



To estimate the association between socio-economic life course and body mass index (BMI), waist circumference (WC) and general and abdominal obesity in adults.
MethodsA cross-sectional analysis of a population-based cohort study of 1,222 adults (aged 22–63) from Florianopolis, southern Brazil. The socio-economic life course was analysed using the educational level of participants and their parents. Height, weight and WC were measured by specially trained staff. Linear and logistic regressions were used with adjustment for confounding factors, and data were stratified according to sex.
ResultsMean BMI and WC were about 2kg/m2 (95% CI: −3.3 to −0.7) and 6cm (95% CI: −9.7 to −2.9) lower in women with a high socio-economic position, while the association was reversed in men with a high socio-economic position, with WC being about 4cm higher (95% CI: 0.1 to 7.5). In addition, women who had always been in a high socio-economic position were less likely to have abdominal obesity (OR: 0.38; 95% CI: 0.20 to 0.76) while no such association was found in men.
ConclusionSocio-economic life course influences BMI, WC and obesity, with differences between males and females, thereby indicating that public policies that contemplate a socio-economic life course approach can be effective for controlling obesity.
Estimar la asociación entre trayectoria socioeconómica e índice de masa corporal (IMC), circunferencia de la cintura (CC) y obesidad general y abdominal en adultos.
MétodosAnálisis transversal de un estudio de cohortes de base poblacional en 1222 adultos (22-63 años de edad) en Florianópolis, sur de Brasil. La trayectoria socioeconómica fue analizada mediante el nivel educativo de los padres y los propios participantes. La medición de altura, peso y CC fue realizada por personal especialmente entrenado. Se usaron modelos de regresión lineal y logística ajustando factores confusores y estratificando por sexo.
ResultadosEl promedio de IMC y CC fue de 2kg/m2 (intervalo de confianza del [IC95%]: −3,3 a −0,7) y 6cm (IC95%: −9,7 a −2,9), menor en las mujeres con mejor posición socioeconómica. Dicha asociación fue la contraria en el caso de los hombres, en los que el promedio de CC fue 4cm mayor (IC95%: 0,1 a 7,5). Las mujeres que siempre permanecieron en mejor posición socioeconómica fueron menos propensas a tener obesidad abdominal (odds ratio: 0,38; IC95%: 0,20 a 0,76), mientras que en los hombres no se observó dicha asociación.
ConclusionesLa trayectoria socioeconómica se asocia al IMC, la CC y la obesidad, con diferencias entre sexos, indicando que la aplicación de políticas públicas que contemplen la trayectoria socioeconómica puede ser efectiva para el control de la obesidad.
Throughout the world, especially in low- and middle-income countries, the prevalence of obesity is increasing,1 and in 2014, Brazil was among the five countries with the highest overall percentage of obese people.2 Data from 2013 indicate that 16.8% of men and 24.4% of women in Brazil reach obesity measured by body mass index (BMI), and with an even higher prevalence when abdominal obesity is considered, which is present in 21.8% of the male and 52.1% of the female population.3
The literature indicates that the socio-economic position (SEP) at every stage of life–childhood, adolescence and adulthood–has an independent relationship with obesity.4 From a life course perspective, obesity is included among the health problems whose prevalence varies in different social groups throughout life, reflecting the cumulative exposure to deleterious factors at different ages. In this sense, having a low socio-economic status in childhood, adolescence and adulthood would also increase the likelihood of obesity, for example.5
However, the profile of the associations found in studies that analyzed the relation between life course and obesity differs according to the average income of the country whose population is being evaluated. In addition, most of the studies were conducted in high-income countries, especially the United States and European countries, while few were carried out in Brazil.6–11
Studies of the Brazilian population seem to converge on higher risk of obesity among men who have always been in the higher socio-economic strata and among women who have always been in the disadvantaged groups in terms of socio-economic status. However, different results were found according to the measure of adiposity used and the category of socio-economic life course analysed.6,8,11
From the perspective of life course, the effect of socio-economic aspects on obesity in adults in low- and middle-income countries, including Brazil, is still unclear. Several interventions and policies have been developed in order to prevent obesity at the population level, but the best way to act has not yet been proven,12,13 which indicates that a better understanding of the problem is necessary. Therefore, the objective of this research was to estimate the association between socio-economic life course with BMI measurements, waist circumference (WC) and general and abdominal obesity in adulthood.
MethodsThis study corresponds to a sectional sample analysis of individuals aged between 22 and 63 years who participated in the first follow-up population-based cohort EpiFloripa Adults. The baseline study was conducted in 2009 and included a representative sample of adults, ages 20 to 59, living in the urban zone of Florianopolis.
Florianopolis is the capital of the state of Santa Catarina (Southern Brazil), and has the third-highest human development index of all Brazilian municipalities (0.847). The population in 2010 was approximately 420,000 inhabitants in an area of 675 km2.14
Details of the sampling, study population and other methodological aspects of the study baseline can be found in another publication.15
Data from 2012 used in this research were collected through individual face-to-face interviews in the households of all individuals surveyed in 2009. Adults who refused to participate or could not be located for an appointment by the interviewers after at least four attempts by phone and four more home visits (at least one in the evening and another during the weekend) were considered losses/refusals.
The socio-economic life course was the exposure variable, measured by the education data of the cohort participants and their parents. The education of the participants was obtained in the collection in 2009 with the questions: “Did you go to school?” and “To what grade/year did you go to school?”. The education of fathers and mothers was obtained by applying two questions to the cohort members in 2012: “Did your father (mother) go to school?” and “To what grade/year did your father (mother) go to school?”. All information on education was noted as successfully completed years of study.
For the creation of the variable socio-economic life course, the age of the participant was considered, bearing in mind that the educational experience of the Brazilian population has undergone important changes in recent decades, with significant increase in schooling for more recent cohorts.
To create the socio-economic life course variable, initially, the variable education of the parents and of the participants themselves was categorized as: 1) education lower than or equal to the median, and 2) education higher than the median. Next, the socio-economic life course was defined: 1) “always low” when the educational level of both parents and participants was less than or equal to the median; 2) “decreasing” when the parents’ educational level was higher than the median and less than or equal to the median participants’; 3) “increasing” when the parents’ educational level was less than or equal to the median and the participants’ was higher than the median; and 4) “always high” when the educational level of the parents as well as the participants themselves was higher than the median. The educational level of both mother and father of the participants was used and included separately in the analyses.
