




Among men who have sex with men (MSM), the association between searching for sexual partners’ on the Internet and increased risk of sexually transmitted infections (STIs)/HIV infection, together with current low levels of partner notification (PN), justifies a study to explore the intention to use new communication technologies for PN in Spain.
MethodsTwo cross-sectional surveys were performed: the first was administered online to visitors to web pages where the survey was advertised; the second was administered on paper to patients attending an STI Unit and centres similar to Community-Based Voluntary Counselling and Testing centres.
ResultsThe study population comprised 1578 Spanish residents (median age, 34 years [range: 18 to 74]); 84% lived in urban areas, and 69% reported searching for sexual partners on the Internet. Thirty-seven per cent would be willing to use a website for PN, 26% did not know if they would use one, and 37% would not want to use one. The main reasons for not intending to notify STI/HIV were “shame or fear” (stable partner) and “not knowing how to contact them” (casual partner). The preferred method of notification was face to face (73%) for both stable and casual partners, although using new technologies (Short Messaging System, e-mail, web page, phone applications) was widely accepted for notifying casual partners.
ConclusionsFighting stigma and promoting alternative methods of PN among MSM and health professionals through new technologies could increase the frequency of PN. This approach will improve early detection and reduce transmission in Spain.
Entre los hombres que tienen sexo con hombres, la asociación entre buscar parejas por internet y el incremento de riesgo para presentar una Infección de Transmisión Sexual (ITS), junto con la baja frecuencia de la práctica de la notificación a las parejas sexuales expuestas a un infectado justifican explorar la intención de uso de las nuevas tecnologías para facilitar dicha notificación en España.
MétodosSe han utilizado dos estudios transversales: el primero, administrado “online” a los visitantes de páginas web donde se publicitaba la encuesta; el segundo, administrado en formato papel en una Unidad Especializada de Atención a las ITS y otros centros similares a los de soporte y realización de pruebas.
ResultadosParticiparon 1578 personas residentes en España, mediana de edad 34 años (Rango: 18- 74); 84% de áreas urbanas, 69% buscaron parejas sexuales en internet. Un treinta y siete por ciento utilizarían un página web si estuviera disponible, un 26% no sabían si lo harían y otro 37% no la utilizarían. Las razones principales para no tener la intención de notificar de ITS/VIH a una pareja estable fueron: “miedo o vergüenza”; a una pareja ocasional: “no saber cómo contactarla”. El método preferido para notificar fue el “cara a cara o por teléfono” (73%), tanto en caso de pareja estable como ocasional. El uso de nuevas tecnologías (SMS, e-mail, web page, aplicaciones de teléfono) fue más aceptado en caso de pareja ocasional
ConclusionesLa lucha contra el estigma y la promoción del uso de nuevas tecnologías para la notificación a las parejas sexuales, entre los hombres que tienen sexo con hombres (HSH) y por parte de los profesionales de la salud, pueden aumentar la notificación, con los beneficios esperados de una más temprana detección de casos y una reducción de la transmisión en España.
Partner notification (PN) is the process whereby the sexual partner(s) of a patient diagnosed with a sexually transmitted infection (STI) who presents for care is identified and informed of his/her exposure. The partner(s) is then invited to attend for testing, counselling, and, where necessary, treatment.1
Although several studies analyse interventions to prevent transmission of HIV among men who have sex with men (MSM)2–6 based on new information and communication technologies, most explore rates of HIV testing. Very few explore PN practices. Evidence-based reviews show the effectiveness of PN in identifying persons at risk of STIs/HIV infection,7 and the public health benefits of PN have recently been highlighted in Europe1. Nevertheless, websites have been used to facilitate PN in Canada and the USA,8 Australia,9 Romania8, and the Netherlands.10
The results of studies evaluating one of these sites, “in SPOT”,11–13 are controversial. While some authors find limited evidence of its effectiveness for PN among MSM, others emphasize the higher accessibility to at-risk populations with Internet PN using pseudonyms14 and the broad acceptability of receiving and sending a notification e-mail15,16 or SMS.17
PN in Spain is by voluntary verbal notification from patients to partners following advice from a clinician. The increasing use of the Internet and other new communication technologies to seek sexual contacts highlights the potential for exploring how these technologies could facilitate PN and thus prevent transmission of STIs/HIV infection.18
Anonymous sexual partnering makes PN almost impossible; however, finding ways to optimize notification among traceable partners based on new communication technologies may increase the number of partners identified. In some Spanish autonomous communities, such as Catalonia, patient referral PN is already in place in the main STI Units, despite significant difficulties in regularly assessing the “yield” of PN in both MSM and heterosexuals. Nowadays, medical and public health practitioners are convinced of the need to strengthen and update this practice, using both traditional methods and new communication technologies (e-Cards, mobile phone, blogs, social networking sites).19
Internet-based PN methods for MSM have proved to be well accepted20 and effective21 in the USA, although not much is known about their acceptability in Spain, or even in Europe.
Among MSM, the rise in the incidence of STIs22 and risky sexual behaviours, the association between searching for sexual partners’ on the Internet and an increased risk of STIs,23 and low levels of PN24 justify a study to explore the intention to use new communication technologies for PN in Spain.
The aim of this study was to describe current PN practices and assess the intention to use new information and communication technologies for notifying partners of STI/HIV infection among MSM in Spain.
