




To transculturally adapt the Spanish version of Pregnancy Physical Activity Questionnaire (PPAQ) analyzing its psychometric properties.
MethodsThe PPAQ was transculturally adapted into Spanish. Test-retest reliability was evaluated in a subsample of 109 pregnant women. The validity was evaluated in a sample of 208 pregnant women who answered the questionnaire and wore the multi-sensor monitor for 7 valid days. The reliability (intraclass correlation coefficient), concordance (concordance correlation coefficient), correlation (Pearson correlation coefficient), agreement (Bland-Altman plots) and relative activity levels (Jonckheere-Terpstra test) between both administrations and methods were examined.
ResultsIntraclass correlation coefficients between both administrations were good for all categories except transportation. A low but significant correlation was found for total activity (light and above) whereas no correlation was found for other intensities between both methods. Relative activity levels analysis showed a significant linear trend for increased total activity between both methods.
ConclusionsSpanish version of PPAQ is a brief and easily interpretable questionnaire with good reliability and ability to rank individuals, and poor validity compared with multi-sensor monitor. The use of PPAQ provides information of pregnancy-specific activities in order to establish physical activity levels of pregnant women and adapt health promotion interventions.
Adaptar transculturalmente la versión española del Pregnancy Physical Activity Questionnaire (cuestionario de actividad física en el embarazo) analizando sus propiedades psicométricas.
MétodoEl cuestionario de actividad física en el embarazo fue transculturalmente adaptado al español. La fiabilidad test-retest se evaluó en una submuestra de 109 embarazadas. La validez se evaluó en una muestra de 208 embarazadas que respondieron el cuestionario y llevaron colocado el monitor multisensor durante 7 días válidos. Se valoraron la fiabilidad (coeficiente de correlación intraclase), la concordancia (coeficiente de correlación de concordancia), la correlación (coeficiente de correlación de Pearson), el grado de acuerdo (gráfico Bland-Altman) y los niveles de actividad relativos (test Jonckheere-Terpstra) entre las dos administraciones y los dos métodos.
ResultadosLos coeficientes de correlación intraclase entre las dos administraciones fueron buenos para todas las categorías, excepto el transporte. Una correlación baja, pero significativa, se encontró para la actividad total (suave y superior), mientras que no se encontró correlación para otras intensidades entre los dos métodos. El análisis de los niveles de actividad relativos mostró una tendencia lineal significativa para el incremento de actividad total entre ambos métodos.
ConclusionesLa versión española del cuestionario de actividad física en el embarazo es un breve y fácilmente interpretable cuestionario, con buena fiabilidad y habilidad para ordenar personas, y baja validez en comparación con el monitor multisensor. El uso del cuestionario de actividad física en el embarazo aporta información sobre actividades específicas del embarazo con el objetivo de establecer los niveles de actividad física de las mujeres embarazadas y adaptar intervenciones para la mejora de la salud.
Physical activity during pregnancy has potential health benefits in pregnant women, such as reduced risk of gestational diabetes mellitus and preeclampsia, and prevention of excessive weight gain and weight retention.1–3 Similarly, inactivity during pregnancy has been associated with adverse perinatal outcomes.4–6 Pregnant women with absence of medical or obstetrics complications, are advised to accumulate at least 30minutes of moderate intensity activity per day on most, if not all, days of the week.7
Valid and reliable methods to measure the duration, frequency and intensity of physical activity during pregnancy are needed to provide information in order to establish health promotion strategies that prevent excessive weight gain and improve pregnant women's health. Questionnaires are the most commonly used method in epidemiologic and large population studies because their inherent characteristics as easy administration, non-invasive and relatively inexpensive method. Several physical activity questionnaires have been developed and validated in adults. Most of them emphasize on moderate and vigorous intensity sports, and fail to include household or childcare activities, which comprise a substantial proportion of the time spend in physical activity during pregnancy.8 This may result in misclassification that limits the ability of questionnaires to estimate and differentiate physical activity levels among pregnant women.9
The Pregnancy Physical Activity Questionnaire (PPAQ)9 is a tool specifically designed and successfully validated for the assessment of physical activity levels among pregnant women. The PPAQ has been translated into different languages as Japanese,10 Vietnamese,11 French,12 Turkish,13 Portuguese14 and Chinese.15 In addition, these versions have been validated against pedometer,11,13 uniaxial accelerometer,9,10,15 and biaxial accelerometer.12 Studies validating this devices and establishing specific cut points have not been developed for pregnant women.12,16 Inherent limitations were found in these devices, such as the limited use for monitoring intensity of activity, impossibility of detect the upper body movements due to its placement, low compliance17 and uncomfortable location for pregnant women.18 Although a new multi-sensor monitor that overcomes these limitations has been validated on pregnant women,18 none of the standardized physical activity questionnaire has been validated against this monitor in this population.
Despite the large amount of Spanish-speaking people in the world, to our knowledge there is currently no validated Spanish version of the PPAQ (PPAQ-S), which takes into account the cultural differences of Spanish-speaking pregnant women. Consequently, the aim of this study was to transculturally adapt the PPAQ-S analyzing its psychometric properties.
