




This paper assesses whether integrated care policy instruments, from a primary care perspective, improve care outputs and outcomes, identifying lessons for the Spanish National Health System (SNS).
MethodA scoping review of 18 reviews (systematic, scoping, narrative, and meta-analyses) focused on disease-agnostic integrated care instruments, including care coordination models, incentive structures, resource distribution, professional competencies, communication channels, and governance. Additional policy documents and studies referring to the SNS were also analysed.
ResultsOverall, the review identified studies addressing partial aspects of integrated care that frequently lacked robust methods to establish meaningful associations with care outcomes. Integrated care instruments were generally associated with modest improvements in service delivery and patient experience, with limited evidence of impact on health outcomes. Some instruments (multidisciplinary coordination, case management, and bundled payments) appeared more relevant, whereas others (resource distribution, use of information and communication technologies, professional training, or patient engagement) showed no consistent association. In Spain, strong regulatory instruments facilitated implementation but did not ensure a sustained transition from fragmented to integrated care. The development of fit-for-purpose information systems seems essential to support this transition, while the lack of publicly available data and independent evaluations limits understanding of the real impact of integrated care.
ConclusionsCurrent evidence does not confirm that integrated care leads to better health outcomes; however, some integrated care instruments may improve certain care outputs. To better inform decision-making, future studies should adopt multifaceted approaches and more robust methodologies.
Evaluar si los instrumentos de política de atención integrada, desde la perspectiva de la atención primaria, mejoran los productos y los resultados de la atención, e identificar lecciones para el Sistema Nacional de Salud (SNS) español.
MétodoRevisión de alcance de 18 revisiones (sistemáticas, de alcance, narrativas y metaanálisis) centrada en instrumentos de atención integrada independientes de la enfermedad, incluidos modelos de coordinación, estructuras de incentivos, distribución de recursos, competencias profesionales, canales de comunicación y gobernanza. Además, se analizaron documentos de política y estudios adicionales referidos al SNS.
ResultadosLa revisión identificó estudios que abordaban aspectos parciales de la atención integrada y que con frecuencia carecían de métodos robustos para establecer asociaciones significativas con los resultados de la atención. En general, los instrumentos de atención integrada se asociaron con mejoras modestas en la prestación de servicios y en la experiencia de los pacientes, con evidencia limitada sobre su impacto en los resultados de salud. Algunos instrumentos (coordinación multidisciplinaria, gestión de casos, pagos agrupados) mostraron mayor relevancia, mientras que otros (distribución de recursos, uso de tecnologías de la información, formación profesional y participación de los pacientes) no mostraron asociaciones consistentes. En España, los instrumentos normativos sólidos facilitaron la implementación, pero no garantizaron una transición sostenida de un modelo fragmentado a uno integrado. El desarrollo de sistemas de información específicos parece clave para apoyar esta transición, mientras que la falta de datos de acceso público y de evaluaciones independientes limita la comprensión del impacto real de la atención integrada.
ConclusionesLa evidencia disponible no confirma que la atención integrada mejore los resultados de salud, pero algunos instrumentos pueden favorecer mejoras en determinados productos de la atención. Para informar la toma de decisiones, los estudios futuros deberían adoptar enfoques multifacéticos y metodologías más robustas.