MethodsWe conducted a survey that was administered in two formats. The first format was an online survey advertised on three web pages: one for sexual contacts (Chueca) (http://www.chueca.com), an online magazine (Universo gay) (http://www.universogay.com) and a lesbian, gay, transgender and bisexual web page for Barcelona (http://www.stopsida.org). The questionnaire was administered to participants throughout Spain using an online survey service (http://www.surveymonkey.com) from 27th June to 1st October 2013. The second format was a centre-based survey, which involved a pen and paper questionnaire and was offered at three different venues in Barcelona: an STI Unit, an HIV outreach program run by the Public Health Agency of Barcelona for the users of a gay sauna and a lesbian, gay, transgender and bisexual social facility. Informed consent was obtained for both formats of the study.
The study measures and procedures were approved by the Clinical Research Ethics Committee of University Hospital Germans Trias i Pujol in Badalona, Catalonia, Spain.
This survey used a convenience sample of at least 100 questionnaires completed at the STI Unit, 50 at the lesbian, gay, transgender and bisexual social facility and 50 at the HIV outreach program of the Public Health Agency of Barcelona.
Participants were recruited opportunistically when attending the centre and were eligible if they were 18 years of age or older, living in Spain and had had sex with another man any time in their lives.
Questionnaire developmentWe conducted two focus groups of 12 participants each (one with HIV-positive MSM and another with HIV-negative MSM). The duration of each focus group was two hours. Average age was 30 years in HIV-negative MSM and 45 years in HIV-positive MSM.
Data from the focus groups were analysed using the grounded theory approach to identify relevant questions.
The centre-based questionnaire was available in Catalan and Spanish and comprised 38 questions. The online questionnaire shared questions with another study exploring the acceptability of pre-exposure prophylaxis and circumcision as bio-behavioural methods of preventing HIV transmission. This questionnaire was only available in Spanish and comprised 86 questions, 38 of which were identical to those in the questionnaires administered in the centres.
Study variablesThe sociodemographic variables were year and country of birth, region of residence, type of residence (urban or rural), level of education, occupation, sexual orientation, places where the patient socialized and number of sexual partners within the 12 months prior to a previous diagnosis of STI. The variables for STI/HIV history were self-reported previous STI, self-reported previous HIV test and self-reported HIV status. The questions used to explore the PN approach were as follows: Did you think of telling your partners about their exposure when you were diagnosed with an STI/HIV? Did you notify them? If you did not notify them, why not? How did you notify them? Do you intend to use new technologies to notify a partner about an STI or an HIV exposure? Does your view depend on the type of relationship (stable or casual)? What is your preferred method of notifying a partner about an STI or HIV exposure? What type of website would you prefer to use for PN?
Statistical methodsIndependent variables included sociodemographic variables and STI/HIV history. Dependent variables included practices and preferences in the use of new technologies for PN. We performed bivariate tests of association using the Fisher exact test and Pearson chi-square test. p values below 0.05 were considered statistically significant. Variables exploring PN of STI and HIV infection were multiple-choice questions, and the answers were treated as separate dichotomous variables (yes/no).
