




Describe the risk of poverty and social exclusion in children aged 8-11 years from Gipuzkoa and Valencia (Spain), through AROPE (At Risk Of Poverty or Social Exclusion) indicators, and evaluate their associated factors in the INMA Project (Childhood and Environment).
MethodFamilies in Gipuzkoa and Valencia (394 and 382, respectively) completed a questionnaire in 2015-2016. Low work intensity (LWI), at risk of poverty (RP) and material deprivation (MD) were estimated. AROPE consisted in meeting any of the previous sub-indicators. Socio-demographic, family and parental characteristics were considered. Frequencies, Venn's diagrams, and chi-square and Fisher tests were used in bivariate analysis and logistic regression in multivariate analysis.
ResultsFor LWI, RP, MD and AROPE, prevalence of 2.5%, 5.6%, 2.3% and 7.2% were obtained in Gipuzkoa, and 8.1%, 31.5%, 7.8% and 34.7% in Valencia, respectively. In the multivariate analysis, the AROPE was associated in both areas with maternal social class and non-nuclear families. In Gipuzkoa, it was also related to maternal education. In Valencia, other factors were the mother's foreign origin, and paternal education and smoking.
ConclusionThere is higher AROPE prevalence in Valencia. Social class and family type were shared factors, but a differential pattern is observed in other social determinants. It is essential to implement social policies to reduce this axis of inequalities in health, especially in childhood.
Describir el riesgo de pobreza y exclusión social en niños/as de 8-11 años de Gipuzkoa y Valencia (España), mediante los indicadores AROPE (At Risk Of Poverty or Social Exclusion), y evaluar sus factores asociados en el Proyecto INMA (Infancia y Medio Ambiente).
MétodoFamilias de Gipuzkoa y Valencia (394 y 382, respectivamente) completaron un cuestionario en 2015-2016. Se estimaron la baja intensidad de trabajo (BIT), el riesgo de pobreza (RP) y la privación material (PM). AROPE consistió en cumplir cualquiera de estos subindicadores. Se consideraron características sociodemográficas, familiares y parentales. Se usaron diagramas de Venn, los test de Ji-cuadrado y Fisher en los análisis bivariados, y regresión logística en los análisis multivariados.
ResultadosSe obtuvieron prevalencias para BIT, RP, PM y AROPE del 2,5%, 5,6%, 2,3% y 7,2% en Gipuzkoa, y del 8,1%, 31,5%, 7,8% y 34,7% en Valencia, respectivamente. En el análisis multivariado, el AROPE se asoció en ambas áreas con la clase social materna y la familia no nuclear. En Gipuzkoa, también se relacionó con la educación materna. En Valencia, otros factores fueron el origen extranjero materno y la educación y el tabaquismo paternos.
ConclusiónHay un AROPE más alto en Valencia. La clase social y el tipo de familia fueron factores compartidos, pero se observa un patrón diferencial en otros determinantes sociales. Es esencial implementar políticas sociales para reducir este eje de desigualdad en salud, especialmente en la infancia.
The Great Recession1 has spurred poverty and social exclusion.2 Poverty is defined as not having enough resources to live with dignity.3 Social exclusion refers to citizens that are not allowed to play a role in society because of their characteristics.3 This exclusion acts through different paths: by impeding access to higher education, employment opportunities and a regular income, by obstructing the way to governance3, and fostering learned helplessness.4
The economic strategy of European Union (EU) “Europe 2020” proposed reducing in 20 million the European population suffering poverty,5 as measured by the At Risk Of Poverty or Social Exclusion (AROPE).2,6–10 This indicator describes poverty (based on income),11 employment problems (based on work intensity), and material deprivation (lacking some items).6
In comparison to 2009 (when “Europe 2020” was introduced), by 2015 several countries had reduced AROPE; other had not met their objectives, and three (Greece, Cyprus, and Spain) showed increasing trends.6 In Spain, 22.3% of the population are at risk of poverty, 14.9% have low work intensity, 5.8% have severe material deprivation, and 29.7% are AROPE.8 This indicator is not homogeneous throughout Spain, as it reached in 2016 a range of 14-40% depending on the region considered.9
This issue is important in general population, but a more vulnerable group such as children has even higher rates of poverty: 32.9% of children are in AROPE households, 29.7% are below the poverty threshold, and 7.1% suffers from severe material deprivation.8 Childhood and adolescence are periods of evolution,12 and influences received by then may have short and long term implications. Firstly, this exposure could increase the risk for health problems such as growth retardation, asthma, or injuries.13,14 Secondly, poverty influences mental wellbeing, by having less copying strategies and expectations,15 presenting more cognitive deterioration, and depression.12 And thirdly, poverty determines health habits such as having a healthy diet or the abuse of substances.13
Child poverty is often determined by family characteristics: having low educated,6,16 young,16,17 unemployed6,17 or immigrant6 parents increased the risk of poverty, as well as living in a rural area6,16,17 or in a single-parent family.6,16 Parental education appears to be a strong determinant that crosses from one generation to the next: 6 in 2015, at least 65.5% of European children of low educated parents were at risk of poverty or social exclusion.6
An approach where both parents may play a role will be necessary to understand the differential effect of maternal a paternal education, social class, or unemployment6 on child poverty. We already reported in the INMA Project18 a socioeconomic gradient in child's cognitive scores at 5 years of age,19 with differential impact, being maternal education and paternal social class the stronger social determinants. Socioeconomic gradient studied by classical concepts such as parental education, social class and employment status has been widely explored; however, more comprehensive indicators need to be considered, such as poverty and social exclusion, to identify those households at social risk.
