facilitates the transfer of information because at these age, individuals can still relatively easily gain knowledge and change.
Age affects knowledge because increasing age brings physical, psychological and psychological change. Psychologically, a person's level of thinking is becomes more mature with age.16
In practice, the characteristics that influence the attitudes of nurses in service are age, education, functional position, and length of work experience; for doctors, the influencing characteristics are age, education and length of work experience.17 This study found similar influencing characteristics, namely, age, education and years of service.
The result of this study showed that a person's beliefs are very necessary to the effective involvement in service. Sometimes, newly graduated midwives lack confidence in their services, and this can interfere with the provision of safe and effective health services. Therefore, an intervention is needed that can help new graduates develop knowledge and experience regarding services for pregnant women, and thus increase their confidence.18
This condition is also in accordance with the concept of Notoadmojo indicating that experience factors can affect knowledge. A health worker with >5 years of experience can be assumed to have more knowledge than a worker with <5 years of work experience. The more experience a person has, the more his or her knowledge will increase.19
KnowledgeThe results of the Mann–Whitney test are shown in Table 2. The value was ρ=0.024; the value (p<0.05) with a mean difference of 1.264 indicates that there was difference between the treatment group and the control group after the implementation of the Ammuntuli Bija model. This intervention model uses local sentences, which is expected to better facilitate local implementation. It is appropriate to conclude that health problems can be resolved more effectively by taking into account the local context than by using medical treatments.20
Knowledge refers to what is known and remembered after experiencing, watching, observing or being taught from birth to adulthood, especially after receiving formal or informal education. Knowledge is the result of knowing, and this happens after people have sensed an object.
Knowledge can be interpreted as a result of knowing, which occurs after sensing. Sensing occurs through the human senses, namely, the senses of sight, hearing, smell and touch. Most human knowledge is obtained through the eyes and ears through both formal and informal education.
Efforts to improve maternal health services can take various forms. One strategy is training activities. In some cases, the training and development of health services have not been fully implemented despite the knowledge that education (counselling) has an influence on knowledge and attitudes.21,22 Knowledge, skills and motivation correlate with the performance of midwives; in contrast, work time does not.23
Training to be one of the meninges efforts ka VING knowledge and skills of midwives in maternal health services, the results of research that an increase in the average knowledge and skills of midwives in maternal health services in the district Jeneponto.24 Therefore, a midwife must have broad knowledge of services, especially midwifery, obtained through both formal education and informal education. In addition, a midwife must be highly motivated to provide good midwifery services to patients.15
MotivationThe results of the Mann–Whitney test are shown in Table 2. The value ρ=0.046 reflects a value of p<0.05 with a mean difference of 2.671, which indicates that there was a difference in the midwives’ motivation regarding health care for pregnant women between treatment group and the control group after the implementation of the Ammuntuli Bija model.
Motivation is an internal and external impulse to make a change in behaviour. It has the following indicators: (1) the desire to perform an activity, (2) the presence of encouragement and the need to perform activities, (3) the existence of hopes and dreams, (4) the presence of respect for others and respect for oneself, (5) the existence of a good environment, and (6) the existence of interesting activities.25
According to Berelson and Steiner in Makruf and Siswanto, motivation is an inner state that gives strength, which activates or moves; hence, it is called “mobilization” or “motivation”. This state directs or channels behaviour towards goals. From the definition above, it can be said that among village midwives, motivation is a condition that can give the midwives strength, enthusiasm, courage to be honest and enjoyment of what they do, which leads them to achieve a high level of performance.
Motivational factors are related to what is done (job content), namely, the content of the work that encourages achievement. Motivational factors are intrinsic, originating in the individual; they are also called the content factor of the work.26
AttitudeThe results of the Mann–Whitney test are shown in Table 2. The value ρ=0.704 reflects a value (p>0.05) with a mean difference of 4.000, which indicates the presence of a difference in attitudes between the treatment group and the control group after the implementation of the Ammuntuli Bija model. Attitude is an evaluation statement describing a relatively consistent feeling or tendency regarding an object or idea; attitude is also a feeling that arises within a person after seeing, feeling and enjoying an object. Attitudes can be considered a willingness to react to an object, including people, events, institutions, values and so on.27
According to Notoadmojo, an attitude does not necessarily translate into an action; for an attitude to transform into a real action, supporting factors or conditions that allow for supportive facilities or infrastructure are needed.
