




To obtain versions of the Primary Care Assessment Tools (PCAT)-Facility version to evaluate primary care (PC) in the Spanish context, and to analyze its feasibility, reliability and validity.
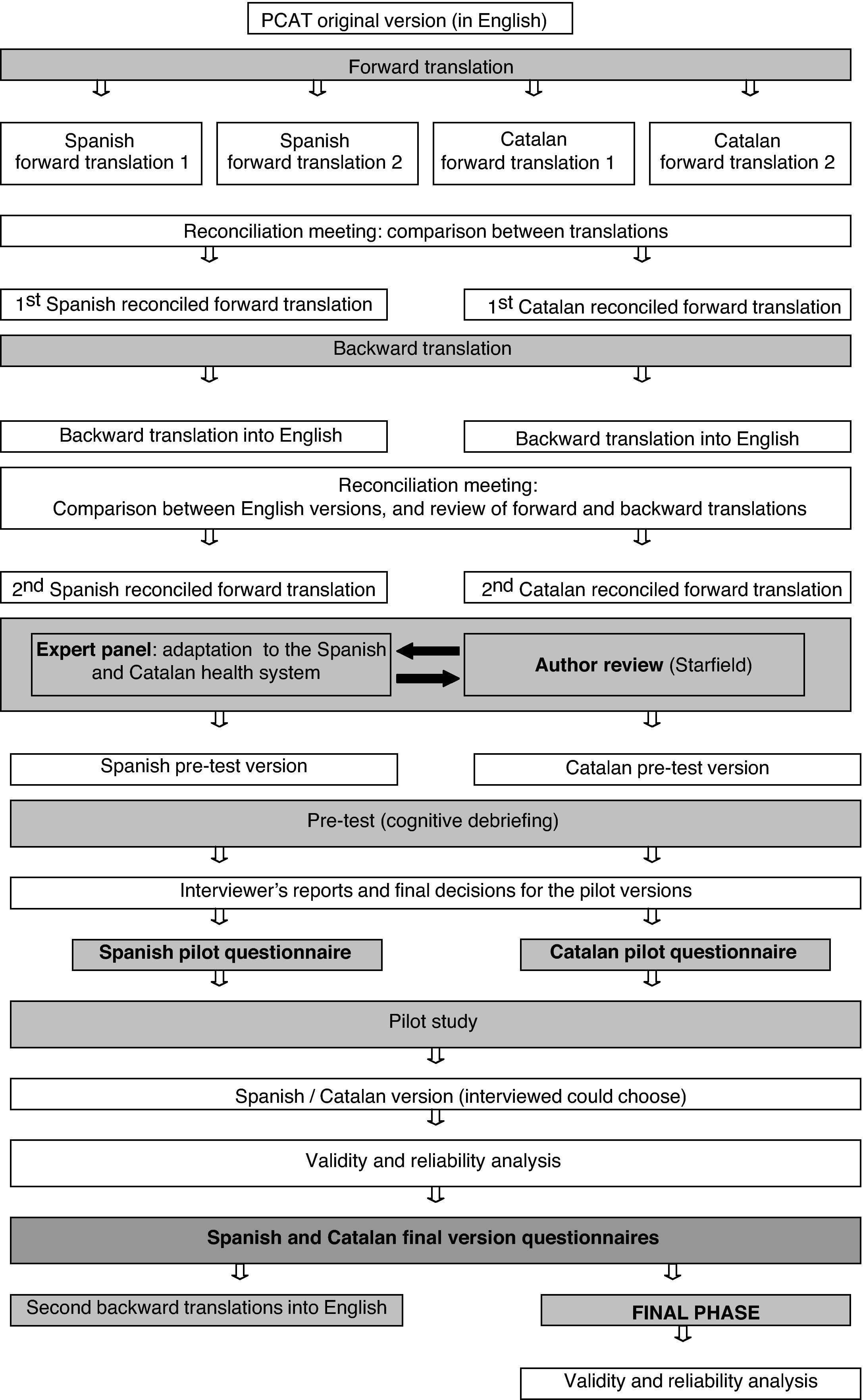
MethodsCultural adaptation was performed through the use of forward and backward translations into Spanish and Catalan, observations and opinions of a panel of experts, and cognitive interviews with target users (PC team managers). A pilot phase was carried out in a sample of 130 managers of PC teams in Catalonia. A post-test questionnaire was sent 4-5 months later to all 194 managers of PC teams in the Barcelona health region. Analysis of metric properties included: 1) description of items and verification of Likert assumptions, since domain scores are obtained by summing item scores; 2) reliability analysis (Cronbach's alpha coefficient, Pearson's correlation coefficient, test-retest analysis); and 3) validity analysis (expert panel, cognitive interviews, and convergent and discriminant validity).
