



To identify the factors associated with bullying behaviors among adolescents by analyzing victims, aggressors and victims/aggressors separately.
MethodsA cross-sectional study was performed in a representative sample of 3,089 secondary school students (13-18 years old) in Barcelona (Spain). To define bullying behaviors, we used three questions about different types of mistreatment (jeering, attacking, marginalizing).
ResultsCompared with secondary school students not involved in bullying, victims, aggressors and victims/aggressors were more likely to be boys and to report negative mood states. Victims were younger, were more overweight or obese and were lighter cannabis users, while aggressors were also younger but reported more antisocial behaviors and more cannabis and alcohol use. Victims/aggressors reported more antisocial behaviors and were overweight.
ConclusionsBeing involved in bullying, independently of the role adopted, was associated with health-related problems, which can lead to psychological disorders in adulthood.
Identificar los factores asociados al acoso escolar entre adolescentes escolarizados, analizando víctimas, agresores y víctimas/agresores por separado.
MétodosEstudio transversal en una muestra representativa de 3089 estudiantes de escuelas de secundaria (13-18 años) de Barcelona. Los roles de acoso escolar se definieron a partir de tres ítems sobre diferentes tipos de maltrato (insultos, agresión física y marginación social).
ResultadosLos escolares involucrados en acoso escolar tenían mayor probabilidad de ser chicos y presentar un estado de ánimo negativo con respecto a los no involucrados. Además, las víctimas eran más jóvenes, presentaban más sobrepeso u obesidad, y consumían menos cannabis, mientras que los agresores también eran más jóvenes pero declaraban realizar conductas antisociales en mayor medida, y un mayor consumo de cannabis y alcohol. Las víctimas/agresores realizaban más conductas antisociales y presentaban sobrepeso.
ConclusionesEstar involucrado en acoso escolar, con independencia del rol, se asoció a problemas relacionados con la salud, que podrían llegar a derivar en trastornos psicológicos en la edad adulta.
Bullying has been defined as an aggressive behaviour in which one or more persons intentionally try to harm another person over time, in a situation defined by a power imbalance.1 Being involved in bullying independently of the role adopted can have negative consequences such as social, emotional or psychological problems.2,3 Being a victim may be a precursor of depression and anxiety,4 and suicidal ideation.2 Aggressors have been associated with antisocial behaviours and psychiatric disorders in adulthood.2 Overall, bullying is currently a prevalent problem among children and adolescents of all ages worldwide,5 especially within the school environment.3 Consequently, bullying has become a concern for parents, teachers and health professionals.
Previous studies have identified different factors associated with being involved in bullying considering the role adopted, including having a deprived socio-economic position,6 sex (being a boy), and age (bullying decreases with age).3 Moreover, victims have been associated with poor peer relationships, psychosomatic complaints and low self-esteem5 while aggressors have been related to substance use,7 truancy and emotional and psychological problems.3 Victims/aggressors have been related to psychosomatic complaints1 and psychological problems,8 even it has been suggested that they are at the highest risk of behavioural and psychological problems.8
Most studies performed have investigated the role of specific factors, while studies that have considered the whole range of possible determinants are scarce. For this reason, the aim of this study was to analyse a wide range of potential determinants together in order to identify factors associated (including negative mood states and antisocial behaviours) with bullying behaviours among adolescents, analysing different roles separately.
MethodsA cross-sectional study was conducted among a representative sample of secondary school students aged 13-18 years old (8th, 10th and 12th grade) in Barcelona (Spain). Data came from the 2008 edition of the FRESC-survey (health and lifestyle risk factors survey) which is performed periodically by the Agència de Salut Pública de Barcelona. Its design took into consideration questions from previous editions and other validated national and international surveys. Classrooms were the sample unit and were randomly selected, stratifying by type of school (public or subsidized/private) and the socio-economic status (SES) of the school's neighbourhood (low, medium or high). Overall, 136 classrooms from 80 secondary schools were included in this study.9
We defined three dependent variables according to the bullying behaviour. As in previous studies,10 being a victim (“victim”) was defined as being laughed at, attacked or marginalized ≥4 times in the last year or reporting at least one episode in each category. Students who reported having taken part in laughing at, attacking or marginalizing others ≥4 times in the last year or reporting at least one episode of each behaviour were classified as “aggressors”. Those students who were classified either as victims or as aggressors were considered as “victims/aggressors”.