To our knowledge, none of the reviewed studies have used primary data at regional level to identify factors potentially influential in child poverty: they rather used national2,7–9 or supranational10 surveys, which are inaccurate at a regional level.20 The aim of the present study is to describe the risk of poverty and social exclusion, as measured by the AROPE indicators, in households of children aged 8 to 11 years in Gipuzkoa and in Valencia INMA cohorts, two regions with different wealth levels; and to assess the relationship of socio-demographic and family characteristics with AROPE indicators in each area, considering maternal and paternal factors.
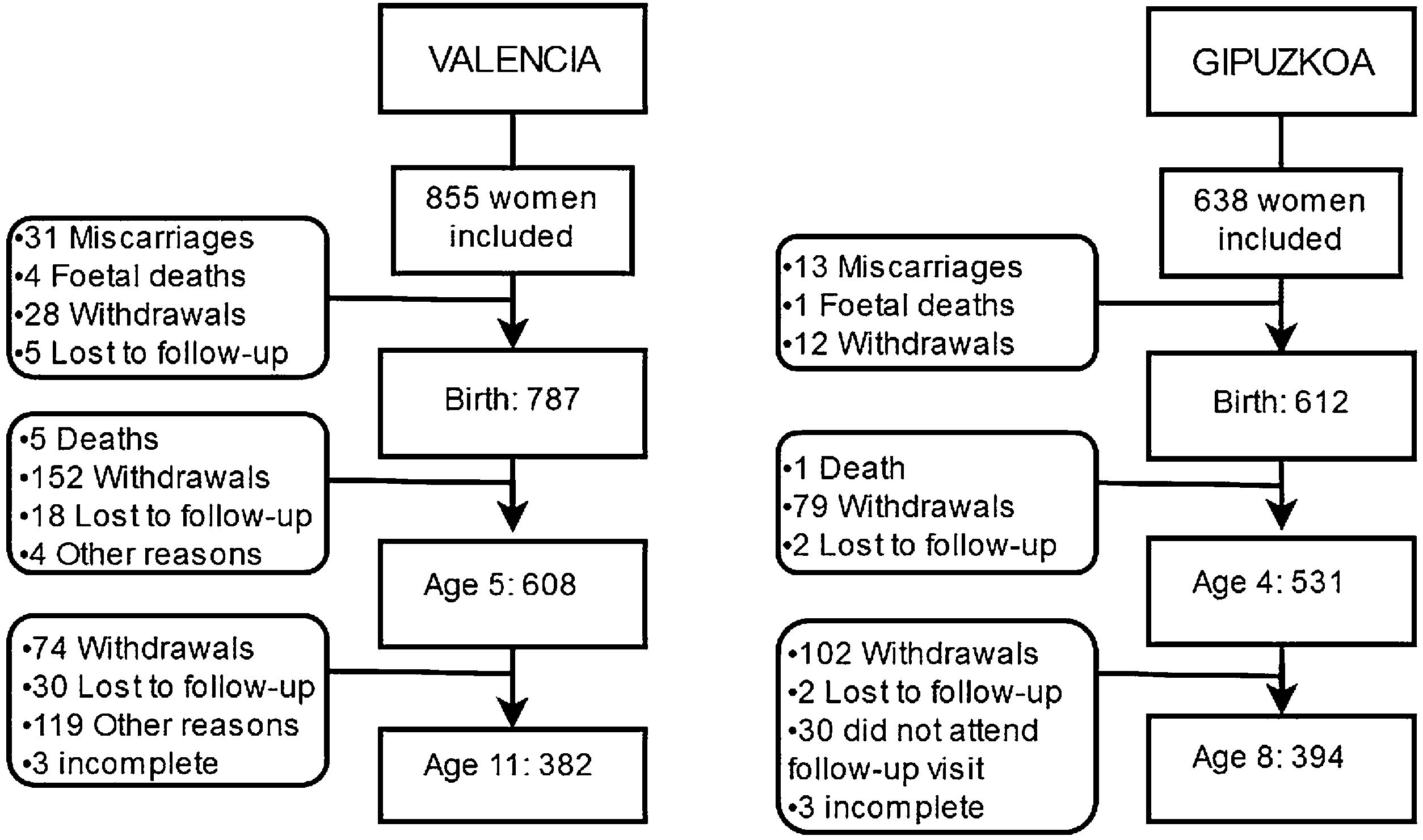
METHODStudy design and populationINMA (INfancia y Medio Ambiente - Environment and Childhood) Project is a Spanish population-based mother-and-child multicenter cohort study.18 This study uses data from INMA Valencia and Gipuzkoa cohorts. Mothers were recruited during their first prenatal visit to La Fe Hospital (Valencia) in 2003-2005, and Zumárraga Hospital (Gipuzkoa) in 2006-2008. The inclusion criteria were>16 years of age, singleton pregnancy, intention of undergoing follow-up and delivery in their hospital, no impediment for communication, and no assisted conception.18,19 Withdrawals, exclusions, and children's age at follow-up visits are shown in Figure 1. A cross-sectional design was used in the present study within the INMA cohort framework. We collected data on AROPE indicators of participant families between 2015 and 2016, when children were 11 and 8 years old in Valencia and Gipuzkoa cohorts, respectively. In the present study, the final sample was 394 families in Gipuzkoa and 382 in Valencia. Cohorts were approved by their local institutional ethical review boards, and consent to participate was obtained from participants.
