




In Spain environmental surveillance has mainly relied on measures of selected pollutants in air, water, food and soil. A study was conducted in Madrid to assess the feasibility of implementing a surveillance system of exposure among the general population to specific environmental pollutants, using biomarkers. The project was basically focused on the environment surrounding newborns. Hence, the study population was made up of 145 triplets of pregnant women at around 8 months’ gestation, their partners, and newborns from two areas, representing the two main types of urban environments in the region, i.e., the City of Madrid and its outlying metropolitan belt. Multiple biologic substrates were collected from each participant in order to assess the most suitable samples for an environmental surveillance system. The selected contaminants represent the main agents to which a population like that of Madrid is exposed every day, including certain heavy metals, persistent organic pollutants and polycyclic aromatic hydrocarbons, as well as micronuclei in peripheral blood, a commonly used unspecific index of cytogenetic damage. In addition, passive air samplers were placed around subjects’ place of residence. This paper reports in detail on the design and response rates, summarizes field work results, and discusses some lessons learned.
En España, la vigilancia medioambiental se basa principalmente en medidas de ciertos contaminantes en muestras de aire, agua, alimentos y suelos. En Madrid se ha realizado un estudio para valorar la posibilidad de poner en marcha un sistema de vigilancia de exposiciones a contaminantes ambientales en la población general utilizando biomarcadores. El proyecto ha tenido como eje el estudio del entorno de los recién nacidos. Por tanto, la población de estudio la constituyen 145 «tríos» formados por mujeres en su octavo mes de embarazo, sus parejas y los recién nacidos de dos áreas geográficas, que representan los dos principales entornos urbanos de la región, es decir, Madrid capital y su area metropolitana. Se recogieron múltiples sustratos biológicos de cada participante con el objeto de valorar las muestras más adecuadas para un sistema de vigilancia de exposiciones ambientales. Los contaminantes elegidos representan los principales agentes tóxicos a los que una población como la de Madrid está expuesta diariamente, e incluyen metales pesados, contaminantes orgánicos persistentes e hidrocarburos aromáticos policíclicos; se ha añadido también una medida inespecífica de daño citogenético, los micronúcleos en sangre periférica. Además, se han colocado muestreadores pasivos de aire en los alrededores del domicilio de los participantes. Este artículo describe en detalle el diseño del estudio y la tasa de respuesta, resume los resultados del trabajo de campo y comenta algunas enseñanzas prácticas de éste.
The last century witnessed an important shift in the pattern of diseases worldwide. While developed countries have managed to bring about a signi- ficant reduction in incidence and mortality associated with infectious agents, chronic disorders have be- come the leading cause of illness, though for some of them their causes are still largely unknown at present. Modern lifestyles and industrial development have im- proved the quality of life but have also exposed the general population to a variety of air-, water- and food-borne toxic substances. Within the complex causal frame pro- posed for chronic disorders, there is increasing evidence of environmental pollutants being involved in the occu- rrence of these diseases1–6.
Although ambient pollutant levels are generally low -and indeed much lower than those found in specific work environments- their health impact can nonethe- less be quite relevant from a public health perspective, since exposure may affect the whole population during long periods of life. The increasing importance of en- vironmental contaminants has led to a great number of studies targeted at improving current knowledge on pollutant exposure levels among humans and their health effects. Since the 1990s, some countries have imple- mented surveillance systems using biomarkers to me- asure exposure to different pollutants in the general population, with the National Health and Nutrition Examination Surveys (NHANES), conducted by the National Center for Health Statistics7 in the USA, and the German Environmental Survey (GerES)8 in Germany being considered paradigms of this type of studies.
Currently, human biomonitoring is becoming one of the main priorities of the European Union. The deve- lopment of a coherent approach to biomonitoring in Eu- rope is specifically included within the actions of the European Environment and Health Action Plan for 2004109. Both European an American Health Authori- ties10,11 have stressed the importance of paying spe- cial attention to pollution levels in susceptible populations, and more specifically, in pregnant women and children. According to the US Agency for Toxic Substances and Disease Registry12, there are critical periods of structural and functional development during both pre- and post-natal life which make children more susceptible than adults to hazardous substances, though for most pollutants these periods are still unknown. Children may also differ from adults in their ca- pacity to repair damage from chemical insults and have a longer lifetime in which to express the deleterious con- sequences of such exposures.