The socio-demographic variables included were age, grade, sex and students’ SES (Family Affluence Scale -FAS-). We also studied mood states, antisocial behaviours, substance use and body mass index (BMI), which was calculated from objective measures.9
Bivariate and multivariate robust Poisson regressions were performed to identify the factors associated with victims, aggressors and victims/aggressors. Non-involved students were the reference group.
ResultsThe mean age of the 3,089 students sampled was 15.8 years, 52% were girls and about 80% attended schools with a medium or high SES (data not shown).9
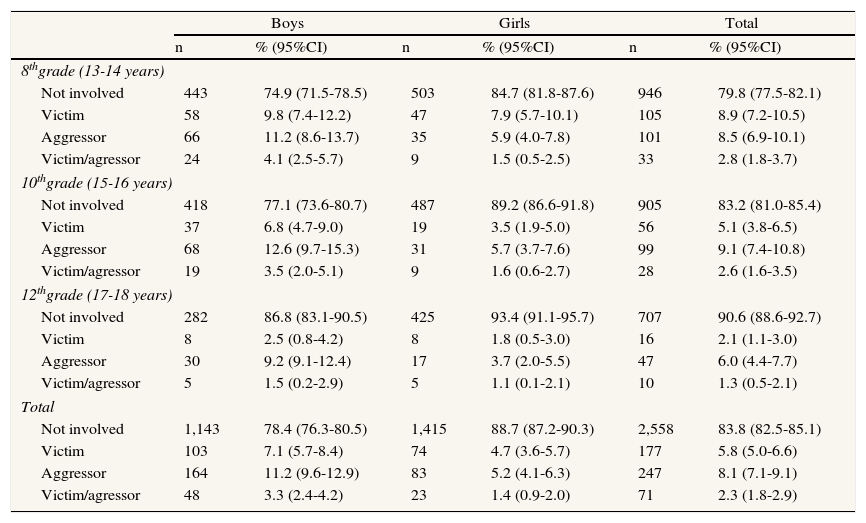
Regarding involvement in bullying, 7.1% of boys reported being a victim, 11.2% reported being an aggressor and 3.3% was classified as victim/aggressor. Among girls these percentages were 4.7%, 5.2% and 1.7% respectively (Table 1).
Prevalence of bullying behaviours (not involved, victim, aggressor and victim/aggressor) among schoolchildren by sex and grade. FRESC report, 2008, Barcelona (Spain).
| Boys | Girls | Total | ||||
| n | % (95%CI) | n | % (95%CI) | n | % (95%CI) | |
| 8thgrade (13-14 years) | ||||||
| Not involved | 443 | 74.9 (71.5-78.5) | 503 | 84.7 (81.8-87.6) | 946 | 79.8 (77.5-82.1) |
| Victim | 58 | 9.8 (7.4-12.2) | 47 | 7.9 (5.7-10.1) | 105 | 8.9 (7.2-10.5) |
| Aggressor | 66 | 11.2 (8.6-13.7) | 35 | 5.9 (4.0-7.8) | 101 | 8.5 (6.9-10.1) |
| Victim/agressor | 24 | 4.1 (2.5-5.7) | 9 | 1.5 (0.5-2.5) | 33 | 2.8 (1.8-3.7) |
| 10thgrade (15-16 years) | ||||||
| Not involved | 418 | 77.1 (73.6-80.7) | 487 | 89.2 (86.6-91.8) | 905 | 83.2 (81.0-85.4) |
| Victim | 37 | 6.8 (4.7-9.0) | 19 | 3.5 (1.9-5.0) | 56 | 5.1 (3.8-6.5) |
| Aggressor | 68 | 12.6 (9.7-15.3) | 31 | 5.7 (3.7-7.6) | 99 | 9.1 (7.4-10.8) |
| Victim/agressor | 19 | 3.5 (2.0-5.1) | 9 | 1.6 (0.6-2.7) | 28 | 2.6 (1.6-3.5) |
| 12thgrade (17-18 years) | ||||||
| Not involved | 282 | 86.8 (83.1-90.5) | 425 | 93.4 (91.1-95.7) | 707 | 90.6 (88.6-92.7) |
| Victim | 8 | 2.5 (0.8-4.2) | 8 | 1.8 (0.5-3.0) | 16 | 2.1 (1.1-3.0) |
| Aggressor | 30 | 9.2 (9.1-12.4) | 17 | 3.7 (2.0-5.5) | 47 | 6.0 (4.4-7.7) |