The other economic and socio-demographic variables (sex, age and equivalized income) were employed to adjust the analysis and were also collected through a questionnaire applied to the participants. The sex of each participant was categorized as female or male; income and total household members were reported by the participant, with the equivalized family income16 calculated by dividing the household income by the square root of the number of dependents for the household income. Age was calculated from the date of birth and the day of the interview.
The outcomes were BMI and WC, evaluated as continuous variables, and the prevalence of general and abdominal obesity was also calculated. General obesity was defined using the values of weight and height, while for abdominal obesity the WC values were used. The body weight and WC data were collected in 2012 and the height was measured in 2009. Body weight was measured using a digital scale (GAMA Italy Professional®) with the interviewees wearing light clothes and weight divided between both lower limbs, arms relaxed laterally to the body, shoulders relaxed and the head maintained in the Frankfurt plane.17 Height was measured using a portable stadiometer built for the study with a tape measure having a maximum capacity of 200cm and a graduation of 1mm. The participant remained in the orthostatic position, barefoot, with heels, buttocks and head in contact with the stadiometer; head in the Frankfurt plane; arms relaxed laterally to the body; and shoulders relaxed.17
In turn, WC was measured with an inextensible anthropometric tape (Sanny) with the participant in upright position. The measure was taken at the narrowest part of the torso below the last rib. For individuals with no visible waist circumference, the perimeter at the midpoint between the iliac crest and the last rib was measured. The measurement was read at the time of expiration.17 Individuals unable to stand, pregnant women and women who had given birth in the six months prior to the research were excluded.
The nutritional diagnosis of general obesity was defined according to the criteria of the World Health Organization18 for a BMI ≥30kg/m2, and used the same cut-off score for both sexes. Abdominal obesity was defined according to sex, corresponding to WC values classified with cut-off scores: in men ≥102cm and in women ≥88cm.
Data were analyzed using Stata version 13.0, and first the description of the sample was made. Linear and logistic regression were used for multivariate analysis and considered statistically significant when p <0.05. Three models for analysis were constructed: the first with the crude analysis of the relationship between socio-economic life course and markers of obesity in adulthood; the second, adjusted to the subject's age; and the third, which included, in addition to age, the current equivalized income in the adjustment. The model adjustment variables were chosen based on the values of the determination coefficient (R2) and also through the global adjustment by means of F-adjusted mean residual test and goodness of fit. The interaction of socio-economic life course with the sex variable was verified, also using p <0.05. Subsequently, in view of the results of the interaction, the data were stratified according to sex. All analyses were done using sample weights (combining the sample design in the baseline, the probability of location in 2012 in each census sector and the estimated population of Florianopolis in 2012), in order to minimize the bias related to loss of follow-up and to maintain the representativeness of the sample. For this, the Stata command “svy” was used in all the analyses performed.
EpiFloripa Adults was approved by the Ethics Committee on Human Research of the Federal University of Santa Catarina (351/08 and 1772/11), and all the respondents signed an informed consent form.
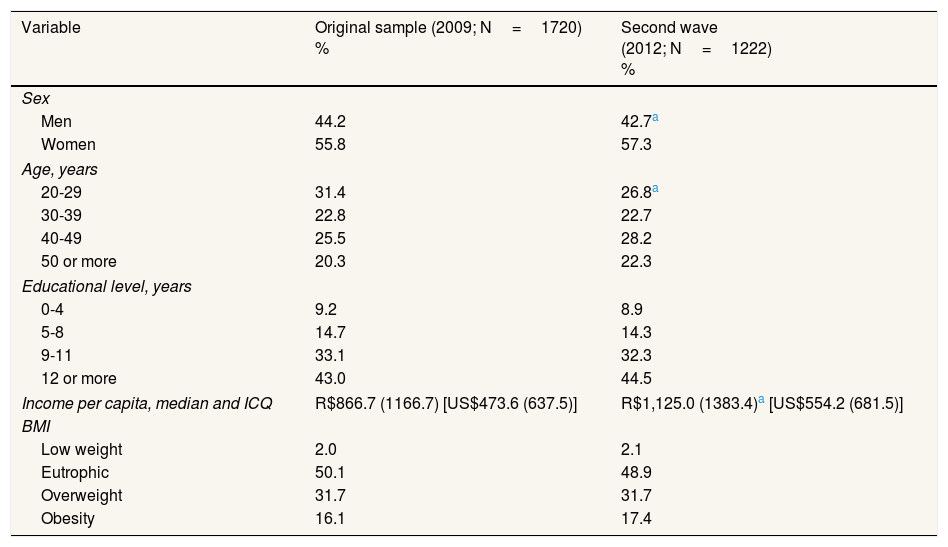
ResultsIn the first follow-up cohort in the year 2012, 1,222 people aged 22 to 63 years (71.1% of baseline) were evaluated, 57.3% of the sample being women. In addition, the current median education was 11 years (p25–p75: 9–15) and equivalized income of R$1,979.90 (p25–p75: R$1154.70 to 3535.50; US$975.30, p25–p75: 568.80 to 1741.60). Comparing the baseline subjects with the first follow-up cohort, there was a greater loss of men and younger subjects (aged 20–29 years), but no differences were found in either sample regarding education and nutritional status (Table 1).
Comparison of the participants’ characteristics in two waves of EpiFloripa study cohort. Florianopolis, Southern Brazil.
| Variable | Original sample (2009; N=1720) % | Second wave (2012; N=1222) % |
|---|---|---|
| Sex | ||
| Men | 44.2 | 42.7a |
| Women | 55.8 | 57.3 |
| Age, years | ||
| 20-29 | 31.4 | 26.8a |
| 30-39 | 22.8 | 22.7 |
| 40-49 | 25.5 | 28.2 |
| 50 or more | 20.3 | 22.3 |
| Educational level, years | ||
| 0-4 | 9.2 | 8.9 |
| 5-8 | 14.7 | 14.3 |
| 9-11 | 33.1 | 32.3 |
| 12 or more | 43.0 | 44.5 |
| Income per capita, median and ICQ | R$866.7 (1166.7) [US$473.6 (637.5)] | R$1,125.0 (1383.4)a [US$554.2 (681.5)] |
| BMI | ||
| Low weight | 2.0 | 2.1 |
| Eutrophic | 50.1 | 48.9 |
| Overweight | 31.7 | 31.7 |
| Obesity | 16.1 | 17.4 |
BMI: body mass index; ICQ: interquartile range.
