






In the context of the Health4EUKids Joint Action, this study aims to outline the current state of policies and programs related to children's obesity prevention, health promotion, and responsive parenthood for children aged 0-12 years across participating European Union Member States, and to identify gaps.
MethodA cross-sectional survey was conducted between October and December 2023, exploring the main dimensions of the questionnaire: policies and programs general information, target groups and settings, key characteristics, formulation and design, implementation, monitoring and evaluation, dissemination, and inclusion of evidence-based actions. All European Union Member States participating in the Joint Action were invited to respond, and responders were professionals holding key roles in public health, health system governance, and policy implementation. Descriptive statistical analyses were used to summarize quantitative data on policies and programs across countries, while a qualitative descriptive approach was applied to open-ended responses.
ResultsThe survey collected data on 79 policies and programs from 12 European Union Member States. Most policies and programs focus on healthcare (63%), education (25%), and social sectors (10%), targeting primarily children aged 6–11 years. The settings include primary schools, communities, and health services. An inter/multi-sectoral approach was reported in 92% of policies and programs. Policies and programs show varying degrees of innovation, controversy, equity, transferability, and sustainability, while systemic impact and public visibility appear less frequent. The formulation and design of policies and programs included problem analysis in 80%, based on national or local data (79%) and stakeholders’ consultation (79%). Implementation was indicated for most policies and programs (59%), though funding (41%), human resources (29%), stakeholder engagement (46%), and structured planning (46%) appeared relatively strong. Monitoring frameworks were present in 68%, but only 52% reported regular indicator tracking. Dissemination to decision-makers (43%) and the public and media (37%) remains limited.
ConclusionsThe Health4EUKids Joint Action offers valuable insights into childhood obesity prevention policies across European Union Member States, revealing both promising practices and persistent gaps. Despite strong multisectoral commitment, challenges remain in implementation, monitoring, and resource allocation. Addressing these challenges requires sustained investment in integrated, equity-oriented, and context-sensitive strategies to empower children, families, and communities and to support long-term public health goals.
En el contexto de la Joint Action Health4EUKids, este estudio tiene como objetivo describir el estado actual de las políticas y los programas relacionados con la prevención de la obesidad infantil, la promoción de la salud y la parentalidad sensible en la infancia de 0 a 12 años en los Estados miembros de la Unión Europea participantes, e identificar las brechas existentes.
MétodoSe realizó una encuesta transversal entre octubre y diciembre de 2023, explorando las principales dimensiones del cuestionario: información general de las políticas y los programas, grupos objetivos y entornos, características clave, formulación y diseño, implementación, monitorización y evaluación, difusión e inclusión de acciones basadas en la evidencia. Se invitó a responder a todos los Estados miembros de la Unión Europea participantes en la Joint Action; los encuestados fueron profesionales con roles clave en salud pública, gobernanza del sistema sanitario e implementación de políticas. Se realizaron análisis estadísticos descriptivos para resumir los datos cuantitativos sobre las políticas y los programas en los distintos países, y se aplicó un enfoque cualitativo descriptivo a las respuestas abiertas.
ResultadosLa encuesta recopiló datos sobre 79 políticas y programas procedentes de 12 Estados miembros de la Unión Europea. La mayoría de las políticas y de los programas se centran en los sectores sanitario (63%), educativo (25%) y social (10%), dirigidos principalmente a niños de 6 a 11 años. Los entornos incluyen escuelas primarias, comunidades y servicios de salud. Un enfoque inter/multisectorial fue reportado en el 92% de las políticas y de los programas. Las políticas y los programas muestran grados variables de innovación, controversia, equidad, transferibilidad y sostenibilidad, mientras que el impacto sistémico y la visibilidad pública parecen menos frecuentes. La formulación y el diseño de las políticas y los programas incluyeron análisis del problema en el 80%, basándose en datos nacionales o locales (79%) y en consultas con actores clave (79%). La implementación fue indicada para la mayoría de las políticas y los programas (59%), aunque la financiación (41%), los recursos humanos (29%), la participación de actores clave (46%) y la planificación estructurada (46%) se consideraron relativamente sólidos. Los marcos de monitorización estuvieron presentes en el 68%, pero solo el 52% informó un seguimiento regular de indicadores. La difusión a los responsables de la toma de decisiones (43%) y al público y los medios de comunicación (37%) sigue siendo limitada.