ResultsSubstantial adaptation was required for the accessory section of the questionnaire, but less was required in PC domain measurements. Items were added to the comprehensiveness domain to reflect services usually available in Spain. The lowest Cronbach's alpha scores were found for Access (0.62) and Coordination (0.59 and 0.65), while values were >0.70 for the remaining domains.
ConclusionThe Spanish version of the PCAT-Facility questionnaire is now available and shows adequate reliability and validity. The Spanish PCAT version will facilitate national and international comparisons of PC and analysis of the determinants of quality of service provision.
Obtener versiones del Primary Care Assessment Tools–Facility version como herramienta de evaluación de la atención primaria (AP) para la aplicación en el contexto español, y analizar su fiabilidad y validez.
MétodosSe realizó una adaptación cultural con traducciones y retrotraducciones al español y al catalán, observaciones y opiniones de un panel de expertos y entrevistas cognitivas con usuarios finales (directivos del equipo de AP). Se realizó una fase piloto con una muestra de 130 directivos de AP de Cataluña. Una versión final se envió 4-5 meses después a los 194 directivos de los equipos de la región sanitaria de Barcelona. El análisis de las propiedades métricas incluyó: 1) descripción de ítems y verificación de las asunciones de la escala Likert, porque las puntuaciones de los dominios se obtienen sumando los ítems; 2) análisis de fiabilidad (alfa de Cronbach, coeficiente de correlación de Pearson, análisis test-retest); y 3) análisis de validez (panel de expertos, entrevistas cognitivas, validez convergente y discriminante).
ResultadosSe requirió una importante adaptación de las secciones accesorias del cuestionario, pero no en las de los dominios de AP. Se añadieron ítems en la dimensión de globalidad. Las menores puntuaciones del alfa de Cronbach se encontraron en acceso (0,62) y coordinación (0,59 y 0,65); el resto de los dominios tuvieron valores > 0,70.
ConclusiónDisponemos de una versión española del PCAT - Equipo de Atención Primaria con unas adecuadas fiabilidad y validez, que facilitará comparaciones nacionales e internacionales, y el análisis de los determinantes de una provisión de servicios de calidad.
A strong primary care (PC) with a high capacity for resolving problems can modulate the use of the rest of the health system, making the system more efficient.1,2 Until now, few studies have attempted to assess the strength of PC because of an unclear conceptualization and specification of its component attributes.3 Moreover, very little use is made of tools that are able to measure the multiple functions of PC or which allow comparison between countries or systems. Although some instruments are already available to measure core attributes of PC4, they are not widely disseminated, nor have they been adapted and validated to obtain equivalent measures in distinct countries.
Starfield's theoretical model defines a number of core and ancillary domains that PC should accomplish.5 For the core domains, PC should be the point of entry into the health system (except for emergency situations); provide care focused on the person, which is longitudinal (based on a long-term personal relationship), and should be comprehensive, and coordinated with other levels of care. For the ancillary domains, PC should focus on the health of individuals in the context of their family and community and be able to adapt and develop a relationship with the various social groups present in the community, demonstrating cultural competence.
The Primary Care Assessment Tools (PCAT) was developed to address that assessment model for PC domains.6,7 Three versions were developed to allow evaluation from the points of view of the population (consumer version), managers (facility version) and health professionals (provider version). The consumer version has been applied in the USA,6,8,9 Brazil,10 Canada,11 Korea,12 Hong Kong,13 and Taiwan,14 and several other countries are currently working on it (Uruguay, Argentina, China, etc.).15,16. In Spain, a brief version of the PCAT-consumer version was included in the 2006 Catalan Health Interview Survey.17–19
The Spanish General Health Service Act (1986) establishes a national health system composed of 17 regional health services. The Spanish health system is financed mainly by taxes and provides universal and free health coverage, including primary, specialized and hospital care.20 Catalonia is one of the regions with transferred health responsibilities within Spain and has two official languages, Spanish and Catalan.