AROPE indicators
AROPE indicators were assessed by structured questionnaires self-completed by parents in their homes and revised by a trained interviewer at the beginning of the follow-up visits. AROPE comprises three sub-indicators which are calculated in each household (see Appendix 1 online): low work intensity (LWI) (having worked <20% of available hours of their members in working age), at risk of poverty (RP) (having <60% of Spanish median income per consumption unit) and risk of material deprivation (MD) (lacking ≥4 necessary items from a list of 9).9 Traditionally, the cut-off point used for determining families at risk of MD has been severe MD (lacking ≥4 elements). However, for this study, this variable was dichotomized as low vs medium and severe MD (lacking ≥3 elements) due to the few number of cases in severe MD.
AROPE8,9 were those households fulfilling at least one of the three previous sub-indicators (LWI, PBUP or MD).
In the same follow-up visit, some additional information regarding family economic situation was requested, such as making ends meet, how was their economic situation in comparison to 2007, and if the household had received any income in the past month (see Appendix 1 online).
Variables and data collectionVariables regarding other socio-demographic and family characteristics were collected by self-completed questionnaires supported by the interviewer at different follow-up visits (week 12, and 32 of pregnancy, and age 4-5, and 8-11). Socio-demographic characteristics (social class, educational level, country of origin, parental age and parental working status), family and child characteristics (type of family, number of siblings), parental characteristics (mental health, smoking status) were collected at different follow-up points (see Appendix 1 online).