ConclusionesLa Joint Action Health4EUKids ofrece información valiosa sobre las políticas de prevención de la obesidad infantil en los Estados miembros de la Unión Europea, revelando tanto prácticas prometedoras como brechas persistentes. A pesar del fuerte compromiso multisectorial, persisten desafíos en la implementación, la monitorización y la asignación de recursos. Abordar estos retos requiere una inversión sostenida en estrategias integradas, orientadas a la equidad y sensibles al contexto, que empoderen a niños, familias y comunidades, y que apoyen los objetivos de salud pública a largo plazo.
Overweight and obesity represent a significant global public health challenge, especially among children.1–3Worldwide, childhood obesity has risen sharply over the past decades, with prevalence quadrupling among children and adolescents aged 5-19 years.4
Data from the WHO European Childhood Obesity Surveillance Initiative (COSI) show that in several Member States (MS), almost 40% of boys aged 7–9 years were living with overweight and almost 20% with obesity in 2015–2017.5 The burden of disease is also higher among children from low-income families. Furthermore, the prevalence of overweight and obesity and/or mean body mass index has increased in children and adolescents during the COVID-19 pandemic.6–9Overweight and obesity are risk factors for noncommunicable diseases (NCD) in the World Health Organization (WHO) European Region.6
Childhood obesity has well-documented long-term consequences, since children with obesity are very likely to become adults with obesity and to develop obesity-related NCD. It also contributes to an earlier onset of several chronic diseases. Moreover, childhood and adolescent obesity can entail significant psychosocial consequences for children's quality of life and academic performance, as these individuals are at increased risk of experiencing discrimination, bullying, and weight-related stigma from their peers.10
Addressing this global health challenge requires a multidimensional approach that spans individual lifestyle choices, family support systems, institutional policies, and broader environmental influences, and should be grounded in a clear conceptual framework. The WHO Commission on Ending Childhood Obesity (ECHO) conceptual framework provides a comprehensive structure, viewing childhood obesity as the result of interacting biological, behavioral, environmental, and societal drivers across six interconnected action areas. This framework helps organize the multiple determinants involved and underscores the need for coordinated, multisectoral strategies.11 Social and health inequalities play a significant role in obesity prevalence, with disadvantaged populations experiencing higher risks due to limited access to nutritious foods, safe physical environments, and healthcare resources.12,13
Given the substantial health, social, and economic consequences of childhood obesity, it has become a strategic priority for international and European institutions.14–16Recent European initiatives, such as the European Union (EU) NCD Initiative and Europe's Beating Cancer Plan, highlight the need for integrated health promotion, disease prevention, and policy interventions to tackle obesity effectively. These efforts emphasize not only personal behavioural change, such as diet and physical activity, but also structural modifications in food systems, urban planning, education, and social equity to create healthier environments.14,15,17,18 Particular attention must be given to childhood obesity prevention, which requires multisectoral interventions in various settings (schools, families, healthcare facilities, and communities) and must engage a broad spectrum of stakeholders, including policymakers, educators, healthcare professionals, third sector, non-governmental organizations, and industry partners.16,19,20 Early-life interventions, with a Nurturing Care approach, combined with long-term policy changes, are crucial to addressing the root causes of obesity and its life-course implications.19–22 Indeed, childhood obesity prevention efforts need to start early, from pregnancy to childhood, and be tightly integrated with other measures to control all significant NCD risk factors.16
Halt the rise in diabetes and obesity between 2010 and 2025 is a target in the WHO Global Action Plan for the Prevention and Control of NCD 2013–2020,23 then extended by 2030.24 Furthermore, overweight, obesity, and malnutrition in all their forms are part of the Sustainable Development Goals to ensure health and well-being for all.25
In this context, the Health4EUKids Joint Action (Health4EUKids JA) was established to support childhood obesity prevention and health promotion across European MS. The Health4EUKids JA is a three-year European initiative launched in February 2023 within the EU4Health Programme 2021–2027, focusing on promoting health and preventing NCD, particularly childhood obesity. Coordinated by Greece and involving multiple European countries, it supports childhood obesity prevention by implementing, transferring and scaling up evidence-based best practices. A key component of Health4EUKids is the adaptation and dissemination of two pretested best practices: Grünau Moves (owned by Germany, coordinated by Spain as Work Package 5 Leader),26 and Smart Family (owned by Finland, coordinated by Finland as Work Package 6 Leader).27 The project also prioritizes policy development to encourage public health investments in disease prevention and management.28
Effective childhood obesity policies and programs (P/P) require clear formulation, adequate resources, multisectoral coordination, structured implementation plans, and robust monitoring and evaluation mechanisms. Mapping these elements across EU countries is essential to identify strengths, gaps, and opportunities for improvement, providing evidence to guide future policy action.29
This study aims to outline the current state of P/P related to children's obesity prevention, health promotion and responsive parenthood for children aged 0-12 years across the participating EU MS. It examines their role as enablers of best practices and identifies existing gaps in the effective implementation of health promotion and childhood obesity prevention actions.