| Victim/agressor | 5 | 1.5 (0.2-2.9) | 5 | 1.1 (0.1-2.1) | 10 | 1.3 (0.5-2.1) |
| Total | ||||||
| Not involved | 1,143 | 78.4 (76.3-80.5) | 1,415 | 88.7 (87.2-90.3) | 2,558 | 83.8 (82.5-85.1) |
| Victim | 103 | 7.1 (5.7-8.4) | 74 | 4.7 (3.6-5.7) | 177 | 5.8 (5.0-6.6) |
| Aggressor | 164 | 11.2 (9.6-12.9) | 83 | 5.2 (4.1-6.3) | 247 | 8.1 (7.1-9.1) |
| Victim/agressor | 48 | 3.3 (2.4-4.2) | 23 | 1.4 (0.9-2.0) | 71 | 2.3 (1.8-2.9) |
95%CI: 95% confidence interval.
FRESC: Factores de Riesgo en ESColares (Risk factors in schoolchildren).
Missing values < 2%.
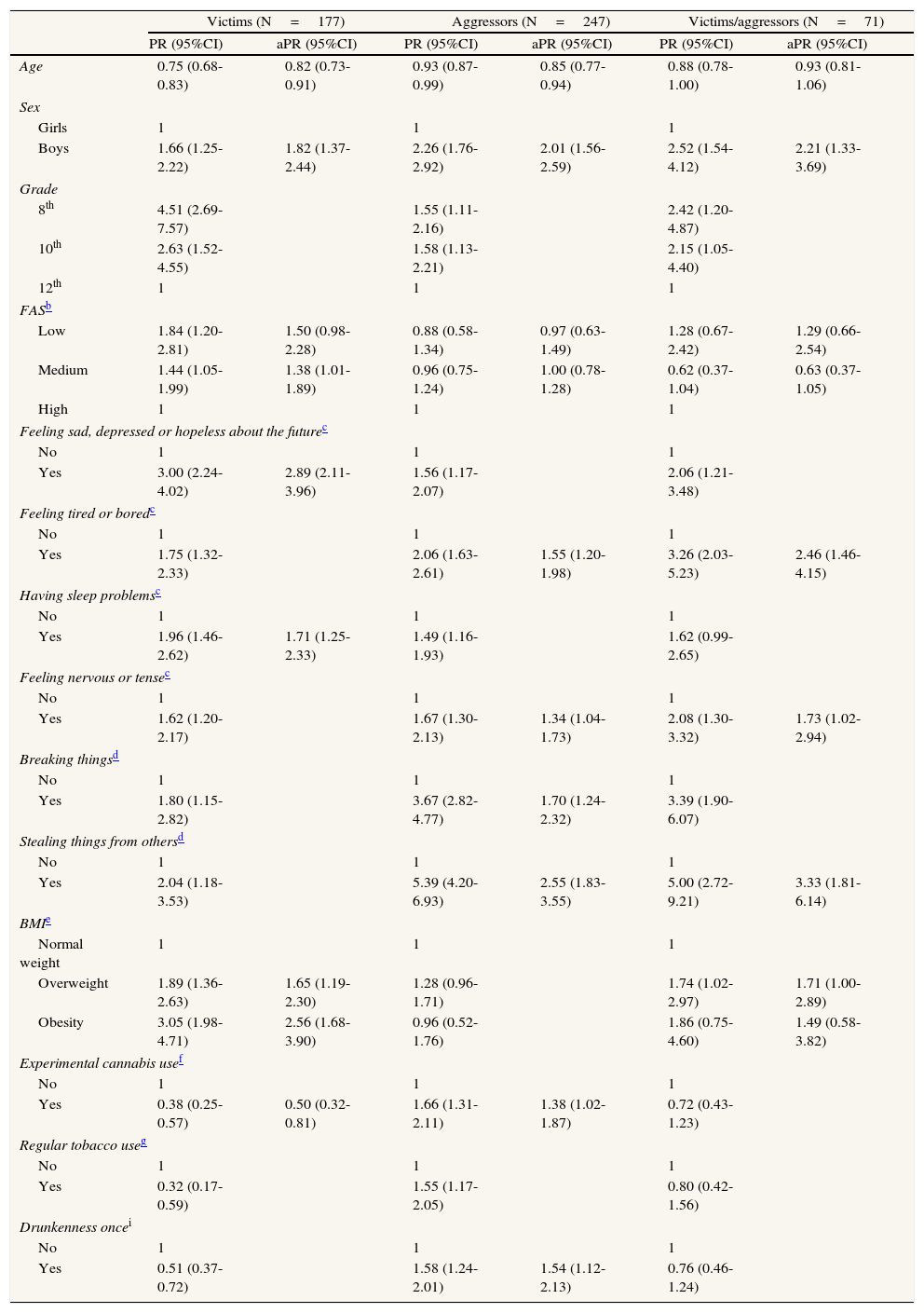
Victims and aggressors were more likely to be boys of younger age. Victims were also associated with overweight or obesity, never having consumed cannabis, feeling sad, depressed or hopeless about the future and having frequent sleep problems compared with non-involved students. Aggressors were also associated with breaking and stealing things, having ever consumed cannabis, having been drunk and feeling frequently tired or bored and nervous or tense. Victims/aggressors were more likely to be boys, feel frequently tired or bored and nervous or tense, steal things and be overweight (Table 2).
Factors associated with bullying behaviours (victim, aggressor or victim/aggressor).a FRESC report, 2008, Barcelona (Spain).
| Victims (N=177) | Aggressors (N=247) | Victims/aggressors (N=71) | ||||
| PR (95%CI) | aPR (95%CI) | PR (95%CI) | aPR (95%CI) | PR (95%CI) | aPR (95%CI) | |
| Age | 0.75 (0.68-0.83) | 0.82 (0.73-0.91) | 0.93 (0.87-0.99) | 0.85 (0.77-0.94) | 0.88 (0.78-1.00) | 0.93 (0.81-1.06) |
| Sex | ||||||
| Girls | 1 | 1 | 1 | |||
| Boys | 1.66 (1.25-2.22) | 1.82 (1.37-2.44) | 2.26 (1.76-2.92) | 2.01 (1.56-2.59) | 2.52 (1.54-4.12) | 2.21 (1.33-3.69) |
| Grade | ||||||
| 8th | 4.51 (2.69-7.57) | 1.55 (1.11-2.16) | 2.42 (1.20-4.87) | |||
| 10th | 2.63 (1.52-4.55) | 1.58 (1.13-2.21) | 2.15 (1.05-4.40) | |||
| 12th | 1 | 1 | 1 | |||
| FASb | ||||||
| Low | 1.84 (1.20-2.81) | 1.50 (0.98-2.28) | 0.88 (0.58-1.34) | 0.97 (0.63-1.49) | 1.28 (0.67-2.42) | 1.29 (0.66-2.54) |
| Medium | 1.44 (1.05-1.99) | 1.38 (1.01-1.89) | 0.96 (0.75-1.24) | 1.00 (0.78-1.28) | 0.62 (0.37-1.04) | 0.63 (0.37-1.05) |