Data imputationSimple data imputation was performed for the household income in 33 and 122 cases in Valencia and Gipuzkoa, respectively, in order to avoid missing data in RP and AROPE (further information on imputation method is described in Appendix 2 on line, Tables Ia and Ib). In both cases, a wide range of related variables were used in a forward procedure, by using linear regression, with a p-value for exclusion of 0.20 and a p-value for inclusion of 0.10. Imputation was performed with Stata 12th Version.
Statistical analysisPercentages and bar and Venn diagrams were used in the descriptive analysis.
The relationship of socio-economic and family characteristics with the AROPE indicator was assessed by cohort and taking into account both mother and father factors, when available, using for bivariate analysis chi-square, Fisher tests, and simple logistic regression. Multivariate logistic models using imputed data were built to identify those factors that better predicted the risk of poverty and social exclusion in the families of each cohort, after adjusting for the other potential determinants. The final model was built according to the following steps: firstly, simple logistic regressions were performed to assess AROPE relation with covariates. Those which obtained a p ≤0.20 were selected, with the exception of employment situation which was part of AROPE. The final models were calculated for each cohort, excluding sequentially those variables not related at p ≤0.10 in the adjusted model following a backward stepwise selection procedure. A sensitivity analysis was performed with non-imputed data including only those variables selected in the final models in order to replicate them. Statistical analyses were carried out using SPSS, version 24.0 and R Version 3.5.1. Figures 2 to 5 were created with R Version 3.5.1, and Figure 1 was created with the open source diagram technology draw.io.