The respondents’ attitudes towards labour delivery services are not surprising; their feelings arise because they recognize that as health workers, when they arrive to help with a delivery, their appearance should be neat and clean, and they should provide opportunities for the families to accompany them during labour. This good attitude, in addition to encouraging patients to ask for the respondents’ help, can also lead to increased coverage of health workers, especially midwives, which means that the risk of death for pregnant women can be reduced as much as possible.28
The attitude of health workers in health care facilities affects the frequency of ANC visits for pregnant women. The better the attitude of health workers, the more often a pregnant woman will visit a health facility to have her pregnancy checked. The unevenness of health workers in remote areas can also reduce access to health services for pregnant women.29 In addition to attitudes and priorities, is the ability to communicate is an important characteristic among health workers.30
Health workers with better attitudes increase pregnant women's participation in antenatal care visits, while those with worse attitudes reduce participation in antenatal care visits. This is in accordance with Lawrence Green's theory that a reinforcing attitude among health workers can influence behaviour change.31
AccessThe results of the Mann–Whitney test are shown in Table 2. The value ρ=1.000 reflects a value of p>0.05, indicated that access to maternal health services did not differ between the treatment and control group after the implementation of the Ammuntuli Bija model. The concept of access to health services refers to the patient's ability to obtain a health service from a health facility. In this study, researchers limited access to ease of service coverage, distance travelled, travel time and transportation used to reach the health service.32
The results of the WHO study stated that although the awareness and knowledge of people in developing countries are already quite high, they have difficulty engaging in healthy behaviours if health facilities are not affordable. Access to health services encompasses several concepts: respondents’ perceptions of cost and transport issues based on travel time to health facilities in minutes (≤30min, 31–60min, >60min) or hours, the distance in kilometres (<1km, 2–3km, 4km), or the degree of transportation difficulty (close, sufficient, far). Gambia found that factors that inhibit access to health services and midwives include time, transport issues, distance, and economic limitations.33–36
In line with the results of research conducted by Karman in South Konawe Regency, the variables distance, travel time and mode of transportation from the respondent's residence to health services have a significant influence on the utilization of health services.37
Distance creates a disturbance because it takes time and energy (costs) to travel from one location to another. In addition, distance also creates information disturbances so that the further away from a location, the less value associated with that location. The farther the distance to be travelled, the lower a person's interest in travelling will be, assuming other factors are all the same.38
Furthermore, health care facilities increasingly support the need for regular antenatal care. Transportation difficulties or long travel times may make a pregnant women reluctant to visit a health service for regular pregnancy checks.31
Midwives’ abilityThe results of the Mann–Whitney test are shown in Table 2. The value ρ=0.017 reflects a value (p<0.05) with a mean difference of 5.105, which indicates a difference in ability between the treatment group and the control group after the implementation of the Ammuntuli Bija model.
The Ammuntuli Bija model was very important for improving the results of health services for patients/clients and families. Competence specifically identifies knowledge, skills, attitudes, values, and dynamic evaluations of development and evolution.
Competence is defined as the abilities needed to perform work tasks based on knowledge, skills and work attitudes. Thus, competence can be defined as a person's observable ability, including knowledge, skills and work attitudes to complete a job or task in accordance with established performance standards.
Another explanation for the importance of ability was proposed by Muchlas, who stated that the higher an employee's abilities, the more tasks or jobs he or she can complete within a certain period, which shows that ability affects the quantity of work an employee can perform.39
This study has various limitations, namely, the small sample, which could not reveal the complete picture of health care for pregnant women. Activities in daily health services in Pustu and Poskesdes allow for limited intervention and communication time when conducting research; thus only a few aspects of health care services for pregnant women could be observed, and environmental, social, economic and family support factors were not addressed. Additionally, the lack of role exchange across sectors (such as the private sector, NGOs and fields and institutions such as agriculture, education, BKKBN, social, Empowerment Women, Ministry of Religion, PKK Enforcement Teams, Posyandu Cadres and government officials such as village/district) contribute to the less-than-optimal health services for pregnant women.
ConclusionThe conclusion of this study shows that the Ammuntuli Bija model increased the knowledge, motivation and ability of midwives providing health services for pregnant women in Jeneponto Regency. The findings support the use of the Ammuntuli Bija model as a reference for midwives to improve health services for pregnant women in Jeneponto Regency.
Conflicts of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