Data showed that older individuals had parents with fewer years of education while among the younger, the median schooling of the father and mother were higher (ages 22–31=11 years; ages 32–41=8 years; ages 42–51=4 years for the father and 4.5 for the mother; ages 52–63=4 years for both). This difference was considered for the creation of the variable socio-economic life course.
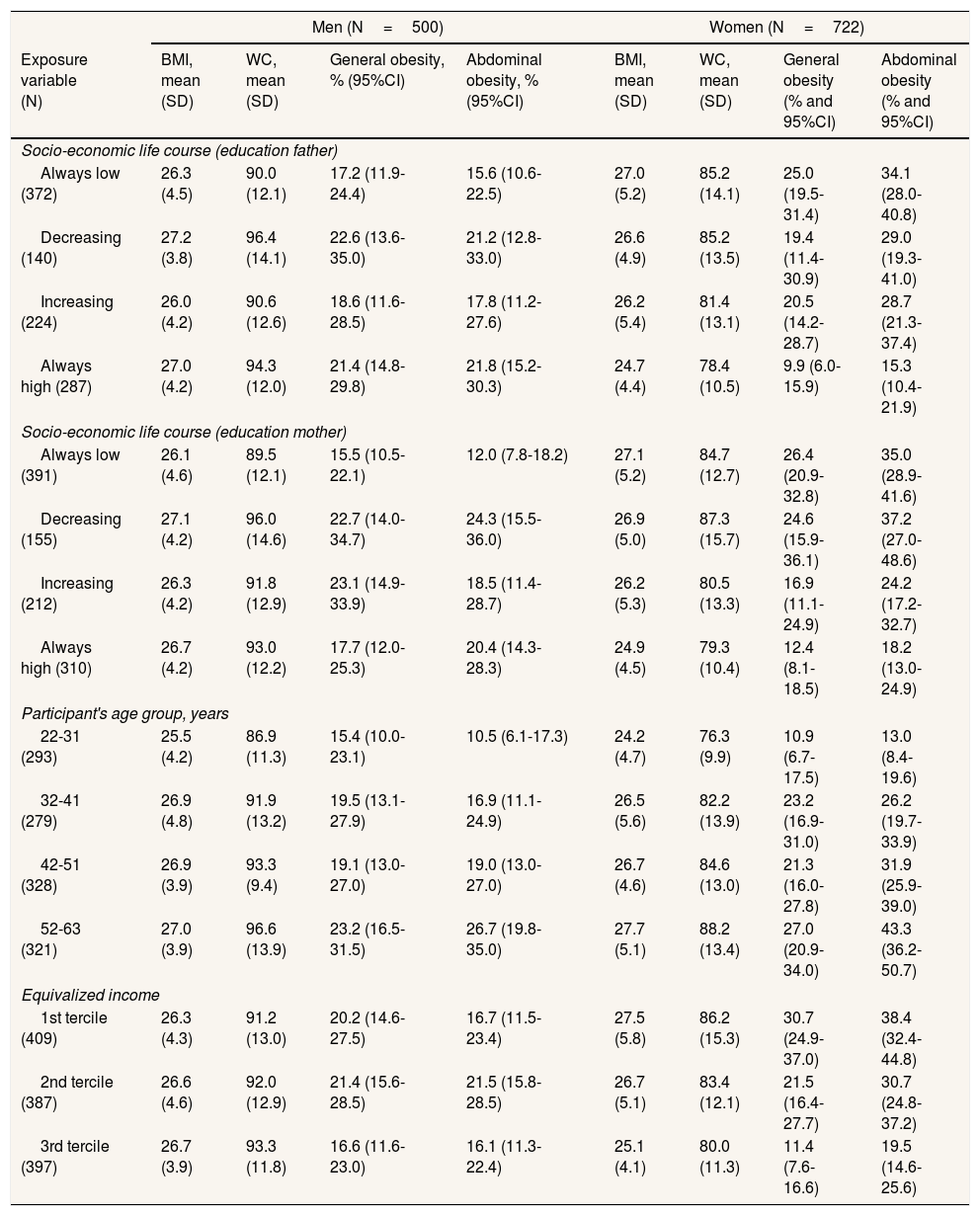
The mean BMI was 26.4kg/m2 (SD: 5.2kg/m2) in women and 26.6kg/m2 (SD: 4.2kg/m2) in men, while the average WC was 83.3cm (SD: 13.4cm) in females and 92.3cm (SD: 12.6cm) in males. The prevalence of general obesity was 20.4% (95%CI: 18.1%;22.8%), with no difference between men and women, and of abdominal obesity 24.8% (95%CI: 22.4%;27.4%), the latter being higher in women than men (p <0.001). Differences were also observed in the prevalence of general and abdominal obesity in relation to age and equivalized income, with the highest percentages of obese identified in the categories of older age and lower income (Table 2).
