

To review the hoaxes’ characteristics spread through WhatsApp in Spain during COVID-19 lockdown and identify what kind of substances were promoted for consumption or application.
MethodA phone number was activated to receive hoaxes via WhatsApp. A total of 2353 messages were collected, and among those 584 different hoaxes were identified and validated, between March 18 and April 18, 2020. From these 584 hoaxes, a sub-sample of 126 was selected, exclusively related to the object of study, and a content analysis table with fourteen registration fields was applied. Besides, the averages and medians of the quantitative fields were extracted.
ResultsMost of the messages received were texts (39%) and videos (30%). In the majority, the acting subject was presented as medical personnel (36.5%) or as an anonymous person (30.9%). The videos lasted between 2’ 40” and 18’ 18”, while the audios ranged between 1’ 35” and 7’ 48”. Regarding the gender of the informant, there was a significant difference, with 45.2% being male, and 13.5%, female and 41.3% non-identifiable.
ConclusionsOne out of five false health claims received was about prevention or cure of the coronavirus, based on the principle of medical authority, and basically promoting the use and consumption of substances of natural origin.
Examinar las características de los bulos difundidos por WhatsApp en España durante el confinamiento por la pandemia de COVID-19 e identificar qué tipo de sustancias se promovieron para su ingesta o uso.
MétodoSe habilitó un número de teléfono para recibir bulos por WhatsApp. Se recibieron 2353 mensajes, de los que se identificaron y validaron 584 bulos distintos, entre el 18 de marzo y el 18 de abril de 2020. De los 584 bulos, se seleccionó una submuestra de 126 relacionados con el objeto de estudio y se aplicó una ficha de análisis de contenido con 14 campos de registro. Además, se extrajeron las medias y medianas de los campos cuantitativos.
ResultadosLa mayor parte de los mensajes fueron cadenas de texto (39%) y vídeos (30%). En la mayoría, el sujeto se presentaba como personal médico (36,5%) o como persona anónima (30,9%). Los vídeos tuvieron una duración de entre 2’ 40” y 18’ 18”, mientras que los audios fueron de entre 1’ 35” y 7’ 48”. Con respecto al sexo, se apreció una gran diferencia: el 45,2% de los protagonistas fueron hombres, frente al 13,5% de mujeres; el 41,3% no era identificable.
ConclusionesUno de cada cinco bulos recibidos fue sobre prevención o curación del coronavirus, argumentados sobre el principio de autoridad médica y básicamente promoviendo el uso y consumo de sustancias de origen natural.
The SARS-CoV-2 coronavirus pandemic, in addition to generating a huge social and economic impact worldwide, has triggered an informative ‘epidemic’ (infodemic) among the world population,1–5 unprecedented in contemporary history.6,7 Authors such as Vaezi and Javanmard7 point out that infodemics are produced by the dissemination of toxic messages at the same speed as epidemics spread. This flow of out-of-context, false, manipulative, conspiratorial or satirical messages, which circulate through different information channels and sources, is generically called disinformation,7 which, albeit not a recent phenomenon, has been exacerbated by the emergence of social networks.8–11
When false information believed to be true is forwarded, it is called ‘misinformation’ and when erroneous information is deliberately shared for a specific purpose, then it is referred to as ‘disinformation’.12,13This deliberate way of spreading false information is what has been popularly called ‘fake news’ since 2016, due to the use to which toxic messages of this type were put during the US presidential campaign.12,13In turn, disinformation messages can be disseminated in the form of memes, fake news, manipulated photos or videos, propaganda or hoaxes.14,15 In this work, hoaxes have been chosen as the object of study. Boese16 defines hoaxes as lies that must have something extra. For this author, they should be somewhat outrageous, resourceful, dramatic or sensationalist. Above all, they should capture the attention and ideally the imagination of the public, and are basically spread as private hoaxes. For their part, Finneman and Thomas17 argue that deception applies to any situation in which the message initially confuses the public. According to a study published by Tasnim, Hossain and Mazumder,6 the pandemic crisis has contributed to increase the quantity of rumours, deceits and disinformation relating to the aetiology, results, prevention and cure of the COVID-19 disease. One of the characteristics of the dissemination of this false information is the promotion of erroneous practices that could increase the spread of the virus and, ultimately, have a negative impact on people's physical and mental health. According to these authors, countless mishaps caused by the spread of rumours among the population have been confirmed worldwide.6 In this context, since the beginning of the pandemic crisis, the World Health Organisation (WHO)18 proposed taking specific action to manage this infodemic, such as suggesting to social media companies that they take measures to control the spread of fake news and offer direct links to institutional information sources.