ResultsParticipantsOut of 1999 individuals who accessed the questionnaire (online or at the centres), 1841 (92%) finally participated in the study. After exclusion of 206 individuals below 18 years of age or of unknown age, 23 individuals living outside Spain and 34 heterosexuals who did not report previous experience of sex with men, 1578 participants were eligible for the study. Following the exclusions, 1337 participants completed the questionnaire online and 241 at the centres. The participation rate was higher among those who completed the questionnaire at the centres (241 out of 250 [96%] vs 1337 out of 1749 [76%]).
Given that some participants did not fully complete the questionnaire, there are wide variations in the number of variables answered; therefore, total numbers in the tables are not always the same.
The response rate was higher than 65% for most of the main variables (Table 1 of online annex)
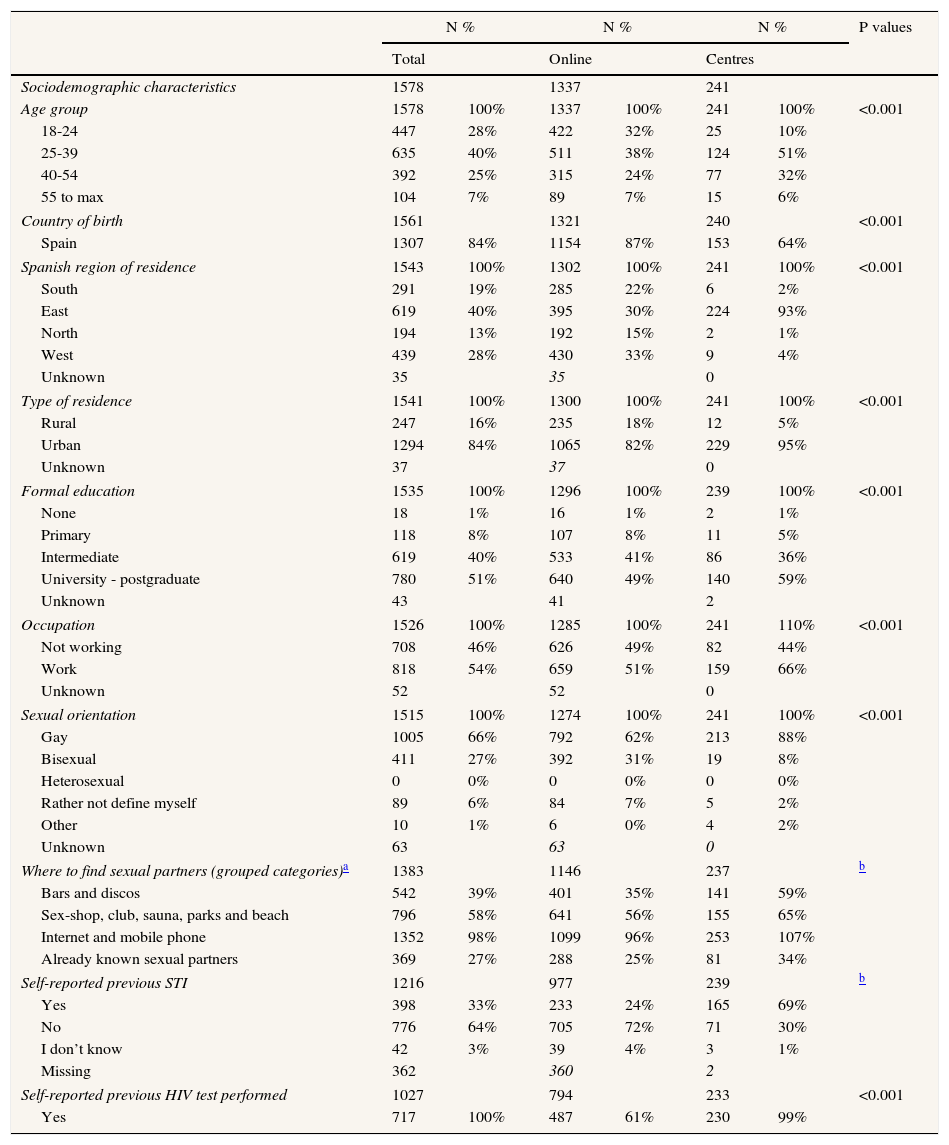
Distribution of main characteristics.
| N % | N % | N % | P values | ||||
|---|---|---|---|---|---|---|---|
| Total | Online | Centres | |||||
| Sociodemographic characteristics | 1578 | 1337 | 241 | ||||
| Age group | 1578 | 100% | 1337 | 100% | 241 | 100% | <0.001 |
| 18-24 | 447 | 28% | 422 | 32% | 25 | 10% | |
| 25-39 | 635 | 40% | 511 | 38% | 124 | 51% | |
| 40-54 | 392 | 25% | 315 | 24% | 77 | 32% | |
| 55 to max | 104 | 7% | 89 | 7% | 15 | 6% | |
| Country of birth | 1561 | 1321 | 240 | <0.001 | |||
| Spain | 1307 | 84% | 1154 | 87% | 153 | 64% | |
| Spanish region of residence | 1543 | 100% | 1302 | 100% | 241 | 100% | <0.001 |
| South | 291 | 19% | 285 | 22% | 6 | 2% | |
| East | 619 | 40% | 395 | 30% | 224 | 93% | |
| North | 194 | 13% | 192 | 15% | 2 | 1% | |
| West | 439 | 28% | 430 | 33% | 9 | 4% | |
| Unknown | 35 | 35 | 0 | ||||
| Type of residence | 1541 | 100% | 1300 | 100% | 241 | 100% | <0.001 |
| Rural | 247 | 16% | 235 | 18% | 12 | 5% | |
| Urban | 1294 | 84% | 1065 | 82% | 229 | 95% | |
| Unknown | 37 | 37 | 0 | ||||
| Formal education | 1535 | 100% | 1296 | 100% | 239 | 100% | <0.001 |
| None | 18 | 1% | 16 | 1% | 2 | 1% | |
| Primary | 118 | 8% | 107 | 8% | 11 | 5% | |
| Intermediate | 619 | 40% | 533 | 41% | 86 | 36% | |
| University - postgraduate | 780 | 51% | 640 | 49% | 140 | 59% | |
| Unknown | 43 | 41 | 2 | ||||
| Occupation | 1526 | 100% | 1285 | 100% | 241 | 110% | <0.001 |
| Not working | 708 | 46% | 626 | 49% | 82 | 44% | |
| Work | 818 | 54% | 659 | 51% | 159 | 66% | |
| Unknown | 52 | 52 | 0 | ||||
| Sexual orientation | 1515 | 100% | 1274 | 100% | 241 | 100% | <0.001 |
| Gay | 1005 | 66% | 792 | 62% | 213 | 88% | |
| Bisexual | 411 | 27% | 392 | 31% | 19 | 8% | |
| Heterosexual | 0 | 0% | 0 | 0% | 0 | 0% | |
| Rather not define myself | 89 | 6% | 84 | 7% | 5 | 2% | |
| Other | 10 | 1% | 6 | 0% | 4 | 2% | |
| Unknown | 63 | 63 | 0 | ||||
| Where to find sexual partners (grouped categories)a | 1383 | 1146 | 237 | b | |||
| Bars and discos | 542 | 39% | 401 | 35% | 141 | 59% | |
| Sex-shop, club, sauna, parks and beach | 796 | 58% | 641 | 56% | 155 | 65% | |
| Internet and mobile phone | 1352 | 98% | 1099 | 96% | 253 | 107% | |
| Already known sexual partners | 369 | 27% | 288 | 25% | 81 | 34% | |
| Self-reported previous STI | 1216 | 977 | 239 | b | |||
| Yes | 398 | 33% | 233 | 24% | 165 | 69% | |
| No | 776 | 64% | 705 | 72% | 71 | 30% | |
| I don’t know | 42 | 3% | 39 | 4% | 3 | 1% | |
| Missing | 362 | 360 | 2 | ||||
| Self-reported previous HIV test performed | 1027 | 794 | 233 | <0.001 | |||
| Yes | 717 | 100% | 487 | 61% | 230 | 99% | |
The median age was 34 years (range: 18 to 74). Most of the respondents were born in Spain (84%) and lived in an urban area (84%). By region, 29% lived in Catalonia, followed by 16% in the Community of Madrid and 11% in Andalucía. More than half of the respondents were employed (54%) and had a university or post-graduate degree (51%).