| High | 1 | 1 | 1 | |||
| Feeling sad, depressed or hopeless about the futurec | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 3.00 (2.24-4.02) | 2.89 (2.11-3.96) | 1.56 (1.17-2.07) | 2.06 (1.21-3.48) | ||
| Feeling tired or boredc | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 1.75 (1.32-2.33) | 2.06 (1.63-2.61) | 1.55 (1.20-1.98) | 3.26 (2.03-5.23) | 2.46 (1.46-4.15) | |
| Having sleep problemsc | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 1.96 (1.46-2.62) | 1.71 (1.25-2.33) | 1.49 (1.16-1.93) | 1.62 (0.99-2.65) | ||
| Feeling nervous or tensec | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 1.62 (1.20-2.17) | 1.67 (1.30-2.13) | 1.34 (1.04-1.73) | 2.08 (1.30-3.32) | 1.73 (1.02-2.94) | |
| Breaking thingsd | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 1.80 (1.15-2.82) | 3.67 (2.82-4.77) | 1.70 (1.24-2.32) | 3.39 (1.90-6.07) | ||
| Stealing things from othersd | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 2.04 (1.18-3.53) | 5.39 (4.20-6.93) | 2.55 (1.83-3.55) | 5.00 (2.72-9.21) | 3.33 (1.81-6.14) | |
| BMIe | ||||||
| Normal weight | 1 | 1 | 1 | |||
| Overweight | 1.89 (1.36-2.63) | 1.65 (1.19-2.30) | 1.28 (0.96-1.71) | 1.74 (1.02-2.97) | 1.71 (1.00-2.89) | |
| Obesity | 3.05 (1.98-4.71) | 2.56 (1.68-3.90) | 0.96 (0.52-1.76) | 1.86 (0.75-4.60) | 1.49 (0.58-3.82) | |
| Experimental cannabis usef | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 0.38 (0.25-0.57) | 0.50 (0.32-0.81) | 1.66 (1.31-2.11) | 1.38 (1.02-1.87) | 0.72 (0.43-1.23) | |
| Regular tobacco useg | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 0.32 (0.17-0.59) | 1.55 (1.17-2.05) | 0.80 (0.42-1.56) | |||
| Drunkenness oncei | ||||||
| No | 1 | 1 | 1 | |||
| Yes | 0.51 (0.37-0.72) | 1.58 (1.24-2.01) | 1.54 (1.12-2.13) | 0.76 (0.46-1.24) | ||
PR: Prevalence Ratio; aPR: adjusted PR.
95%CI: 95% confidence interval; FRESC: Factores de Riesgo en ESColares (Risk factors in schoolchildren); BMI: Body mass index.
Our results showed that victims, aggressors and victims/aggressors were more likely to be boys, and to report negative mood states. Aggressors were also more likely to consume addictive substances and to report antisocial behaviours. Victims were more likely to be overweight or obese. Victims/aggressors were also more likely to engage antisocial behaviours and be overweight.
