





Until 2016, around 3 million persons had limited access to health care in Greece due to the economic crisis. We describe a massive solidarity movement of community clinics and pharmacies in Greece.
MethodWe conducted a survey in 2014-15 and describe the characteristics of community clinics and pharmacies spontaneously established all over Greece after 2008.
ResultsA characteristic of the 92 active solidarity clinics is autonomous collective functioning, free services, and funding from non-governmental sources. The largest clinics examined more than 500 uninsured or partly insured patients per month. Clinics covered a wide range of clinical and preventive services. Funding, availability of drugs, vaccines, medical material and their legal status were the main problems identified. The solidarity movement involved thousands of health professionals covering essential population needs.
ConclusionsThe community outpatient clinics were an outstanding example of solidarity and temporarily alleviated the health needs of a large part of the population.
Hasta 2016, alrededor de 3 millones de personas tenían acceso limitado a la atención médica en Grecia debido a la crisis económica. Describimos un movimiento masivo de solidaridad de clínicas comunitarias y farmacias en Grecia.
MétodosRealizamos una encuesta en 2014-15 y describimos las características de las clínicas comunitarias y de las farmacias espontáneamente establecidas en toda Grecia después de 2008.
ResultadosUna característica de las 92 clínicas solidarias activas es el funcionamiento colectivo autónomo, con servicios gratuitos y financiación de fuentes no gubernamentales. Las clínicas más grandes examinaron más de 500 pacientes no asegurados o parcialmente asegurados por mes. Las clínicas cubrieron una amplia gama de servicios clínicos y preventivos. La financiación, la disponibilidad de medicamentos, vacunas y material médico, y su estado legal, son los principales problemas identificados. El movimiento de solidaridad involucró a miles de profesionales de la salud que cubrieron las necesidades esenciales de la población.
ConclusionesLas clínicas ambulatorias comunitarias fueron un ejemplo de solidaridad y aliviaron temporalmente las necesidades de salud de una gran parte de la población.
The economic crisis in Greece started around 2008 and resulted in a 25% reduction of the GDP, a massive increase in unemployment particularly in young ages and an increase in migration outflows, including biomedical personnel.1–4 Around 3 million persons were uninsured in a population of 11 million until 2016.1,4,5 A new law at 2016 provided access to health care to all uninsured persons living in Greece.
The Greek healthcare and social security systems are semi-public/semi-private and have been chronically malfunctioning.6 Following the crisis, the funding of public hospitals and the number of health professionals in the public sector decreased while shortages of drugs and medical material are reported, including childhood vaccines. About 30% of the population (long term unemployed, new generations entering the labour force) and more than 700,000 undocumented migrants were excluded from the health and social security system. The uninsured were covered by the national health system only for emergencies. The acute effects of the austerity measures on the access to healthcare and the health of the population include increases in child poverty and under-nutrition, HIV infections among drug users, stillbirths and suicides.5
At international level and at periods of crisis, grass roots social solidarity movements are common in many societies. These movements cover the basic needs of different population groups, for example the provision of food and clothing for the poor and homeless, medications and vaccines for the uninsured or selling of agricultural products directly by the producers to the public. The alarming malfunctioning of the health system in Greece after the crisis resulted in the spontaneous development of a large solidarity movement among healthcare personnel in the form of outpatient health clinics to provide free services and medications to wide sectors of the population with limited access to healthcare.7 In this article we describe the functioning and organization of these outpatient solidarity clinics and pharmacies (in Greek, KIΦA, from Kοινωνικά Iατρɛία Φαρμακɛία Aλληλɛγγύηζ).
MethodsIn December 2014 we identified 137 solidarity clinics through internet searches and personal contacts. Of those, 92 identified themselves as solidarity clinics, were operational in 2014, provided medical services, were not directly connected and funded by state owned organizations or big NGOs and had an email address available.
We abstracted in a structured template publicly available information using solidarity clinics’ websites or other on-line publications, e.g., Facebook pages (see Table I in Online Appendix A). We developed a structured questionnaire that included information on the operation and services of the clinics and invited all 92 clinics to participate (see Online Appendix B). We collected data from December 2014 to February 2015. After several contacts and follow up emails and telephones we received responses from 19 (21%) clinics, including the three major solidarity clinics in Athens (Mitropolitiko), Thessaloniki and Heraklion. We entered data in Epidata v.3.1. and performed descriptive analysis of the solidarity clinics’ responses using STATA 12 software (StataCorp, Texas, USA).