ResultsSample distributionThe sample description is shown in Table II in Appendix 2 online. Distributions across cohorts were statistically different. More advantaged positions were observed in Gipuzkoa, where parents were slightly older and more often classified as being employed, or having higher social position or education than in Valencia. In Gipuzkoa, there was a higher proportion of nuclear families than in Valencia and parents were less likely to be smokers or foreigners. No differences were found across parental mental health and paternal current smoking habit.
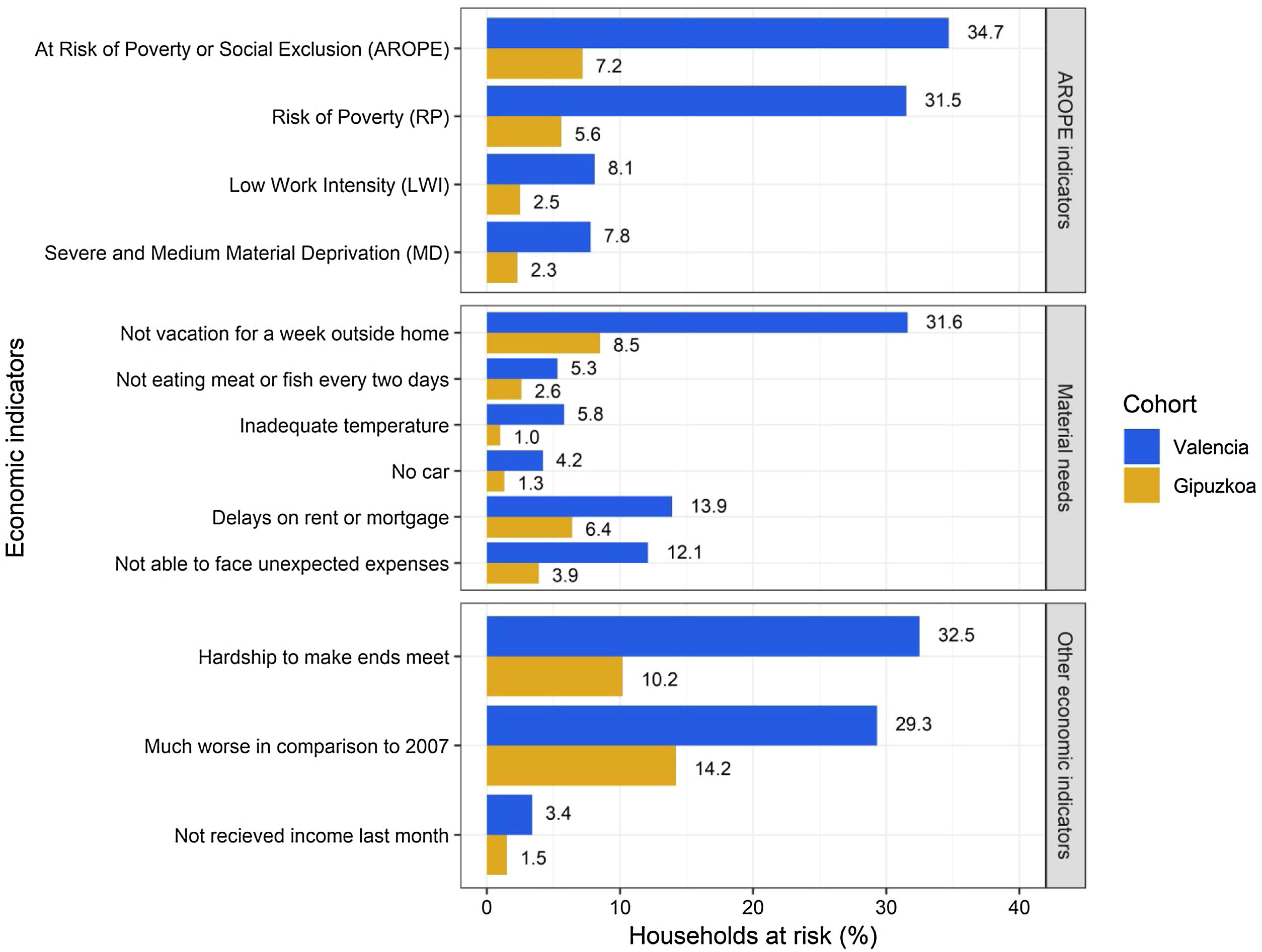
AROPE indicators and other family economic characteristicsDescriptive analysis of the AROPE and other family's economic indicators is plotted in Figure 2. Most of the indicators considered were found statistically different between cohorts, with the exception of “Not eating meat or fish every two days” and “Not having received income in the last month”. Higher risks were observed in Valencia, in comparison to Gipuzkoa: in Valencia, 7.8% of households had MD, 8.1% had LWI, 31.5% were RP and 34.7% were AROPE; in Gipuzkoa, these rates were 2.3%, 2.5%, 5.6% and 7.2%, respectively.
Interrelation of AROPE sub-indicators
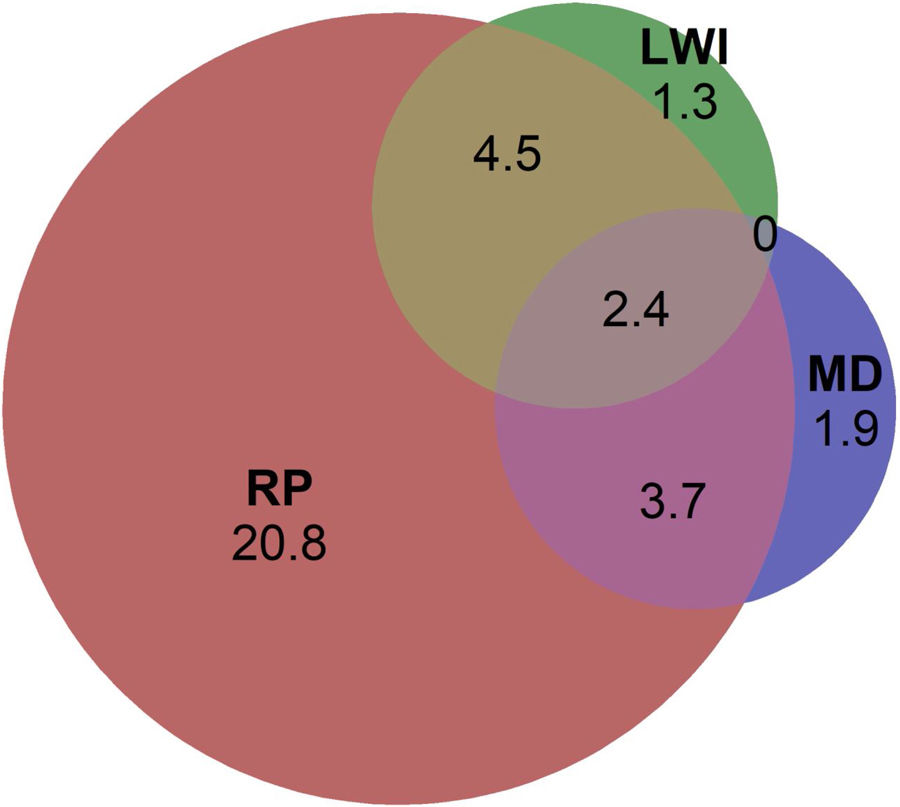
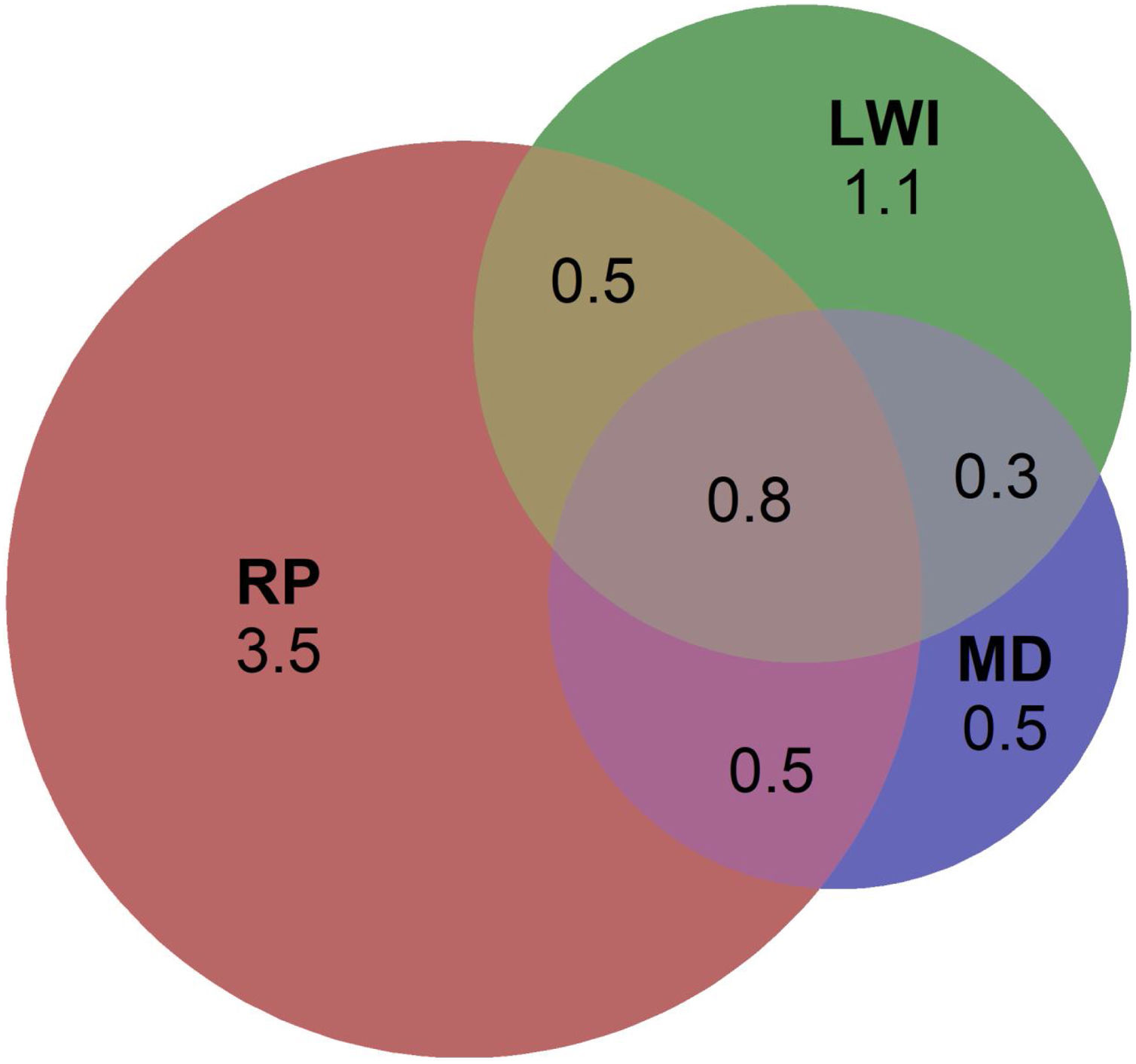
The interrelation between MD, LWI, RP are represented in Figures 3 and 4 by Venn's diagrams for Valencia and Gipuzkoa. When considering non-shared contributions to AROPE, RP sub-indicator emerged as the most relevant, representing 20.8% and 3.5% of the sample for Valencia and Gipuzkoa, respectively. In Valencia, no overlapping between MD and LWI was observed. Several cases were found to be at risk in all three sub-indicators, representing the 2.4% and 0.8% of AROPE in Valencia and Gipuzkoa, respectively.