In Spain, environmental surveillance has mainly re- lied on measures of selected pollutants in air, water, food and soil. In the last decade, however, several initiatives have been implemented with the aim of including human data in the framework of environmental research in different areas of the country13–18. One of the most recent examples of studies including biological measures is the Spanish Childhood and Environment (Infancia y Medio Ambiente [INMA]) study, a multicenter cohort project with 3100 pregnant women, designed to investigate the ef- fect of the most important pollutants during pregnancy and the first years of life19.
Purpose of the studyMadrid city and its metropolitan belt constitute the biggest urban area in Spain, with similar environmen- tal problems than other big western cities. Vallecas Health District presents some of the worst socioeconomic and health indicators within the region. In 2000 the Regional Government approved an important investment plan to promote the development of this District, which included specific Public Health objectives.
In this context, the Public Health Authority of the Madrid Autonomous Region, which had decided to promote biomarker-based assessment of exposure to specific en- vironmental pollutants in the general population, selected Vallecas Health District as one of the pilot study areas. The primary objective of this initiative was to design a surveillance system focused on newborns and their environment. Accordingly, a study was designed to study the feasibility of implementing a biomonitoring surveillance system in the region. The aims of that explora- tory research were to ascertain the population's exposure status using biomarkers; to test the selected participant enrolment strategy; to measure a wide range of pollutants, for the purpose of selecting a subgroup to be monitored in the proposed surveillance system; to obtain samples of several substrates, in order to choo- se those most suitable for use at a population level; and to obtain reference levels in the study areas. This paper reports the design, response rates and field work re- sults, and provides a description of the study population.
Study designThis is a descriptive study intended to enhance current knowledge of the pollution in the environment su- rrounding newborns. For that reason, it was decided that pregnant women at approximately 8 months' gestation and their partners would be included in the study population. In order to participate, subjects had to agree to answer an epidemiologic questionnaire and provide biologic specimens taken from themselves and the child, thereby constituting so-called «mother-father-newborn triplets».
Initially, this study was set out to recruit 100 complete mother-father-newborn triplets. To fulfill this ob- jective, however, the number of couples to be enrolled was increased by 50% (150), since there was a certain risk of losing mothers at delivery and, by extension, new- born participants.
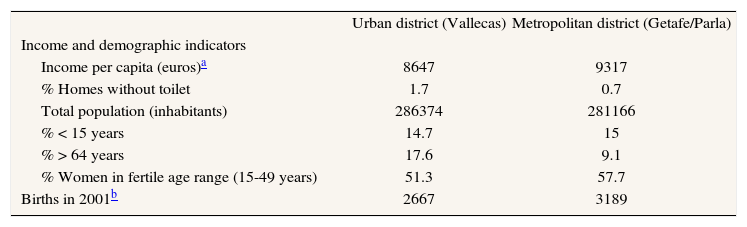
Furthermore, we decided to include the two main types of urban environment in which most of the regional population lived. To this end, half the sample was thus recruited from the Madrid City district of Vallecas and the other half was drawn from the Greater Madrid metropolitan belt (Parla and Getafe health districts). Some basic sociodemographic features of these two areas are shown in table 1. In this paper, most data are reported for the study sample overall.
Sociodemographic characteristics of the two study areas, according to the 2001 census
| Urban district (Vallecas) | Metropolitan district (Getafe/Parla) | |
| Income and demographic indicators | ||
| Income per capita (euros)a | 8647 | 9317 |
| % Homes without toilet | 1.7 | 0.7 |
| Total population (inhabitants) | 286374 | 281166 |
| % < 15 years | 14.7 | 15 |
| % > 64 years | 17.6 | 9.1 |
| % Women in fertile age range (15-49 years) | 51.3 | 57.7 |
| Births in 2001b | 2667 | 3189 |
| Men | Women | Men | Women | |
| Education | ||||
| Unfinished compulsory education in > 16 years (%) | 37.9 | 45.1 | 29.4 | 34.6 |
| University studies in > 30 years (%) | 8.6 | 8.2 | 8.6 | 8.3 |
| Occupation | ||||
| Unemployment % | 12.4 | 18.5 | 9.05 | 18.65 |
| Manual workers in > 16 years (%) | 65.9 | 51 | 68 | 50 |
| Immigration from low-income countries % Residents | 6.9 | 6.5 | 6.0 | 5.5 |
The research team presented the study to hospital managers, pediatricians, gynecologists, and midwives at public hospitals in the selected areas, as well as to the primary-care departments of local health authori- ties and primary-care midwives.