One potential limitation of this study is that data were collected from self-reported questionnaires. Therefore, social desirability may have influenced the responses, suggesting a possible information bias. However, anonymous questionnaires for self-reported behaviours have previously been proven to have good validity and reliability.11 Another limitation is the lack of an agreed-upon scale for measuring bullying roles which hampers comparing our outcomes with those of other studies. Finally, data are cross-sectional, so it is not possible to establish causality. Despite these limitations, it should be mentioned that the sample was representative of the secondary school students in a large city in Spain.
VictimsSome studies have shown an association between victims and different risk factors such as overweight and obesity,12 psychosomatic complaints, sleeping problems, negative mood states and low self-esteem.2,5 Findings reported by the Global School-based Student Health Survey (GSHS) suggested that victims felt sad or hopeless more frequently.13 Additionally, some longitudinal studies have reported that being a victim could lead to emotional, behavioural or psychosocial problems.4,14 Similarly, our results showed that victims were more likely to feel sad, depressed and hopeless about the future and to have sleeping problems. Moreover, we also found that overweight and obese adolescents were at higher risk of being a victim than those of normal weight. Negative social stereotypes about overweight may play an important role in making overweight and obese adolescents a target of teasing or social marginalization. For substance use, we found a negative association between victims and cannabis use, while previous studies have reported discrepant results.7,15 These results could reflect a general pattern among victims defined by having low self-esteem, being physically different, accepting social rules and avoiding some risk behaviours such as substance consumption.
