



The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
More infoThis study aimed to determine the relationship between eating habits and hyperemesis gravidarum with preeclampsia incidence.
MethodThis study used a cross-sectional design. The total sample was 48 pregnant women with normal and preeclamptic pregnancies who had a gestational age above 20 weeks, collecting data using a questionnaire and data analysis using the chi-square test and odds ratio (OR).
ResultsThe habit of eating irregular fruit during pregnancy was significantly associated with the incidence of preeclampsia, with an OR value of 8.57. Mothers who had hyperemesis gravidarum increased their risk 3.86 times for developing preeclampsia.
ConclusionEating habits and history of hyperemesis gravidarum is a risk factor of preeclampsia. Nutritional intervention is needed through nutrition education for pre-pregnant women so that their nutritional adequacy during pregnancy can be fulfilled, especially during the 1st trimester, namely the implantation phase and socialization of the community movement program for healthy living, especially the consumption of vegetables and fruits for women of childbearing age, women during pre-pregnancy, pregnant and breastfeeding.
Preeclampsia (PE) is the most common problem of various hypertensive disorders of pregnancy and is estimated to affect 2–10% of pregnant women.1 Preeclampsia is a major cause of fetal morbidity and mortality and accounts for 15–20% of maternal deaths worldwide.2 The incidence of preeclampsia in African countries such as South Africa, Egypt, Tanzania, and Ethiopia varies from 1.8% to 7.1%. The prevalence of preeclampsia in Nigeria ranges from 2% to 16.7%. The incidence of preeclampsia varies widely around the world. Approximately 50,000 deaths worldwide each year are related to PE,3 so reducing maternal mortality by 75% between 1990 and 2015 is part of the Millennium Development Goals (MDGs) of the World Health Organization (WHO).4
The WHO estimated the incidence of preeclampsia is seven times higher in developing countries (2.8% of live births) than in developed countries (0.4%). The condition of preeclampsia that is not appropriately treated will lead to eclampsia. The incidence of eclampsia in developed countries, such as North America and Europe, was estimated to be around 5–7 cases per 10,000 births. On the other hand, the incidence of eclampsia in developing countries varies widely, ranging from 1 case per 100 pregnancies to 1 case per 1700 pregnancies. The incidence of PE in African countries such as South Africa, Egypt, Tanzania, Ethiopia varies from 1.8% to 7.1%. In Nigeria, the prevalence of preeclampsia ranges from 2% to 16.7%.4 In Indonesia, the incidence of preeclampsia continues to increase. Based on household health survey data in 1995, there were three main causes of maternal death, namely bleeding (45%), infection (15%), and hypertension in pregnancy (preeclampsia) 13%. The 2001 household health survey results showed that 50% of deaths were caused by bleeding (27%) and eclampsia (23%), while 11% of deaths were due to infection. This showed that the causes of maternal death due to bleeding and infection could be significantly reduced, in contrast to preeclampsia sufferers, due to ignorance and often late seeking help after clinical symptoms develop into severe preeclampsia and eclampsia, the incidence increases.
Risk factors for preeclampsia include nulliparous pregnancy, Gemelli pregnancy, history of preeclampsia in a previous pregnancy, obesity, diabetes mellitus, blood vessel and connective tissue disorders, such as systemic lupus erythematosus and antiphospholipid antibodies, age >35 years at first pregnancy, smoking, lifestyle and African American race.5 Unfortunately, many of these risk factors are non-modifiable or very difficult to modify, especially during pregnancy.