MethodsParticipantsWe recruited healthy pregnant women, 18-45 years old at the first prenatal care visit from health clinics of the Sanitary Area of Seville (Spain). The exclusion criteria included physical illnesses or disabilities that affect normal daily routine and high risk pregnancy (i.e., diabetes or hypertension). We obtain written informed consent of participants prior to enrolling in the study and after receiving detailing information about the study aims and protocol. A previous sample of 16 pregnant women was used for the transcultural adaptation process. A total sample of 260 and a subsample of 120 eligible women were used to analyze validity and test-retest reliability, respectively, but pregnant women with incomplete protocol were excluded. Finally, 208 and 109 pregnant women were included in the validity and reliability analysis, respectively.
Study protocolThe study protocol obtained ethical approval from the Medical Research Ethics Committee of the University Hospital Virgen del Rocío (Seville, Spain) according to the Declaration of Helsinki. The study protocol was performed in two stages: the transcultural translation process of the PPAQ from English to Spanish, and the analysis of reliability and validity of the PPAQ-S.
Transcultural adaptation processAs prescribed the scientific literature,19 the adaptation process for the PPAQ used the direct and reverse translation (forward-backward translation). Figure I of online Appendix showed the steps followed in this process. Subsequently, individual interviews were conducted for the pregnant women to evaluate their understanding, comprehensibility and feasibility of the questionnaire (cognitive debriefing), as described by previous studies.20
Reliability and validityTwo face-to-face sessions, separated by an interval of 8 days was performed to complete the reliability and validity process. At the first session, sociodemographic and anthropometrical characteristics, weight and height, were evaluated following the standard procedures with calibrated digital scale (Tanita Corporation BC-420, Tokyo, Japan) and a stadiometer (Seca-780, Hamburg, Germany). Body mass index (BMI) (kg/m2) was calculated. In addition, pre-pregnancy BMI was calculated using the weight and height measured by sanitary professionals at the first prenatal care visit. In this session pregnant women completed the first PPAQ-S and a multi-sensor monitor was placed on the left arm of each participant who was asked not to change their habitual lifestyle. At the second session, the second PPAQ-S was completed and the monitor was removed.
InstrumentsThe PPAQ9 is a semiquantitative questionnaire which reports the time spending in 32 activities categorized in five types of activity. Respondents are asked to select the category which best approximates the amount of time spent in each activity per day or week during the current trimester. The number of hours spent in each activity was multiplied by the activity intensity to arrive at average daily energy expenditure (MET-hours/day) attributable to each activity. This tool used specific metabolic equivalents (METs) values for pregnant women when is possible as previously established.9 Activities were categorized by intensity, type or as total activity.
A multi-sensor monitor, Sensewear Mini Armband (SWA; BodyMedia Inc., Pittsburgh, USA) was used to assess physical activity and energy expenditure. This monitor provides more accurate estimation of energy expenditure than accelerometry-based devices21 and have shown a well correlation with indirect calorimetry measured on pregnant women.18 The SWA includes sensors to measure energy expenditure by monitoring the heat flow from the body, skin temperature, galvanic skin response and 3-axis accelerometer for motion detector. Data were downloaded using Sensewear professional software version 8.1, and were exported as METs data minute-to-minute into excel, where we calculated the METs·h/week. The monitor was worn for eight completed days, except during water-based activities, including five week days and two weekend days completed. It must have been carried over more than 95% of the whole day (1368min) for consider a completed day. Data of swimming were substituted for a constant MET value according to the Compendium of Ainsworth as explained by previous research.22 To avoid any kind of immediate reactivity, we removed from the analysis the first completed day monitored.
Statistical analysisTest-retest reliability was studied calculating two-way mixed average intraclass correlation coefficient (ICC) with 95% confident interval. Estimated means and differences between the measurements, the standard deviations of the differences, the intraindividual standard deviation,23 and the standard error of measurement24 was studied. The agreement between test and retest was assessed using Bland-Altman plots, including the 95% levels of agreement.23
To assess the validity of the PPAQ-S we followed the Edinburgh Framework25 and the COSMIN checklist.26 Estimated means of subjective (PPAQ) and objective (SWA) measures were calculated for the time spent in each intensity categories. The systematic differences between both measures were calculated by means of paired t-test. The concordance between the objective and subjective measures was studied with concordance correlation coefficient.27 The Pearson correlation coefficient was used as additional information for the concordance correlation coefficient, and to compare with previous validity studies for the PPAQ.
Bland-Altman plots were calculated as previously explained. The association between the difference and the magnitude of the measurement (i.e., heterocedasticity) was examined by regression analysis. Receiver operating characteristic curve was constructed to determine the areas under the curve and 95% confidence intervals, specificity and sensitivity of the PPAQ as predictor of the fulfillment of minimum physical activity recommendations of ≥150min/week in bouts of ≥10min28 or 600 METsmin/week.29 To assess relative activity levels, we used the Jonckheere-Terpstra test to evaluate whether the tertile groups of the PPAQ-S total time ranked activity from the objective measurement in an anticipated graded order.
We used parametric statistics because of the large sample size; however, some of the study variables were non-normally distributed. We repeated the analysis using a nonparametric statistics, and the result did not substantially change. Date were analyzed using SPSS package version 20.0 for windows (IBM Corporation) with statistical significance set at p <0.05.