MethodStudy design and settingA cross-sectional study was carried out through a survey, as part of the Health4EUKids JA.
The sampling frame included EU MS involved in the Health4EUKids JA: Belgium, Croatia, Finland, Greece, Hungary, Italy, Lithuania, Malta, Poland, Portugal, Slovenia and Spain.
Among the MS involved, the survey was conducted by the Italian National Institute of Health (Istituto Superiore di Sanità – ISS), National Centre for Disease Prevention and Health Promotion, as part of the activities of Work Package 4 “Transferability and sustainability”, which it coordinates for Italy.
The survey was conducted between October and December 2023.
Participants and responder identificationParticipants were identified among the JA partners and key stakeholders in each MS. As the coordinating institution, the ISS contacted the representatives of the consortium who had signed the Grant and the Consortium Agreement. Each country then organised the completion of the survey by involving its own relevant contacts. For countries with federal or decentralized governance systems, where public health responsibilities are shared, national and sub-national authorities were allowed to respond independently; therefore, separate entries were collected when applicable. Inclusion criteria for responders included individuals holding key roles in public health and health system governance, research, and policy implementation. These encompassed professionals from national and regional public health institutions, governmental bodies, academic and biomedical research institutes, and public administration, such as senior advisers, policy coordinators, researchers, public health officers, and specialists in health promotion and disease prevention. To allow multiple stakeholders to contribute, the survey file could be completed multiple times by different individuals if a review by colleagues or other entities was deemed necessary. Depending on national organisation, contact points either circulated the questionnaire to relevant institutions and professionals, or coordinated joint completion through internal meetings. This approach ensures a broader and more comprehensive description of the information provided. A questionnaire was completed for each P/P described. Non-responders MS received reminder emails two and six weeks after the initial invitation.
Survey developmentThe questionnaire was specifically developed for this study within the framework of Work Package 4 of the Health4EUKids JA. It was developed by the Work Package 4 coordination team, composed of public health researchers with expertise in health promotion and disease prevention. Its development was informed by key international frameworks and guidance documents relevant to childhood obesity prevention and public health policy.11,15,17,18,31 Content validity was ensured through a review involving public health experts from EU MS participating in the JA, as well as additional external specialists. The tool underwent internal piloting within the Work Package 4 team to assess clarity, consistency, technical functionality, and completeness, leading to minor revisions before dissemination.
Tool variablesThe survey questions included closed-ended formats (single choice, multiple choice, Likert scale) and open-ended questions. The questionnaire explored several dimensions for each P/P, including:
- •
Sector (health, education, social; multiple choice questions).
- •
Level (national/federal or subnational; single choice question).
- •
Multi-, inter-, or trans-sectorality approach (single choice question).
- •
Targeting and setting (multiple choice question).
- •
Characteristics (degree of innovation, degree of controversy, structural or systemic impact, equity dimension, public visibility, transferability, sustainability; 5 points Likert scale).
- •
Formulation, design and endorsement of politicians and stakeholders in planning (multiple choice questions).
- •
Implementation and management (yes; yes, partially; no; not applicable).
- •
Human resources, technology, and information systems (yes; yes, partially; no; not applicable).
- •
Monitoring, evaluation, and dissemination (yes; no; not applicable).
- •
A set of evidence-based actions (n. 29) on disease prevention, health promotion, and responsive parenthood for children aged 0-12 years (5 points Likert scale for each action to determine the extent to which it was included in the described P/P).