It was decided that women were to be invited to participate in the study by the primary-care midwives in char- ge of pregnancy classes. The main reasons for opting for such an approach were: a) the desire to ensure that the research project was incorporated within the insti- tutional health framework, so that the data-extraction schedule for this study could be coordinated with the standard follow-up of pregnant women, and b) the im- portance of having a person who was trusted by the women, involved in the enrollment process.
Training sessions were held at which midwives le- arned about the different steps of the designated field- work protocol and were provided with the basic material needed to fulfill the role that they were expected to play.
EnrollmentAll pregnant women in their eighth month of pregnancy, residing in the selected areas and attending child- birth preparation classes in the public health care system were invited to participate, until the designated sample size had been attained. Midwives outlined the study goals and requirements and provided informative brochures. All couples willing to participate and mee- ting the inclusion criteria were recruited. Both parents were required to give their prior written informed con- sent to participate. No financial rewards were offered, but the social utility of the study was explained.
No exclusions were made in terms of parents' or newborns' disease, race or place of origin. Inclusion criteria were: to have resided in one of the study areas for a minimum of one year; and not to have reported re- ceiving a blood transfusion during the previous year. For logistic reasons, we also required women to be aged over 15 years, had single pregnancies, and intended to deliver their babies at the local public hospital.
After a small pilot trial, recruitment started in Octo- ber 2003 and lasted until May 2004. In all, 630 women in 35 sessions of delivery-preparation courses were in- formed about the project and invited to participate. Of those eligible, 52% stated that they were willing to take part in the study and invite their partners to collabor- ate. Finally, 149 couples (29%) were enrolled (table 2). Two of these women gave birth before the first sche- duled date. Additionally, two couples and one father fail- ed to attend any appointment. All of them declined any subsequent call from the research group and withdrew from the study at an early stage.
BioMadrid study: women recruitment results
| Urban district | Metropolitan districts | Total | ||||
| N.o subjects | Participation (%) | N.o subjects | Participation (%) | N.o subjects | Participation (%) | |
| Meeting inclusion criteria | 273 | 100 | 242 | 100 | 515 | 100 |
| Initial agreement | 147 | 54 | 121 | 50 | 268 | 52 |
| Enrolled (with both parents’ agreement) | 74 | 27 | 75 | 31 | 149 | 29 |
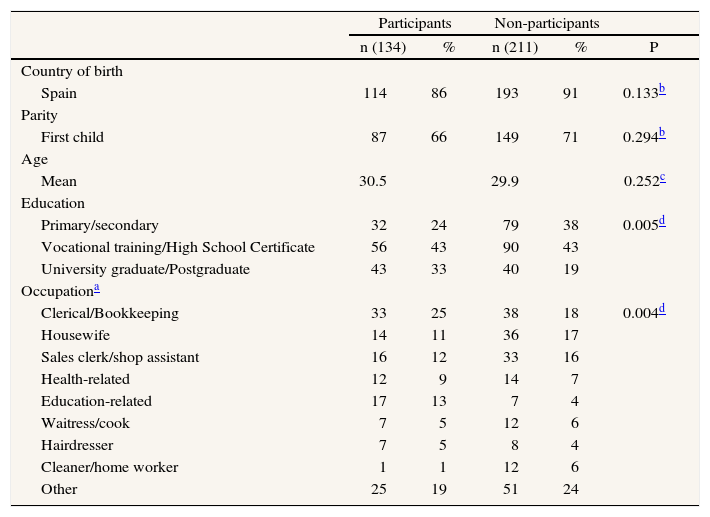
Approximately 70% of the pregnant women attending the labor classes completed a brief questionnaire, designed to collect basic sociodemographic data so as to enable the representativeness of the final sample to be evalua- ted. The characteristics of participants and non-participants who completed this form are shown in table 3.