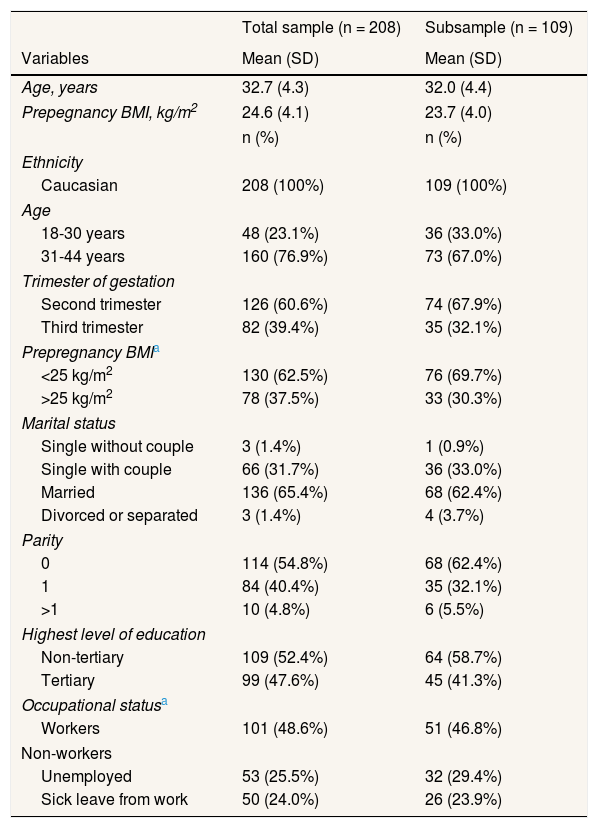
ResultsStudy populationThe transcultural adaptation process was developed in a sample of 16 pregnant women, with ages from 21 to 37 years old, gestational age between 9 and 35 weeks, and educational levels from no schooling to university. Sociodemographic characteristic of sample and subsample used in the validity and reliability analysis, respectively, are shown in Table 1. The main intensity and type of physical activity reported using the PPAQ-S were light intensity and household and caregiving activities, 57% and 52% of total activity respectively.
Socioemographic characteristics.
| Total sample (n = 208) | Subsample (n = 109) | |
|---|---|---|
| Variables | Mean (SD) | Mean (SD) |
| Age, years | 32.7 (4.3) | 32.0 (4.4) |
| Prepegnancy BMI, kg/m2 | 24.6 (4.1) | 23.7 (4.0) |
| n (%) | n (%) | |
| Ethnicity | ||
| Caucasian | 208 (100%) | 109 (100%) |
| Age | ||
| 18-30 years | 48 (23.1%) | 36 (33.0%) |
| 31-44 years | 160 (76.9%) | 73 (67.0%) |
| Trimester of gestation | ||
| Second trimester | 126 (60.6%) | 74 (67.9%) |
| Third trimester | 82 (39.4%) | 35 (32.1%) |
| Prepregnancy BMIa | ||
| <25 kg/m2 | 130 (62.5%) | 76 (69.7%) |
| >25 kg/m2 | 78 (37.5%) | 33 (30.3%) |
| Marital status | ||
| Single without couple | 3 (1.4%) | 1 (0.9%) |
| Single with couple | 66 (31.7%) | 36 (33.0%) |
| Married | 136 (65.4%) | 68 (62.4%) |
| Divorced or separated | 3 (1.4%) | 4 (3.7%) |
| Parity | ||
| 0 | 114 (54.8%) | 68 (62.4%) |
| 1 | 84 (40.4%) | 35 (32.1%) |
| >1 | 10 (4.8%) | 6 (5.5%) |
| Highest level of education | ||
| Non-tertiary | 109 (52.4%) | 64 (58.7%) |
| Tertiary | 99 (47.6%) | 45 (41.3%) |
| Occupational statusa | ||
| Workers | 101 (48.6%) | 51 (46.8%) |
| Non-workers | ||
| Unemployed | 53 (25.5%) | 32 (29.4%) |
| Sick leave from work | 50 (24.0%) | 26 (23.9%) |
During the process of the forward and backward translation, the range of difficulty perceived by translators varied between 1 and 6, whereas the conceptual equivalence varied between 7 and 10. Items that presented the greatest difficulty and/or the least conceptual equivalence are shown in Table I of online Appendix, and were discussed during the first and second consensus meeting. Individual interviews were conducted for 16 pregnant women, to analyze the cognitive debriefing of questionnaire. Table II of online Appendix shows the complete process of transcultural adaptation for the four items discussed. Regarding the acceptance and formality of the PPAQ-S, all pregnant women found the format comfortable and considered their comprehension sufficient to suggest changes in specific items of the questionnaire.
Operational qualitiesThe mean time required to complete the PPAQ-S was 8 ± 4min per patient (ranged 3 to 20). None of patients needed external help to complete the questionnaire.