Compared with the online respondents, centre-based respondents were older (37 versus 33 years), were less frequently born in Spain, more frequently lived in an urban area and were more likely to have a university degree. They were also more likely to be employed, to report having had an STI and to have taken an HIV test. (Table 1)
Searching for sexual partnersInternet was the most popular place to look for sexual partners (69%), followed by mobile phone applications (e.g. Grindr or Scruff) (29%).
The number of partners within the last 12 months was only explored in the online questionnaire. Of the 769 respondents to this question, 57% reported having had up to 5 partners, 18% reported between 6 and 10 partners and 25% reported more than 10 partners.
Self-reported lifetime STI/HIV infection and previous HIV testThe response rate was 77% for lifetime STI/HIV infection and 65% for self-reported previous HIV testing. A total of 398 out of 1216 respondents (33%) reported having had an STI, and 717 out of 1027 (70%) had had at least one HIV test.
Older age groups and those with higher educational levels were more likely to have had an STI and undergone a previous HIV test (p<0.001).
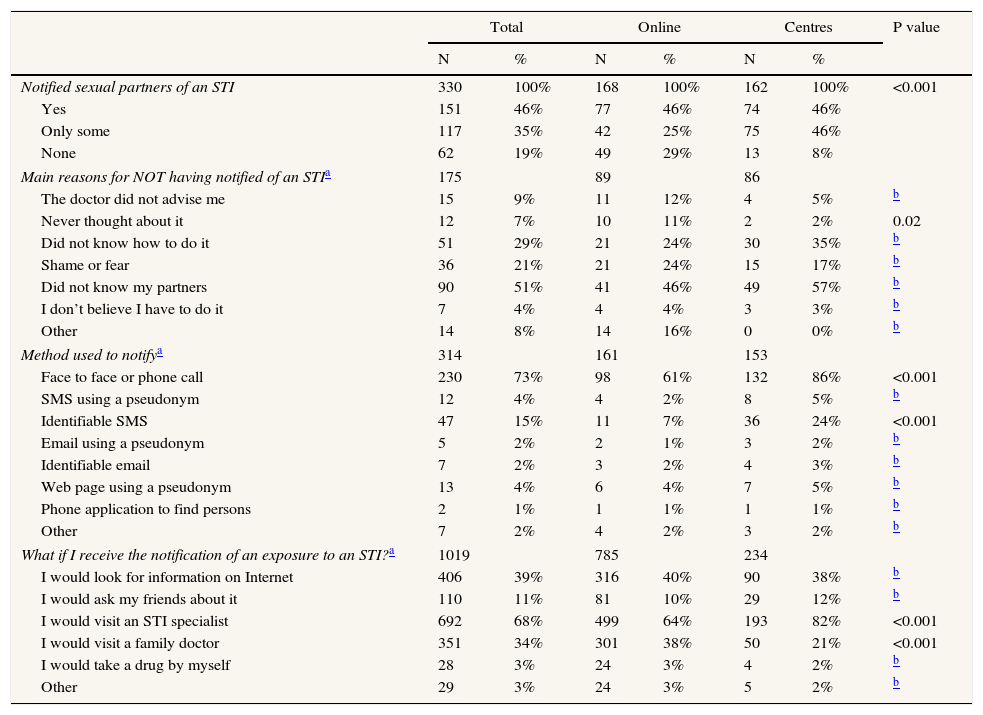
What did I do when diagnosed with an STI?Almost half of those diagnosed with an STI within the previous 12 months notified all their sexual partners, 35% notified only some partners and 19% notified none of their partners.
Centre-based respondents were more likely to notify than online respondents (p<0.001), and participants recruited through the STI Unit notified their partners more frequently than other centre-based participants. The main reason for not having notified an STI was “Did not know my partners”. (Table 2)
Partner notification approach to Sexually Transmitted Infection (STI) in general: What did I do?