- •
A final open-ended question explored the gaps in P/P's evidence-to-practice alignment and implementation, identifying strengths and facilitators, as well as weaknesses and barriers in the collected P/P.
To establish a common understanding of the key concepts addressed in the questionnaire, a series of definitions was provided, including national policy, national program, subnational level, and children's 0–12 obesity prevention, health promotion, and responsive parenthood. A description of these key concepts and the full questionnaire (text format) is available in Appendix A and Appendix B on Supplementary data.
Data collection and data analysisSurvey responses were recorded in an electronic data sheet. The data analysis was conducted using STATA 17 software. A qualitative descriptive approach was used for the open-ended questions, coded inductively and deductively, according to a categorical analysis,30 using Nvivo software. The STROBE checklist was used for reporting applicable items.31
Ethical considerationsEthical approval was obtained from the Bioethics Committee of the University of Patras and the Regional Directorate of Primary and Secondary Education of Western Greece (approval number:304; date:26/10/2023).
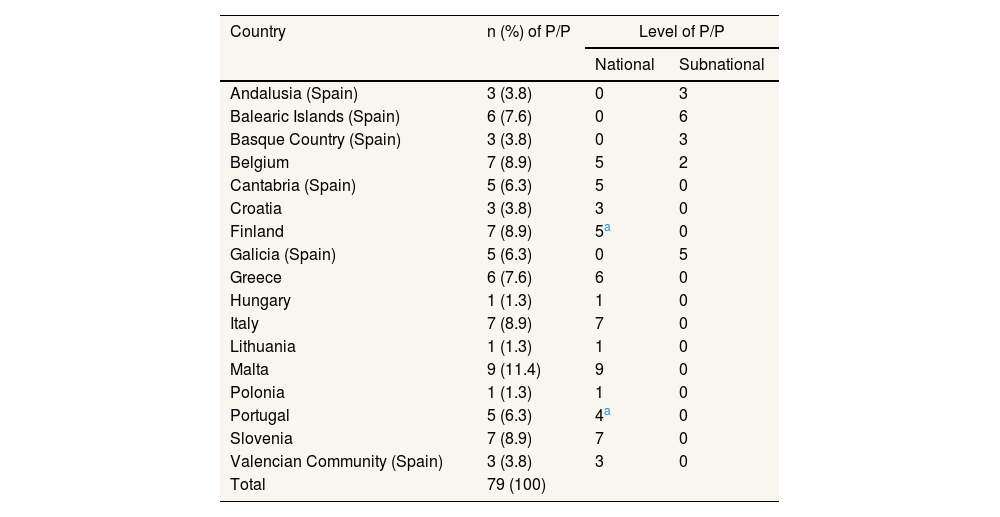
ResultsPolicies and programs context and general informationFrom October to December 2023, information was collected on 79 P/P from 12 EU MS participating in the Health4EUKids JA. Responses were received from all participating MS, achieving a 100% response rate (Table 1).
Policies and programs reported by EU JA Health4EUKids Member States, by country and governance level.
| Country | n (%) of P/P | Level of P/P | |
|---|---|---|---|
| National | Subnational | ||
| Andalusia (Spain) | 3 (3.8) | 0 | 3 |
| Balearic Islands (Spain) | 6 (7.6) | 0 | 6 |
| Basque Country (Spain) | 3 (3.8) | 0 | 3 |
| Belgium | 7 (8.9) | 5 | 2 |
| Cantabria (Spain) | 5 (6.3) | 5 | 0 |
| Croatia | 3 (3.8) | 3 | 0 |
| Finland | 7 (8.9) | 5a | 0 |
| Galicia (Spain) | 5 (6.3) | 0 | 5 |
| Greece | 6 (7.6) | 6 | 0 |
| Hungary | 1 (1.3) | 1 | 0 |
| Italy | 7 (8.9) | 7 | 0 |
| Lithuania | 1 (1.3) | 1 | 0 |
| Malta | 9 (11.4) | 9 | 0 |
| Polonia | 1 (1.3) | 1 | 0 |
| Portugal | 5 (6.3) | 4a | 0 |
| Slovenia | 7 (8.9) | 7 | 0 |
| Valencian Community (Spain) | 3 (3.8) | 3 | 0 |
| Total | 79 (100) | ||
P/P: policies and programs.