Characteristics of participants and non-participants who answered the initial questionnaire, the BioMadrid study (November 2003-March 2004)
| Participants | Non-participants | ||||
| n (134) | % | n (211) | % | P | |
| Country of birth | |||||
| Spain | 114 | 86 | 193 | 91 | 0.133b |
| Parity | |||||
| First child | 87 | 66 | 149 | 71 | 0.294b |
| Age | |||||
| Mean | 30.5 | 29.9 | 0.252c | ||
| Education | |||||
| Primary/secondary | 32 | 24 | 79 | 38 | 0.005d |
| Vocational training/High School Certificate | 56 | 43 | 90 | 43 | |
| University graduate/Postgraduate | 43 | 33 | 40 | 19 | |
| Occupationa | |||||
| Clerical/Bookkeeping | 33 | 25 | 38 | 18 | 0.004d |
| Housewife | 14 | 11 | 36 | 17 | |
| Sales clerk/shop assistant | 16 | 12 | 33 | 16 | |
| Health-related | 12 | 9 | 14 | 7 | |
| Education-related | 17 | 13 | 7 | 4 | |
| Waitress/cook | 7 | 5 | 12 | 6 | |
| Hairdresser | 7 | 5 | 8 | 4 | |
| Cleaner/home worker | 1 | 1 | 12 | 6 | |
| Other | 25 | 19 | 51 | 24 | |
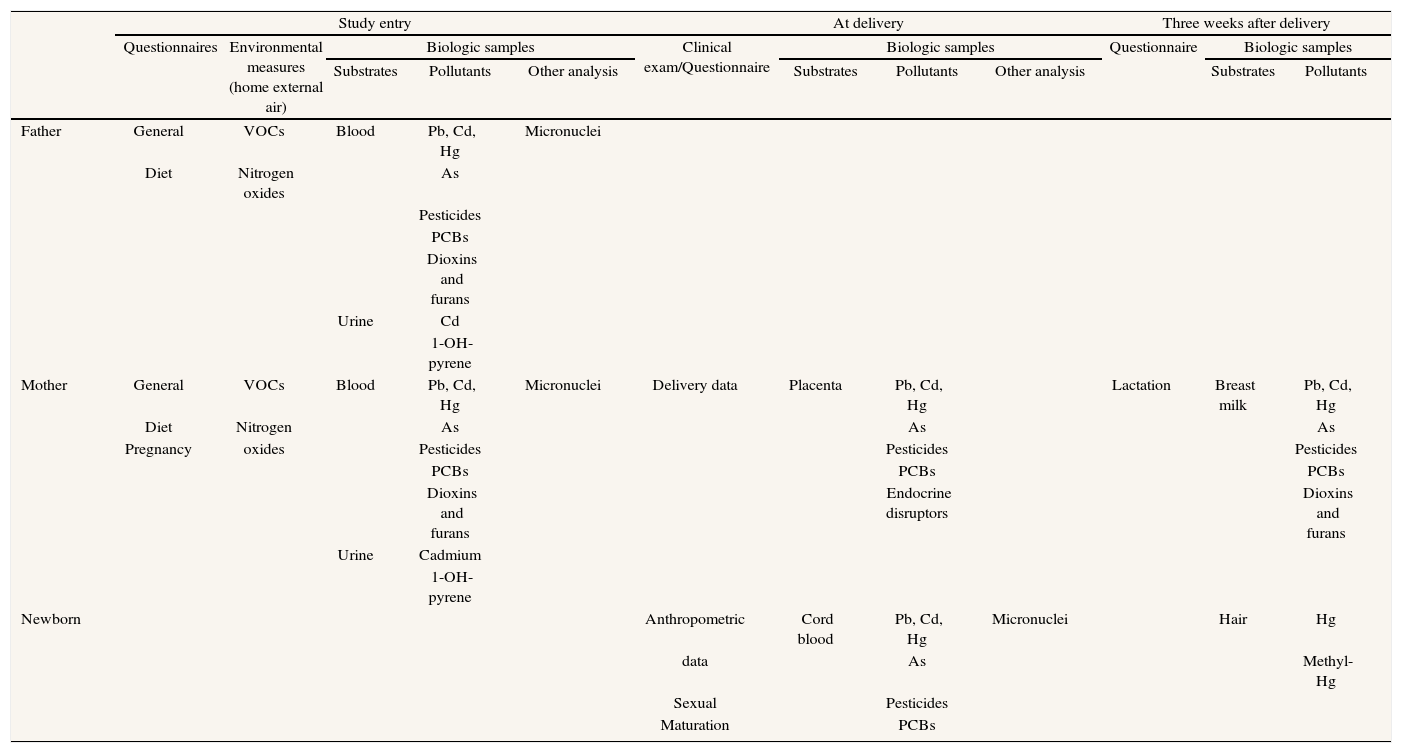
Table 4 summarizes the schedule for the field work in which parents were intended to play an active role. At enrolment, midwives assigned an identification num- ber to the future triplet, and presented them with a small bag. It contained general information about the project, an instruction leaflet, and the logistic material for the study, including a breast-milk pump to collect milk samples, which was also handed out as a gift. All the material in the bag was pre-labeled with the trio number plus an identification character that would allow each of its members to be distinguished («M» [madre]for mo- thers, «P» [padre]for fathers, and «H» [hijo/a]for children). The necessary material for collecting biologic spe- cimens was suitably labeled and wrapped in three packs, one for each member of the triplet.