| Total | Online | Centres | P value | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Notified sexual partners of an STI | 330 | 100% | 168 | 100% | 162 | 100% | <0.001 |
| Yes | 151 | 46% | 77 | 46% | 74 | 46% | |
| Only some | 117 | 35% | 42 | 25% | 75 | 46% | |
| None | 62 | 19% | 49 | 29% | 13 | 8% | |
| Main reasons for NOT having notified of an STIa | 175 | 89 | 86 | ||||
| The doctor did not advise me | 15 | 9% | 11 | 12% | 4 | 5% | b |
| Never thought about it | 12 | 7% | 10 | 11% | 2 | 2% | 0.02 |
| Did not know how to do it | 51 | 29% | 21 | 24% | 30 | 35% | b |
| Shame or fear | 36 | 21% | 21 | 24% | 15 | 17% | b |
| Did not know my partners | 90 | 51% | 41 | 46% | 49 | 57% | b |
| I don’t believe I have to do it | 7 | 4% | 4 | 4% | 3 | 3% | b |
| Other | 14 | 8% | 14 | 16% | 0 | 0% | b |
| Method used to notifya | 314 | 161 | 153 | ||||
| Face to face or phone call | 230 | 73% | 98 | 61% | 132 | 86% | <0.001 |
| SMS using a pseudonym | 12 | 4% | 4 | 2% | 8 | 5% | b |
| Identifiable SMS | 47 | 15% | 11 | 7% | 36 | 24% | <0.001 |
| Email using a pseudonym | 5 | 2% | 2 | 1% | 3 | 2% | b |
| Identifiable email | 7 | 2% | 3 | 2% | 4 | 3% | b |
| Web page using a pseudonym | 13 | 4% | 6 | 4% | 7 | 5% | b |
| Phone application to find persons | 2 | 1% | 1 | 1% | 1 | 1% | b |
| Other | 7 | 2% | 4 | 2% | 3 | 2% | b |
| What if I receive the notification of an exposure to an STI?a | 1019 | 785 | 234 | ||||
| I would look for information on Internet | 406 | 39% | 316 | 40% | 90 | 38% | b |
| I would ask my friends about it | 110 | 11% | 81 | 10% | 29 | 12% | b |
| I would visit an STI specialist | 692 | 68% | 499 | 64% | 193 | 82% | <0.001 |
| I would visit a family doctor | 351 | 34% | 301 | 38% | 50 | 21% | <0.001 |
| I would take a drug by myself | 28 | 3% | 24 | 3% | 4 | 2% | b |
| Other | 29 | 3% | 24 | 3% | 5 | 2% | b |
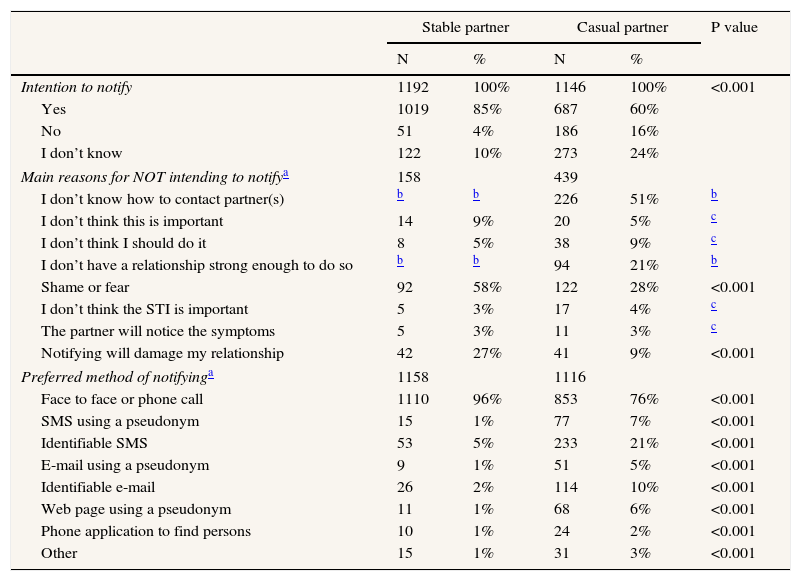
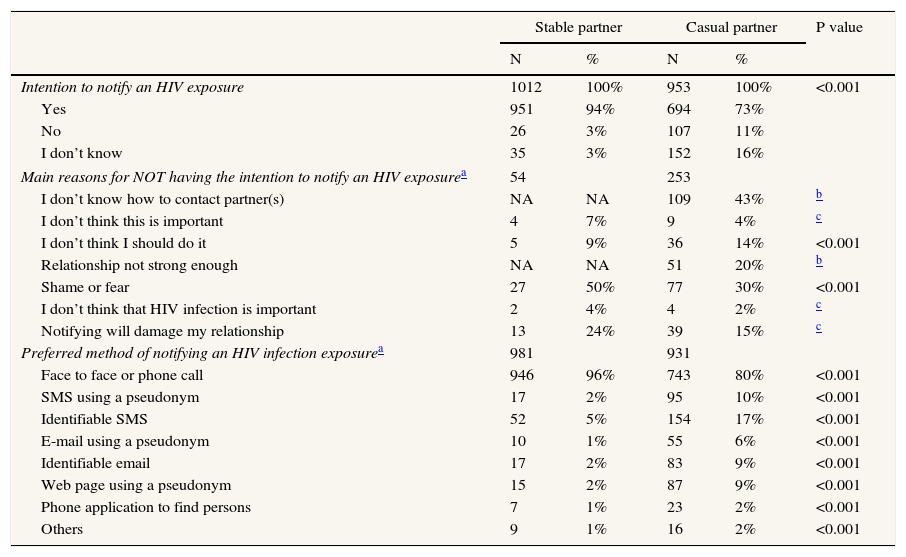
Respondents intended to notify stable partners more frequently than casual partners for both HIV (94% versus 73%, respectively) (p<0.001) and other STIs (85% versus 60%, respectively) (p<0.001).