The role of oxidative stress or lipid peroxidation excess has been implicated in preeclampsia. There is an imbalance between antioxidant enzyme activity and pro-oxidant production. In preeclamptic pregnant women, the plasma levels of a thiobarbituric acid reactive substance (a marker for lipid peroxidation) were increased, while the total glutathione peroxidase decreased significantly. Increased levels of lipid peroxidase will also activate the coagulation system, resulting in platelet aggregation and thrombus formation. Nutrients can affect oxidative stress by increasing or decreasing free radicals or antioxidants, providing substrates for the formation of free radicals, or modulating the functions of antioxidant enzymes. For instance, lipids are extensively involved in the generation of free radicals. Antioxidants (vitamin C, E, alpha- or betacarotene, copper, selenium, zinc, etc.) can indirectly or directly scavenge free radicals or function as essential substrates or cofactors for the adequate functioning of antioxidant enzymes. Therefore, adequate dietary antioxidant intake is crucial for maintaining pro-oxidant and antioxidant balance since some nutrients are not synthesized in humans. It has also been suggested that nutrients such as trace elements, fatty acids, and folic acid can contribute to insulin resistance, a risk factor for PE.6
Nutritional factors are important things that can affect the success of a pregnancy process and prevent pregnancy complications and fetal disorders. Nutrition is a factor that can be modified during pregnancy to prevent preeclampsia compared to other risk factors. Without realizing it, pregnant women may experience a relative deficiency of trace elements, which is related to nausea and vomiting that occurs in early pregnancy, especially in hyperemesis gravidarum. Usually, pregnant women, when nauseous and vomiting, tend to be picky about types of food and usually only consume dry foods to avoid nausea and vomiting. There is an association between hyperemesis gravidarum and placental dysfunction disorders, especially in women with hyperemesis gravidarum in the second trimester. This is very likely to cause pregnant women to lack nutrients in minerals and vitamins that affect the mother and fetus.7
Trace element deficiency during pregnancy is closely related to morbidity and mortality in newborns.8 Lack of particular antioxidant activity associated with the micronutrients selenium, copper, zinc, and manganese can result in poor pregnancy outcomes, including fetal growth retardation,9 preeclampsia,10 and associated increased risk of disease adulthood, including heart disease and type 2 diabetes.11–14 The contribution of macronutrients to the success of pregnancy has recently begun to be researched, which focuses on the role of certain important micronutrients because certain micronutrients are an absolute requirement and are required only in small amounts each day.15
Research results found an association between hyperemesis gravidarum and diseases associated with placental dysfunction (preeclampsia, placental abruption, stillbirth, and small for gestational age (SGA)). This association was robust in women who experienced hyperemesis gravidarum in the second trimester.16 Others also showed that preeclampsia could also predispose the fetus to increase the risk for cardiovascular disease in adulthood,17 so detecting the occurrence of preeclampsia can help early management to reduce morbidity and mortality in mothers and babies, and become the basis for making preventive efforts so that cardiovascular disease does not occur in the future.
Preeclampsia and eclampsia are still diseases of theory, so further research is still needed. Preeclampsia is a complex disease. In many cases, the clinical manifestations are unpredictable, but they affect the health of the mother and fetus. Therefore, routine screening for preeclampsia through blood pressure measurement in all pregnant women should be carried out as recommended by WHO. In addition, urine protein checks should be carried out routinely every antenatal visit for pregnant women in developing countries to complement blood pressure checks. This study aims to determine the relationship between eating habits and hyperemesis gravidarum with the incidence of preeclampsia.
MethodThis type of research was an analytic observational study with a cross-sectional design. This research was conducted from November to December 2017 in Kendari City, namely the working area of the public health center of Poasia, Mekar, Lepo-Lepo, and the public hospital of Kendari City. The sample in this study were pregnant women with preeclampsia and normal pregnancies. The total sample was 48 pregnant women. The sample was selected pregnant women with gestational age ≥20 weeks who had obtained informed consent and signed consent to participate in the study. Sampling was carried out by consecutive sampling: every pregnant woman with a gestational age ≥20 weeks who came to the examination. Collecting data using a questionnaire instrument compiled by the researcher. The process of collecting data in the field was carried out by midwives who served in the public health center and hospital, which were the research locations. Before data collection was carried out, a common perception was made for the midwives who will collect the data. Data analysis used the chi quadrat test and odds ratio (OR).