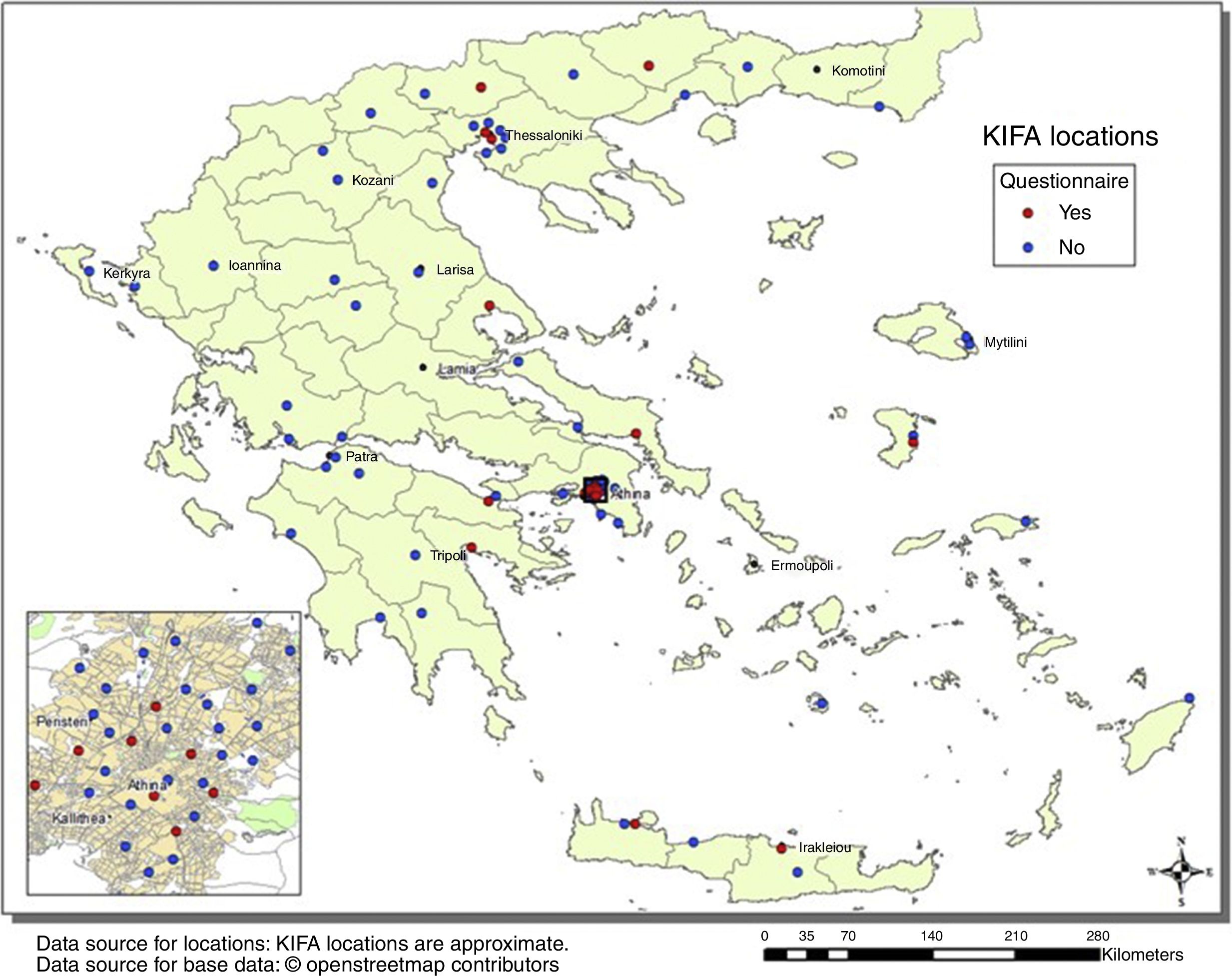
ResultsThe 92 solidarity clinics are distributed throughout Greece (Fig. 1) following approximately the population density with more than 50% located in Athens and Thessaloniki (Table 1). Among the 92 solidarity clinics, many are citizens’ initiatives (43%), operate with volunteers and the support of the wider community and function outside the national health system, 33% are initiatives of the municipality, 12% of the church and 8% of the medical associations (Table 1). The majority formed after 2010 with a peak in 2012-2013.