For evaluation of health services, equivalent instruments are essential. Originally designed for the USA, a cross-cultural adaptation of the PCAT is needed when used in other contexts. The general objective of this study was to obtain and evaluate an instrument to assess the domains of primary care (accessibility, continuity, comprehensiveness, coordination, family-centeredness, community orientation and cultural competence) that are useful for the Spanish health system. The specific objectives were to adapt the PCAT to the Spanish health system and culture and to analyze its feasibility, reliability and validity. This article describes the adaptation process that may be useful in other contexts because it followed international recommendations for cross-cultural adaptations,21,22 adding a specific step of health system adaptation, in order to ensure the equivalence between PC measures in an international context.
MethodsA cross-cultural adaptation process was conducted to obtain versions of the PCAT - Facility questionnaire to be applied in the Spanish National health system and to test its reliability and validity. The procedure followed is represented in figure 1. Since this study was conducted in Catalonia, the Castilian (Spanish) and Catalan languages were used because they are the main official languages spoken in this autonomous region, language being the only difference between Spanish health regions relevant to the measure of PC.
The PCAT Facility Questionnaire
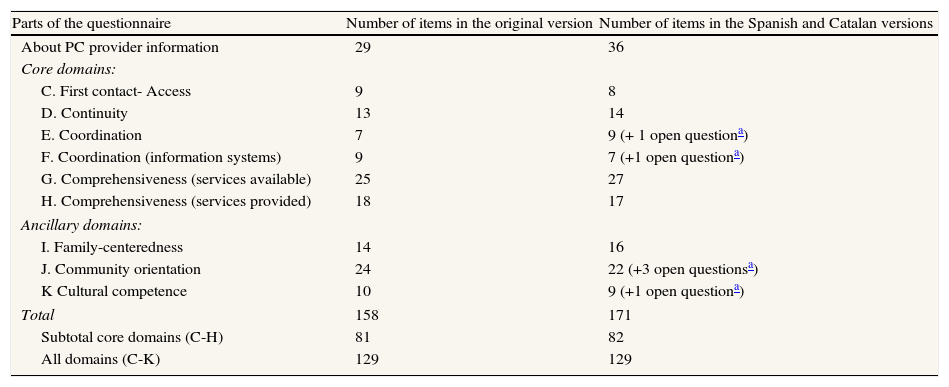
The original questionnaire measures seven domains of PC (two of them divided in two subdomains), through 158 items (Table 1). Each item is answered by a 4-point Likert-type scale (1=definitely not; 2=probably not; 3=probably; 4=definitely). The score of each domain is the arithmetic mean of its item responses.23 Two global scores can be calculated, one reflecting the score for core domains, the other a summary of all domains. In both cases, scores were calculated as the average of scores from the domains included. The questionnaire includes 29 additional questions about the characteristics of the PC provider and its potential users. The original version is designed to be answered by the PC team director, or another professional in the center able to answer questions about the center's characteristics and services offered to the population covered. The Spanish version was prepared to be answered by PC team managers or coordinators.
Structure of the Primary Care Assessment Tools (PCAT) - Facility extended version questionnaire: the original, in English, and the final Spanish and Catalan versions. Number of items in different sections.
| Parts of the questionnaire | Number of items in the original version | Number of items in the Spanish and Catalan versions |
| About PC provider information | 29 | 36 |
| Core domains: | ||
| C. First contact- Access | 9 | 8 |
| D. Continuity | 13 | 14 |
| E. Coordination | 7 | 9 (+ 1 open questiona) |
| F. Coordination (information systems) | 9 | 7 (+1 open questiona) |
| G. Comprehensiveness (services available) | 25 | 27 |
| H. Comprehensiveness (services provided) | 18 | 17 |
| Ancillary domains: | ||
| I. Family-centeredness | 14 | 16 |
| J. Community orientation | 24 | 22 (+3 open questionsa) |
| K Cultural competence | 10 | 9 (+1 open questiona) |
| Total | 158 | 171 |
| Subtotal core domains (C-H) | 81 | 82 |
| All domains (C-K) | 129 | 129 |
Two trilingual (English, Spanish and Catalan) translators worked on the original English version and each translator produced one Spanish and one Catalan version. Subsequently, the translators met with the research team to obtain one agreed version in Spanish and one in Catalan. Through discussion, items were categorized as presenting: a) no problems, b) some language or cultural problems, and c) no cultural equivalence, i.e. items related to the USA health system not applicable to Spain.