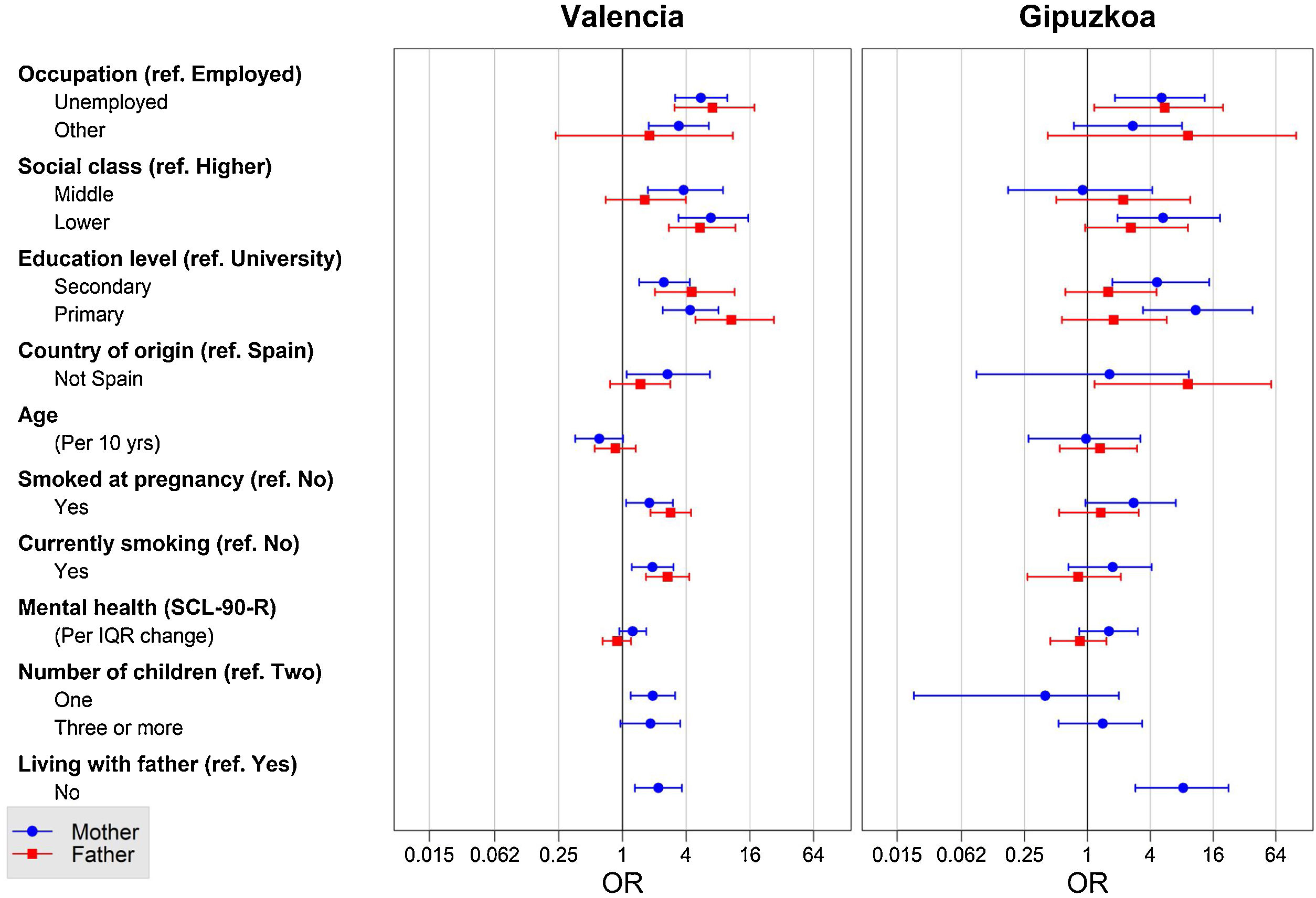
Bivariate analysis between AROPE and all the variables considered is depicted in Table III in Appendix 2 online, and unadjusted univariate regressions comparing the effect of maternal and paternal characteristics through both cohorts can be observed in Figure 5. Those parents who were unemployed, or those who were placed in the lowest social class, were more prone of being AROPE. Regarding education, in Valencia both parents presented higher risks when having lower education. The same happened for mothers in Gipuzkoa, but not for fathers. In general terms, parents from foreign country of origin, as well as those who lived in non-nuclear families were more likely to be AROPE. Number of children and tobacco use was significantly related in Valencia. To be more precise, in Valencia was found this association for both parents at pregnancy and in the last follow-up visit. Mothers who smoked during pregnancy in Gipuzkoa were also more likely to be AROPE, even when this relation was not statistically significant. Mothers and fathers showed differential patterns of risk when considering cohort: in Valencia, mothers showed stronger associations than fathers in social class and country of origin, and fathers in education and smoking habits. In Gipuzkoa, mothers had a stronger relation than fathers in low social class and education, and fathers in country of origin.
Risk factors model
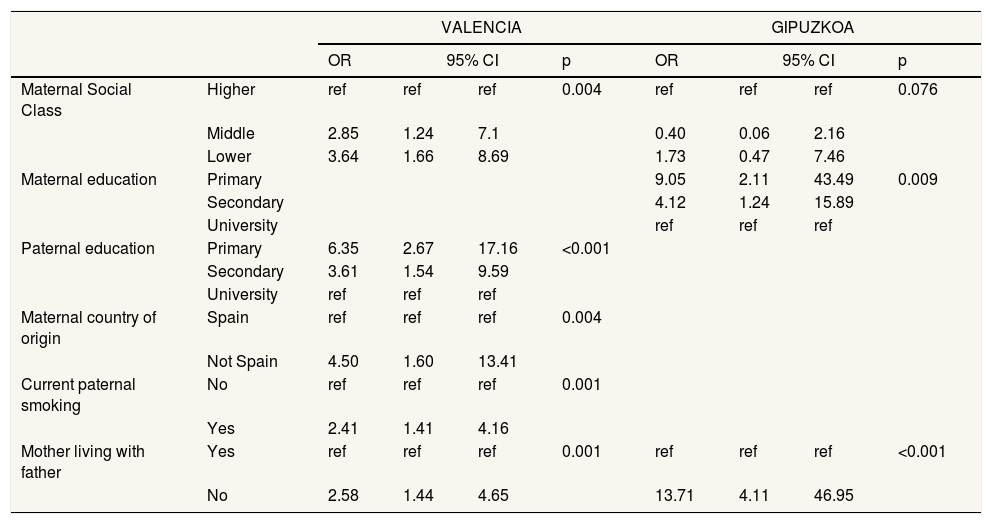
Our final adjusted risk factors models are shown in Table 1. Social class and type of family were associated with AROPE in both cohorts, being at higher risk those households with low social class mothers and those non-nuclear families. Additionally, in Gipuzkoa, lower educated mothers were also at higher risk (upper vs. lower [odds ratio (OR): 9.05; 95% confidence interval (95%CI): 2.11-43.49]). However, the final model in Valencia showed as predictor paternal rather than maternal education (upper vs. lower [OR: 6.35; 95%CI: 2.67-17.16]), maternal country of origin (Spain vs. not Spain [OR: 4.50; 95%CI: 1.60-13.41]), and current paternal smoking (no vs. yes [OR: 2.41; 95%CI: 1.41-4.16]).