Distribution of the sample according to the average body mass index and waist circumference and prevalence of general and abdominal obesity according to characteristics of the participants. Florianopolis, Southern Brazil, 2012.
| Men (N=500) | Women (N=722) | |||||||
|---|---|---|---|---|---|---|---|---|
| Exposure variable (N) | BMI, mean (SD) | WC, mean (SD) | General obesity, % (95%CI) | Abdominal obesity, % (95%CI) | BMI, mean (SD) | WC, mean (SD) | General obesity (% and 95%CI) | Abdominal obesity (% and 95%CI) |
| Socio-economic life course (education father) | ||||||||
| Always low (372) | 26.3 (4.5) | 90.0 (12.1) | 17.2 (11.9-24.4) | 15.6 (10.6-22.5) | 27.0 (5.2) | 85.2 (14.1) | 25.0 (19.5-31.4) | 34.1 (28.0-40.8) |
| Decreasing (140) | 27.2 (3.8) | 96.4 (14.1) | 22.6 (13.6-35.0) | 21.2 (12.8-33.0) | 26.6 (4.9) | 85.2 (13.5) | 19.4 (11.4-30.9) | 29.0 (19.3-41.0) |
| Increasing (224) | 26.0 (4.2) | 90.6 (12.6) | 18.6 (11.6-28.5) | 17.8 (11.2-27.6) | 26.2 (5.4) | 81.4 (13.1) | 20.5 (14.2-28.7) | 28.7 (21.3-37.4) |
| Always high (287) | 27.0 (4.2) | 94.3 (12.0) | 21.4 (14.8-29.8) | 21.8 (15.2-30.3) | 24.7 (4.4) | 78.4 (10.5) | 9.9 (6.0-15.9) | 15.3 (10.4-21.9) |
| Socio-economic life course (education mother) | ||||||||
| Always low (391) | 26.1 (4.6) | 89.5 (12.1) | 15.5 (10.5-22.1) | 12.0 (7.8-18.2) | 27.1 (5.2) | 84.7 (12.7) | 26.4 (20.9-32.8) | 35.0 (28.9-41.6) |
| Decreasing (155) | 27.1 (4.2) | 96.0 (14.6) | 22.7 (14.0-34.7) | 24.3 (15.5-36.0) | 26.9 (5.0) | 87.3 (15.7) | 24.6 (15.9-36.1) | 37.2 (27.0-48.6) |
| Increasing (212) | 26.3 (4.2) | 91.8 (12.9) | 23.1 (14.9-33.9) | 18.5 (11.4-28.7) | 26.2 (5.3) | 80.5 (13.3) | 16.9 (11.1-24.9) | 24.2 (17.2-32.7) |
| Always high (310) | 26.7 (4.2) | 93.0 (12.2) | 17.7 (12.0-25.3) | 20.4 (14.3-28.3) | 24.9 (4.5) | 79.3 (10.4) | 12.4 (8.1-18.5) | 18.2 (13.0-24.9) |
| Participant's age group, years | ||||||||
| 22-31 (293) | 25.5 (4.2) | 86.9 (11.3) | 15.4 (10.0-23.1) | 10.5 (6.1-17.3) | 24.2 (4.7) | 76.3 (9.9) | 10.9 (6.7-17.5) | 13.0 (8.4-19.6) |
| 32-41 (279) | 26.9 (4.8) | 91.9 (13.2) | 19.5 (13.1-27.9) | 16.9 (11.1-24.9) | 26.5 (5.6) | 82.2 (13.9) | 23.2 (16.9-31.0) | 26.2 (19.7-33.9) |
| 42-51 (328) | 26.9 (3.9) | 93.3 (9.4) | 19.1 (13.0-27.0) | 19.0 (13.0-27.0) | 26.7 (4.6) | 84.6 (13.0) | 21.3 (16.0-27.8) | 31.9 (25.9-39.0) |
| 52-63 (321) | 27.0 (3.9) | 96.6 (13.9) | 23.2 (16.5-31.5) | 26.7 (19.8-35.0) | 27.7 (5.1) | 88.2 (13.4) | 27.0 (20.9-34.0) | 43.3 (36.2-50.7) |
| Equivalized income | ||||||||
| 1st tercile (409) | 26.3 (4.3) | 91.2 (13.0) | 20.2 (14.6-27.5) | 16.7 (11.5-23.4) | 27.5 (5.8) | 86.2 (15.3) | 30.7 (24.9-37.0) | 38.4 (32.4-44.8) |
| 2nd tercile (387) | 26.6 (4.6) | 92.0 (12.9) | 21.4 (15.6-28.5) | 21.5 (15.8-28.5) | 26.7 (5.1) | 83.4 (12.1) | 21.5 (16.4-27.7) | 30.7 (24.8-37.2) |
| 3rd tercile (397) | 26.7 (3.9) | 93.3 (11.8) | 16.6 (11.6-23.0) | 16.1 (11.3-22.4) | 25.1 (4.1) | 80.0 (11.3) | 11.4 (7.6-16.6) | 19.5 (14.6-25.6) |
In the interaction analysis with the variable sex, associations of BMI, WC and abdominal obesity with the variable socio-economic life course according to father's education were found as well as associations of all outcomes according to the mother's education (data not shown). Therefore, the results are presented separately for men and women.
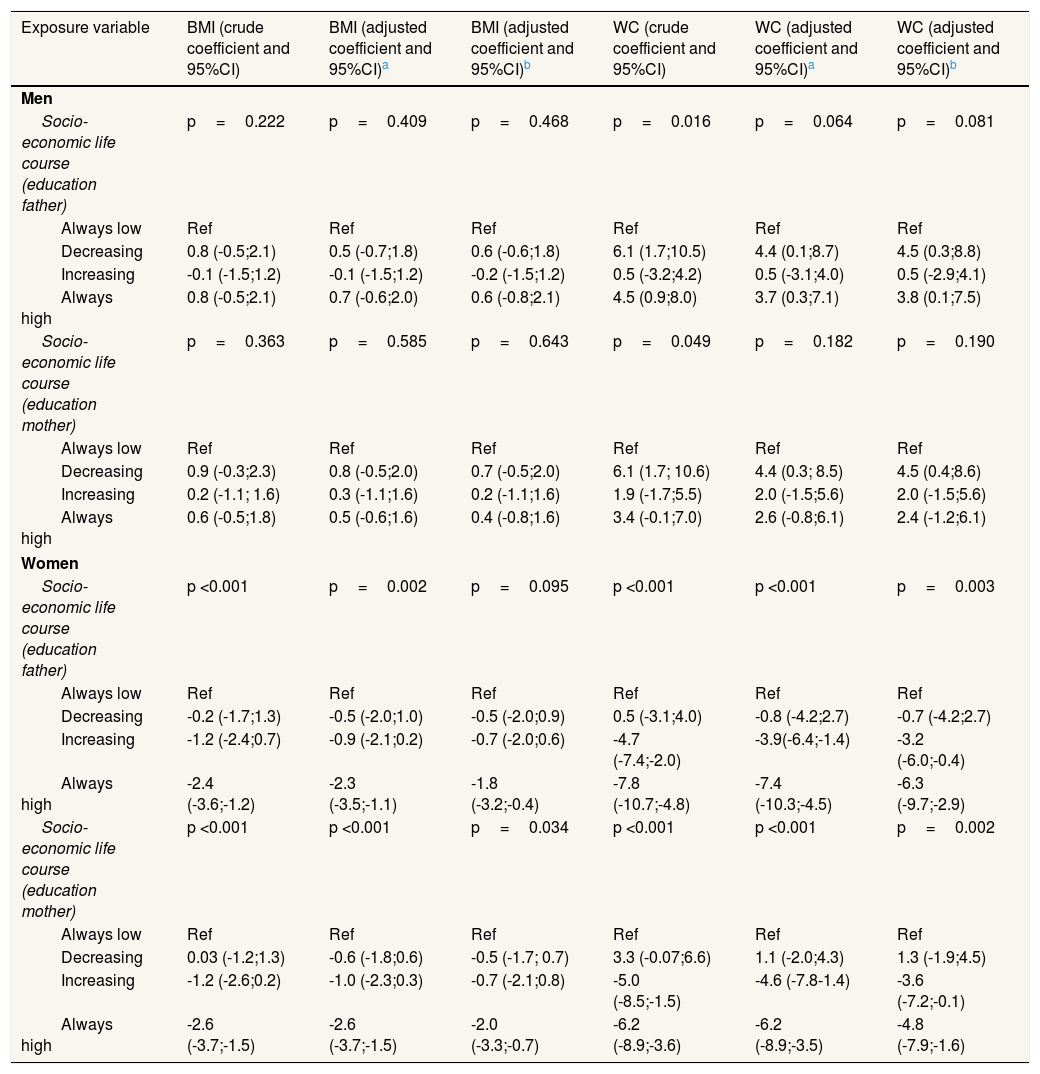