ResultsThe sample in this study were pregnant women with the category of normal pregnancy and pregnancies with preeclampsia. The data collected was then analyzed using STATA software. The results of data analysis are displayed in tabular form accompanied by an explanation.
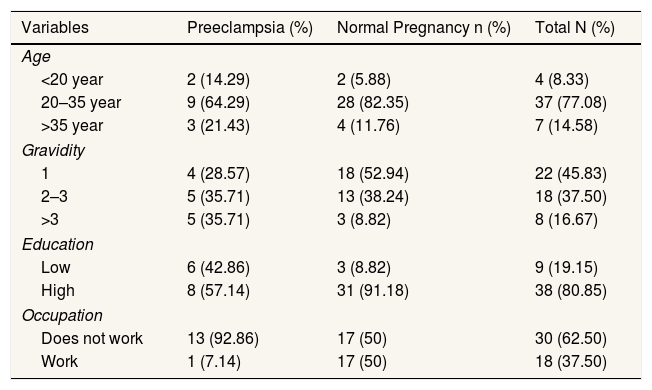
Characteristics are characteristics inherent in the mother, including age, gravidity, education, occupation. Respondent characteristics can be displayed in Table 1.
Characteristics of respondents.
| Variables | Preeclampsia (%) | Normal Pregnancy n (%) | Total N (%) |
|---|---|---|---|
| Age | |||
| <20 year | 2 (14.29) | 2 (5.88) | 4 (8.33) |
| 20–35 year | 9 (64.29) | 28 (82.35) | 37 (77.08) |
| >35 year | 3 (21.43) | 4 (11.76) | 7 (14.58) |
| Gravidity | |||
| 1 | 4 (28.57) | 18 (52.94) | 22 (45.83) |
| 2–3 | 5 (35.71) | 13 (38.24) | 18 (37.50) |
| >3 | 5 (35.71) | 3 (8.82) | 8 (16.67) |
| Education | |||
| Low | 6 (42.86) | 3 (8.82) | 9 (19.15) |
| High | 8 (57.14) | 31 (91.18) | 38 (80.85) |
| Occupation | |||
| Does not work | 13 (92.86) | 17 (50) | 30 (62.50) |
| Work | 1 (7.14) | 17 (50) | 18 (37.50) |
Based on Table 1, the highest number of pregnant women who experienced preeclampsia was 20–35 years. However, from gravidity and education, the distribution of preeclampsia was almost the same in all age and education groups. For occupational characteristics, pregnant women with preeclampsia were mostly in a group of mothers who did not work.
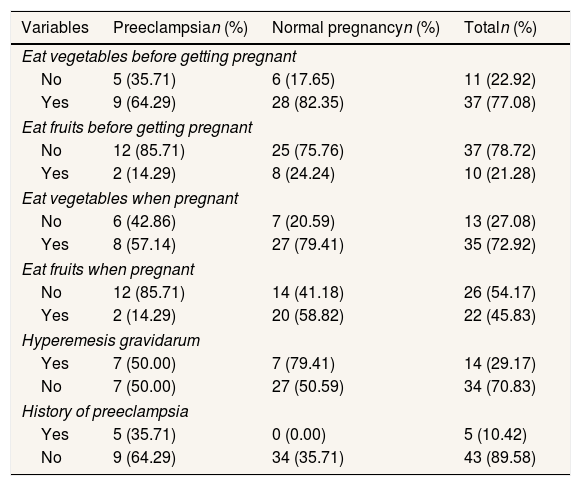
Based on Table 2, it can be seen that 35.71% of preeclamptic mothers did not eat vegetables every day before becoming pregnant, and 85.71% did not eat fruit every day before becoming pregnant. In normal pregnant women, there were also 75.76% who did not eat fruit every day before becoming pregnant. The percentage of women with preeclampsia eating vegetables decreased during pregnancy, whereas in the normal pregnant group, there was an increase in fruit consumption every day compared to before pregnancy. 50% of pregnant women who experienced hyperemesis gravidarum in the 1st trimester had preeclampsia. Furthermore, 35% of women with preeclampsia currently had a history of preeclampsia in a previous pregnancy.