The National Health System of England National Collaboration for Integrated Care and Support states that for health, care and support to be integrated, it must be person-centred, coordinated, and tailored to the needs and preferences of the individual, their career and family.1 It means moving away from episodic care to a more holistic approach to health, care and institutional support, that puts the needs and experience of people at the centre of how services are organised and delivered. A similar vision is provided by The Nuffield Trust when describing the aim of integrated care as the effort to join up the health and care services required by individuals, to deliver care that meets their personal needs in an efficient way.2 Similar orientation is observed in New South Wales Health in Australia where involves the provision of seamless, effective, and efficient care that reflects the whole of a person's health needs.3 A similar perspective is offered by the World Health Organization (WHO), which describes integrated care as an approach aimed at strengthening person-centred health systems through the comprehensive delivery of quality services across the life course, tailored to the multidimensional needs of both populations and individuals, and coordinated across settings and levels of care by multidisciplinary teams.4
There is a general notion that integrated care (i.e., access to family- and community-oriented primary health care supported by a responsive hospital system) leads to better health outcomes.5 Beyond rhetoric, there is a general notion that this approach to integrated care leads to better health outcomes through care defragmentation. Indeed, in health systems with a strong reliance on regulated provision and primary care gatekeeping as Italy, Portugal, Spain or Sweden, potentially avoidable admissions for chronic conditions, those likely benefitting from integrated care, tend to be lower in international comparison; however, it is also true that countries as United Kingdom, with the same institutional design, do not follow the same pattern; and, on the contrary, systems as the Dutch, a system reliant on market mechanisms in service provision and ample capacity for patients to choose insurance, consistently exhibit very low rates of avoidable admissions.6
From a procedural perspective, integrated care is used to describe a connected set of clinical, organizational, and policy changes aimed at improving service efficiency, patient experience, and health outcomes. Hughes et al. identified four perspectives on integrated care.7 First, the concept of person-centeredness as the space to be recognised and heard, where patients take appropriate control of their own care. Second, strategies to integrated care that include change management (i.e., proactive, planned, preventive, self-managed), multidisciplinary working (i.e., health and social care collaboration, roles shifting), linking organizations (i.e., seamless technological coordination, multisite cooperation, overall care pathway accountability), and overall system approaches (i.e., universal primary care with gatekeeping roles, hospital centric, long-term care oriented). Third, models that range from linkages (referrals between services) through coordination (smoothing transitions between services) to full integration (into a single organizational body); and fourth, theoretical and critical analysis that comprises strategies to unify care and organizations, shaped by economic, political, and social contexts and subject to the governance and power relations.