AggressorsOur results showed that aggressors were associated with antisocial behaviour and with frequently feeling tired, bored, nervous or tense. This is consistent with previous literature suggesting that aggressors display more negative and antisocial behaviour2 but also have psychological problems such as depression, anxiety or psychosomatic symptoms.2,4 Regarding substance use, our results are also consistent with other findings that identified a positive association between aggressors and cannabis and alcohol consumption.7 In addition, a longitudinal study16 suggested that being an aggressor was a significant predictor of smoking initiation in adolescents. These associations could be because aggressors are generally more self-confident and uncontrolled than other students and may tend not to abide by social rules.
Victims/aggressorsVictims/aggressors engaged more frequently in antisocial behaviours and feeling frequently tired, bored, nervous or tense. Thus, we mostly observed that they were very similar to aggressors, but the associations found were even stronger in victims/aggressors than in aggressors. These results support the hypothesis suggested by previous studies that victims/aggressors are similar to aggressors but that they are at higher risk than other bullying behaviours of having behavioural and psychological problems.8 Otherwise, our results showed that victims/aggressors were more likely to be overweight than non-involved students as occurred among victims. It could be that some overweight adolescents were physically stronger than other students taking this as an advantage for bullying them. Previous literature also showed that victims/aggressors have some psychological similarities with both aggressors and victims2, but we did not find similarities with victims regarding negative mood states.
ConclusionsAlthough our results show some differences in behavioural and mood state patterns between different roles, bullying behaviours were associated with health-related problems that can lead to psychological disorders in adulthood. Therefore, bullying may have negative consequences on adolescents’ health for victims, aggressors and victims/aggressors. Several schools report antisocial and violent behaviours of students yearly. Specific school-based programs for bullying prevention which include training of students in social and emotional skills in order to create a positive and safe school climate could help to reduce bullying. The results of this study show different behaviours and health-related factors that characterize victims, aggressors and victims/aggressors which should be considered when developing and implementing bullying prevention programs.
The substantial prevalence of bullying among schoolchildren and its consequences have become a great public health concern. Most of the existing studies related to bullying are centred in victimization and some identified factors associated are being a boy, being young and an overprotective family environment. Studies considering aggressors are scarce in our context and it is necessary to go in depth in this area to deal with bullying.
What does this study contribute to the literature?This study includes profiles involved in bullying behaviours. It shows differences and similarities in mood states patterns, overweight and obesity, antisocial behaviours and addictive substance use between victims, aggressors and victims/aggressors. These results provide essential information to understand the problem and should be considered when developing and implementing bullying prevention programs.
X. Garcia-Continente participated in data analysis and interpretation and drafted the manuscript. M. Nebot and A. Pérez were involved in the study design and the coordination of the survey and helped to interpret data and write the manuscript. A. Espelt participated in data interpretation and writing of the manuscript. All authors approved the final version of the manuscript.
FundingThis work was supported by the Agència de Gestió d’Ajuts Universitaris i de Recerca de la Generalitat de Catalunya (AGAUR SGR 2009-1345).
Conflict of interestNone.
The authors would like to thank the teachers and students of the participating schools. We would also like to thank the personnel of the Community Health Service and of the Evaluation and Intervention Methods Service of the Agència de Salut Pública de Barcelona who collaborated in the administration of the questionnaires, height and weight measurements, and in the creation of the data set. This paper represents partial fulfilment of the requirements for the PhD program of X. Garcia-Continente at the Pompeu Fabra University (Barcelona, Spain).
Dr. Manel Nebot died in October 18, 2012. This work would not have been possible without his convincement, perseverance and dedication.











