



With the first European case of Ebola recently reported in Spain, the global spread of the virus 1 and the corresponding concern that this has caused, we consider the moment opportune to comment upon the current situation of malaria within the European Union (EU).
Malaria 2 is a life-threatening infectious disease caused by parasites (protozoa) of the Plasmodium genus, transmitted through the bite of the infected female Anopheles mosquito. The most common symptoms of malaria are high fever, headache, diarrhoea, chills and vomiting, which manifest themselves some 1-4 weeks after infection, whilst relapses due to Plasmodium vivax may occur months and in some cases, to 8 years later.
Globally, the World Health Organization (WHO) estimated that in 2012 about 207 million people (range: 135-287 million) were infected, with a resulting 627,000 deaths. In the majority of cases, 80% of the infections and 90% of deaths occurred in Africa, with children under 5 being the most affected.
Bearing this in mind, and in contrast to global data, malaria was designated as a rare disease in 2007 3 by the EU, which considers a rare disease to be a life-threatening or chronically debilitating condition which affects no more than 5 in 10,000 people in its territory.
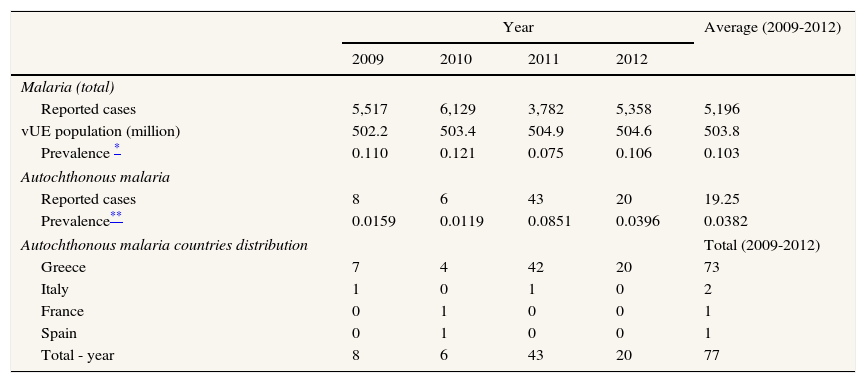
Table 1 shows the number of cases per year, between 2009 and 2012 and the prevalence frequency per 10,000 Europeans, which ranged from 0.121 to 0.075, with an average of 5,196 cases being reported. In addition, sporadic cases of autochthonous malaria have been reported in southern 4 European countries. Autochthonous malaria occurs when a human is infected in a malaria-free zone, which has been transmitted by a vector-borne (mosquito) from another human who has been previously infected from a malaria endemic or epidemic area.
Total malaria cases reported, prevalence of malaria per 10,000 Europeans citizen in the EU and autochthonous malaria cases reported.4
| Year | Average (2009-2012) | ||||
|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2012 | ||
| Malaria (total) | |||||
| Reported cases | 5,517 | 6,129 | 3,782 | 5,358 | 5,196 |
| vUE population (million) | 502.2 | 503.4 | 504.9 | 504.6 | 503.8 |
| Prevalence * | 0.110 | 0.121 | 0.075 | 0.106 | 0.103 |
| Autochthonous malaria | |||||
| Reported cases | 8 | 6 | 43 | 20 | 19.25 |
| Prevalence** | 0.0159 | 0.0119 | 0.0851 | 0.0396 | 0.0382 |
| Autochthonous malaria countries distribution | Total (2009-2012) | ||||
| Greece | 7 | 4 | 42 | 20 | 73 |
| Italy | 1 | 0 | 1 | 0 | 2 |
| France | 0 | 1 | 0 | 0 | 1 |
| Spain | 0 | 1 | 0 | 0 | 1 |
| Total - year | 8 | 6 | 43 | 20 | 77 |
The average rate of autochthonous malaria cases during the study period was 19.3 representing a prevalence of 0.0382 per million Europeans (Table 1). 94.8% of all reported P. vivax infections 4 were in Greece. The first 6 autochthonous malaria transmission cases appeared in 2009, in people who had no reported travel (or history of travel) to endemic areas. A further 3 reported cases occurred in 2010, with 40 more in 2011 and 8 in 2012.
In the spring of 2012 a specific plan4 against malaria was initiated by Greek Health Authorities in collaboration with the WHO and the European Centre for Disease Prevention and Control (ECDC). It is thought that for tourists and travellers to areas with indigenous cases, there is no motive for antimalarial chemoprophylaxis to be introduced but anti-mosquito measures do need to be followed.
In conclusion, it can be said that malaria remains a rare disease in the EU and, in the case of autochthonous malaria further action plans are being introduced to avoid its reintroduction and subsequent expansion. These results will be known after 2015.
Conflict of interestNone declared.
Author contributionsConceived the idea of the report: AO, JMR, MG. Extracted and analysed data: AO, JMR, MG. Wrote the paper: AO, JMR. All authors have seen and approved the final manuscript.
FundingNo funding has been received.