The disinformation that is spread through social media, such as Facebook or Twitter, is neutralised as soon as someone reports content as false.19–23However, private messaging services, such as WhatsApp and Telegram, are employed to send isolated messages to people who cannot immediately confirm, or obtain confirmation on, whether they are true or not. These networks have thus become a means of disseminating very harmful messages that could pose a serious public health risk or exacerbate the condition of people with early symptoms.6 The lockdown imposed as a preventive measure to keep the number of infections under control during the pandemic encouraged the public to use social media and private messaging services. Indeed, the traffic of instant messaging services, such as WhatsApp, quintupled in Spain.24 A public opinion study performed on the public's exposure to hoaxes and fake news during the initial stages of the SARS-CoV-2 crisis in Spain indicates that most of these messages (64.3 per cent) were received via social networking sites and instant messaging services, with WhatsApp leading the field (68.8 per cent).25
The objective of this exploratory study was to identify the specific characteristics of hoaxes about COVID-19 disseminated via WhatsApp during the first month of the state of alarm in Spain, which prompted the public to consume pharmacological substances, miracle remedies or alternative therapies or urged them to take specific action or to abstain from doing so.26 Specifically, the focus was placed on those hoaxes that might have posed a public health risk27 or might have had a negative impact on the epidemic's evolution.28
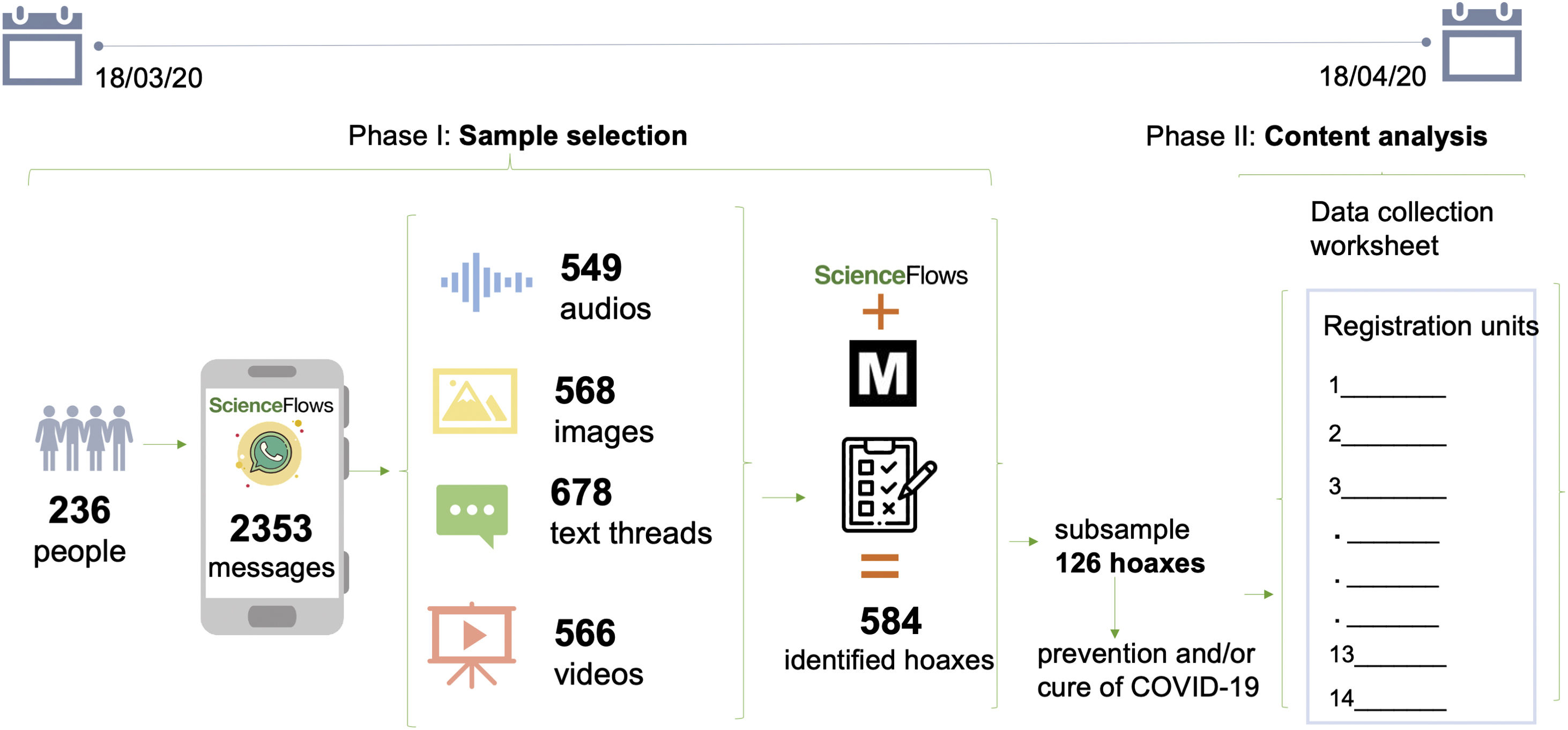
MATERIAL AND METHODTo perform this study, a Spanish mobile phone number was provided so that people could participate in the research, voluntarily sending the hoaxes that they received on their devices, in accordance with the protocols for personal data protection established by the Organic Law on the Protection of Personal Data (Ley Orgánico de Protección de Datos, LOPD). The phone number was disseminated in an institutional press release issued by the University of Valencia. It was also posted on the websites