Table 3 shows that the BMI and WC values were lower among women who always remained in the categories of higher SEP and among those whose SEP increased in adulthood. In men, those whose SEP both descended from childhood to adulthood and always remained in the highest SEP had higher WC values. After adjustment for age, BMI values of women were about 2.6kg/m2 (95%CI: −3.7;−1.5) lower and the WC averages were up to 7.4cm lower (95%CI: −10.3;−4.5) among those with higher SEP since childhood and WC was up to 4.4cm lower (95%CI: −7.8;−1.4) in those whose SEP increased compared to the schooling of the parents. In males, this association was in the opposite direction, with approximately 3.7cm higher (95%CI: 0.3;7.1) WC in men who were always in the higher education category and 4.4cm higher (95%CI: 0.1;8.7) among those whose SEP decreased. In the third regression model, which included the variable current equivalized income, BMI was about 2kg/m2 lower (95%CI: −3.3;−0.7) and WC up to about 6cm lower (95%CI: −9.7;−2.9) in women who always had a high SEP, and WC about 3.6cm lower (95%CI: −7.2;−0.1) for those whose SEP increased in adulthood compared to childhood. In men, WC was about 4.5cm higher (95%CI: 0.3;8.8) among those whose SEP decreased and 4cm higher among those who always had a higher SEP (95%CI: 0.1;7.5).
Crude and adjusted coefficient of body mass index and waist circumference of the sample according to the socio-economic life course, stratified by sex. Florianopolis, Southern Brazil, 2012.
| Exposure variable | BMI (crude coefficient and 95%CI) | BMI (adjusted coefficient and 95%CI)a | BMI (adjusted coefficient and 95%CI)b | WC (crude coefficient and 95%CI) | WC (adjusted coefficient and 95%CI)a | WC (adjusted coefficient and 95%CI)b |
|---|---|---|---|---|---|---|
| Men | ||||||
| Socio-economic life course (education father) | p=0.222 | p=0.409 | p=0.468 | p=0.016 | p=0.064 | p=0.081 |
| Always low | Ref | Ref | Ref | Ref | Ref | Ref |
| Decreasing | 0.8 (-0.5;2.1) | 0.5 (-0.7;1.8) | 0.6 (-0.6;1.8) | 6.1 (1.7;10.5) | 4.4 (0.1;8.7) | 4.5 (0.3;8.8) |
| Increasing | -0.1 (-1.5;1.2) | -0.1 (-1.5;1.2) | -0.2 (-1.5;1.2) | 0.5 (-3.2;4.2) | 0.5 (-3.1;4.0) | 0.5 (-2.9;4.1) |
| Always high | 0.8 (-0.5;2.1) | 0.7 (-0.6;2.0) | 0.6 (-0.8;2.1) | 4.5 (0.9;8.0) | 3.7 (0.3;7.1) | 3.8 (0.1;7.5) |
| Socio-economic life course (education mother) | p=0.363 | p=0.585 | p=0.643 | p=0.049 | p=0.182 | p=0.190 |
| Always low | Ref | Ref | Ref | Ref | Ref | Ref |
| Decreasing | 0.9 (-0.3;2.3) | 0.8 (-0.5;2.0) | 0.7 (-0.5;2.0) | 6.1 (1.7; 10.6) | 4.4 (0.3; 8.5) | 4.5 (0.4;8.6) |
| Increasing | 0.2 (-1.1; 1.6) | 0.3 (-1.1;1.6) | 0.2 (-1.1;1.6) | 1.9 (-1.7;5.5) | 2.0 (-1.5;5.6) | 2.0 (-1.5;5.6) |
| Always high | 0.6 (-0.5;1.8) | 0.5 (-0.6;1.6) | 0.4 (-0.8;1.6) | 3.4 (-0.1;7.0) | 2.6 (-0.8;6.1) | 2.4 (-1.2;6.1) |
| Women | ||||||
| Socio-economic life course (education father) | p <0.001 | p=0.002 | p=0.095 | p <0.001 | p <0.001 | p=0.003 |
| Always low | Ref | Ref | Ref | Ref | Ref | Ref |
| Decreasing | -0.2 (-1.7;1.3) | -0.5 (-2.0;1.0) | -0.5 (-2.0;0.9) | 0.5 (-3.1;4.0) | -0.8 (-4.2;2.7) | -0.7 (-4.2;2.7) |
| Increasing | -1.2 (-2.4;0.7) | -0.9 (-2.1;0.2) | -0.7 (-2.0;0.6) | -4.7 (-7.4;-2.0) | -3.9(-6.4;-1.4) | -3.2 (-6.0;-0.4) |
| Always high | -2.4 (-3.6;-1.2) | -2.3 (-3.5;-1.1) | -1.8 (-3.2;-0.4) | -7.8 (-10.7;-4.8) | -7.4 (-10.3;-4.5) | -6.3 (-9.7;-2.9) |
| Socio-economic life course (education mother) | p <0.001 | p <0.001 | p=0.034 | p <0.001 | p <0.001 | p=0.002 |
| Always low | Ref | Ref | Ref | Ref | Ref | Ref |
| Decreasing | 0.03 (-1.2;1.3) | -0.6 (-1.8;0.6) | -0.5 (-1.7; 0.7) | 3.3 (-0.07;6.6) | 1.1 (-2.0;4.3) | 1.3 (-1.9;4.5) |
| Increasing | -1.2 (-2.6;0.2) | -1.0 (-2.3;0.3) | -0.7 (-2.1;0.8) | -5.0 (-8.5;-1.5) | -4.6 (-7.8-1.4) | -3.6 (-7.2;-0.1) |
| Always high | -2.6 (-3.7;-1.5) | -2.6 (-3.7;-1.5) | -2.0 (-3.3;-0.7) | -6.2 (-8.9;-3.6) | -6.2 (-8.9;-3.5) | -4.8 (-7.9;-1.6) |
BMI: body mass index; 95%CI: 95% confidence interval; SD: standard deviation; WC: waist circumference.