BioMadrid field-work schedule: data collected, substrates, and pollutants
| Study entry | At delivery | Three weeks after delivery | ||||||||||
| Questionnaires | Environmental measures (home external air) | Biologic samples | Clinical exam/Questionnaire | Biologic samples | Questionnaire | Biologic samples | ||||||
| Substrates | Pollutants | Other analysis | Substrates | Pollutants | Other analysis | Substrates | Pollutants | |||||
| Father | General | VOCs | Blood | Pb, Cd, Hg | Micronuclei | |||||||
| Diet | Nitrogen oxides | As | ||||||||||
| Pesticides | ||||||||||||
| PCBs | ||||||||||||
| Dioxins and furans | ||||||||||||
| Urine | Cd | |||||||||||
| 1-OH-pyrene | ||||||||||||
| Mother | General | VOCs | Blood | Pb, Cd, Hg | Micronuclei | Delivery data | Placenta | Pb, Cd, Hg | Lactation | Breast milk | Pb, Cd, Hg | |
| Diet | Nitrogen | As | As | As | ||||||||
| Pregnancy | oxides | Pesticides | Pesticides | Pesticides | ||||||||
| PCBs | PCBs | PCBs | ||||||||||
| Dioxins and furans | Endocrine disruptors | Dioxins and furans | ||||||||||
| Urine | Cadmium | |||||||||||
| 1-OH-pyrene | ||||||||||||
| Newborn | Anthropometric | Cord blood | Pb, Cd, Hg | Micronuclei | Hair | Hg | ||||||
| data | As | Methyl-Hg | ||||||||||
| Sexual | Pesticides | |||||||||||
| Maturation | PCBs | |||||||||||
VOCs: volatile organic compounds, including benzene, toluene, ethylbenzene, m+p-xylene and o-xylene; PCBs: polychlorinated biphenyls.
Midwives scheduled a date for both parents to col- lect blood and urine specimens, coinciding with the pro- grammed control of the pregnant women at approxi- mately 38 weeks of pregnancy. By appointment, trained personnel interviewed both parents at their home to complete the epidemiologic questionnaires.
Phase 2: delivery roomAt delivery, mothers informed the hospital that they were BioMadrid participants, and provided the newborn pack included in the kit, with the blood tubes for cord blood and the labels to identify the placenta container, previously supplied to the hospital by the research team. Midwives attending the birth collected the required bio- logic specimens and registered basic information on labor. Placenta was collected and frozen whole. During hospitalization, pediatricians performed a clinical ex- amination of the newborns and collected data on clinical, anthropometric and sexual development at birth.
Phase 3: at homeThree weeks after delivery, women were contacted by telephone at home to answer a brief breastfeeding questionnaire and to arrange for the breast milk and new- born hair specimens to be picked up. Mothers had pre- viously received written instructions on how to collect these specimens properly, by using the breast pump pro- vided and cutting a lock of their children's hair.