Final models for AROPE in Valencia and Gipuzkoa.
| VALENCIA | GIPUZKOA | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | ||||
| Maternal Social Class | Higher | ref | ref | ref | 0.004 | ref | ref | ref | 0.076 |
| Middle | 2.85 | 1.24 | 7.1 | 0.40 | 0.06 | 2.16 | |||
| Lower | 3.64 | 1.66 | 8.69 | 1.73 | 0.47 | 7.46 | |||
| Maternal education | Primary | 9.05 | 2.11 | 43.49 | 0.009 | ||||
| Secondary | 4.12 | 1.24 | 15.89 | ||||||
| University | ref | ref | ref | ||||||
| Paternal education | Primary | 6.35 | 2.67 | 17.16 | <0.001 | ||||
| Secondary | 3.61 | 1.54 | 9.59 | ||||||
| University | ref | ref | ref | ||||||
| Maternal country of origin | Spain | ref | ref | ref | 0.004 | ||||
| Not Spain | 4.50 | 1.60 | 13.41 | ||||||
| Current paternal smoking | No | ref | ref | ref | 0.001 | ||||
| Yes | 2.41 | 1.41 | 4.16 | ||||||
| Mother living with father | Yes | ref | ref | ref | 0.001 | ref | ref | ref | <0.001 |
| No | 2.58 | 1.44 | 4.65 | 13.71 | 4.11 | 46.95 | |||
Sensitivity analysis with non-imputed data is shown in Table IV in Appendix 2 online. The trends and estimates did not change greatly when comparing imputed and non-imputed models.
DiscussionWe explored the distribution of household poverty or social exclusion in children of two different areas, described by a wide range of variables such as AROPE sub-indicators, economic characteristics and material constraints highly related to child poverty. In the families of our study samples, we found 34.7% and 7.2% of AROPE in Valencia and Gipuzkoa, respectively. For all these descriptive variables, Valencia showed higher risks. In addition, we decomposed AROPE in its sub-indicators, being RP the greater non-shared contributor to AROPE condition, followed by the other two sub-indicators which were widely overlapped to RP. AROPE was more prevalent in unemployed, low educated, low social class and non-Spanish parents, with smoking habits, and in non-nuclear families. Maternal social characteristics showed a preeminent role in Gipuzkoa, especially level of education, in which fathers showed a null effect. Contributions to AROPE were more evenly distributed between parents in Valencia.
AROPE indicators in our data and in general populationEuropean Anti-Poverty Network (EAPN) has previously described regional AROPE, estimating 30.5% in Valencian Community and 15.9% in Basque Country8 for 2016 (Table V in Appendix 2 online). The differences with our results could be explained because our recruitment area was a part of the region which could not be absolutely representative. In fact, average income in Valencian Community was slightly higher than the average income in Valencia recruitment area,21 (12.398 vs. 12.127 € of family available income), and Basque Country population was less affluent than Gipuzkoa recruitment area (33.766 vs. 35.579 € of family available income).22
Additionally, in the general population very different types of household can be found. However, in this study we used data of families with children which are more prone to poverty.23 Moreover, nuclear and non-nuclear families have different rates of poverty, showing the latter greater risks.8 The AROPE prevalence in Valencia may be higher in our sample than in the general population because our cohort has a high rate of non-nuclear families (20.5%).
Finally, in this work, AROPE was calculated using moderate and not severe MD, and this could be overestimating AROPE. However, MD has small weight on AROPE, and the re-estimation with severe MD yielded AROPE rates of 33.6% and 6.6% for Valencia and Gipuzkoa, respectively (Table V in Appendix 2 online).24
AROPE is highly correlated with RP.7 Smaller overlapping of LWI and RP was observed in Gipuzkoa in comparison to Valencia, and non-shared rate of LWI is very similar in both cohorts. Coexistence of high rates of RP and low rates of LWI in Valencia reflects that employed people are at risk of poverty (the working poor).25 Having an employment does not protect from having low wages, mainly due to precarious contracting. No overlapping of LWI and MD could be partly explained by black economy, which may have been omitted for desirability.
Disparities between Valencia and Gipuzkoa could be consequence of better public policies in Basque Country in comparison to Valencian Community.26 Taking as an example the minimum insertion income, we can observe that is an unequal policy across regions in Spain: for example, the same household could receive an insertion income of 945.88 € in Basque Country, while in Valencian Community it would be 434.88 €.27 It is then crucial to implement social policies more equally across the country. In this line of action, Spanish Government proposed the vital minimum income as a national policy to ameliorate situations of poverty and exclusion.28 However, political instability has not allowed the development of this proposal yet.
AROPE risk factors in each cohortIn our study, parental education and social class played an important role, as observed also in a recent European study23 and in an EU report.6 However, the role of parental education varied according to area: maternal and paternal education was related to AROPE in Valencia, but in Gipuzkoa only maternal education played a role. This may be because in Valencia occupation was highly related with education in mother and father, while these variables were only related in mothers in Gipuzkoa (data not shown), where men seem to be employed independently to their level of education.