The level of P/P described has been predominantly national (69%). The primary sectors covered by P/P are healthcare (63%), followed by the educational (25%) and social sectors (10%). An inter/multi-sectoral approach has been reported in 92% of the P/P.
Policies and programs target and settingsThe primary target of the relevant age groups for P/P is children aged 6-11 years, constituting 78.1%. This is followed by children 3-5 years (75%), family/parents (66%), infant aged 0-2 years (60%), pregnancy-childbirth-breastfeeding (44%), general public/civil society (43%), local authority (37%), academia and professional organizations (33%), non-governmental organizations/associations (29%), food manufacturers and producers (29%), and media (23%). The settings of P/P included primary school (66%), community (63%), secondary school (59%), community health service (56%), pre-school (52%), municipalities (33%), hospitals (33%), and workplace (25%).
Policies and programs key characteristicsThe survey assessed several characteristics of the P/P, including innovation, controversy, systemic impact, equity, public visibility, transferability, and sustainability (Fig. 1). Regarding the degree of innovation, responses varied, showing a trend towards higher innovation levels, with 34.8% of respondents rating the P/P as highly innovative. About half of the responses (49%) described the P/P as highly consensual, while a significant portion (40%) assessed the structural or systemic impact as moderate. The equity dimension was deemed a fundamental aspect in many P/P (49%), while public visibility scores were distributed, with 28% rating it as high. The transferability of P/P was rated predominantly high, with 44% selecting 5 and 35% choosing 4. Sustainability ratings were largely positive, with 36% rating it as strongly sustainable.
Policies and programs formulation and design
The formulation and design of P/P included problem analysis in 80%, based on national or local data (79%) and stakeholders’ consultation (79%).
Regarding the types of stakeholders involved in the planning process, the primary stakeholders involved include scientific societies (30%), followed by community associations (15%), the public (13%), the third sector (10%), and non-governmental organizations (9%). About 23% reported that other stakeholders were involved in the comments, related for example to food producers or the agriculture sector, politicians, or independent experts.
Policies and programs implementationAbout the implementation of P/P, the survey results indicate that 59% of P/P have been implemented. Adequate financial and human resource support remains a challenge, with only 41% confirming sufficient funding and 29% adequate human resource allocation. Stakeholders’ involvement appears relatively strong, with 46% confirming active participation. Regarding institutional support, 55% of P/P were endorsed by relevant agencies and stakeholders, but structured implementation planning is less prevalent, with only 46% confirming the existence of a binding plan (Fig. 2).
Policies and programs monitoring and evaluation
Regarding monitoring and evaluation of P/P, most respondents (68%) confirmed that a set of outcomes, standards, and indicators has been defined, while 23% reported the absence of such frameworks. However, the systematic measurement of indicators remains less prevalent, with only 52% confirming regular monitoring. A notable 30% stated that indicators are not measured regularly, and 17% considered it not applicable.
Policies and programs disseminationThe results indicate that dissemination of P/P implementation findings remains inconsistent. While 43% of respondents confirmed that results have been communicated to decision-makers and stakeholders, 34% reported that this has not occurred. Similarly, the dissemination of results to the public and media is even less common, with only 37% affirming that communication has taken place.
Policies and programs evidence-based actions includedThe analysis of the evidence-based actions selected reveals significant variability in their level of implementation within P/P (see Appendix C in Supplementary data). Breastfeeding promotion and skin-to-skin contact show relatively better implementation rates (29% fully and 18% partially implemented), while in the school setting, nutrition education (40%), school meal composition control (36%), and physical activity promotion (41%) reached moderate levels, but screen time control (22%) and monitoring of unhealthy product marketing (13%) remain underdeveloped. The most successfully implemented school interventions include life skills promotion (63%) and supporting student participation and inclusion (57%). In the community, networking across sectors (69%) and active family involvement (62%) show the highest levels of implementation, while mental health and emotional well-being support (80% not implemented), peer-to-peer support groups for parents (23%) and culturally sensitive actions (46%) remain limited.