The concept of integrated care is framed within a context of social justice, emphasizing that if equity is not prioritized, the integrated care model could perpetuate existing inequities instead of addressing them.8 Furthermore, recent studies highlight that even well-established integrated care models may fail to achieve equitable outcomes unless they are intentionally designed with equity in mind9. Whereas equity is recognized as a fundamental aspect of integrated care, an in-depth exploration of equity is beyond the intended scope and space of the current manuscript.
In this manuscript, we review relevant literature to shed light on whether integrated care can improve health outputs and outcomes. We use the term integrated care as a synonym for “coordinated care”, “transmural care”, “interprofessional care”, “seamless care”, “comprehensive care”, and “patient-centred care”. The paper aims to identify lessons for fostering integrated care in the Spanish National Health System.
MethodThis scoping review aimed to map the literature on integrated care policy instruments from a primary care perspective, classify them by conceptual domains, and identify available evidence on their effects on health outcomes.
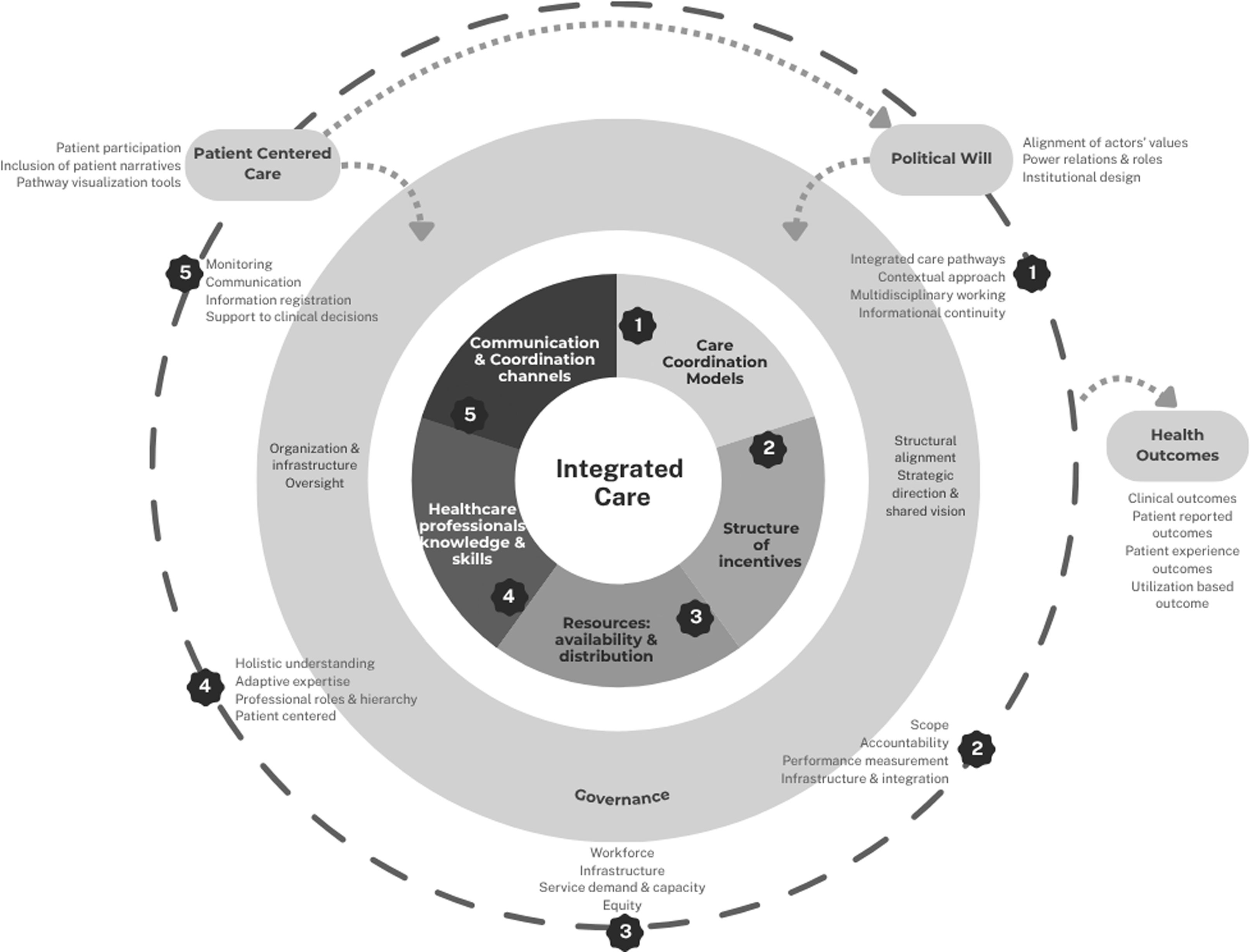
A conceptual map (Fig. 1) was developed, covering domains such as coordination mechanisms, incentive structures, resource distribution, professional capacities, communication channels, and governance, with political will and patient-related factors treated as cross-cutting drivers. The framework was refined inductively as new dimensions emerged during screening (Table S1 in Supplementary Material describes the dimensions of the conceptual map).

Searches were conducted in PubMed in April–May 2025 using the term “integrated care” combined with predefined analytical dimensions. Reference lists of included reviews were also screened. Reviews were eligible if they addressed integrated care instruments relevant to primary care or across care settings; disease-specific reviews were excluded. The process included a structured search and examination of academic, peer-reviewed publications. In addition, the review was informed by prior related work and the study team's expertise in integrated care. Three reviewers (AF, DV, DGA) screened titles and abstracts. Coauthors were assigned the topics for analysis; after literature revision, overlaps in scope, unclarity, and gaps in the retrieved information were jointly discussed. When information on a topic was missed, additional literature was searched. Given inconsistent reporting of impacts on health outcomes, relevance was determined by each review's conceptual contribution to understanding these relationships. Additional attention was paid to the depth with which political determinants were linked to integrated care implementation.
Data were charted according to the conceptual map and synthesised narratively. In line with scoping review methodology, no formal quality appraisal or meta-analysis was undertaken. 36 full-text papers were assessed for eligibility, while 18 papers were included in the review.
ResultsThis scoping review included 18 reviews (10 scoping reviews, 5 systematic reviews and 3 meta-analyses) for a total of 1037 individual studies (see Table S2 in Supplementary Material). The search yielded in addition one comparative secondary analysis, one realistic synthesis report, two policy papers, semistructured interviews and qualitative case-studies that, along with relevant papers within the reviews, were analysed apart to complement the analyses. No reviews were found addressing political will.
The most prevalent approach to study integrated care was narrative and partial. Evidence on the potential impact of integrated care on outputs and health outcomes was found to be scarce, and those studies aiming to show the effect suffered from methodological limitations and rarely sought to be generalisable.