Biologic sample processingAll specimens were collected in accordance with specific protocols, in containers labeled with the subject identification number and date. In brief, five different types of specimens were collected (table 4). Adult blood specimens (30 ml) and cord blood (12.5 ml) were taken, using the vacutainer system with different tubes, namely: he- parine tubes for heavy metal and micronuclei analysis; tubes containing gelose for routine biochemical analyses; tubes with EDTA for routine hemogram; and empty, simple glass standard tubes for organochlorines and dioxins. The recipient laboratory identified the specimens with the case codes, performed the systematic hemogram and biochemical determinations, extracted the serum and then sent the heparinized tubes to the Genetic Department of the Ramón y Cajal Hospital for micronuclei analysis, and all remaining specimens to the Madrid Regional Public Health Laboratory (RPHL), where they were centra- lized, classified, frozen and stored at –70 oC.
Urine specimens (100 ml) corresponded to the first morning urine passed on the date appointed for blood extraction. Receptacles had to be wrapped in aluminum foil to avoid light exposure, and were kept refrigerated at 2-8 oC by the recipient laboratory until submission to the RPHL.
Placentas were frozen at –20 °C immediately after birth at the maternity ward.
Milk samples (20 ml) were collected by mothers at the end of third week post-delivery, after having fed their babies. Milk receptacles were kept refrigerated (2-8 oC) until collected by study personnel, and frozen and sto- red at the RPHL. Three weeks postpartum and after the baby had been bathed, a lock of newborn hair was cut with scissors by the parents and kept at room tempe- rature until analysis.
Environmental measuresAs part of this research project, passive air samplers were positioned around study participants' place of re- sidence, in order to take outdoor measurements of air pollutants. The aim was to ascertain exposure to nitrogen dioxide and volatile organic compounds (benzene, to- luene, ethylbenzene, m+p-Xylene and o-xylene) in the two study areas. Passive air samplers, analytical determinations and methodology were in accordance with the INMA protocols20, though in our case a single sam- pling campaign was completed. A total of 80 passive air samplers were deployed, 29 in the urban area (Vallecas district) and 51 in the outlying area (Getafe and Parla districts). These measures may help to have a bet- ter knowledge of the study areas pollution profile.
QuestionnairesQuestionnaires were used in all three phases of the field work. The design of the principal epidemiologic questionnaire, completed at study entry, took the INMA protocols into account so as to allow for future comparisons with INMA results. Sex-specific versions were initially tes- ted on a small sample of mothers and fathers in each area, and some questions were reworded in line with the results of this trial. The interview lasted around 40 minutes and included questionnaires with several modules: sociodemographic information; tobacco exposure (lifelong use, recent and current smoking, and second- hand exposure); occupational history; socioeconomic data; environmental exposures at home; and, reproductive and general medical history (diseases, drug consump- tion, radiological exposure, and dental fillings). For women, an additional module registered characteristics and cli- nical events during the pregnancy. Dietary information was recorded, using a previously developed and validated food-frequency questionnaire21–23, which enables nutrient intake to be estimated.
At the hospital, health staff completed a sheet re- cording delivery and newborn health status and an- thropometric data. Finally, a lactation questionnaire re- gistered information on the lactation process and sample collection.
Ethical considerationsBoth the study protocol and informed consent form complied with the principles of the Helsinki Declaration and were formally approved by the Ethical Committee of the Carlos III Institute of Health. As children were in- volved in this project, the final version of the protocol was also submitted to the official Children's Ombuds- man for the Madrid Autonomous Region. Personal data and biologic samples were stored in accordance with prevailing Spanish legal and ethical requirements. Confidentiality was guaranteed. Participants were pro- vided with a contact telephone number in the event that they might have any doubts or queries, or wish to with- draw their consent to participate at any time.
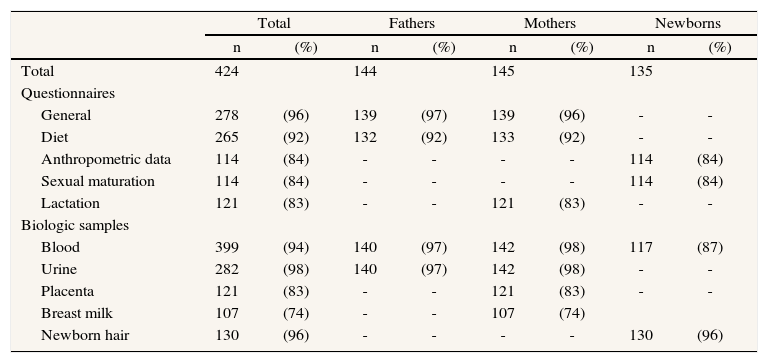
Field work resultsTable 5 summarizes the main results. Of the origi- nally planned 150 triplets, we finally recruited 145 mothers, 144 fathers and 135 newborns. It has to be taken into account that blood cord collection, which took place at approximately one month after initial parents' sample collection, had additional difficulties as it required that: a) mothers provide the material included in the kit to the hospital personnel, and inform that they were BioMadrid participants, and b) delivery circumstances per- mit the normal collection of samples.