![Solidarity clinics in Greece (n = 92). The map includes all reported functioning solidarity clinics in 2014 irrespective of size. In red the 19 solidarity clinics responding to the questionnaire. (KIFA [KIΦA]: acronym in Greek for Kοινωνικά Iατρɛία Φαρμακɛία Aλληλɛγγύηζ.).](https://static.elsevier.es/multimedia/02139111/0000003300000003/v3_201905030657/S021391111830013X/v3_201905030657/en/main.assets/gr1.jpeg?xkr=p4rfv/yGgUzP1q5IvG4zJ4SjawujJuC4cSkUtr3nFWDIe63MoirZj0eK472jDLSpUWqOjGHzQGlDiQZy2uDoqYJBgR4RjO+gAKcXSlsoVK+EebO8q/QBG/8O4GY/Dxg5EZUEmrTy/4xcVJ4NUoDEulpJm+vU7/PbmimRQ9FPphpzRPGuAoKW+HLc7bBWOny41Z4295RplKO8FW3x66RRjKRTpszDgL/oOILLKvVHvVwFmn1CGPiFe2kxA6yim0yu60fs4MiJtwcysUMua9fNNHUkvEdeOT9FVXLcHjm17YY=)
Main characteristics of the 92 functioning solidarity outpatient clinics, Greece, 2014.
| Number of clinics with information | n | % | |
|---|---|---|---|
| Region | |||
| Athens metropolitan area | 92 | 38 | 41 |
| Macedonia (including Thessaloniki) | 92 | 17 | 18 |
| Peloponnese | 92 | 10 | 11 |
| Aegean Islands | 92 | 7 | 8 |
| Central Greece | 92 | 6 | 7 |
| Crete | 92 | 5 | 5 |
| Thessaly | 92 | 4 | 4 |
| Thrace-Epirus-Ionian Islands | 92 | 5 | 5 |
| Start year of operation | |||
| <2008 | 84 | 3 | 3.3 |
| 2008-2011 | 84 | 11 | 12 |
| 2012-2014 | 84 | 72 | 76 |
| Main entity organizing | |||
| Citizens’ group | 90 | 39 | 43 |
| Municipality | 90 | 30 | 33 |
| Church | 90 | 11 | 12 |
| Medical Association | 90 | 7 | 8 |
| Other | 90 | 3 | 3 |
| Legal frame | |||
| Public entity: municipality, medical association, church | 63 | 33 | 52 |
| Private entity: citizen association | 63 | 20 | 32 |
| Political party | 63 | 1 | 2 |
| None | 63 | 9 | 14 |
| Main services provided | |||
| Medical | 92 | 85 | 92 |
| Pharmacy | 91 | 80 | 88 |
| Days/week open | |||
| 1 to 2 | 73 | 19 | 26 |
| 3 to 4 | 73 | 13 | 18 |
| 5 or more | 73 | 41 | 56 |
| Hours/day open | |||
| 1 to 2 | 70 | 27 | 39 |
| 3 to 4 | 70 | 16 | 23 |
| 5 or more | 70 | 27 | 39 |
| Beneficiaries and documentation | |||
| Uninsured/unemployed | 86 | 86 | 100 |
| Requirement to present legal documents for services | 52 | 46 | 88 |
| Free services | 79 | 77 | 97 |
Although it is unknown how many solidarity clinics have a licence to practice as a medical practice/pharmacy, nearly all functioned under either a private (society, association of persons, non-profit organization/company, etc.) or a public legal framework (Municipal Corporation, Church, etc.) but 14% had no legal framework. Of 92 clinics, 92% and 88% provided free medical and pharmacy services respectively to uninsured or unemployed people (86; 100%) that had to present legal documentation for enrolment (46/52; 88%). Of 73 clinics, about half functioned 5 days per week and 39%, 5 or more hours daily. There is no central national coordination of the activities of the solidarity clinics although a nationwide meeting is held annually.8 Although the solidarity clinics are a social movement oriented to the supplementary provision of health care, their members are frequently politically active supporting anti-austerity policies, see for example the website of the “Mitropolotiko” KIFA in Athens9 and elsewhere (see Table I in Online Appendix A).