Evidence on integrated care instrumentsGenerally, the literature analysed does not provide sufficient evidence on the effectiveness of integrated care policy instruments on improving health outputs and outcomes.
- 1)
Care coordination models
Knai et al.10 have described common challenges for the development of coordination in chronic care in Europe. The usual barriers include the focus on complications management, the lack of disease prevention and the care fragmentation within and between sectors. Other barriers include misalignment between overarching strategy and local capacity, as well as insufficient structures for patient participation in self-management. In turn, the authors suggest that successful chronic care coordination would require a patient-centered approach, engaging professionals to put policy into practice, elevating the roles of general practitioners and nurses, shared learning, integrating prevention, addressing inefficiencies, and a clearer political will.
According to Khatri et al.,11 effective care coordination depends on three key elements: 1) multidisciplinary collaboration bringing together various healthcare professionals to meet patient needs in a holistic way; 2) services integration across healthcare settings which entails information sharing and coordination across providers; and 3) management continuity within and beyond the system. Care coordination elements that were found to be effective in improving care outputs were interdisciplinary teamwork, communication and information exchange, shared care guidelines or pathways and training and education programs.
A model based on personalising care (i.e., case management approach) was also found to lead to improvements in certain long term care conditions such as diabetes, mental health, heart failure, renal disease, asthma, and multi-morbid patients, although just in some indicators of physical and psychological health status, and people's capability to self-manage. The effects were found not to be large, although they appeared to be larger when the intervention is more comprehensive, more intensive, and better integrated into routine care.12
- 2)
The structure of incentives: effect of payment typologies
Stokes et al.13 reviewed the typology of payments for integrated care in several European countries classifying the payment mechanism according to the scope of payment (i.e., target population, period covered, number of sectors), the participation of providers (i.e., provider coverage, financial pooling/sharing), and the provider/patient involvement (i.e., income, multiple needs, quality measurement). In addition, Yordanov et al.14 reviewed different types of financial incentives including bundled payments, pay for coordination, pay for performance, shared savings, gain sharing, and global budget capitation.
Evidence, although weak, tends to favour bundled payment approaches, in particular episode-based payments and shared savings.12. A study by Casale et al.15 compared bundled services for 117 patients in the intervention with those of 137 patients from a year prior to implementation of bundling and found that hospital costs dropped by 5%. The evaluation of first-year health outputs of Geisinger's ProvenCare coronary bypass program showed a 10% reduction in readmissions and shorter average length of stay. More recent data showed that over the course of 18 months, the program achieved a 44% drop in readmissions16.
Besides incentives intrinsic to the financial mechanisms, financial programmes should be well-communicated and easy to understand and implement by providers, require training, and guidance and must be supported by health information and communication technologies (ICT) and continuous monitoring quality and costs.12,14
- 3)
Resources availability and distribution
No evidence has been found addressing the association between resources availability or adequate distribution of resources and integrated care. Nonetheless, it is plausible to assume that integrated care may be affected by the uneven distribution or the shortage of professional resources; even more so in those, so named, “medical deserts” (areas where population healthcare needs are not fully met due to barriers access or improper quality of healthcare services caused by insufficient human resources17).
Articles in this revision identified several types of factors contributing to the development of “medical desserts”: work-related factors (for example, job dissatisfaction, burnout, fewer professional opportunities, limited access to other healthcare resources), lifestyle-related factors (for example, feelings of isolation, limited access to other desirable services such as internet or leisure activities, lack of anonymity), and socio-demographics and cultural factors (for example, not having a rural background or the lack of interest in primary care). Literature describes strategies that have been shown effective in the mitigation of medical desert effects. So, for example, undergraduate training focused on increased rural exposure, continuing medical education adapted to the scope of rural practice, and professional engagement based on economic incentives, better work scheduling, peer support, and availability of high-quality infrastructures and innovative services, such as tele-health.18
- 4)
Health professionals’ knowledge and skills
Barraclough et al.19 analysed health workforce developments fostering integrated care concluding that is often not well suited due to working silos and deficiencies in knowledge, skills, and attitudes towards integrated care, a lack of a deeper understanding of health and social care systems, and an approach that privileges treating the disease over a global management of the individual needs. In the specific case of the primary care workforce, key competencies needed in the management of person-centred integrated care include patient-centred communication, interprofessional collaboration, teamwork, and leadership. Specific communication skills would involve open dialogue, listening, and adapting to a patient's understanding. In turn, effective collaboration would require team members to know each other's roles and competencies, build trust and respect, and share language.20 A necessary step towards effective collaboration would be reducing the ambiguity and lack of consensus on the roles in care coordination and case management.21,22
Some solutions encompass the development of new academic programmes, competencies, and training models prioritising interprofessional education, and the facilitation of cross-professional learning opportunities in the workplace.17 All in all, workforce planning should shift to be patient-centred, addressing identified barriers, such as insufficient time for patient consultations, interprofessional collaboration, and unsupportive financial systems.18
- 5)
Communication channels
According to Tahsin et al.,23 ICT are potential instrumental enablers of integrated care; potential advantages are information sharing, self-management support, clinical decision-making, and remote service delivery, teamwork facilitation and services coordination.