Policies and programs qualitative insightsFrom the analysis of the open-ended questions (see Appendix D in Supplementary data), it emerges that health policy and programs face several challenges, including outdated data, limited resources and difficulties in monitoring and coordination. Although several P/P are based on strong scientific evidence and aim at a comprehensive approach to health, problems such as insufficient funding, lack of cultural sensitivity and reliance on self-reported data hamper their effectiveness. Several challenges need to be addressed to improve the effectiveness and sustainability of health P/P, ensuring better public health outcomes.
DiscussionThis cross-sectional study, conducted across 12 EU MS as part of the Health4EUKids JA, provided an in-depth overview of the diversity and complexity of P/P dedicated to childhood obesity prevention, health promotion, and responsive parenthood. Based on the analysis of 79 P/P, primarily developed at the national or federal level, the findings highlighted a significant uptake of multisectoral approaches involving the health, education, and social sectors. These efforts reflect both the strengths and the ongoing challenges of current initiatives and are aligned with global and European policy priorities promoting integrated public health responses to NCD. A key strength emerging from the analysis was the widespread adoption of multisectoral approaches, present in 92% of the P/P. The high level of cross-sector collaboration, particularly among the health, education, and social sectors, including the third sector, community associations and non-governmental organizations, facilitated the implementation of evidence-based actions. It also aligns closely with international frameworks, including the EU NCD Initiative and Europe's Beating Cancer Plan, which advocate for integrated, whole-of-society, life-course strategies to prevent NCD, especially among vulnerable populations.18 Data from the previous CHRODIS-PLUS Joint Action highlights the complexity of achieving genuine cross-sectoral participation in policy-making and programme planning; however, this challenge now appears to be a well-established aspect of the health promotion policies analysed.32
Most P/P prioritized primary school-aged children and family-focused interventions, with schools, communities, and health services emerging as the dominant and interrelated settings. This pattern corresponds with literature indicating that multifaceted, community- and school-based interventions are more effective than single-setting approaches. Schools, communities, and health services are widely recognized as key leverage points for public health intervention, with evidence from the STOP project and WHO reviews showing that school-based programs targeting physical activity, healthy eating, and behavioural change can contribute meaningfully to weight status improvements in children.17,33–36 Viewed in light of the WHO Commission on ECHO framework, which identifies six interconnected action areas —e.g. healthy food environments, physical activity environments, early-life nutrition, health services and clinical management, governance and leadership, and monitoring and surveillance—, these patterns suggest that actions related to healthy diets and physical activity are more easily integrated within established institutional settings, whereas early-life and family-oriented components, which require stronger system capacity and coordinated pathways, tend to be implemented less consistently across countries.11
Although equity was explicitly addressed in nearly half of the P/P analysed, this proportion highlights the need for further commitment. Children from low-income families and marginalised communities are particularly vulnerable to obesogenic environments and often face structural barriers to access health-promoting resources and services.5 Evidence shows that (individually-based) interventions are less effective in disadvantaged settings unless they are socially and culturally adapted.35,37 Mainstreaming health equity in childhood obesity prevention, through targeted outreach and adapted interventions, remains a critical step to ensure that actions do not widen existing gaps. Evidence from WHO ECHO reviews indicates that early-life and family-based components, which are crucial for reducing inequities, are also among the least implemented and most resource-dependent, contributing to persistent gaps in vulnerable populations.11 Facing the challenges of social and commercial determinants of health in children and caregivers requires adopting a model of proportionate universalism, that is, universal policies and actions that are implemented with a scale and intensity proportionate to the level of disadvantage.38 This approach ensures that interventions do not merely benefit those already better off, but instead actively work to flatten the social gradient in health and prevent the Matthew Effect, namely the tendency for public health interventions to disproportionately benefit more advantaged groups, thereby unintentionally widening existing health inequalities.39
Another promising result was the reported high degree of innovation and consensus, this latter indicating that most P/P were seen as widely accepted rather than divisive, while structural or systemic impact remained uneven. Only a minority of P/P were perceived as having high public visibility, indicating a possible gap in public engagement and communication. This observation aligns with previous calls for stronger advocacy and media strategies to shift public norms and increase awareness of children's right to healthy lifestyles.15 The implementation of interventions was highly variable. Some policies were fully implemented, while others remained partial or theoretical. Barriers included insufficient human and financial resources, cultural mismatches with target populations, and gaps in data infrastructure. Although evaluation frameworks were often defined, consistent and structured monitoring practices are also lacking. The lack of systematic monitoring hampers the ability to assess real-time effectiveness and make timely policy adjustments. The development of more robust, standardized monitoring systems is essential to regularly measure relevant indicators and intervention impact.