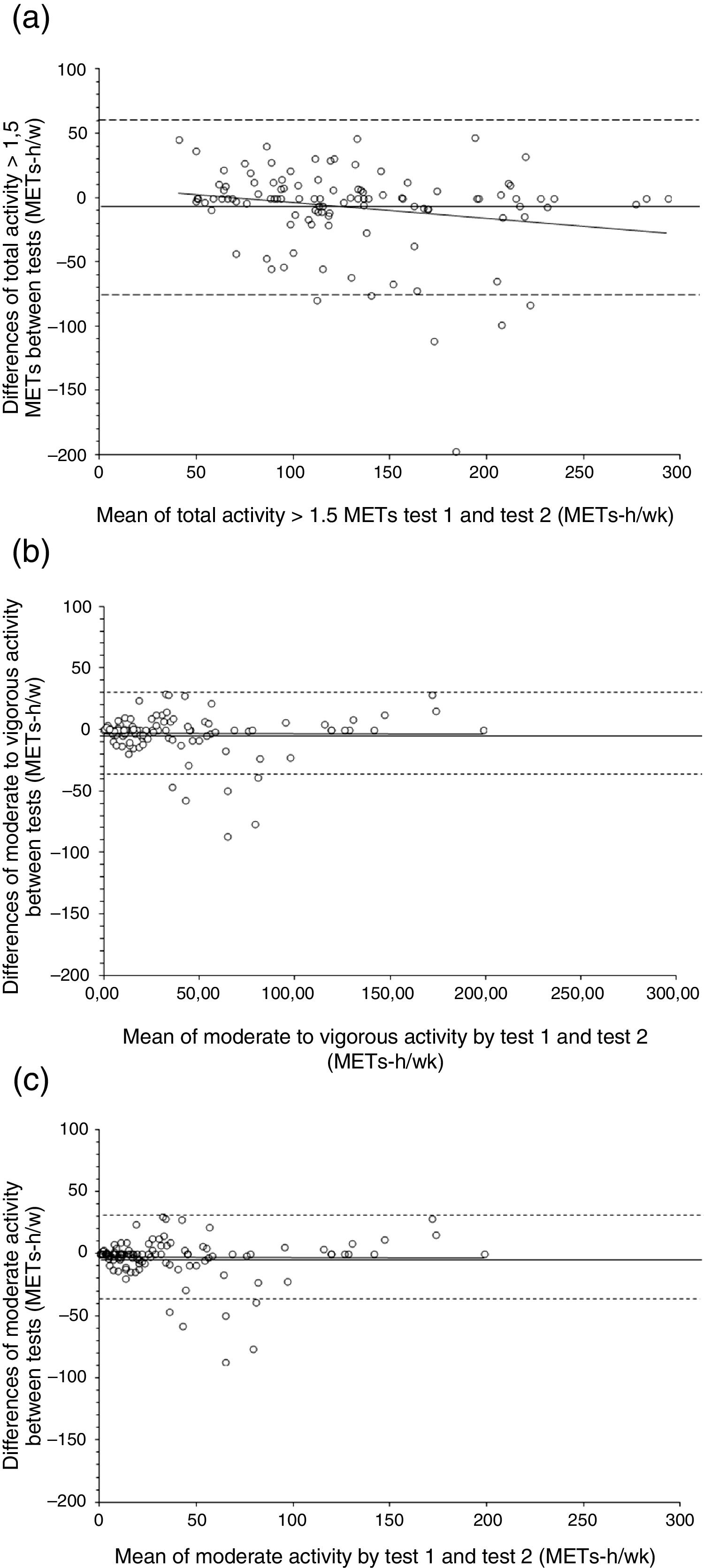
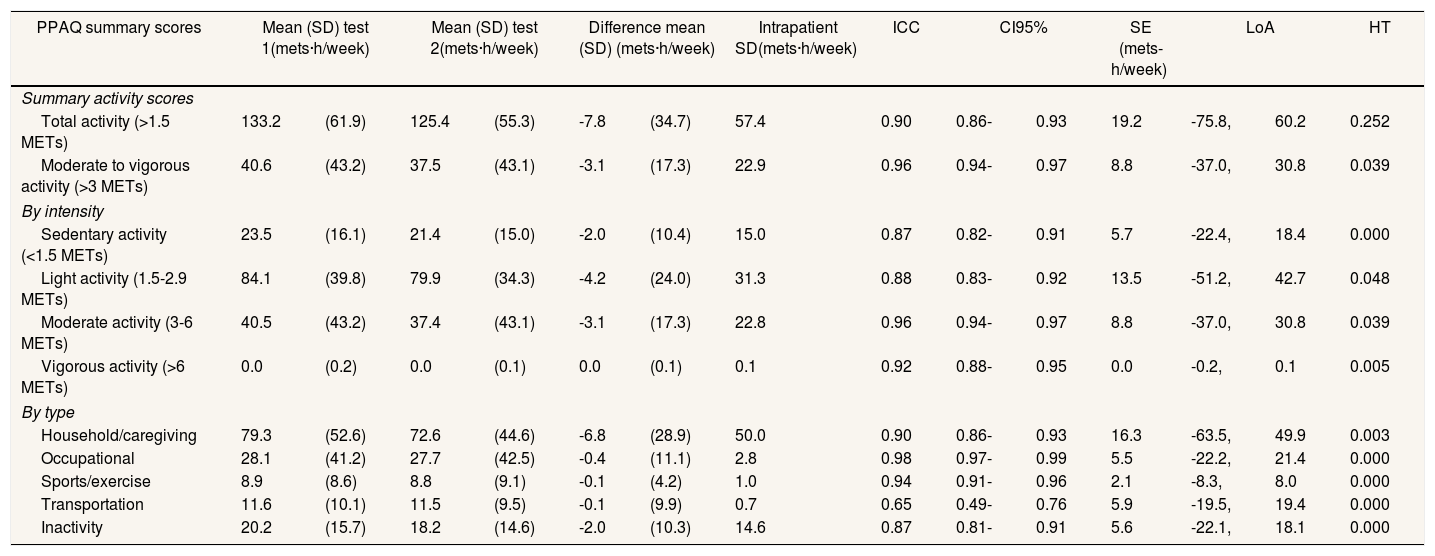
Test-retest reliabilityResults of test-retest reliability for the PPAQ-S scores are presented in Table 2. ICC were good for both total activity scores (ICC: 0.90 and 0.96), all intensity categories (ICC: 0.87-0.92) and all type of activities (ICC: 0.87-0.98); except transportation domain which was moderate (ICC: 0.65). Mean differences between test and retest did not differ substantially from zero and were lower than the standard error of the mean. Standard error of measurement for all PPAQ-S summaries varied from 0.0 to 19.2 METsh/week. Bland-Altman plots and the limits of agreement for total activity (−75.8, 60.2), moderate to vigorous activity and moderate activity (−37.0, 30.8 for both) were shown in Figure 1. There was a significant association between the difference and the magnitude of the test-retest PPAQ-S scores for all summaries (β from 0.190 to 0.487), except for total activity summary which was not significant.