Main digital health innovations currently used in European clinical practice include applications and platforms designed for monitoring diseases and managing common chronic conditions such as diabetes, cardiovascular issues, and chronic respiratory diseases. These tools are typically integrated with additional digital resources and are often supported by healthcare professionals. However, the effective use of ICT-based interventions depends on several implementation factors encompassing patient-provider relationship, technology interoperability, organizational support (funding, willingness), and the availability of information and technology support or care coordination roles. Studies with successful digital health interventions often involve organizational changes, suggesting that technology alone is not enough for improvement. Although digital literacy has improved, professional support remains essential in empowering patients in prevention and self-management in primary care.24
A recent meta-analysis by Ambrosi et al.25 assessed the effectiveness of digital health interventions against interventions without digital components implemented over the last 10 years in primary care settings for the management of chronic diseases. The findings are disappointing; out of the 23 studies included, most studies conducted in the United Kingdom and Spain, interventions based on patient monitoring, self-care education, and digital communication tools showed no significant differences with usual care in reducing hospitalizations, depressive symptoms, anxiety, glycated haemoglobin, diastolic blood pressure, weight, or quality of life.
- 6)
Inclusion of patients’ perspective
Patients’ perspective in integrated care encompasses, for example, the explicit inclusion of patient narrative, patient empowerment activities, shared-decision making and/or ICT co-design. Cassidy et al.,26 in a scoping review, meant to analyse approaches to include patients’ perspective in the care pathway found improved care coordination, enhanced quality of care, increased patient satisfaction, and better organizational and patient outcomes. More specifically, some studies demonstrated optimised resource utilization and increased efficiency by identifying process weaknesses and designing corrective measures; establishing standardized, shared pathways also improved communication and adherence among healthcare professionals, streamlined handovers and eliminated redundant work; and monitoring protocol deviations and failures facilitated early error identification, enhancing patient safety.
However, the strength of evidence was found to be limited and scarcely generalisable, likely due to the complexity of including patients’ perspective in real life. The development and implementation of the patients’ perspective in care pathways faces challenges such as the hardship of organisational change, time-consumption in everyday practice implying delays, and the need for staff cultural change and training in new roles.
Evidence on the impact of integrated care on care outputs and health outcomesRocks et al.27 found that integrated care had improved any health outcome (quality of life, quality-adjusted life-years, clinical outcomes, or mortality) with an overall ratio of mean outcomes of 1.06 (95% confidence interval [95%CI]: 1.05-1.08) compared with usual care, especially in studies with a follow-up period over one year; in turn, costs were found to slightly decrease (ratio: 0.94; 95%CI: 0.90-0.99). Similarly, Mitchell et al.28 and Jackson et al.29 although demonstrating a slight impact on clinical outcomes, integrated care was found to show substantial effects on service delivery measures at a modestly increased cost; thus, improvement in patient non-attendance rates in diabetes 14 percent points reduction in 12 months of follow up; reduction in service use in diabetic patients from 478.5 attendance rate to 361.6 in two years;30 24% relative reduction in heart failure re-admission rate as well as reduction in 200 bed days after re-admission in a year.31,32 Integrated care was also found effective in improving access perception in dermatology (15.6% difference) as well as a reduction in 41 days to first appointment.33,34 Yet, no significant differences were found in hospital and emergency presentations and prescribing patterns in chronic obstructive pulmonary disease (COPD)35 or in general practitioner consultations in heart failure.29,30
Baxter et al.36 did not find any effect of integrated care on intermediate outputs as prescribing rates, access to resources, number of general practitioner appointments, length of stay, unscheduled admissions, number of admissions, re-admissions, attendance at accident and emergency, quality of care standards, staff work experience, and cost of provision. Finally, studies involving primary care37 showed that integrated care interventions can have positive effects on strengthening some primary care functions, improving access (effect size: 0.17; 95%CI: 0.05-0.29) and continuity of care (effect size: 0.32; 95%CI: 0.14-0.50); however, no effect was demonstrated on wider outcomes such as quality of care, mortality and hospital admissions.