of the scientific news agency SINC, the Salud Sin Bulos Institute and ScienceFlows. From 18 March to 18 April 2020, 236 people voluntarily sent a total of 2,353 messages (568 images, 678 text threads, 566 videos and 549 audios). Each message received was validated on the Maldita.es database, a non-profit communication media outlet specialising in fact checking. To this end, a collaboration agreement was signed between Maldita.es and the ScienceFlows team, in which the platform sent the authors of this paper a TSV file, separated by tabs and encoded in UTF-8, with the hoaxes registered from 18 March to 18 April. Of the 2,353 messages received, only 584 different ones were validated as hoaxes. After a preliminary examination of the 584 identified hoaxes, a subsample of 126 was chosen following the two criteria previously established for this exploratory study: being verified hoaxes and dealing with the prevention and/or cure of COVID-19. (Figure 1)

Sample selection and study method. The diagram shows the two phases of the research. Phase 1: selection of the sub-sample of 126 hoaxes. To reach this sub-sample of hoaxes, a participatory research was designed, in which 236 people voluntarily sent 2353 documents, which were labelled one by one and validated as hoaxes through the Maldita.es database, whose methodology for verifying the information can be found at https://educa.maldita.es/metodologia-y-herramientas-de-verificacion/. Phase 2: exploratory study of each of the hoaxes by applying standard content analysis through a registration form with 14 items. Means and medians were calculated for the quantitative data.
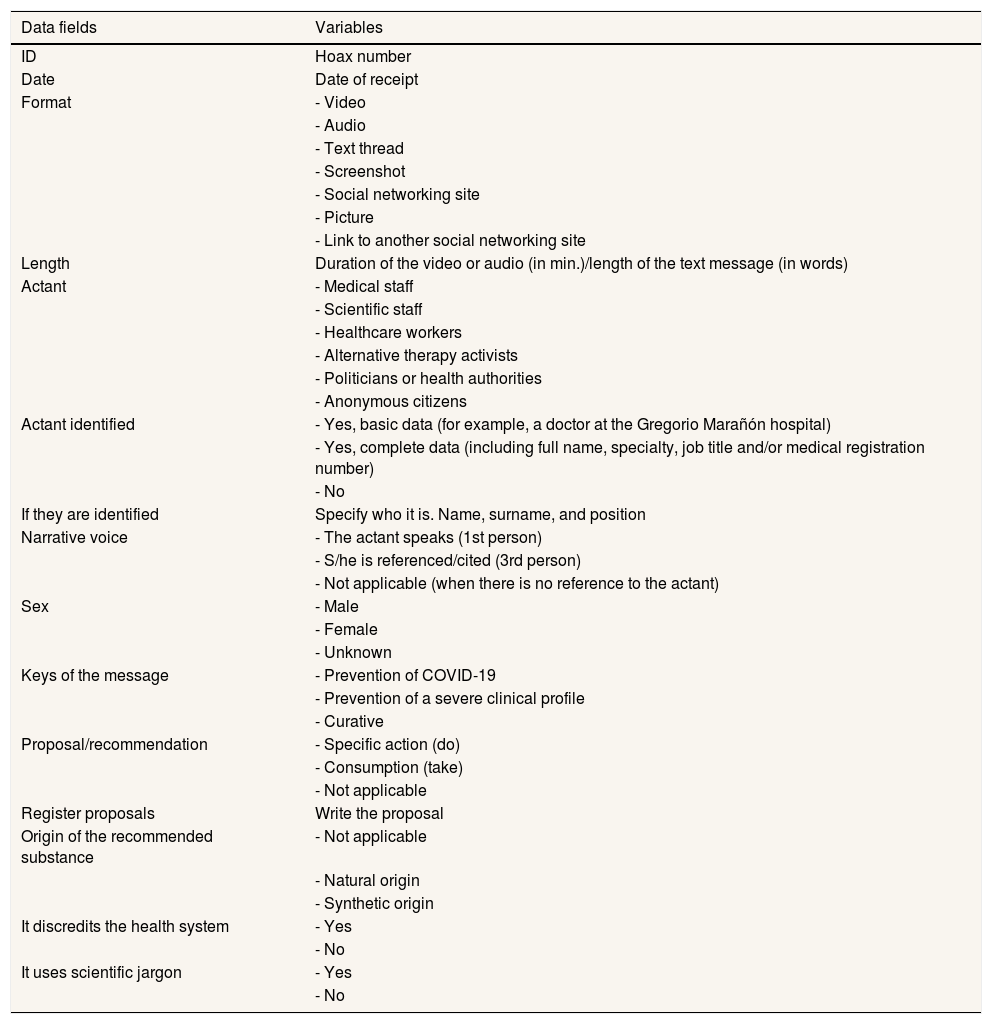
Subsequently, the registration units and the variables necessary to meet the research objective were specially designed. The data collection worksheet used is shown in Table 1.
Data fields and variables of the worksheet for analysing the hoaxes retrieved from the Maldita.es database.
| Data fields | Variables |
|---|---|
| ID | Hoax number |
| Date | Date of receipt |
| Format | - Video |
| - Audio | |
| - Text thread | |
| - Screenshot | |
| - Social networking site | |
| - Picture | |
| - Link to another social networking site | |