From the agreed version, a back translation into English was obtained (through a native-born English translator), and a final meeting was held with the research team and all translators in order to compare the original English version with the English back translation version to check the semantic equivalence between the original and the adapted questionnaires. The team agreed on amendments and the Spanish and Catalan versions of the questionnaire went through the next step.
For the adjustment of the questionnaire to the Spanish health system, a panel of PC experts was held to: 1) assess the suitability of each item within the health system (content validity), and 2) propose new items to add when needed. The panel was composed of three PC professionals (a general practitioner-director of a PC team, a general practitioner with experience in managerial aspects of PC at the regional level, and the third was a physician with experience in research on PC), and three public health professionals (one of whom had experience in PC evaluation and the others were experts in evaluation and measures). From this phase a pre-pilot version was obtained.
Feasibility and understanding of the questionnaireFinally, a pre-test including a cognitive interview was conducted to test the feasibility and understanding of the pre-pilot version. Semi-structured individual interviews were conducted with six directors of PC teams in the public system. These directors were asked to complete the questionnaire and were later asked for their opinions on and experience of completing the questionnaire. From this phase a pilot version was obtained.
Study of metric properties of the questionnaireAll the analyses were done at two time points, i.e. with the pilot version of the questionnaire and with the final version. The pilot questionnaire was sent to a sample of 130 managers of PC teams in Catalonia (one of Spain's 17 autonomous regions). The final version was mailed to the 194 managers of PC teams in the Barcelona health region (the largest health region in Catalonia, with a population of over 5 million), 56 of which had responded to the pilot questionnaire.
Likert scaling assumptions were tested as item responses are summed in each score without standardization or weighting. We analyzed the following elements: a) item-convergent validity (tested by item-scale correlations); b) item-discriminant validity (the correlation of each item with its own domain score should be higher than with other domains); c) analysis of variance for equal items, calculating the mean, standard deviation and percentage of variability of each item; d) equal item-score correlation (tested by the range of correlations between each item and its domain score); and e) domain score reliability (tested by Cronbach's alpha coefficient).6
The reliability of the domain scores was measured through test-retest and internal consistency. Test-retest stability was measured by comparing the responses of the 56 people who completed both the pilot version and the final version 4-5 months afterwards. This period was chosen to be long enough to avoid a relevant memory effect in the response to items, but at the same time short enough to reduce the likelihood of changes occurring which could cause problems with internal validity. The means of the domain scores were compared (T-test for paired data), and the intraclass correlation coefficient (ICC) was calculated. The occurrence of any significant changes in the PC team (composition, organization, etc.) was also determined. To identify internal consistency, Cronbach's alpha coefficients of the scales and item-total correlations for items in each domain were calculated. A Cronbach's alpha between 0.70 and 0.95 was expected,24 while the total correlation between an individual item and the sum of the remaining items of the domain was expected to be>0.20, and preferably>0.30.22 For each domain, the percentages of PC teams with domain scores equal to 1 and to 4 were determined; a ceiling or floor effect was considered to be present when the corresponding percentage was >15%.22
The content validity of the scales measuring PC domains was assessed by using both the information collected from the panel of experts and the results of the cognitive interviews. Construct validity was analyzed throughout the measures of convergent validity and discriminant validity explained above. Finally, criterion validity was approximated through the correlation between the score value for the Accessibility domain and a question, not forming part of any PCAT domain, which asked whether the center was open 24hours a day.
ResultsCultural adaptationThe forward-backward translations showed low difficulty and high linguistic equivalence according to the translators’ evaluations. Some exceptions were items on the characterization of PC services and population. The major change made in this phase was the exclusion of items that were only applicable to the US health system. Those items belonged to the accessory section of the questionnaire, not to the PC attributes section. Another change made was the addition of new items to collect features of the national health system in Spain such as the goal of universal coverage. The Spanish and Catalan versions showed similar results, with few important discrepancies among experts. The only concept that required discussion in the translation process was the “special test”, because in Spanish and Catalan professional jargon the term used is “complementary test”.