Test-retest reliability of the PPAQ-S scores in pregnant women (n = 109).
| PPAQ summary scores | Mean (SD) test 1(mets·h/week) | Mean (SD) test 2(mets·h/week) | Difference mean (SD) (mets·h/week) | Intrapatient SD(mets·h/week) | ICC | CI95% | SE (mets-h/week) | LoA | HT | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Summary activity scores | ||||||||||||||
| Total activity (>1.5 METs) | 133.2 | (61.9) | 125.4 | (55.3) | -7.8 | (34.7) | 57.4 | 0.90 | 0.86- | 0.93 | 19.2 | -75.8, | 60.2 | 0.252 |
| Moderate to vigorous activity (>3 METs) | 40.6 | (43.2) | 37.5 | (43.1) | -3.1 | (17.3) | 22.9 | 0.96 | 0.94- | 0.97 | 8.8 | -37.0, | 30.8 | 0.039 |
| By intensity | ||||||||||||||
| Sedentary activity (<1.5 METs) | 23.5 | (16.1) | 21.4 | (15.0) | -2.0 | (10.4) | 15.0 | 0.87 | 0.82- | 0.91 | 5.7 | -22.4, | 18.4 | 0.000 |
| Light activity (1.5-2.9 METs) | 84.1 | (39.8) | 79.9 | (34.3) | -4.2 | (24.0) | 31.3 | 0.88 | 0.83- | 0.92 | 13.5 | -51.2, | 42.7 | 0.048 |
| Moderate activity (3-6 METs) | 40.5 | (43.2) | 37.4 | (43.1) | -3.1 | (17.3) | 22.8 | 0.96 | 0.94- | 0.97 | 8.8 | -37.0, | 30.8 | 0.039 |
| Vigorous activity (>6 METs) | 0.0 | (0.2) | 0.0 | (0.1) | 0.0 | (0.1) | 0.1 | 0.92 | 0.88- | 0.95 | 0.0 | -0.2, | 0.1 | 0.005 |
| By type | ||||||||||||||
| Household/caregiving | 79.3 | (52.6) | 72.6 | (44.6) | -6.8 | (28.9) | 50.0 | 0.90 | 0.86- | 0.93 | 16.3 | -63.5, | 49.9 | 0.003 |
| Occupational | 28.1 | (41.2) | 27.7 | (42.5) | -0.4 | (11.1) | 2.8 | 0.98 | 0.97- | 0.99 | 5.5 | -22.2, | 21.4 | 0.000 |
| Sports/exercise | 8.9 | (8.6) | 8.8 | (9.1) | -0.1 | (4.2) | 1.0 | 0.94 | 0.91- | 0.96 | 2.1 | -8.3, | 8.0 | 0.000 |
| Transportation | 11.6 | (10.1) | 11.5 | (9.5) | -0.1 | (9.9) | 0.7 | 0.65 | 0.49- | 0.76 | 5.9 | -19.5, | 19.4 | 0.000 |
| Inactivity | 20.2 | (15.7) | 18.2 | (14.6) | -2.0 | (10.3) | 14.6 | 0.87 | 0.81- | 0.91 | 5.6 | -22.1, | 18.1 | 0.000 |
CI95%: confidence interval of 95%; HT: heterocedasticity analysis; ICC: intraclass correlation coefficient; LoA: limits of agreement; SD: standard deviation; SE: standard error of the mean.

Bland and Altman plots of the differences between test 1 and test 2 for the Pregnancy Physical Activity Questionnaire scores. a) Total activity. b) Moderate to vigorous activity. c) Moderate activity. The means of the differences (solid lines) and limits of agreement (dashed lines) within ± 2 standard deviations are shown.