Distribution of fruit and vegetable consumption habits, history of hyperemesis gravidarum, and preeclampsia.
| Variables | Preeclampsian (%) | Normal pregnancyn (%) | Totaln (%) |
|---|---|---|---|
| Eat vegetables before getting pregnant | |||
| No | 5 (35.71) | 6 (17.65) | 11 (22.92) |
| Yes | 9 (64.29) | 28 (82.35) | 37 (77.08) |
| Eat fruits before getting pregnant | |||
| No | 12 (85.71) | 25 (75.76) | 37 (78.72) |
| Yes | 2 (14.29) | 8 (24.24) | 10 (21.28) |
| Eat vegetables when pregnant | |||
| No | 6 (42.86) | 7 (20.59) | 13 (27.08) |
| Yes | 8 (57.14) | 27 (79.41) | 35 (72.92) |
| Eat fruits when pregnant | |||
| No | 12 (85.71) | 14 (41.18) | 26 (54.17) |
| Yes | 2 (14.29) | 20 (58.82) | 22 (45.83) |
| Hyperemesis gravidarum | |||
| Yes | 7 (50.00) | 7 (79.41) | 14 (29.17) |
| No | 7 (50.00) | 27 (50.59) | 34 (70.83) |
| History of preeclampsia | |||
| Yes | 5 (35.71) | 0 (0.00) | 5 (10.42) |
| No | 9 (64.29) | 34 (35.71) | 43 (89.58) |
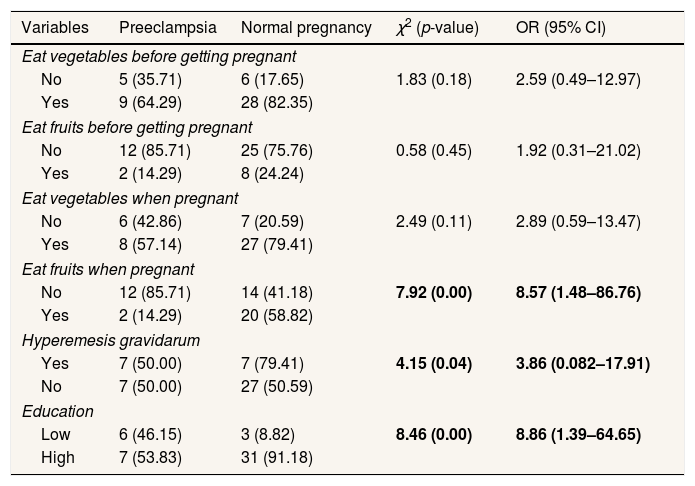
The bivariable analysis aimed to see the relationship between the independent and the dependent variables using the chi-square test and then measured how much risk the independent variable can pose to the dependent variable calculated using the OR test with 95% CI. The results of the analysis were shown in Table 3.
Relationship between fruits and vegetables consumption habits, history of hyperemesis gravidarum, history of preeclampsia, and preeclampsia with preeclampsia incidence.