The expert panel also proposed modifications. For example, references to the weekend were separated into “Saturday” and “Sunday”, as some PC centers may be open on Saturday but generally not on Sunday. Major changes were made in the Comprehensiveness attribute, with some items excluded (such as colonoscopy, which is not usually done in Spanish PC) and other items added for their importance in the Spanish context (e.g. advice on alcohol consumption, acenocumarol monitoring and eye examination for diabetes). In table B of the appendix in online version, those items are marked with “m” (modified, 1 item) or “n” (new/added, 14 items).
Feasibility and understanding of the questionnaireCognitive interviews showed that an average of 37.4minutes was needed to complete the questionnaire. The degree of difficulty was rated as very low (mean=1.2 on a scale of 0, no difficulty, to 5, very difficult), while the degree of understanding of questions was high (mean=4). In addition, the level of interest of questions was moderate/high (mean=3.5) and language appropriateness was good/moderate (mean=3.8).
Metric properties of the questionnaireThe comprehensive results of the analysis by item, given their length, are available exclusively in the online version of this work.
The response rate of the pilot phase was 80% (105 of 130 questionnaires). The analysis performed yielded similar results to those obtained with the final version, which is described below. Most of the changes were in items not related to PC domains, and most of them were not part of the original PCAT (table A of the appendix in online version, lists the changes emerging from the pilot phase). The final version was answered by 68.6% (133 of 194) managers of the PC teams.
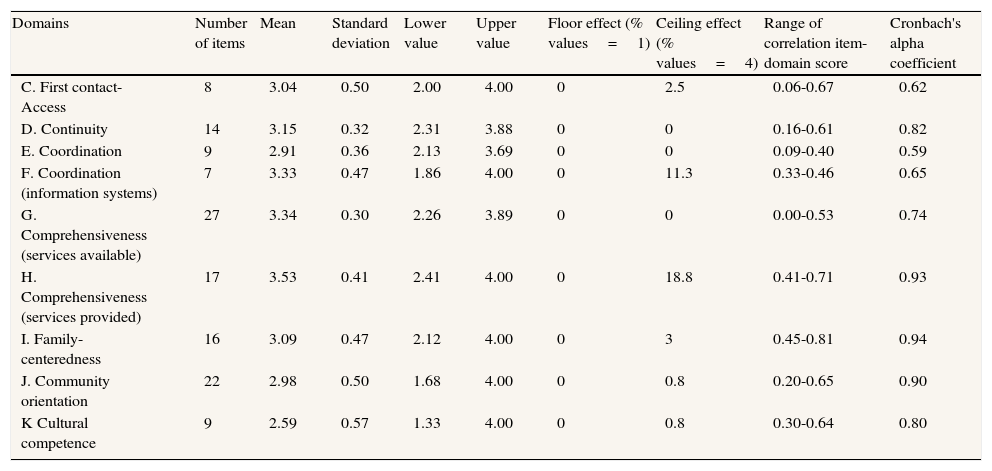
None of the items measuring PC domains presented problems of non-response, while some showed low variability, especially in the Comprehensiveness domain (table B of the appendix in online version). In the item-total correlation analysis, 84% of the items (n=108) showed Pearson correlation coefficients ≥0.20, and 81% (n=105) ≥0.30, while over 95% (n=123) showed correlations of each item with its scale that were higher than with other dimensions.
Cronbach's alpha coefficient was >0.70 for the scores for most the domains, but was lower for Accessibility (0.62) and Coordination (0.59, and 0.65 in the subdomain of coordination-information systems) (Table 2). The internal consistency of Accessibility (0.62) increased to 0.65 if item C1n1 (center opens every Saturday) was excluded. None of the domains showed a floor effect, but in Comprehensiveness (services provided), 18.8% of teams showed the maximum value (4).
Summary measures of domains in the Spanish version of the Primary Care Assessment Tools (PCAT) - Facility.