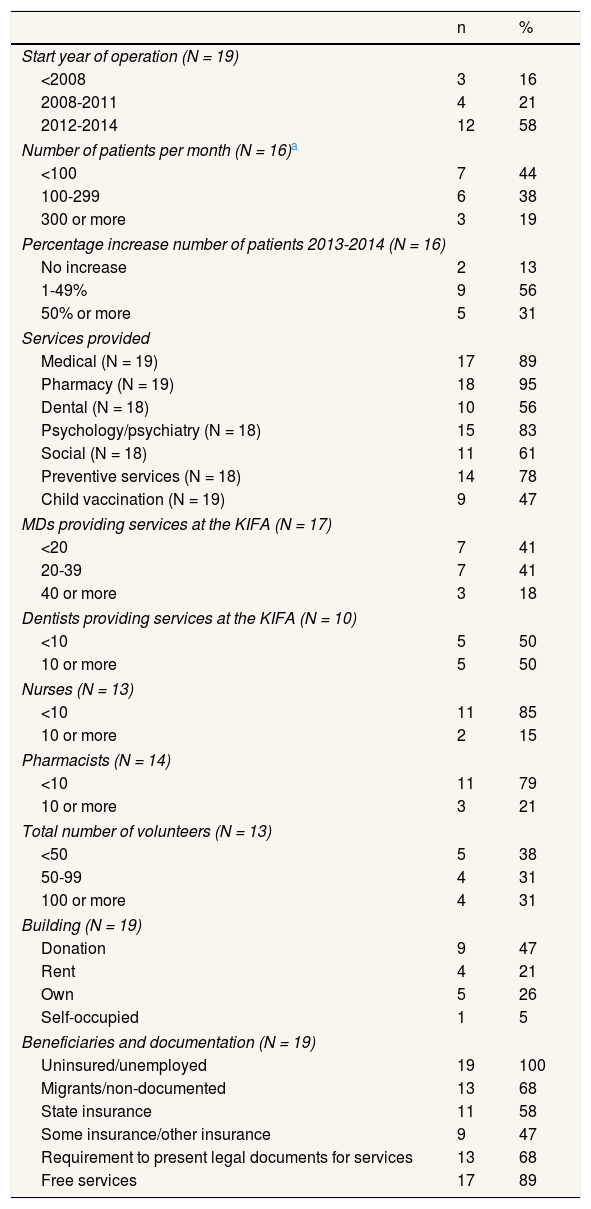
The 19 solidarity clinics responding to the questionnaire followed approximately the overall distribution of the clinics (Fig. 1) with 8 (42%) located in the metropolitan area of Athens, 4 (21%) in the area around Thessaloniki. Table 2 shows a description of their main characteristics. Among 19 clinics, the majority (n= 12) started their operation after 2012 and all reported collaborations with other entities (university, municipality, church, medical associations). In the clinics that identified themselves as ‘civilian groups’, decisions were taken by the general assembly that includes all volunteers. In the municipal solidarity clinics, decisions may be taken by the board of directors or the corresponding department. Each solidarity clinic has a basic or more elaborate administration that plans and organizes the activities.
Characteristics of 19 solidarity clinics included in the survey, Greece, 2013-2014.