Specific studies carried out within the Spanish National Health SystemSome of the literature reviews in this paper included quasi-experimental studies assessing the impact of integrated care in care processes and outcomes within the Spanish Health System. A quasi-experimental study demonstrated that home care services that included nursing case management streamlined access to healthcare services and resources, while impacting positively on patients’ functional capacities and satisfaction.38 A quasi-experiment showed that community-based comprehensive nursing services prevented emergency visits and increased survival in stable frail community-dwelling COPD patients; underlying reasons for these results were appropriate risk-stratification and preparation of the health professionals, caregivers and patients for community-based services.39
While nurse case management is undoubtedly a positive and effective model for promoting patient-centred and coordinated care, it is worth questioning whether placing the weight of systemic fragmentation on a single professional profile, however traditionally and epistemically committed to integrated and patient-centred care, may risk oversimplifying a structural issue that demands the active engagement and responsibility of all healthcare professionals. In a different study, the use of a mobileHealth-enabled integrated care model for complex chronic patients empowering the patient, and connecting primary, hospital, and social care professionals reduced unplanned contacts with the health system and health costs and was cost-effective. The approach did not find statistical differences in the functional status of the patients.40
A study evaluating the impact of CareWell integrated care model for older patients with multimorbidity in the Basque Country found improvement in clinical intermediate outputs and reduction of emergency visits and hospitalisations, while primary care visits increased. The CareWell model was based on patient empowerment, home-support pathways and coordination between health providers supported by ICT tools.41
Finally, a randomized trial assessed the cost-utility of an intervention based on a reference internist and a liaison nurse, who aimed to improve continuity of care after hospitalisation. The intervention was not found efficient although it increased cost-utility in multimorbid patients younger than 80.42 A cost-effectiveness analysis built on a randomised controlled trial in which authors compared a collaborative care program with usual care for patients with musculoskeletal pain and depression did not show any improvement in quality-adjusted life years nor in incremental cost-effectiveness.43
DiscussionThis review of reviews, where integrated care was analysed from the perspective of primary care, sought to elicit evidence on the effect of different policy instruments on integrated care, as well as, on the association between integrated care and care process and health outcomes improvements. With the caveat of these results being based on limited evidence, generally built on studies with methodological flaws and restricted capacity for generalisation, care models seemed to be more effective when addressing integrated care in a comprehensive way, considering patients’ perspectives in usual care, and are funded using bundled episode-based schemes with shared-savings. For the rest of policy instruments (availability of resources, professional knowledge and skills, and communication channels) although it has been described plausible mechanisms towards better integrated care, there is no available evidence, or evidence was found to be weak or showed no association.
When it comes to the impact of integrated care on care processes and health outcomes, irrespective of the policy instruments, evidence is generally inconclusive. The literature revised showed contradictory findings and evidence varied widely. The heterogeneity in the conditions and processes analysed, and the measurements used to assess effectiveness do not allow drawing uniform conclusions.
Some lessons can be drawn out of those specific studies for our health system. The Spanish experience shows that isolated interventions, such as case management or ICT tools, are not sufficient unless embedded in broader, systemic reforms. Effective integration requires coordination across all levels of care, strong primary care leadership, and genuine patient empowerment. Importantly, political and institutional commitment at our multilevel governance framework is essential to move from successful pilots to sustainable, system-wide change.