Non-nuclear families, especially monomarental ones, are more vulnerable to income scarcity6,8,23 because they also have less flexibility to distribute housework, childcare and paid work in comparison to a nuclear family.29
Foreign country of origin have shown trends of higher risk of poverty.8,23 This gap is different across European countries, finding Norway and the Netherlands with the smallest differences between native and non-native citizens, and Spain with the greatest, followed by Greece and Italy.23
In Valencia, child poverty was also related to current paternal smoking (Table VI in Appendix 2 online). In INMA cohorts, smoking is highly related to social class and education.30 Households living in economic strain are more vulnerable to stress and anxiety,31,32 and those with less tolerance to anxiety could have more difficulties for dropping tobacco.31
According to recent reports, one third of children in Spain are at risk of poverty or social exclusion.33,34 The main factors of poverty are having a non-nuclear family,33,34 and having non-native, and low educated parents.34,35 However, it is also argued that the main tool to break the cycle of poverty is children's education.34
Limitations of this workFirstly, lack of data on household income made necessary a data imputation, but sensitivity analysis showed no differences. Secondly, small numbers in some factors did not allow arising strong conclusions. Thirdly, AROPE was calculated considering medium and severe MP, instead of severe MP, but re-estimation did not changed prevalence greatly. Finally, representativeness of the sample was a problem to generalization; because sample selection was non-representative of population in Gipuzkoa and Valencia and because those families with less advantaged social positions tend to abandon the study follow-up19.
Strengths of this workFirstly, AROPE is the gold standard for measuring poverty in EU. Secondly, we considered a wide range of variables depicting parental characteristics, and both parents were represented. Finally, although this work presented a cross-sectional design, the prospective nature of the INMA cohort study allow the use of data collected at different stages. Therefore, AROPE will be a key tool to be used as a social determinant for present but also upcoming health outcomes.
Implications for policy makersIt is crucial to foster the accessibility to education by the use of public scholarships and investments in public schools. Additionally, regulating and protecting labour market, would increase economic affluence. Moreover, increasing and equalizing economic policies such as minimum insertion income or developing recent proposals such as the minimum vital income, would reduce poverty and social exclusion. Finally, non-nuclear and foreign country of origin families would have a better support if some services were partially funded by the government, in order to equalize the lack of resources non-nuclear families have in comparison to nuclear families.
Poverty is a powerful determinant on health, especially at young age. The At Risk of Poverty or Social Exclusion (AROPE) indicator is the European Union preferred indicator to measure poverty. Child poverty is conditioned by maternal and paternal characteristics.
What does this study add to the literature?This is the first cohort study assessing AROPE in Spain, which was mainly related to parental education, maternal social class and country of origin, paternal smoking, and non-nuclear family. It is crucial to foster the accessibility to education, protect and improve labour market and economic and social support to non-nuclear families.
María-Victoria Zunzunegui.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsL. González contributed to the manuscript by data collection, analysis and data interpretation, drafting the manuscript for revision, approving the final version for publication, and responding for its precision and integrity. M. Estarlich, I. Larrañaga and M. Rebagliato contributed to the manuscript by designing the work, analysis and data interpretation, revising critically with important intellectual contributions, approving the final version for publication, and responding for its precision and integrity. M. Murcia contributed to the manuscript by analysis and data interpretation, revising critically with important intellectual contributions approving the final version for publication, and responding for its precision and integrity. F.B. Barreto contributed to the manuscript by data collection, revising critically with important intellectual contributions approving the final version for publication, and responding for its precision and integrity. L. Santa-Marina, E. Arranz, L. Cirugeda and S. Simó contributed to the manuscript by data interpretation, revising critically with important intellectual contributions approving the final version for publication, and responding for its precision and integrity.
AcknowledgementsThe authors would particularly like to thank all participants for their generous collaboration, and Esperanza Alabarta Domínguez for her support with the fieldwork. A full list of the INMA Project researchers is available at ht**tp://www.proyectoinma.org
FundingThis study was funded by Grants from European Union (FP7-ENV-2011 code 282957 and HEALTH.2010.2.4.5-1), Spain: Instituto de Salud Carlos III (ISCIII) (Red INMA G03/176, CB06/02/0041; FIS-FEDER: PI03/1615, PI04/1509, PI04/1112, PI04/1931, PI05/1079, PI05/1052, PI06/0867, PI06/1213, PI07/0314, PI09/00090, PI09/02647, PI11/01007, PI11/02591, PI11/02038, PI13/1944, PI13/2032, PI13/02187, PI14/00891, PI14/01687, PI16/1288, and PI17/00663), Generalitat Valenciana: Fundación para el Fomento de la Investigación Sanitaria y Biomédica de la Comunitat Valenciana (FISABIO) (UGP 15-230, UGP-15-244, and UGP-15-249), Consorcio de Investigación Biomédica en Red de Epidemiología y Salud Pública (CIBERESP), Department of Health of the Basque Government (2005111093, 2009111069, 2013111089 and 2015111065), and the Provincial Government of Gipuzkoa (DFG06/002, DFG08/001 and DFG15/221) and annual agreements with the municipalities of the study area (Zumarraga, Urretxu, Legazpi, Azkoitia y Azpeitia y Beasain).
Conflicts of interestsNone.