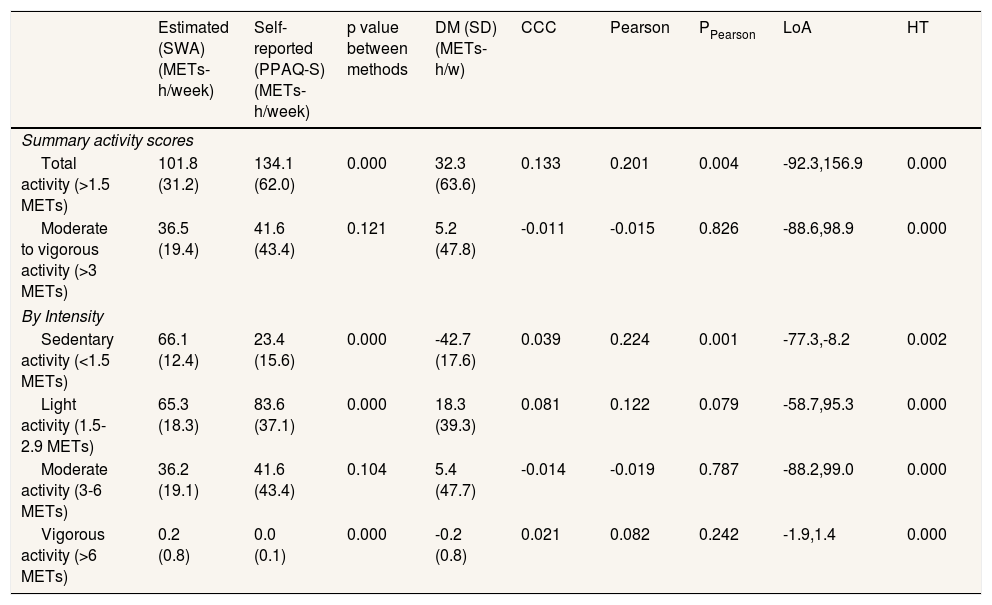
The PPAQ-S overestimated physical activity by 32% of total activity (32.3 METsh/week) and 14% of moderate to vigorous activity (5.1 METsh/week) compared with the SWA. The difference between both methods was significant for all intensity categories, except for moderate activity and moderate to vigorous activity (Table 3). However, assessing relative activity levels, we found a significant linear trend for increased total activity based on the SWA data across tertiles of activity based on the PPAQ-S scores (p = 0.005). A low but significant correlation was found for sedentary activity and total activity, whereas no significant correlation was found for other intensity categories. The concordance correlation coefficient value between the PPAQ-S and the SWA ranged from −0.011 to 0.133 for all summary categories. Attending to specific subgroups, the PPAQ-s presented significantly higher total activity compared with the SWA across all stratified subgroups, and significant differences between moderate to vigorous physical activity values were found on workers, non-workers, BMI ≥25kg/m2, second trimester and multiparous subgroups. The subgroup of young, BMI ≥25, second trimester, nulliparous and workers showed slightly stronger correlations in total activity between the PPAQ-S and the SWA measurements compared with their respective counterparts (Table III of online Appendix).
Comparison of intensity category values between SenseWear Armband and PPAQ-S in pregnant women (n = 208).
| Estimated (SWA) (METs-h/week) | Self-reported (PPAQ-S) (METs-h/week) | p value between methods | DM (SD) (METs-h/w) | CCC | Pearson | PPearson | LoA | HT | |
|---|---|---|---|---|---|---|---|---|---|
| Summary activity scores | |||||||||
| Total activity (>1.5 METs) | 101.8 (31.2) | 134.1 (62.0) | 0.000 | 32.3 (63.6) | 0.133 | 0.201 | 0.004 | -92.3,156.9 | 0.000 |
| Moderate to vigorous activity (>3 METs) | 36.5 (19.4) | 41.6 (43.4) | 0.121 | 5.2 (47.8) | -0.011 | -0.015 | 0.826 | -88.6,98.9 | 0.000 |
| By Intensity | |||||||||
| Sedentary activity (<1.5 METs) | 66.1 (12.4) | 23.4 (15.6) | 0.000 | -42.7 (17.6) | 0.039 | 0.224 | 0.001 | -77.3,-8.2 | 0.002 |
| Light activity (1.5-2.9 METs) | 65.3 (18.3) | 83.6 (37.1) | 0.000 | 18.3 (39.3) | 0.081 | 0.122 | 0.079 | -58.7,95.3 | 0.000 |
| Moderate activity (3-6 METs) | 36.2 (19.1) | 41.6 (43.4) | 0.104 | 5.4 (47.7) | -0.014 | -0.019 | 0.787 | -88.2,99.0 | 0.000 |
| Vigorous activity (>6 METs) | 0.2 (0.8) | 0.0 (0.1) | 0.000 | -0.2 (0.8) | 0.021 | 0.082 | 0.242 | -1.9,1.4 | 0.000 |
CCC: concordance correlation coefficient; DM: difference mean between methods; HT: heterocedasticity analysis; LoA: limits of agreement; Pearson: Pearson correlation coefficient; PPearson: p value for Pearson correlation coefficient; SD: standard deviation.