| Domains | Number of items | Mean | Standard deviation | Lower value | Upper value | Floor effect (% values=1) | Ceiling effect (% values=4) | Range of correlation item-domain score | Cronbach's alpha coefficient |
| C. First contact- Access | 8 | 3.04 | 0.50 | 2.00 | 4.00 | 0 | 2.5 | 0.06-0.67 | 0.62 |
| D. Continuity | 14 | 3.15 | 0.32 | 2.31 | 3.88 | 0 | 0 | 0.16-0.61 | 0.82 |
| E. Coordination | 9 | 2.91 | 0.36 | 2.13 | 3.69 | 0 | 0 | 0.09-0.40 | 0.59 |
| F. Coordination (information systems) | 7 | 3.33 | 0.47 | 1.86 | 4.00 | 0 | 11.3 | 0.33-0.46 | 0.65 |
| G. Comprehensiveness (services available) | 27 | 3.34 | 0.30 | 2.26 | 3.89 | 0 | 0 | 0.00-0.53 | 0.74 |
| H. Comprehensiveness (services provided) | 17 | 3.53 | 0.41 | 2.41 | 4.00 | 0 | 18.8 | 0.41-0.71 | 0.93 |
| I. Family-centeredness | 16 | 3.09 | 0.47 | 2.12 | 4.00 | 0 | 3 | 0.45-0.81 | 0.94 |
| J. Community orientation | 22 | 2.98 | 0.50 | 1.68 | 4.00 | 0 | 0.8 | 0.20-0.65 | 0.90 |
| K Cultural competence | 9 | 2.59 | 0.57 | 1.33 | 4.00 | 0 | 0.8 | 0.30-0.64 | 0.80 |
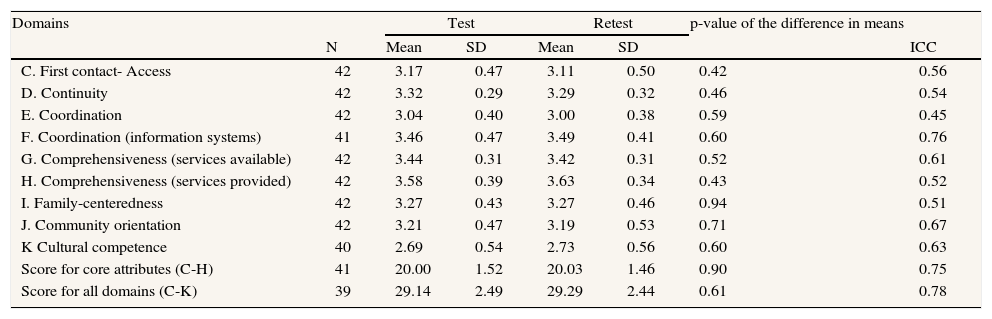
Analysis of test-retest reliability (Table 3) showed no significant differences for any domain between the two time points. For overall scores (score for core domains, and score for all domains), the ICC was >0.75. The highest score was for Coordination (adequacy of information systems) with an ICC >0.70, while the lowest were for Coordination of care (0.45) and Family orientation (0.51).
Reliability measures in the test-retest analysis.
| Domains | Test | Retest | p-value of the difference in means | ||||
| N | Mean | SD | Mean | SD | ICC | ||
| C. First contact- Access | 42 | 3.17 | 0.47 | 3.11 | 0.50 | 0.42 | 0.56 |
| D. Continuity | 42 | 3.32 | 0.29 | 3.29 | 0.32 | 0.46 | 0.54 |
| E. Coordination | 42 | 3.04 | 0.40 | 3.00 | 0.38 | 0.59 | 0.45 |
| F. Coordination (information systems) | 41 | 3.46 | 0.47 | 3.49 | 0.41 | 0.60 | 0.76 |
| G. Comprehensiveness (services available) | 42 | 3.44 | 0.31 | 3.42 | 0.31 | 0.52 | 0.61 |
| H. Comprehensiveness (services provided) | 42 | 3.58 | 0.39 | 3.63 | 0.34 | 0.43 | 0.52 |
| I. Family-centeredness | 42 | 3.27 | 0.43 | 3.27 | 0.46 | 0.94 | 0.51 |
| J. Community orientation | 42 | 3.21 | 0.47 | 3.19 | 0.53 | 0.71 | 0.67 |
| K Cultural competence | 40 | 2.69 | 0.54 | 2.73 | 0.56 | 0.60 | 0.63 |
| Score for core attributes (C-H) | 41 | 20.00 | 1.52 | 20.03 | 1.46 | 0.90 | 0.75 |
| Score for all domains (C-K) | 39 | 29.14 | 2.49 | 29.29 | 2.44 | 0.61 | 0.78 |
SD: standard deviation; ICC: intraclass correlation coefficient.
The questionnaire's content validity was checked and increased during the phase in which the expert panel adjusted the adaptation of items to the Spanish and Catalan health system, taking into account the theoretical model.