| n | % | |
|---|---|---|
| Start year of operation (N = 19) | ||
| <2008 | 3 | 16 |
| 2008-2011 | 4 | 21 |
| 2012-2014 | 12 | 58 |
| Number of patients per month (N = 16)a | ||
| <100 | 7 | 44 |
| 100-299 | 6 | 38 |
| 300 or more | 3 | 19 |
| Percentage increase number of patients 2013-2014 (N = 16) | ||
| No increase | 2 | 13 |
| 1-49% | 9 | 56 |
| 50% or more | 5 | 31 |
| Services provided | ||
| Medical (N = 19) | 17 | 89 |
| Pharmacy (N = 19) | 18 | 95 |
| Dental (N = 18) | 10 | 56 |
| Psychology/psychiatry (N = 18) | 15 | 83 |
| Social (N = 18) | 11 | 61 |
| Preventive services (N = 18) | 14 | 78 |
| Child vaccination (N = 19) | 9 | 47 |
| MDs providing services at the KIFA (N = 17) | ||
| <20 | 7 | 41 |
| 20-39 | 7 | 41 |
| 40 or more | 3 | 18 |
| Dentists providing services at the KIFA (N = 10) | ||
| <10 | 5 | 50 |
| 10 or more | 5 | 50 |
| Nurses (N = 13) | ||
| <10 | 11 | 85 |
| 10 or more | 2 | 15 |
| Pharmacists (N = 14) | ||
| <10 | 11 | 79 |
| 10 or more | 3 | 21 |
| Total number of volunteers (N = 13) | ||
| <50 | 5 | 38 |
| 50-99 | 4 | 31 |
| 100 or more | 4 | 31 |
| Building (N = 19) | ||
| Donation | 9 | 47 |
| Rent | 4 | 21 |
| Own | 5 | 26 |
| Self-occupied | 1 | 5 |
| Beneficiaries and documentation (N = 19) | ||
| Uninsured/unemployed | 19 | 100 |
| Migrants/non-documented | 13 | 68 |
| State insurance | 11 | 58 |
| Some insurance/other insurance | 9 | 47 |
| Requirement to present legal documents for services | 13 | 68 |
| Free services | 17 | 89 |
Of 19 clinics, 17 (89%) offered medical services, 18 (95%) had a pharmacy, 15/18 (83%) offered mental health and 14/18 (78%) preventive services, while a lower proportion offered dental (10/18; 56%), child vaccination (9/19; 47%) and social services (11/18; 61%). Microbiological and imaging testing was free of charge and, mostly done in collaborative laboratories. Nearly all clinics (17/18) referred to hospitals patients needing secondary healthcare while 12 also referred to external private volunteer doctors. Ten clinics operated exclusively and seven partially using an appointment system.
All solidarity clinics worked with volunteer personnel while municipal solidarity clinics may have also used salaried staff (secretaries, nurses, etc.). The number of volunteers varied from 10 to 250 (median: 63) and similarly the number of physicians (range: 2-99, median: 23) that depended also on structure of the clinic and the number of external collaborating volunteer doctors (e.g. Heraklion: n = 61). The specialties covered the entire medical spectrum, with higher numbers of internists, general practitioners, paediatricians, cardiologists, gynaecologists, psychiatrists, orthopaedic surgeons and dermatologists. Fewer clinics had dentists (n = 10) and pharmacists (n = 13) while the number of nurses, midwives, physiotherapists and paramedical specialties was low. All solidarity clinics had a considerable number of administrative and logistic support from community members.
There are no valid estimates of the total number of patients examined overall because most clinics do not keep detailed statistics of patient attendance. The largest clinic in Athens examined around 1300 patients per month while the range in the other clinics was from 1 to 452 (median: 133/month). A mean of 243 additional visits per month were for prescription of chronic diseases medications in uninsured patients. Nearly all solidarity clinics reported a 10% or more increase in number of patients attending from 2013 to 2014. Around 10% of patients were children and 40% were women. The majority of patients were Greeks but statistics on ethnic origin are incomplete.
Of 19 solidarity clinics, 13 required some kind of documentation to evaluate the social security status, all accepted uninsured patients and 13 clinics accepted undocumented immigrants. Municipalities or solidarity citizens provided the physical space for most solidarity clinics, while four solidarity clinics rent the premises. Regarding funding, 12 clinics functioned through private donations and 11 organized different fundraising activities. Vaccines were mostly bought through own funds (7/12). Costs for most solidarity clinics were in the order of a few hundred Euros per month (mean: 580€; range: 40-2000€). These costs did not include personnel, and in most solidarity clinics they did not include payment of the building or functioning (electricity, water). Of 19 solidarity clinics, 7 reported funding problems, 10 faced difficulties in the supply of biomedical material and shortages of drugs and about half reported limited vaccine supply.
DiscussionFollowing the profound economic crisis in 2008 and the subsequent crisis of the health care system in Greece, a widespread social movement providing food, clothes, informal education and other much needed services was developed for the support of the growing impoverished and uninsured population, which by 2016 reached 3 million (27% of the Greek population).7 In response to the health system crisis, active citizens and grass roots movements organized primary health care clinics in the form of solidarity outpatient clinics providing preventive, chronic and emergency healthcare to, mostly, uninsured people. The clinics covered also health interventions that the state post-crisis was unable to cover such as repeat prescriptions and childhood vaccinations, although the child population is entitled to having them freely administered.10 In the absence of the solidarity clinics, and lacking funds for attending private practice, many patients would simply have no care or medication.