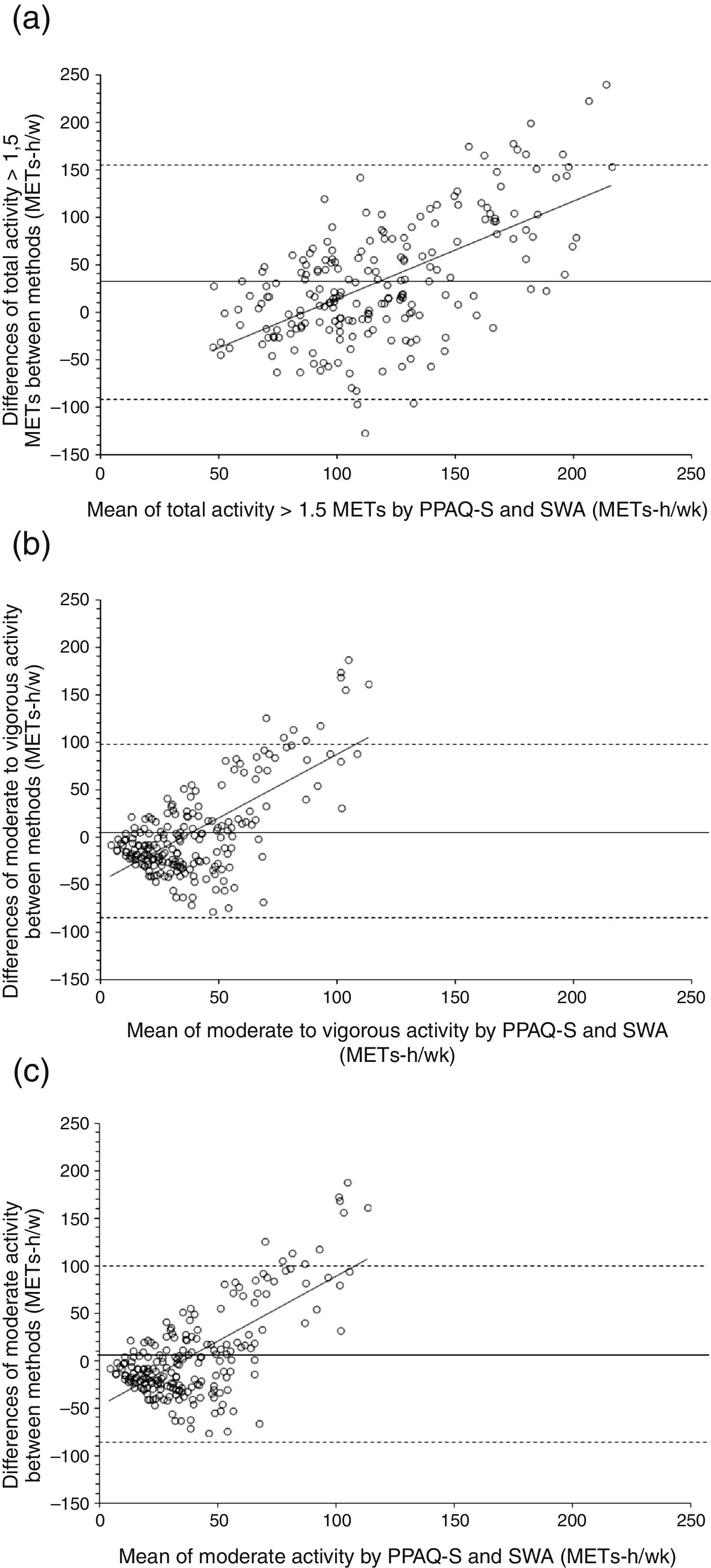
Figure 2 shows Bland-Altman plots and the limits of agreement for total (−92.3, 32.4), moderate to vigorous (−88.6, 5.2) and moderate (−88.2, 5.4) activity. There was a significant association between the difference and the magnitude of the PPAQ-S and the SWA measurements for all intensity categories (β from −0.211 to 0.981).

Bland and Altman plots of the differences between Pregnancy Physical Activity Questionnaire and Sensewear for (a) total activity, (b) moderate to vigorous activity, and (c) moderate activity. The means of the differences (solid lines) and limits of agreement (dashed lines) within ± 2 standard deviations are shown.
Receiver operating characteristic analysis identified the PPAQ-S as poor predictor of the proportion of women who meeting minimum physical activity recommendation of ≥150minutes of moderate to vigorous physical activity in bouts of 10minutes and ≥600 METsmin/week, showing a high sensitivity (81% and 78% true positive, respectively) but low specificity (29% and 20% true negative, respectively).
DiscussionThis study provides adequate transcultural adaptation, good reliability, good ability to rank physical activity levels of pregnant and poor validity analysis of the PPAQ-S, which is the first standardized physical activity questionnaire validated against a multi-sensor monitor in pregnant women.
In the transcultural adaptation process, no significant problems appeared throughout the translation into Spanish or the evaluation of the conceptual equivalence of the items. The ability of pregnant women to comprehend the questionnaire was good and the mean administration time of the questionnaire was similar to the original version, approximately 8 versus 10minutes.9
The median total activity reported was similar to Japanese version,10 lower than Turkish,13 and higher than original,9 Vietnamese11 and Chinese15 versions. The predominance of light intensity and household and caregiving activities found in our sample is in line with other PPAQ versions,9–11,13, and can be explained by the selection of less demanding activities30 during pregnancy for compensate the increase of basal energy expenditure31 and because approximately half of our sample were un-employed or sick from work and multiparous, prevailing household and caregiving activities in their daily life.