| Variables | Preeclampsia | Normal pregnancy | χ2 (p-value) | OR (95% CI) |
|---|---|---|---|---|
| Eat vegetables before getting pregnant | ||||
| No | 5 (35.71) | 6 (17.65) | 1.83 (0.18) | 2.59 (0.49–12.97) |
| Yes | 9 (64.29) | 28 (82.35) | ||
| Eat fruits before getting pregnant | ||||
| No | 12 (85.71) | 25 (75.76) | 0.58 (0.45) | 1.92 (0.31–21.02) |
| Yes | 2 (14.29) | 8 (24.24) | ||
| Eat vegetables when pregnant | ||||
| No | 6 (42.86) | 7 (20.59) | 2.49 (0.11) | 2.89 (0.59–13.47) |
| Yes | 8 (57.14) | 27 (79.41) | ||
| Eat fruits when pregnant | ||||
| No | 12 (85.71) | 14 (41.18) | 7.92 (0.00) | 8.57 (1.48–86.76) |
| Yes | 2 (14.29) | 20 (58.82) | ||
| Hyperemesis gravidarum | ||||
| Yes | 7 (50.00) | 7 (79.41) | 4.15 (0.04) | 3.86 (0.082–17.91) |
| No | 7 (50.00) | 27 (50.59) | ||
| Education | ||||
| Low | 6 (46.15) | 3 (8.82) | 8.46 (0.00) | 8.86 (1.39–64.65) |
| High | 7 (53.83) | 31 (91.18) | ||
The analysis results using the chi-square test showed that the habit of eating vegetables and fruit before pregnancy did not have a significant relationship, but the OR value showed a value of more than 1. The analysis results between the variable eating habits of fruit regularly before pregnancy were also not related to preeclampsia. However, the OR value was also more than 1. The OR value greater than 1 indicated that practically irregular eating habits of vegetables and fruits before pregnancy would increase the risk of preeclampsia.
Likewise, with the condition during pregnancy, women who did not regularly eat vegetables during pregnancy were not statistically associated with preeclampsia. However, the OR value=2.89 showed that practically mothers who did not consume vegetables regularly during pregnancy could increase the risk of experiencing preeclampsia by 2.9 times. Furthermore, based on the chi-square test value, the variable of irregular fruit consumption every day during pregnancy was associated with the incidence of preeclampsia. The OR result of 8.57 also showed that pregnant women who did not regularly consume fruit during pregnancy increased their risk of experiencing preeclampsia by 8.57 times.
Based on the chi-square test, it was found that pregnant women who experienced hyperemesis gravidarum were significantly associated with the incidence of preeclampsia and increased their risk of experiencing preeclampsia with an OR value of 3.86. For the education variable, the analysis results showed a statistically significant relationship with the incidence of preeclampsia. Based on the OR value obtained, mothers who had low education increase their risk of experiencing preeclampsia by 8.9 times.
DiscussionThe results of this study indicated that eating fruits during pregnancy was associated with the incidence of preeclampsia. There were several previous research results related to fruit consumption that support the results of this study. Research by Brantsaeter et al. (2009) found that the characteristics of a diet high in vegetables, fruits, rice, and vegetable oil were associated with a reduced risk of preeclampsia, while the characteristics of a diet with a high intake of processed foods such as hamburgers, white bread, salty snacks, and sugary drinks increase the risk of preeclampsia.18
Based on the results of this study, it was also found that the incidence of hyperemesis gravidarum was significantly associated with the incidence of preeclampsia, and it increased the risk of pregnant women experiencing preeclampsia by 3.86 times. These results were in line with previous research that pregnant women with hyperemesis gravidarum in the 1st trimester would have an increased risk of developing preeclampsia. If it occurred in the 2nd trimester of pregnancy, pregnant women had two times the risk of giving birth to preterm babies with preeclampsia and had three times the risk of placental abruption, so it can be concluded that hyperemesis gravidarum is closely related to placental dysfunction/disorders.16
Without realizing it, pregnant women may experience relative trace element deficiency. This is associated with nausea and vomiting that occurs in early pregnancy, especially in conditions of hyperemesis gravidarum. Usually, pregnant women at times of nausea and vomiting tend to be picky about types of food and usually only eat dry foods to avoid nausea and vomiting. This condition is very likely to cause pregnant women to experience nutritional deficiencies in the form of minerals and vitamins that impact the mother and the fetus. Trace element deficiency during pregnancy is closely related to morbidity and mortality in newborns.8 Sources of trace elements come from fruits and vegetables, which should be consumed regularly to meet the body's needs. The contribution of macronutrients to pregnancy success has recently begun to be researched and focused on the role of certain important micronutrients because certain micronutrients are an absolute requirement and are only needed in small amounts every day.15 Based on the description, according to the authors, nutritional factors are one of the important things that can affect the success of a pregnancy process, prevent pregnancy complications and fetal disorders, so nutrition is a modifiable factor during pregnancy to prevent preeclampsia compared to other risk factors.