The genesis of this movement is connected to the reaction of the Greek society against the imposition of extreme austerity measures in a very short period that did not allow the state or the society to adapt. The solidarity clinics were therefore characterized as a social movement with a strong wider political character, although they were not formally connected to political parties or other institutions.
At least 92 solidarity clinics were operational in 2014 in Greece while 137 clinics were initially identified. The vast majority appeared after the 2008 financial crisis, were geographically widespread, following the population distribution, and operated with volunteer medical, paramedical and administrative personnel. Before the crisis, some big Greek NGOs (Médecins Sans Frontières, PRAKSIS, Médecins du Monde) provided primary care services to primarily to migrants and uninsured people in Athens and Thessaloniki. Some major municipalities were also operating ambulatory primary healthcare clinics,6 but due to budget cuts many had to either cease their operation, incorporate volunteer doctors in their schedule or collaborate with the church and/or medical associations and thus “transforming” into solidarity municipal clinics.
All major solidarity clinics responded to the survey, most after discussing the invitation in their general assemblies. The overall low response rate and the difficulties in contacting most clinics reflect the lack of a formal organization in most. This communal organization preserves their spontaneous and grass roots functioning and support by the community but may also complicate an efficient functioning.
The solidarity clinics provide primarily medical and pharmacy services while some also offer dental, mental health, preventive and social services. The biggest solidarity clinic in Athens does around 1300 consultations/month, while most clinics see more than 100 patients monthly. They are citizens’ initiatives or civil-public (municipality, church, medical association) collaborations and the majority operates under a legal framework (society, association, non-profit organization) however, it is unknown how many have a medical practice/pharmacy licence. The clinics are manned predominately by specialized physicians (general practitioners, internists, paediatricians) while nurses and other paramedical personnel is much less, following the chronic lack of these professional categories in the Greek health system. The funding and functioning of the solidarity clinics is a continuous serious consideration since they depend only on voluntary contributions. Similarly, consumables, medical material, drugs and vaccines are obtained mainly through private donations or they have to be bought, and many times are in shortage. The non-paid work by the volunteers cover a large part of what would have been the budget of a health care system.
The massive community outpatient clinics and pharmacies were an outstanding example of solidarity within a community that lost more than 25% of the GDP in a few years and that observed the dismantlement of the welfare state.1–5 This movement alleviated temporarily the health needs of a large part of the uninsured population of around 3 million. The solidarity clinics, however, could not be a long-term option for the provision of health care. The adaptation of the Greek welfare state to the new financial and social conditions was partially achieved by a new legislation in 201611,12 that provided access to all uninsured persons in the public system of Greece. The malfunctioning and underfunding, however, of the public system has resulted to the continuation of the functioning of the solidarity clinics even today that cover part of the care of the newly arrived refuge populations.
Editor in chargeCarlos Álvarez-Dardet.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
A massive solidarity movement of community clinics and pharmacies involving thousands of health specialists and other volunteers was spontaneously established all over Greece during the period of the economic crisis. There is very limited research on informal health care systems.
What does this study add to the literature?The study provides the first comprehensive description of the outpatients solidarity clinics in Greece and gives information on functioning, type of activities and patients examined. The solidarity outpatient clinics provided, temporarily, an alternative to the malfunctioning national health care system in Greece but could not be a long term option for the provision of health care.
I. Evlampidou: concept and design of the work, collection of data, statistical analysis and interpretation of results, writing and approval of final version. M. Kogevinas: concept and design of the work, interpretation of results, writing and approval of final version of the article.
FundingNone.
Conflicts of interestNone.
We would like to dedicate this article to our colleague and good friend Dr. Antonis Koutis, Medical School, Heraklion, Crete, who had commented on this article. Antonis had been one of the key promoters of the solidarity clinic in Heraklion; he passed away in September 2017. We would like to thank Prof. Takis Panagiotopoulos, National School of Public Health, Athens, Greece, for commenting on the design of the survey and on the manuscript; and Mrs. Antonia Valentin, ISGlobal, Barcelona, Spain, for the preparation of the figure; and also the numerous volunteers in the solidarity clinics who completed the questionnaires.