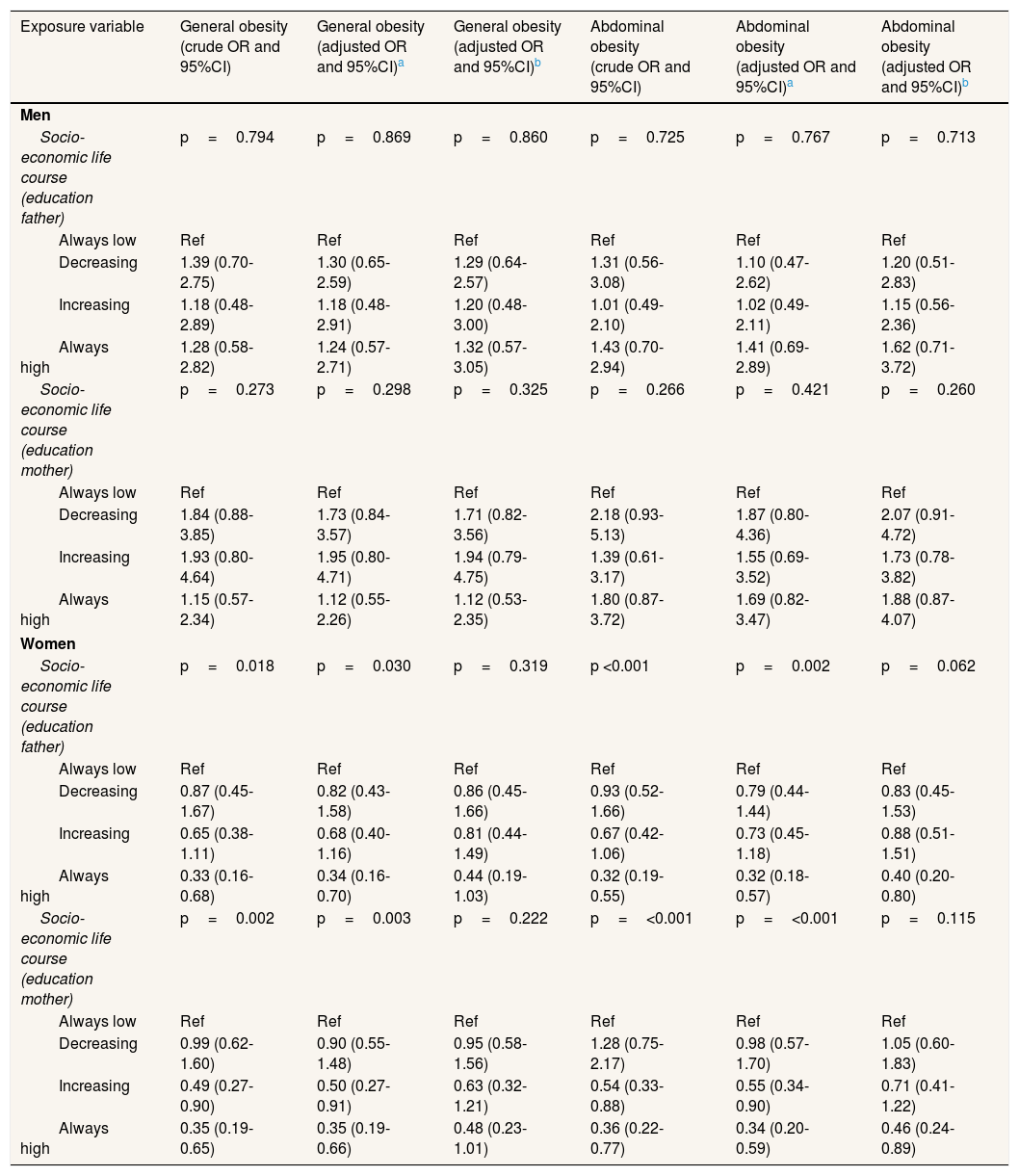
The results of the logistic regression (Table 4) show that, among men, there was no association of general or abdominal obesity with various categories of SEP over the life course. Among women, always being in the categories of high SEP and an increase in SEP compared with the mother's education in childhood were protective factors for obesity. In models adjusted for age, high SEP throughout life was associated with lower odds of general (OR: 0.34; 95%CI: 0.16;0.70) and abdominal obesity (OR: 0.32; 95%CI: 0.18;0.57), a result similar to those who increased in SEP (OR: 0.50; 95%CI: 0.27;0.91 for general obesity, and OR: 0.55; 95%CI: 0.34;0.90 for abdominal obesity) compared with the mother's education in childhood. This difference was only maintained for abdominal obesity and for those who always remained in a high SEP to include the current equivalized income in the model (OR: 0.40; 95%CI: 0.20;0.80 when compared with the father's education, and OR: 0.46; 95%CI: 0.24;0.89 in comparison with the mother's education).