The main reason for not notifying an STI or HIV infection was “shame or fear” in the case of stable partners and “I don’t know how to contact my partner(s)” in the case of casual partners. “Face to face or phone call” was the preferred method of notification for both types of partner, while new technologies (SMS, e-mail, web page, phone applications to find persons) were preferred by casual partners (p<0.001). (Tables 3 and 4)
Intention to notify an Sexually Transmitted Infection (STI) by type of relationship: What would I do?
| Stable partner | Casual partner | P value | |||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Intention to notify | 1192 | 100% | 1146 | 100% | <0.001 |
| Yes | 1019 | 85% | 687 | 60% | |
| No | 51 | 4% | 186 | 16% | |
| I don’t know | 122 | 10% | 273 | 24% | |
| Main reasons for NOT intending to notifya | 158 | 439 | |||
| I don’t know how to contact partner(s) | b | b | 226 | 51% | b |
| I don’t think this is important | 14 | 9% | 20 | 5% | c |
| I don’t think I should do it | 8 | 5% | 38 | 9% | c |
| I don’t have a relationship strong enough to do so | b | b | 94 | 21% | b |
| Shame or fear | 92 | 58% | 122 | 28% | <0.001 |
| I don’t think the STI is important | 5 | 3% | 17 | 4% | c |
| The partner will notice the symptoms | 5 | 3% | 11 | 3% | c |
| Notifying will damage my relationship | 42 | 27% | 41 | 9% | <0.001 |
| Preferred method of notifyinga | 1158 | 1116 | |||
| Face to face or phone call | 1110 | 96% | 853 | 76% | <0.001 |
| SMS using a pseudonym | 15 | 1% | 77 | 7% | <0.001 |
| Identifiable SMS | 53 | 5% | 233 | 21% | <0.001 |
| E-mail using a pseudonym | 9 | 1% | 51 | 5% | <0.001 |
| Identifiable e-mail | 26 | 2% | 114 | 10% | <0.001 |
| Web page using a pseudonym | 11 | 1% | 68 | 6% | <0.001 |
| Phone application to find persons | 10 | 1% | 24 | 2% | <0.001 |
| Other | 15 | 1% | 31 | 3% | <0.001 |
Intention to notify an HIV infection by type of relationship: What would I do?
| Stable partner | Casual partner | P value | |||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Intention to notify an HIV exposure | 1012 | 100% | 953 | 100% | <0.001 |
| Yes | 951 | 94% | 694 | 73% | |
| No | 26 | 3% | 107 | 11% | |
| I don’t know | 35 | 3% | 152 | 16% | |
| Main reasons for NOT having the intention to notify an HIV exposurea | 54 | 253 | |||
| I don’t know how to contact partner(s) | NA | NA | 109 | 43% | b |
| I don’t think this is important | 4 | 7% | 9 | 4% | c |
| I don’t think I should do it | 5 | 9% | 36 | 14% | <0.001 |
| Relationship not strong enough | NA | NA | 51 | 20% | b |
| Shame or fear | 27 | 50% | 77 | 30% | <0.001 |
| I don’t think that HIV infection is important | 2 | 4% | 4 | 2% | c |
| Notifying will damage my relationship | 13 | 24% | 39 | 15% | c |
| Preferred method of notifying an HIV infection exposurea | 981 | 931 | |||
| Face to face or phone call | 946 | 96% | 743 | 80% | <0.001 |
| SMS using a pseudonym | 17 | 2% | 95 | 10% | <0.001 |
| Identifiable SMS | 52 | 5% | 154 | 17% | <0.001 |
| E-mail using a pseudonym | 10 | 1% | 55 | 6% | <0.001 |
| Identifiable email | 17 | 2% | 83 | 9% | <0.001 |
| Web page using a pseudonym | 15 | 2% | 87 | 9% | <0.001 |
| Phone application to find persons | 7 | 1% | 23 | 2% | <0.001 |
| Others | 9 | 1% | 16 | 2% | <0.001 |
There were no age differences in notifying (p=0.961) or intending to notify stable (p=0.628) or casual (p=0.551) partners of an STI exposure. Similarly, there were no age differences in intention to notify stable (p=0.124) or casual (p=0.232) partners of an HIV exposure.
No differences in educational level were found for intending to notify casual partners of an STI (p=0.452) or HIV exposure (p=0.955), although respondents with higher levels of education were more likely to notify their stable partners of an exposure to HIV (p<0.001) or any other STI (p<0.05).
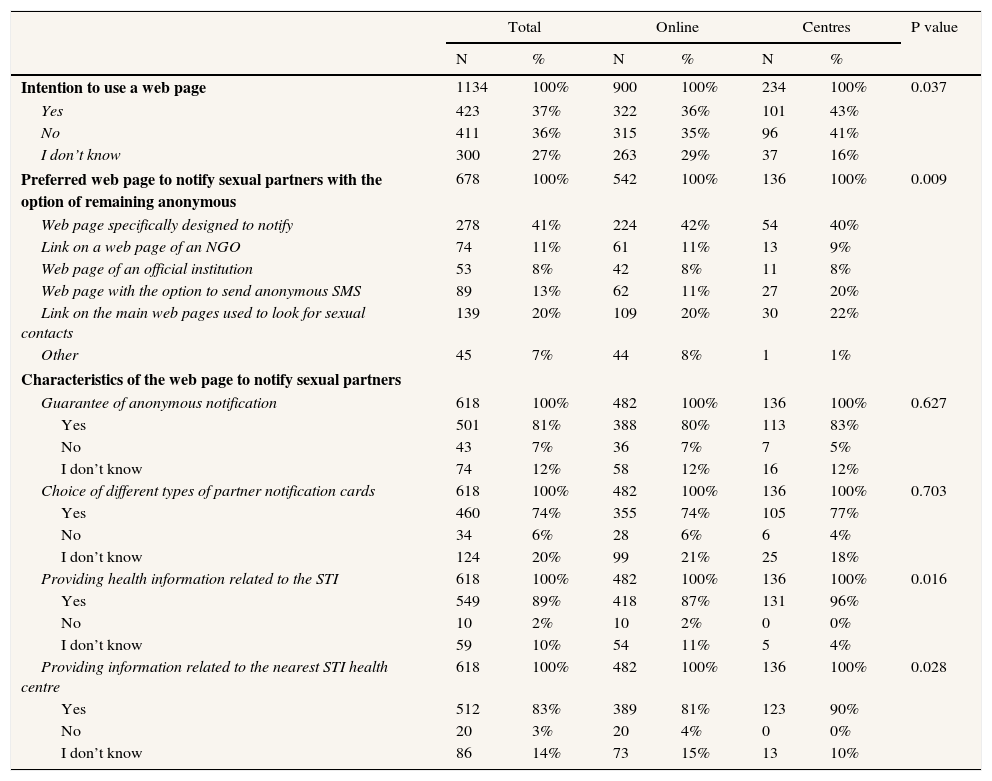
Intention to use a web page to notify sexual partners and type of web pageThirty-seven per cent of all respondents said they would be willing to use a web page, 27% were unsure whether they would use it and 36% would not use a web page to notify sexual partners. Centre-based respondents were less likely to use a web page than online respondents.