LimitationsThis study included narrative, scoping, systematic reviews and meta-analyses where integrated care (and its synonyms) and the different policy instruments towards integrated care was the objective. Although the first intention was carrying a review of systematic review with meta-analyses, validating the hypothesis that integrated care was better than non-integrated care in many endpoints —process care outputs and health outcomes— the majority of evidence does not come from quasi-experimental designs. We tried to mitigate this fact, separately analysing those quasi-experiments carried out in the Spanish SNS.
Despite the extensive literature assessment, some knowledge gaps persist and will require further assessments; notably, the limited evidence found on the effect of some integrated care instruments (e.g., resources distribution, roles-shifting, application of eHealth and mHealth tools, inclusion of the patients’ perspective), the lack of quasi-experimental research at system-level, the absence of comparative research at meaningful levels of decision (i.e., comparison of integrated care implementation across health care areas and autonomous communities), or the lack of efficiency analysis from the societal perspective.
Policy lessonsThe reviewed evidence highlights that political will is a necessary condition for advancing integrated care, but not sufficient to produce the required cultural and organisational change, and therefore improve care process outputs or health outcomes. Indeed, Mur-Veeman et al.44 showed that although active government policies can foster integrated care, alignment with values (between professionals, but also between institutions) and sufficient resources are also needed. Their comparative analysis across European countries indicated that dynamics between actors (shaped by power relations, roles, and expectations) are conditioned by the broader architecture of the health system, other public administration sectors, and their governance. This last idea also developed in Martens et al.45 referred to the dispersion of authority across federal and regional levels that prevented sustainable care integration and hindered measurable improvements in coordination or efficiency. In turn, Borgermans et al.46 argued that integrated care requires not only high-level commitment but also disruptive innovation (deep structural reforms), adaptative models based on person-centred care and intersectoral collaboration.
Nicholson et al.47 identified as key elements for the governance of care integration: joint planning, integrated information and technology, change management, shared clinical priorities, incentives, population focus, data-driven quality improvement, continuous professional development, patient and community engagement, and innovation. Successful integration would in any case require political will, investment, risk-management and adaptive paths. Along the same lines, leadership is crucial for a successful integration, particularly between health and social care systems.48 Leaders must navigate complex environments and foster trust and collaboration, balancing inspiration with practical knowledge. Shared leadership is often more effective, with leaders prioritizing community needs while promoting innovation and learning despite current pressures. Despite this narrative, users’ and patients’ perspective, and policymakers’ views regarding the impact of integration and leadership benefits is currently lacking.
When it comes to the specific case of Spain, a recent Organisation for Economic Co-operation and Development and WHO report analysing the purchasing arrangements to strengthen the quality of chronic care in three Spanish Autonomous Communities assessed different policy instruments used to ensure integrated care.49 The successful implementation of purchasing instruments requires wide consensus and commitment from the main stakeholders, including health professionals and health systems managers. Strong regulatory instruments facilitate implementation, but do not guarantee sustainable change towards integrated care. The development of fit-for-purpose information systems is key to foster improvements in the quality of care. The lack of publicly available data and lack of independent evaluations impede full understanding of the programmes’ impact.
This literature review has highlighted the need for strengthening coordination between the health and social sectors. However, the knowledge gap on the actual impact of this coordination on care outputs and health outcomes is still scarce. The development of the 2025-2027 Action Plan of Primary and Community Health may well be an opportunity for the development of that intersectoral space, potentially evaluable, while filling in the lack of evidence.50
On a final note, the Spanish examples in this review highlight the need for strengthened governance in the evaluation of integrated care interventions within our health system. Advancing towards high-quality, people-centred care calls for shared research frameworks, appropriate methodologies and outcome measures, and structured mechanisms for reporting and learning from implementation. A more consistent and evidence-informed evaluation approach will be key to ensuring that integrated care efforts are effective, scalable, and responsive to the needs of patients, caregivers, and professionals alike.
Availability of databases and material for replicationThe data underlying this study are available from the lead author upon reasonable request.
Editor in chargeSalvador Peiró.
Authorship contributionsAll the authors contributed equally in the design, execution and final approval of this manuscript.
FundingNetwork for Research on Chronicity, Primary Care, and Health Promotion (RICAPPS), Spain Grant numbers RD24/0005/0005; RD24/0005/0014; RD24/0005/0019; RD24/0005/0020.
Conflicts of interestNone.