Crude and adjusted odds ratio of general and abdominal obesity in the sample according to the socio-economic life course of participants, stratified by sex. Florianopolis, Southern Brazil, 2012. BMI: body mass index; 95%CI: 95% confidence interval; WC: waist circumference.
| Exposure variable | General obesity (crude OR and 95%CI) | General obesity (adjusted OR and 95%CI)a | General obesity (adjusted OR and 95%CI)b | Abdominal obesity (crude OR and 95%CI) | Abdominal obesity (adjusted OR and 95%CI)a | Abdominal obesity (adjusted OR and 95%CI)b |
|---|---|---|---|---|---|---|
| Men | ||||||
| Socio-economic life course (education father) | p=0.794 | p=0.869 | p=0.860 | p=0.725 | p=0.767 | p=0.713 |
| Always low | Ref | Ref | Ref | Ref | Ref | Ref |
| Decreasing | 1.39 (0.70-2.75) | 1.30 (0.65-2.59) | 1.29 (0.64-2.57) | 1.31 (0.56-3.08) | 1.10 (0.47-2.62) | 1.20 (0.51-2.83) |
| Increasing | 1.18 (0.48-2.89) | 1.18 (0.48-2.91) | 1.20 (0.48-3.00) | 1.01 (0.49-2.10) | 1.02 (0.49-2.11) | 1.15 (0.56-2.36) |
| Always high | 1.28 (0.58-2.82) | 1.24 (0.57-2.71) | 1.32 (0.57-3.05) | 1.43 (0.70-2.94) | 1.41 (0.69-2.89) | 1.62 (0.71-3.72) |
| Socio-economic life course (education mother) | p=0.273 | p=0.298 | p=0.325 | p=0.266 | p=0.421 | p=0.260 |
| Always low | Ref | Ref | Ref | Ref | Ref | Ref |
| Decreasing | 1.84 (0.88-3.85) | 1.73 (0.84-3.57) | 1.71 (0.82-3.56) | 2.18 (0.93-5.13) | 1.87 (0.80-4.36) | 2.07 (0.91-4.72) |
| Increasing | 1.93 (0.80-4.64) | 1.95 (0.80-4.71) | 1.94 (0.79-4.75) | 1.39 (0.61-3.17) | 1.55 (0.69-3.52) | 1.73 (0.78-3.82) |
| Always high | 1.15 (0.57-2.34) | 1.12 (0.55-2.26) | 1.12 (0.53-2.35) | 1.80 (0.87-3.72) | 1.69 (0.82-3.47) | 1.88 (0.87-4.07) |
| Women | ||||||
| Socio-economic life course (education father) | p=0.018 | p=0.030 | p=0.319 | p <0.001 | p=0.002 | p=0.062 |
| Always low | Ref | Ref | Ref | Ref | Ref | Ref |
| Decreasing | 0.87 (0.45-1.67) | 0.82 (0.43-1.58) | 0.86 (0.45-1.66) | 0.93 (0.52-1.66) | 0.79 (0.44-1.44) | 0.83 (0.45-1.53) |
| Increasing | 0.65 (0.38-1.11) | 0.68 (0.40-1.16) | 0.81 (0.44-1.49) | 0.67 (0.42-1.06) | 0.73 (0.45-1.18) | 0.88 (0.51-1.51) |
| Always high | 0.33 (0.16-0.68) | 0.34 (0.16-0.70) | 0.44 (0.19-1.03) | 0.32 (0.19-0.55) | 0.32 (0.18-0.57) | 0.40 (0.20-0.80) |
| Socio-economic life course (education mother) | p=0.002 | p=0.003 | p=0.222 | p=<0.001 | p=<0.001 | p=0.115 |
| Always low | Ref | Ref | Ref | Ref | Ref | Ref |
| Decreasing | 0.99 (0.62-1.60) | 0.90 (0.55-1.48) | 0.95 (0.58-1.56) | 1.28 (0.75-2.17) | 0.98 (0.57-1.70) | 1.05 (0.60-1.83) |
| Increasing | 0.49 (0.27-0.90) | 0.50 (0.27-0.91) | 0.63 (0.32-1.21) | 0.54 (0.33-0.88) | 0.55 (0.34-0.90) | 0.71 (0.41-1.22) |
| Always high | 0.35 (0.19-0.65) | 0.35 (0.19-0.66) | 0.48 (0.23-1.01) | 0.36 (0.22-0.77) | 0.34 (0.20-0.59) | 0.46 (0.24-0.89) |
BMI: body mass index; 95%CI: 95% confidence interval; WC: waist circumference.
The results of this study point towards different associations of socio-economic life course with BMI and WC values between the sexes. In women, both measurements were lower among those who always remained in the categories of higher SEP, while in men, the association was reversed, with higher WC values among the highest SEP both in childhood and adulthood, and only in crude analysis. In the other outcomes for men, no associations were found.
Different studies seem to converge on a higher risk of obesity among women who maintain a low SEP throughout life.6–8,11,19 Among men, however, associations are not consistent. Other studies carried out with a sample of Brazilians corroborate the results of this research and suggest an inverse relationship compared to the one found in women, in which men who were always in the highest group of SEP had a higher chance of being obese,6,8,11 But it has also been reported in the literature that maintaining a high SEP decreases the measures related to adiposity, while no association was found between this exposure and outcome in the male group.19–21
Moreover, associations were found in the categories of socio-economic mobility, in which WC was higher among men whose SEP decreased and lower in women whose SEP increased. Similar results were recorded in the study of Aitsi-Selmi et al.,6 also conducted in Brazil, while different results were shown by other authors. For example, Hart et al.,22 in a study with adults in Sweden, found that a decrease in SEP was associated with a higher average WC among men, and women who increased in SEP were those with the highest WC values.