There were no differences in intention to use a web page to notify sexual partners by age group (p=0.922) or by educational level (p=0.452)
The preferred characteristics of the web pages are presented in Table 5.
Intention to use and type of web page to notify sexual partners.
| Total | Online | Centres | P value | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Intention to use a web page | 1134 | 100% | 900 | 100% | 234 | 100% | 0.037 |
| Yes | 423 | 37% | 322 | 36% | 101 | 43% | |
| No | 411 | 36% | 315 | 35% | 96 | 41% | |
| I don’t know | 300 | 27% | 263 | 29% | 37 | 16% | |
| Preferred web page to notify sexual partners with the option of remaining anonymous | 678 | 100% | 542 | 100% | 136 | 100% | 0.009 |
| Web page specifically designed to notify | 278 | 41% | 224 | 42% | 54 | 40% | |
| Link on a web page of an NGO | 74 | 11% | 61 | 11% | 13 | 9% | |
| Web page of an official institution | 53 | 8% | 42 | 8% | 11 | 8% | |
| Web page with the option to send anonymous SMS | 89 | 13% | 62 | 11% | 27 | 20% | |
| Link on the main web pages used to look for sexual contacts | 139 | 20% | 109 | 20% | 30 | 22% | |
| Other | 45 | 7% | 44 | 8% | 1 | 1% | |
| Characteristics of the web page to notify sexual partners | |||||||
| Guarantee of anonymous notification | 618 | 100% | 482 | 100% | 136 | 100% | 0.627 |
| Yes | 501 | 81% | 388 | 80% | 113 | 83% | |
| No | 43 | 7% | 36 | 7% | 7 | 5% | |
| I don’t know | 74 | 12% | 58 | 12% | 16 | 12% | |
| Choice of different types of partner notification cards | 618 | 100% | 482 | 100% | 136 | 100% | 0.703 |
| Yes | 460 | 74% | 355 | 74% | 105 | 77% | |
| No | 34 | 6% | 28 | 6% | 6 | 4% | |
| I don’t know | 124 | 20% | 99 | 21% | 25 | 18% | |
| Providing health information related to the STI | 618 | 100% | 482 | 100% | 136 | 100% | 0.016 |
| Yes | 549 | 89% | 418 | 87% | 131 | 96% | |
| No | 10 | 2% | 10 | 2% | 0 | 0% | |
| I don’t know | 59 | 10% | 54 | 11% | 5 | 4% | |
| Providing information related to the nearest STI health centre | 618 | 100% | 482 | 100% | 136 | 100% | 0.028 |
| Yes | 512 | 83% | 389 | 81% | 123 | 90% | |
| No | 20 | 3% | 20 | 4% | 0 | 0% | |
| I don’t know | 86 | 14% | 73 | 15% | 13 | 10% | |
In this study, we used online and centre-based questionnaires to explore what was and would be done in the event of being diagnosed with an STI or HIV infection, whether PN would vary by type of relationship (stable or casual) and what the preferences would be for the use of new technologies. Sociodemographic characteristics differ depending on the source of information (online or centre), with centre-based respondents being older and more frequently having had a previous STI/HIV infection. The intention to notify is higher among centre-based respondents and within stable relationships. Conversely, the intention to use a web page to notify was highest among online respondents. On the other hand, neither age group nor educational level seems to affect the intention to use a web page for PN.
Participants recruited through the STI Unit were guided by STI specialists and were more likely to notify their partners of a recently diagnosed STI.
Of note, respondents reported that they did not notify partners for the following reasons: “I didn’t know how to do it”, “My doctor didn’t advise me” and “I never thought about it”. Consequently, raising awareness among GPs and other medical staff combined with counselling for STI/HIV infection could improve PN.
Because the main reasons for not having notified a partner were “I didn’t know my partners” and “I didn’t know how to do it”, the main challenges in PN arise from anonymous or non-contactable partners. In this regard, new communication tools such as gay web pages, social networks and mobile applications may help to identify otherwise untraceable individuals. Encouragement by health professionals to contact partners by mobile phone while the patient is still in the clinic could speed up the consultation process and the diagnosis and treatment of partners.