For construct validity, item-scale correlations, already mentioned in reference to internal consistency, are shown in the table B of the appendix in online version. Seventeen items (13%) showed low item-convergent validity (Pearson's r <0.20) in the dimensions of Access (5 items), Continuity (1 item), Coordination (1 item), and Comprehensiveness- services available (10 items). A total of 24 items (18.6%) showed a Pearson's r <0.30. When discriminant validity was analyzed, some items had a moderate or high correlation (coefficient >0.30) with another dimension than with that expected: in the domains of Access (item C4), Continuity (D4), Coordination (E12), Coordination-systems information (F6), Comprehensiveness- services available (G19,G23), and Community-oriented (J1n, J13).
Finally, the correlation between reported Access attribute and the PC team being located in a 24-hour center was 0.65, providing some evidence of criterion validity.
DiscussionPC evaluation should involve multiple perspectives and tools.25–27 This study describes an instrument to measure whether PC provision achieves the standards of the theoretical model. A review highlighted the PCAT, as the only tool that includes psychometrically tested domains for all of the PC core domains and is available in multiple and comparable formats (for providers as well as users).4 The PCAT measures the key characteristics of PC defined by the World Health Organization-Europe,28 as well as other basic components of particular interest for Spain, such as Family-centeredness and Cultural competence.
The method used for obtaining the Spanish version ensures equivalence with the original. All the analyses conducted with the items, as well as the test-retest analysis, indicate the good reliability of the questionnaire. The PCAT-Facility has shown acceptable convergent validity (81% of items showed item-total correlation, with Pearson's correlation coefficients ≥0.30)22 and good discriminant validity (in 95% of cases, the correlation of each item with its scale was higher than with other domains), as well as good internal consistency in most of the domains (Cronbach's alpha coefficient >0.70).24 Repeatability was less good (ICC <0.70),22 which may be due to the difficulty of choosing a suitable time lapse between the two measures. When health effects are measured in people, a 2-week lapse has been reported to be advisable, but in the case of measures of the health system we have found no references on a recommended period. The period used may have been too long.
The use of the PCAT adapted to Spain allows comparison between our health system and others, which is the main reason to adhere to the original instrument. There are other tools, such as PC Monitor,29 to compare PC in distinct countries, but PCAT specifically provides assessment of the theoretical components that should be met by PC. The PCAT instrument has already been validated for assessing the theoretical model of PC,5 making it suitable for use in different contexts. In Spain, there is extensive experience of having adapted and validated instruments designed in other contexts, especially in the field of measuring health and quality of life,30–32 but there is less experience in the field of health services evaluation, specifically PC, and fewer tools for international comparability are available.
As expected, the main differences between the original instrument and its Spanish adaptation are in sections concerning aspects of organization and structure of PC teams and their assigned populations. For the sections of PC domains of the questionnaire, the Spanish version of the PCAT-Facility shows good linguistic and conceptual equivalence with the original. The low variability in some items can be explained by the homogeneity of PC teams, since many aspects of PC provision and functioning are determined by the system not by the team (e.g. items related to the services covered). We decided to maintain these items to allow international comparability.
The main weakness of the instrument obtained concerns its criterion validity; being a new instrument, there are no other good measures to obtain evidence about this feature. Even so, the result of the approximation used, consisting of correlating the score for accessibility to the fact that the center is open 24hours, suggests confidence in the measure. The results for the questionnaire's content validity are considered appropriate, firstly, because the original questionnaire was designed by one of the authors (Starfield) and the consumer version has already been validated in the English version,6 and secondly the members of the research team and expert panel that collaborated in the adaptation phases are knowledgeable about the PC model and functioning in Spain and, more specifically, in Catalonia.
In the measure of PC domains, Comprehensiveness -subdomain services provider- showed a ceiling effect; one of the reasons could be the above-mentioned homogeneity of the public healthcare system in specifying the services portfolio covered. Comparing different systems or suppliers outside the public system would probably result in less homogeneity. Continuity, Family-centeredness, Community orientation and Cultural competence had the best Cronbach's alpha results (0.82, 0.94, 0.90 and 0.80, respectively) and showed no ceiling effects. In the Spanish health system, these PC attributes are less determined by the system and depend more on the dynamics and organization of each team. The PCAT-Facility in Brazil, the only country with published results on its psychometric properties, showed that the dimensions of access, comprehensiveness and community orientation had Cronbach's alpha scores close to 0.70, but the remaining dimensions had scores below 0.60.33 Similarly, in the Spanish PCAT, coordination has a Cronbach's alpha score under 0.60, but in all the other domains, our scores are higher.