The influence of socio-economic life course on obesity has as one of its explanatory models the accumulation of risks in which exposure to harmful factors at different stages of life promote a greater likelihood of increased BMI and WC. To the extent that a low socio-economic position promotes worse health outcomes, having a lower SEP in childhood, adolescence and adulthood would also further increase the risk of obesity. Thus, the identification and modification of the factors harmful to health in each stage of life may change their to a point, but the deleterious effect earlier in life brings health consequences depending on the exposure time.23–25
In this sense, the environment in which one lives in childhood will or will not promote better opportunities and lifestyles at different ages, which include factors associated with obesity, such as physical activity and nutrition.25,26 With regard to food consumption among women, a high SEP at different stages of life predicts a healthier eating pattern,27,28 while among men, current conditions are more strongly associated with the consumption pattern.27 Regarding physical activity, a study in Australia indicated that always remaining in the highest socio-economic categories was related to greater physical activity in both men and women.29 Another study, in which aspects related to physical activity over the life course were reviewed, indicated that, especially among women, this should be a habit throughout entire life to remain stable over time.30
The literature also points out the association of socio-economic life course with biological markers, which shows changes in metabolism resulting from socio-economic conditions throughout life. C-reactive protein, for example, which serves as an inflammatory marker that can predict cardiovascular diseases, had increased levels in individuals with low SEP at different ages, indicating a chronic inflammation throughout life.31 Other inflammatory markers, such as fibrinogen and von Willebrand factor, were also higher in individuals with low SEP, in childhood as well as in adulthood.32
An important aspect to highlight in this study is the difference in association between men and women, also reported by other studies. The nutritional transition experienced in Brazil may be related to this result. Population-based surveys conducted in the country show that since the 1970s, cases of malnutrition have declined, leading to obesity. However, despite the fact that higher prevalence of obesity in this transition is associated with higher income population, a decrease in obesity is seen among women with higher income from more developed regions, starting from the 1990s. As a result, women with lower SEP are the most affected in these regions, by malnutrition as well as by obesity.33 The process of nutritional transition in countries with different economic realities indicates that among the individuals with higher SEP, decreasing obesity prevalence in the long run takes longer among men than among women, which may explain the difference between the sexes found in this study.34
Concomitant with this fact, Schlüssel et al.35 point out that Brazilian adult women who have gone through a situation of food insecurity in childhood were 49% more likely to be obese. It has been shown that food insecurity is associated with malnutrition in low-income countries and with obesity in high-income countries. This shows the effects of nutritional transition in Brazil and confirms the fact that women with lower SEP throughout life have higher BMI and WC in this sample. Moreover, Pudrovska et al.36 indicate that women are more susceptible to the effects that a lifelong low SEP have on obesity: these two characteristics have a mutual effect, and in females its unfavorable effect appears to maintain both a lower SEP as well as higher levels of obesity. In this sense, although in both sexes low socio-economic status perpetuates itself in different stages of life, obesity was more persistent among women in low SEP groups.
With regard to socio-economic mobility, Brazil has one of the highest rates of inequality in the world, reflected in its Gini coefficient of 0.519 in 2012.37 Several state policies have been developed in order to reduce poverty in the country, such as income transfer programmes.38 In this sense, the possibility to change one's SEP is increasing, and a greater number of people may be able to do so over the years, which is likely also to change the average BMI and WC.
Strengths and limitationsAmong the limitations of this study is the cross-sectional design with information about the educational level of parents reported by the participants themselves. Despite possible loss of accuracy, this information is relatively stable over time and the results are less affected by recall bias. In addition, other studies have also used familial socio-economic information based on reports in adult life, and showed results consistent with those of studies that collected the data from a longitudinal perspective.11 Another limitation of this study is the absence of variables that could adjust the analyses, especially from data related to the respondents’ childhood, such as family income at birth, which could alter the magnitude of the results.
Strengths of this study were that a representative sample of adults from Florianopolis was included in the baseline and a high response rate was obtained. In addition, there are few studies on this subject conducted in low- and middle-income countries, including Brazil.
ConclusionThe results of this study point towards different associations of socio-economic life course with body mass index and waist circumference values between sex. In women, both measurements were lower among those who always remained in the categories of higher socio-economic position. In men, no associations were found between socio-economic position life course and obesity in adulthood.
In so far as the effect of socio-economic aspects in a perspective of life course on obesity in adults in low- and middle-income countries, including Brazil, is still unclear, the results of this scientific article provide evidence to reinforce a life course approach as an effective strategy to help reduce the prevalence of obesity in adults. Public policies, should be developed and applied throughout the course of life, taking into account the difference between sexes and focusing on groups that are more likely to develop obesity.
Brazil has undergone a rapid process of nutritional transition in a way that obesity increased more than three times in adults over the past 20 years and there is still no consensus on the best way to prevent this disease from a population perspective. The literature indicates that the socio-economic position at every stage of life −childhood, adolescence and adulthood− has an independent relationship with obesity. Concomitant to this fact, the socio-economic conditions in each have cumulative effects on body weight in the long term. From a life course perspective, obesity is included among the health problems whose prevalence varies in different social groups throughout life, reflecting the cumulative exposure to deleterious factors at different ages.
What does this study add to the literature?The results of this study point towards different associations of socio-economic life course with body mass index and waist circumference values between sex. In women, both measurements were lower among those who always remained in the categories of higher socio-economic position. In men, no associations were found between socio-economic position life course and obesity in adulthood. In so far as the effect of socio-economic aspects in a perspective of life course on obesity in adults in low- and middle-income countries, including Brazil, is still unclear, the results of this scientific article provide evidence to reinforce a life course approach as an effective strategy to help reduce the prevalence of obesity in adults. Public policies, should be developed and applied throughout the course of life, taking into account the difference between sex and focusing on groups that are more likely to develop obesity.
Leila P. García.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsK. Jakovljevic Pudla Wagner was responsible for structuring the manuscript, analysis and interpretation of results and writing of the manuscript. J.L. Bastos was responsible for the design of the research and critical review of the manuscript. A. Navarro was responsible for writing, analysis and critical review of the manuscript. A.F. Boing was responsible for the design of the research, analysis and interpretation of results and critical review of the manuscript.
FundingThis work was supported by the Brazilian National Council for Scientific and Technological Development (CNPq) number 485327/2007-4 and 477061/20109.
Conflict of interestsNone.