Regarding evidence-based actions, some were more frequently integrated into P/P, while others were only marginally addressed, e.g. measures aimed at counteracting the marketing strategies of breastmilk substitutes and baby food were included in only 17% of cases.40 As part of the Health4EUKids JA, this study provided an opportunity to review the P/P within which the best practices Grünau Moves and Smart Family are implemented for childhood obesity prevention. The multi-stakeholder, multisectoral, multisetting, co-creation approach underpinning the P/P analysed appeared promising for the successful transferability of these best practices, aiming to provide replicable models for sustainable, context-sensitive interventions across MS. These findings align with the implementation challenges and contextual specificities explored in the CHRODIS-PLUS Joint Action. Barnfield et al. examined the transferability of good practices in health promotion across EU MS, highlighting the critical role of local context, stakeholder involvement, and a structured implementation framework in adapting effective practices to new environments.41
A final reflection concerns the nature of health promotion interventions, which are inherently long-term processes grounded in the enhancement and empowerment of individuals and communities.42 The analysed P/P incorporated several WHO Best Buys defined as evidence-based and highly cost-effective interventions for the prevention and control of noncommunicable diseases, targeting major risk factors such as unhealthy diet, physical inactivity, tobacco and alcohol use.17 Indeed, both the Grünau Moves and Smart Family best practices encompass such interventions. Health promotion is a slow and sustained process, which differs significantly from the more recent Quick Buys approach, which refers to a subset of cost-effective interventions capable of demonstrating measurable population-level health impacts within a short timeframe (≤5 years), often aligned with political and electoral cycles.43 The latter, by its very nature focused on achieving rapid, measurable, and cost-effective outcomes, may be less suited to fostering meaningful empowerment among families and communities, and is therefore more appropriate for regulatory, fiscal or single-sector interventions, while long-term, multisectoral health promotion strategies remain essential for sustainable behavioural change.45 This study has some limitations. The P/P analysed might not be exhaustive of those existing in each country and, in some cases, reflect the selection made by respondents. Moreover, the responsibility for completing the survey was delegated to the JA partners, leading to variability in the involvement of stakeholders and policy makers across countries. Furthermore, as P/P were also collected from federal or decentralized countries, the number of P/P reported varied substantially across MS: some countries reported only one P/P, whereas others (e.g. Spain) reported a much higher number, a pattern partly influenced by countries with multi-level governance systems, where both national and regional P/P may be developed. This heterogeneity in national contributions may have influenced the comparability of the findings and introduced a potential sample bias.
Although not without areas for improvement, the analysed P/P provide a solid foundation for the successful and sustainable transfer of best practices, ensuring that implementation efforts are context-sensitive, equity-oriented, and capable of generating lasting impact across MS. Framing our findings within the WHO ECHO framework also helps identify areas where future policies could be strengthened, especially those requiring more sustained and coordinated system capacity.11
ConclusionsThe Health4EUKids JA provides valuable insights into the current landscape of childhood obesity prevention P/P across EU MS. This study highlights both promising practices and persistent challenges. While many policies demonstrate a strong commitment to multisectoral collaboration and evidence-based interventions, gaps remain in implementation, monitoring, and resource allocation. Addressing these issues requires a sustained investment in integrated, equity-oriented, and context-sensitive approaches, capable of empowering children, families, and communities. Strengthening these foundations is key to advancing public health goals and securing healthier futures for the next generation.
Availability of databases and material for replicationData made available to those who request it.
Childhood obesity is a major public health issue in Europe, linked to inequalities and calling for multisectoral prevention strategies.
What does this study add to the literature?The study maps 79 policies and programs in 12 EU Member States, highlighting multisectoral approaches but also gaps in implementation, monitoring, resources, and visibility.
What are the implications of the results?The results highlight the need for integrated, equity-oriented, sustainable and transferable strategies, showing how policies support obesity prevention and where gaps hinder implementation.
Jorge Marcos.