Our reliability results for total activity were higher than original version9, and similar with other versions,10,11 explained by the similar period of time between both applications. The difference with original version may be due to the mailed administration used for the second administration in the original version. Bland-Altman plots and heterocedasticity analysis revealed that for total activity summary when the amount of activity reported by the PPAQ-S was higher, the differences between test-retest scores did not increase, suggesting that this summary may be repeatable irrespective of the amount of activity reported. Focus on intensity categories, the reliability results were slightly greater for moderate activity than other intensity categories, consistent with other PPAQ versions.9,11–13. Focus on type of activity categories, in line with others PPAQ versions, the reliability results were good for all types of activity,10–13 except transportation.10,12 This may reflect a true variability on this activity and could be explained because pregnancy implies structured medical visits that may change this behavior in the daily life of pregnant women. Nevertheless household and caregiving, and occupational activities could be more routine activities.
In line with previous study,16 the PPAQ-S overestimated physical activity levels for all intensity categories compared with the SWA, except for sedentary and vigorous activities. The validity results showed only significant relationship for total and sedentary activities, and Bland Altman plots and heterocedasticity analysis for total and moderate to vigorous activity indicated that just as the amount of physical activity reported was higher the differences between methods increase. This overestimation of physical activity shows the difficulty of pregnant women to discriminate the intensity or the duration of their activities, and could be explain by the increase of weight and basal energy expenditure31 and the difficulties on movement32 inherent to pregnancy that could make pregnant women to perceive these difficulties with a higher duration or effort level. Receiver operational characteristic analysis revealed a poor prediction of fulfillment of physical activity recommendations, showing a high sensitivity and low specificity, leading to consider this instrument a bad discriminator of people who reach the physical activity recommendations, but a good instrument to detect moderate to vigorous physical activity. However, the significant linear trend showed on relative activity levels assessment suggests the ability of the PPAQ-S to discriminate activity levels, reflecting the true ranking of physical activity, and allowing to examine associations between physical activity levels and health variables during pregnancy.9,10,15 The use of both objective and subjective measures of physical activity should be used simultaneously in future studies in order to adequate capture physical activity during pregnancy.
This study presents several limitations, such as the exclusion of high risk pregnant women and the recruitment only of pregnant women who meet eligibility criteria and voluntarily participated. The percentages of young, overweight/obese, and third trimester women were considerably lower than their counterparts so it may result in self-selection bias. In contrast parity, educational level and occupational status subgroups had a similar percentage. The cross-sectional design of our study precludes the identification of any casual relations. Longitudinal studies are needed to examine the sensitivity to change of this questionnaire after interventions. The know limitation of nonprobability samples, including their less representativeness and unknown levels of sampling error, are further limitations.
The strengths of this study were the systematic and rigorous process of the transcultural adaptation, the strict standardization of methodology, and the use, for first time, of 24hours multi-sensor monitor to validate the PPAQ, which may solve the main limitations of accelerometers and pedometers, used in previous validation studies. Moreover, the use of the same units (METs·h/week) for both methods, allow the direct comparison without needing to establish cut points to estimate the intensities.33 In addition, the use of specific METs values for pregnant women by the PPAQ and the quantification of energy expenditure by the Sensewear may appropriately account for the physiological and cardiovascular changes that occur during pregnancy. Other strength of this study is the strict quantification period used. Although between 3 to 5 days of monitoring are sufficient to estimate habitual physical activity,22 we used a period of at least eight completed days (upper than 95% of the day), eliminating the first and the last day to minimize the reactivity of wore the Sensewear Armband and to capture an habitual week of lifestyle of pregnant women.
Since self-reported instruments facilitate the study of physical activity patterns on clinical practices, epidemiologic and large population studies, future research should considerer the comparison of the psychometric properties of different questionnaires against multi-sensor devices on pregnant women to know the most adequate self-report measure of physical activity during pregnancy.
ConclusionsThe results obtained in the present study indicated that the PPAQ-S is a brief and easy to interpret questionnaire with a good reliability and ability to rank pregnant women respect to their physical activity, and a poor validity compared against multi-sensor monitor. The availability of validated versions of the original questionnaire into different languages allows the use of this questionnaire in cross-national clinical trials.
We recommend the usefulness of this instrument to discriminate physical activity levels among pregnant women, providing pregnancy-specific activities information in order to predict maternal and fetal health outcomes and to propose health promotion strategies during pregnancy.
PPAQ is a specifically designed questionnaire for pregnant women that overcomes the limitation of questionnaires designed for adults, taking into account household and childcare activities and not only moderate and vigorous sports. PPAQ have not been transculturally adapt into Spanish.
What does this study add to the literature?This study provides the Spanish version of PPAQ and establishes the first validation of standardized physical activity questionnaire in pregnant women using a multi-sensor monitor, which overcomes the limitations of accelerometers. The Spanish version of PPAQ, which includes specific cultural adaptation, is required to develop research studies among Spanish-speaker pregnant women.
Mercedes Carrasco Portiño.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsD. Munguía-Izquierdo and M.A. Oviedo-Caro designed the study and planned the data collection. All authors were responsible for the acquisition of the data. M.A. Oviedo-Caro and D. Munguía-Izquierdo performed the statistical analyses and wrote the manuscript. All authors provided critical review of the manuscript and approved the final version.
FundingThe study was funded by Research Group CTS-948 of University Pablo of Olavide (Seville), this funding included material and equipment for the research. There was no external financial support. J.B. is supported by the Spanish Ministry of Education (grant number FPU13/05130).
Conflicts of interestsNone.
The authors gratefully acknowledge all women for their collaboration. We also acknowledge the health clinic members involved in the recruitment for their effort and great enthusiasm.