Once an exposure is notified, half of the respondents would consult an STI specialist and 30% a family doctor. This indicates that the STI Unit and primary care centres are key locations for promoting alternative methods of PN as a complement to the standard notification card used in patient referral PN.
In the present study, 37% of respondents reported a clear intention to use a web page to notify partners, and 26% did not know whether they would use one. This finding may be attributable to cultural issues or a preference for face-to-face contact rather than technology-based communication.
The preferred web page was “one that was specifically designed to notify” followed by the “one linked to web pages used to look for sexual partners” and a “web page with the option of sending anonymous SMS”. These three options could be easily merged when designing a public health intervention. Cost issues related to staff training, monitoring and program evaluation could arise, although expert opinion suggests that online PN systems are relatively inexpensive25 and that there is potential for email and text-notification to improve the efficiency and cost-effectiveness of PN.26 Nevertheless, this hypothesis has to be assessed locally. Furthermore, a very recent evidence review of new technologies for PN of STI concludes that the importance of technology in the prevention and treatment of STI is expected to increase.27 Our results suggest that some types of new technology solutions for PN among MSM may be more acceptable than others depending on age, education level and type of relationship.
The fact that “shame or fear” is the main reason for not intending to notify a stable partner warrants further analysis in order to explore ways to overcome this barrier. For example, societal changes could be promoted to reduce the stigma of STI/HIV infection, and sexual health information could be provided on the benefits of PN. Not surprisingly, other studies28 have also found that up to one-third of patients fail to tell all their partners because of embarrassment or fear.
Consistent with the results of other studies,29 we found that the preferred method of notification is face to face, although most of the additional comments are along the lines of “as long as I get to know it, it doesn’t matter how”. “Identifiable SMS” and “a webpage using a pseudonym” or “SMS using a pseudonym” are also mentioned as good PN methods. Surprisingly, these methods differ substantially, and further research should be conducted to characterize discrepancies.
Experiences that enhance PN through new information and communication technologies are currently being used throughout the world. Examples include the use of Facebook in the USA,30 the “suggest a test” project/intervention in the Netherlands,31 and “Let them know”32 and “the Drama Downunder”33 in Australia. These experiences should lead to the revision of the PN strategies used to date in Spain.
“Canal Salut”34 is an evidence-based health-related website run by the Catalan Department of Health with a section on promotion of sexual health for young people that could host a section to support PN in both this group and in MSM.
LimitationsFirst, we report on practices related to STI in general without differentiating between HIV and other STI; therefore, some of our findings may not be representative of HIV infection in general.
Second, online sampling may lead to biases in demographic characteristics and other risk factors,35,36 and although we tried to minimise this by using different survey delivery methods (online and centre-based), the sample sizes obtained in the different sub-groups of the centre-based questionnaire are too small to detect significant differences. Therefore, selection bias cannot be ruled out.
Many highly educated MSM respondents are more likely to use novel technologies for PN than those who have a lower educational level and less access to mobile applications or online partner referral. Therefore, because those recruited through the Internet may not be representative of all MSMs, the generalizability of the results is questionable.
Thirdly, the use of multiple-choice questions makes results difficult to interpret, thus limiting multivariate analysis and weakening the robustness of the analysis.
Finally, although unlikely, respondents may have participated more than once, as it was impossible to identify duplication directly on the web page or resulting from respondents completing both the centre-based questionnaire and the online questionnaire.
ConclusionsThis is one of the first surveys to analyse the intention to use new communication technologies for PN among MSM in Spain.
Our data reveal differences depending on the source of information (online or centre) and type of partner (stable or casual). Patients attending an STI clinic tend to notify more frequently and to prefer personal approaches, and MSM are more likely to notify to their stable partners than their casual ones. Nevertheless, half of the respondents are open to new technologies (Internet, SMS, mobile phone apps) to notify their casual partners, indicating that this approach should be promoted among MSM and health professionals.
Fighting stigma and promoting alternative methods of PN through new technologies could increase the frequency of PN. Such an approach will improve early detection and reduce transmission of STIs/HIV in Spain.
- -
Among men who have sex with men, using the Internet to find sexual partners has been associated with an increased risk of syphilis.
- -
Partner notification could reduce the chain of transmission and strengthen preventive attitudes.
- -
New communication technologies can help to trace partners who cannot be contacted otherwise.
- -
Intention to use new technologies for partner notification of sexually transmitted infections depends on the type of partnership; patients in casual partnerships are more likely to use these technologies
- -
General practitioners, sexually transmitted infections units, and community-based centres are best positioned to promote the use of new technologies for partner notification among MSM.
- -
A web page with a partner notification service should provide clinical information, information on the prevention of sexually transmitted infections, and a list of health centres the receiver of the notification could attend.
Pere Godoy.
Author contributionsConceived and designed the study: DCP, MJB, PFD, PGO, RM, CJA and JC
Performed the study: DCP, MJB, PFD, PGO, RM, CJA, MPS, MGE, and EAM
Analysed the data: DCP
Wrote the manuscript: DCP and all the authors contributed with comments to the manuscript.
FundingNo funding
Conflict of interestThere is no conflict of interest
We are grateful to Dolors Ramirez Tarruella, MD, MPH who conducted the initial literature search and participated in the preliminary part of the project by contributing to the focus group and to the design of the study questionnaires. This study was financed through public funds by the Public Health Agency of Catalonia (ASPCAT).