Some of the micronutrients needed by the body are useful for producing antioxidants because our body's ability is very limited to produce antioxidants (glutathione), so it needs intake from outside. This intake comes from fruits and vegetables, such as oranges, strawberries, apples, grapes, and other fruits around us. The antioxidant content of vegetables and fruit varies greatly, so we should consume a wide variety of vegetables and fruits. In preeclampsia, endothelial dysfunction occurs, which causes an increase in stress oxidation reactions which will increase levels of oxidants (free radicals). This condition will cause various complications. Therefore the intake of vegetables and fruit in sufficient portions is needed by a pregnant woman. Lack of certain antioxidant activity associated with micronutrients such as selenium, copper, zinc, and manganese can result in poor pregnancy outcomes, including fetal growth restriction,9 preeclampsia,10 and associated increased risk of disease in adulthood, including heart disease and type 2 diabetes.11–14
There have been several mechanisms of biological factors from the nutritional intake on the risk of preeclampsia. In the nonpregnant female population, the characteristics of the dietary intake pattern with high consumption of fruits and vegetables, and low consumption of manufactured foods, foods containing sugar and fat, showed the ability to reduce markers of metabolic syndrome, inflammation, and heart disease.19 The consumption pattern of eating vegetables also showed benefits in preventing chronic disease.20 The results of other studies also showed that preeclampsia could predispose the fetus to experience an increased risk of developing cardiovascular disease in adulthood.17 This causes the detection of preeclampsia can help early management to reduce morbidity and mortality in mothers and babies and become the basis for making prevention efforts so that cardiovascular disease does not occur in the future.
This study indicated that from the aspect of education, statistically and practically, low education increased the risk of experiencing preeclampsia by 8.9 times. The results of this study were in line with the research, which found that low education had a 2.3 times higher risk of preeclampsia (OR=2.3; 95% CI: 1.11–4.92) compared to higher education.21 This is, of course, related to how a mother's education can support her knowledge of matters related to pregnancy information. Mothers who have higher education will undoubtedly try to find important information about the changes and complications of pregnancy so that by knowing these things, there will be efforts to take precautions. This can be realized through the behavior of regular pregnancy checks at health facilities and the behavior of consuming nutritious food during pregnancy to support the health of the mother and the fetus. According to the author, the results of this study were also in line with the community movement program launched by the government so that people cultivate a culture of eating vegetables and fruits, which can reduce the incidence of preeclampsia. Mothers must also be continuously educated to prepare themselves from the start of pregnancy by consuming natural foods derived from vegetables and fruits and reducing the habit of consuming fast food that does not contain vitamins and minerals. Pregnant women need to check at least four times during pregnancy to monitor the condition of the mother and fetus and find out as early as possible any pregnancy complications.
ConclusionThe results showed that the habit of eating irregular fruits during pregnancy was significantly associated with the incidence of preeclampsia, with an OR value of 8.57. Mothers who had hyperemesis gravidarum increased their risk 3.86 times for developing preeclampsia. Nutritional intervention is needed through nutrition education for pre-pregnant women so that their nutritional adequacy during pregnancy can be fulfilled, especially during the 1st trimester, namely the implantation phase and socialization of the community movement program for healthy living, especially the consumption of vegetables and fruits for women of childbearing age, women during pre-pregnancy, pregnant and breastfeeding. It is necessary to carry out further research by conducting trials of fruits and vegetable extracts administration in preeclamptic patients.
Conflicts of interestThe authors declare no conflict of interest.
We thank all pregnant women who participated in the study. We also thank the Polytechnic of Health Ministry of Health, Kendari, Indonesia, which had provided funding for conducting this study.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