Transparency declarationThe corresponding author, on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsA. Giusti and C.C. conceptualized the study. A. Giusti and V. Di Stefano wrote the main manuscript text. A. Giusti, V. Di Stefano, P. Scardetta and F. Zambri collected and analyzed the data. V. Palermo, A. Di Nolfi, F. Splendore, A. Vantarakis, G. Karydas, P. Csizmadia, M. García-Sierra, P. Mäki and C. Cattaneo contributed to manuscript revision. All authors reviewed and approved the manuscript.
Conflicts of interestsNone.
FundingThis work was supported by the Health4EUKids Joint Action, co-funded by the European Union and the Health and Digital Executive Agency (HaDEA) as part of the EU4Health program (Project ID n.101082462).
We would like to express our sincere gratitude to all individuals from the Member States involved in the Health4EUKids Joint Action for their participation and valuable contributions to the survey. We also wish to thank the team providing technical and administrative support: Eva Appelgren, Roberta D’Angelo, Arianna Dittami, Gabriella Martelli, and Sabrina Sipone (Health4EUKids Work Package 4).
Health4EUKids working group: Vasiliki Iliopoulou, Eleni Papachatzi, Emmanuella Magriplis, Lamprini Lachanioti, Kyriaki Premtou (Health4EUKids Work Package 1 and 2); Zsófia Kimmel (Health4EUKids Work Package 3); Esther Gonzalez María, Laura Albornos Muñoz; Gil Luciano Ana; Rosana Peiro Pérez, Ana Boned Ombuena, Joan Quiles Izquierdo, Jaime Jiménez Pernett, Guadalupe Longo Abril, Pablo García Cubillana, Maria Ramos Monserrat, Catalina Núñez Jiménez, Trinidad Planas Juan, Elena Cabeza Irigoyen, Biosistemak, Ines Urieta, Amaia Mentxaka Etxebarria, Irati Erreguerena Redondo, Jessie Van Kerckhove, Stefanie Vandevijvere, David Cantarero Prieto, Oliver Ramos-Álvarez, María Jesús Cabero, Paloma Lanza León, Javier Lera Torres, Marina Barreda Gutiérrez, Silvia Suárez Luque, Carolina Muñoz Ibáñez, Sharon Vella, Paula Vassallo, Mariella Borg Buontempo, Miguel Telo de Arriaga, Leonor Quelhas Pinto (Health4EUKids Work Package 5); Heli Kuusipalo, Emma Koivurinta, Nella Savolainen, Kati Kuisma, Taina Sainio (Health4EUKids Work Package 6).

Questionnaire key concepts.

Questionnaire (text format).

Evidence-based actions included in P/P.

Overview of the qualitative analysis of open-ended responses: policy gaps, strengths and facilitators, and weaknesses and barriers of policies and programs.
Vasiliki Iliopoulou, Eleni Papachatzi, Emmanuella Magriplis, Lamprini Lachanioti, Kyriaki Premtou (Health4EUKids Work Package 1 and 2); Zsófia Kimmel (Health4EUKids Work Package 3); Esther González María, Laura Albornos Muñoz, Ana Gil Luciano, Rosana Peiró Pérez, Ana Boned Ombuena, Joan Quiles Izquierdo, Jaime Jiménez Pernett, Guadalupe Longo Abril, Pablo García Cubillana, María Ramos Monserrat, Catalina Núñez Jiménez, Trinidad Planas Juan, Elena Cabeza Irigoyen, Biosistemak, Inés Urieta, Amaia Mentxaka Etxebarria, Irati Erreguerena Redondo, Jessie Van Kerckhove, Stefanie Vandevijvere, David Cantarero Prieto, Oliver Ramos-Álvarez, María Jesús Cabero, Paloma Lanza León, Javier Lera Torres, Marina Barreda Gutiérrez, Silvia Suárez Luque, Carolina Muñoz Ibáñez, Sharon Vella, Paula Vassallo, Mariella Borg Buontempo, Miguel Telo de Arriaga, Leonor Quelhas Pinto (Health4EUKids Work Package 5); Heli Kuusipalo, Emma Koivurinta, Nella Savolainen, Kati Kuisma, Taina Sainio (Health4EUKids Work Package 6).