BioMadrid study: field work results
| Total | Fathers | Mothers | Newborns | |||||
| n | (%) | n | (%) | n | (%) | n | (%) | |
| Total | 424 | 144 | 145 | 135 | ||||
| Questionnaires | ||||||||
| General | 278 | (96) | 139 | (97) | 139 | (96) | - | - |
| Diet | 265 | (92) | 132 | (92) | 133 | (92) | - | - |
| Anthropometric data | 114 | (84) | - | - | - | - | 114 | (84) |
| Sexual maturation | 114 | (84) | - | - | - | - | 114 | (84) |
| Lactation | 121 | (83) | - | - | 121 | (83) | - | - |
| Biologic samples | ||||||||
| Blood | 399 | (94) | 140 | (97) | 142 | (98) | 117 | (87) |
| Urine | 282 | (98) | 140 | (97) | 142 | (98) | - | - |
| Placenta | 121 | (83) | - | - | 121 | (83) | - | - |
| Breast milk | 107 | (74) | - | - | 107 | (74) | ||
| Newborn hair | 130 | (96) | - | - | - | - | 130 | (96) |
Among adults, blood and urine specimens were ob- tained in over 97% of subjects, the general questionnaire attained similar figures, and dietary record she- ets were completed in 92% of cases.
In newborns, the most frequently obtained specimen was hair (96%) followed by cord blood (87%) (table 5). In one case lost to follow up was due to miscarriage. Other nine children with no biological samples were born alive, though were lost due to different reasons: one woman forgot to take the kit including instructions and material needed to collect the biological samples; four mothers were sent to a non-participant hospital to give birth due to overcrowded maternal wards in the refe- rence centers, and in four other cases complications in delivery distorted the logistical arranged procedures.
The lowest figures corresponded to placentas (81%) and milk samples (74%). Fourteen of the lactating mothers answered the lactation questionnaire but failed to collect a breast milk specimen or provided an insuffi- cient volume of milk. In general, participants reported that the instructions supplied were clearly understan- dable. All BioMadrid protocols are available upon request.
DiscussionThis project is the first comprehensive study of po- llutant levels in the population of the Madrid Region. It will provide an estimate of environmental exposure to different pollutants in several biologic specimens from fathers, mothers and newborns in the study areas, and will help design a feasible environmental surveillance system based on human biomarkers. In spite of the study's complex design, field work results can be con- sidered as satisfactory.
Why triplets? Three populations at handAfter considering different strategies, it was decided that the target population of the study were to be triplets of mothers, fathers and newborns. This design en- ables environmental exposures to be simultaneously as- sessed in adults and newborns. The short follow-up included in the study rendered it possible for data about the whole perinatal period to be obtained. Fathers are not usually included in these types of studies, yet they nevertheless represent half the adult population and an important part of the environment in which children will be raised.
Our aim was to obtain a representative sample of the general population. The decision to study women who intended to give birth in a public hospital implied the exclusion of a proportion of couples with private insurance and, in all likelihood, higher income. Yet, there are several factors that probably served to lessen this bias: a) the universal coverage of the public health system in Spain; b) the good image of the recently-open- ed public maternity ward in the urban study area (Vallecas District), which even attracted people from other health districts, and c) the lack of private hospitals in the Madrid metropolitan area. Additionally, account must be taken of the fact that the design selected fertile couples in the third trimester of pregnancy, which means that, if a contaminant affects fertility or shortens pregnancy length, the concentration in our adult sample might underestimate its levels in the general population.