The results should be analyzed in light of the existing organizational system, given that some aspects of services provision will be determined by distinct levels: the macro-system organization, the provider, and the organization of the PC team. Finally, it is important to acknowledge that the provision of care will ultimately depend on the professionals providing the care.
Importantly, the PCAT-Facility version assumes a certain homogeneity among the distinct professionals within the PC team, and those completing the questionnaire could have been biased toward the mean or otherwise have tended to respond positively.
Given the response rate obtained, nearly 70%, and the good results (not shown) of a comparative analysis between the total sample and that finally obtained with respect to geographical area and type of healthcare provider, we are confident that the sample on which the tests were based did not show a sufficient selection bias to influence the psychometric characteristics obtained by the questionnaire.
We conclude that, even taking into account the limitations of this study, we have an instrument with which to expand the scope of PC assessment, with adequate reliability and validity. Moreover, we believe this instrument could be especially useful as it is feasible to implement (being completed by the PC team manager/coordinator), requires only about 35minutes to complete and presents low difficulty. This questionnaire also provides a measure of the domains of PC with good reliability, and their assessed validity has been partly corroborated by the analysis performed.
This instrument could be useful for national (at the regional level) and international comparisons, especially in light of the World Health Report 2008 on primary care.34 In addition, the PCAT could be used to ascertain whether the results for the PC domains are associated or not with the characteristics of the team and/or the population, and an inequality perspective can be introduced in this analysis. Furthermore, the PCAT could be useful to monitor the health system, at PC level, especially in the present context, with the current economic crisis provoking changes in the health system.
¿What is known about this topic?
Evaluating public services, in this case primary care (PC), has always been important and is even more so in the context of the current crisis. There is a theoretical model for the basic domains of PC. PC domains have been well defined: PC should be accessible, should provide longitudinal as well as comprehensive and person-focused care, and should be coordinated with other levels of care. Furthermore, PC should focus on the health of individuals in the context of their family and community and should show cultural competence. However, research has not addressed these functions with valid tools. The Primary Care Assessment Tools grew out of this model and is increasingly used internationally.
¿What does the present study add?
This study provides a new tool for the assessment of PC in the Spanish context, the Primary Care Assessment Tools (PCAT), which is used in PC teams, and provides information on its reliability and validity. So far, no published studies have evaluated a full version of the PCAT-Facility, with high equivalence to the original version. Consequently, our study could be useful to researchers from other nations. This instrument will allow evaluation of PC domains in Spain and facilitate comparisons with other settings where this tool has been applied (Brazil, Canada, USA, Argentina, etc.).
M.I. Pasarín and S. Berra conceived the project and the article. M.I. Pasarín, S. Berra, A. Segura, A. García-Altés and B. Starfield participated in the study design, in the definition of the analysis strategy and in the discussion of results. M.I. Pasarín wrote the first draft of the manuscript. All the authors critically reviewed the manuscript. A. González performed most of the fieldwork and analyzed the data, guided and supervised by M.I. Pasarín and S. Berra. M.I. Pasarín conducted the interviews in the fieldwork. A. Gonzalez, C. Tebé and I. Vallverdú participated in the definition of the analysis strategy and discussion of the results and critically reviewed the manuscript. All the authors approved the final version.
FundingThis study was partially funded by the Fondo de Investigaciones Sanitarias [proyecto FIS number 052763] and the CIBER de Epidemiología y Salud Pública (CIBERESP).
Conflict of interestNone.
The authors thank the managers of the primary healthcare teams that completed the questionnaire and all those who participated in some phases of this study (interviews and expert panel).

Prof. Barbara Starfield passed away on June 10, 2011, only days before the last version of this paper was finished. With these lines, all the authors wish to recognize and thank her for her important contributions to our work, as well as to primary healthcare in Spain and in many other countries around the word. We greatly appreciate her generously open attitude and her unfailing willingness to collaborate and share her knowledge. Many thanks Professor Barbara Starfield!