ParticipationThis study was organized by Public Health Autho- rities, which wanted to incorporate the project within the public health care organization. Thus midwives, who were not part of the research team, were in charge of enrol- ment. Differences of involvement of midwives might have partially influenced recruitment rates by centres, though the research team maintained repeated personal con- tacts in order to encourage them. Even if it seems ob- vious, it is important to insist on the fact that recruitment is one of the critical points in this kind of studies and perhaps additionally efforts to explain the research and to motivate candidates might improve participation rates.
One might wonder if recruitment rates could have been higher, had we hired specific personnel for it. Ho- wever, population studies which require active participation generally have low participation rates. In our case, the rate of women's initial agreement to participate (52%) was similar to those described in other studies of preg- nant women in Spain (54%)24 and lower than that of the general population of Western Germany (63%)8. Ho- wever, our design entailed the need for agreement by a second population, i.e., the fathers, whose rate of con- sent to participate was similar. Consequently, overall agreement for this study decreased to 29%. In contrast, participants were highly motivated and played an active role in the logistics of the project, since they kept most of the specimen-collection material at home and were responsible for taking it to the extraction points and the maternity ward.
Our results showed that women who refused were similar to those who agreed to participate in this study in terms of age and parity, and proportion of non-Spa- nish subjects. Our sample might perhaps overrepresent people with healthier lifestyles and, probably, with a slightly higher socioeconomic status, since a higher edu- cational level was observed for participants versus non- participants. Among mothers who took part, education- related and, to a lesser extent, health-related jobs were more frequent than cleaning-related occupations and housewives.
Biologic substrates and measuresOne of the study objectives was to assess which biologic substrates might be more suitable for an environmental surveillance system. Owing to budget constraints, we had to find an equilibrium between sample size and the number of substrates and pollutants to be studied. We wished to test: a) the acceptability of each biolo- gical sample; b) logistic aspects linked to specimen -collection, -processing and -storage, and c) informati- ve output, i.e., number and type of pollutants that can be effectively measured and the time frame that these represent. With respect to the toxicants to be studied, we selected the main agents to which a population like of Madrid is thought to be exposed daily, including cer- tain heavy metals, persistent organic pollutants (POPs), and polycyclic aromatic hydrocarbons (PAH). Finally, mi- cronuclei, a commonly used unspecific index of cyto- genetic damage25, was incorporated to provide a biologic response marker of exposure to genotoxic agents.
Some initial lessons learnedThough blood is the most versatile substrate, it re- quires trained personnel, and there is an ethical limit to the amount of specimen that can be collected. Thus, for some of the pollutants, e.g., dioxins, blood from several participants had to be pooled in order to achieve the size needed for analysis. Some types of bio specimens, such as placenta and cord blood, were easier to obtain than had been supposed, since maternity ward staff are used to collecting these for other purposes. Moreover, in the case of placenta, it is a large organ that can be easily collected. In contrast, most newborn hair samples were regarded by the laboratory as being insufficient (less than 5 mg) for the purpose of obtai- ning accurate measurements. Additional non-invasive substrates that could have been included in the study protocol were nails and meconium. Repeated milk specimens, also easy to collect, could have been taken in order to store part for future purposes, though in that case telephone calls to remind subjects of specimen collection should be scheduled to avoid any possible over- sights. Insofar as the selected biomarkers are concerned, cotinine could have been as well considered.
ConclusionsThis project has enabled the complexity of imple- menting a surveillance program using biologic samples to be estimated. In the next future, we have still several questions to answer when laboratory analyses are completed, including the discussion about the most suit- able toxicants and biological samples to be considered in a surveillance system. Nevertheless, the financial and human effort needed to put a system like this into ope- ration calls for firm political backing. The results of this study will serve to tailor the design of any future surveillance system to the reality of the Madrid Region.
AcknowledgmentsFinancial support was obtained from the Madrid Regional Health & Consumer Affairs Authority and the Spanish Health Research Fund (Fondo de Investigación Sanitaria [FIS]) grant PI040777.
The authors are deeply indebted to the primary-care midwives and health staff of the Gregorio Marañón and Getafe Hospital maternity wards and laboratories, and, in particular, to the study participants themselves. Their unstinting and al- truistic collaboration made this study possible. We should also like to thank: the INMA study research team for their encour- agement and assistance; and Michael Benedict for his help with the English.