| Length | Duration of the video or audio (in min.)/length of the text message (in words) |
| Actant | - Medical staff |
| - Scientific staff | |
| - Healthcare workers | |
| - Alternative therapy activists | |
| - Politicians or health authorities | |
| - Anonymous citizens | |
| Actant identified | - Yes, basic data (for example, a doctor at the Gregorio Marañón hospital) |
| - Yes, complete data (including full name, specialty, job title and/or medical registration number) | |
| - No | |
| If they are identified | Specify who it is. Name, surname, and position |
| Narrative voice | - The actant speaks (1st person) |
| - S/he is referenced/cited (3rd person) | |
| - Not applicable (when there is no reference to the actant) | |
| Sex | - Male |
| - Female | |
| - Unknown | |
| Keys of the message | - Prevention of COVID-19 |
| - Prevention of a severe clinical profile | |
| - Curative | |
| Proposal/recommendation | - Specific action (do) |
| - Consumption (take) | |
| - Not applicable | |
| Register proposals | Write the proposal |
| Origin of the recommended substance | - Not applicable |
| - Natural origin | |
| - Synthetic origin | |
| It discredits the health system | - Yes |
| - No | |
| It uses scientific jargon | - Yes |
| - No |
With the aim of establishing the concordance between the responses, the paper's four authors agreed on the variables of each one of the data fields. Subsequently, two evaluators independently coded all the hoaxes making up the subsample, resulting in a Kappa value of 0.80 for the only data field in which there was some disagreement between the variables (‘Origin of the recommended substance’). The rest of the data fields did not show any disagreement, with Kappa values equal to 1. Likewise, an attempt was made to identify clusters, means and medians between the actant of the hoaxes and the type of substance or action promoted, but no conclusive data were obtained. The results were very disparate and not statistically significant. In this connection, the research technique employed in this exploratory study was standardised content analysis, according to Krippendorff,29 aimed at formulating reproducible and valid inferences, based on the recorded data.
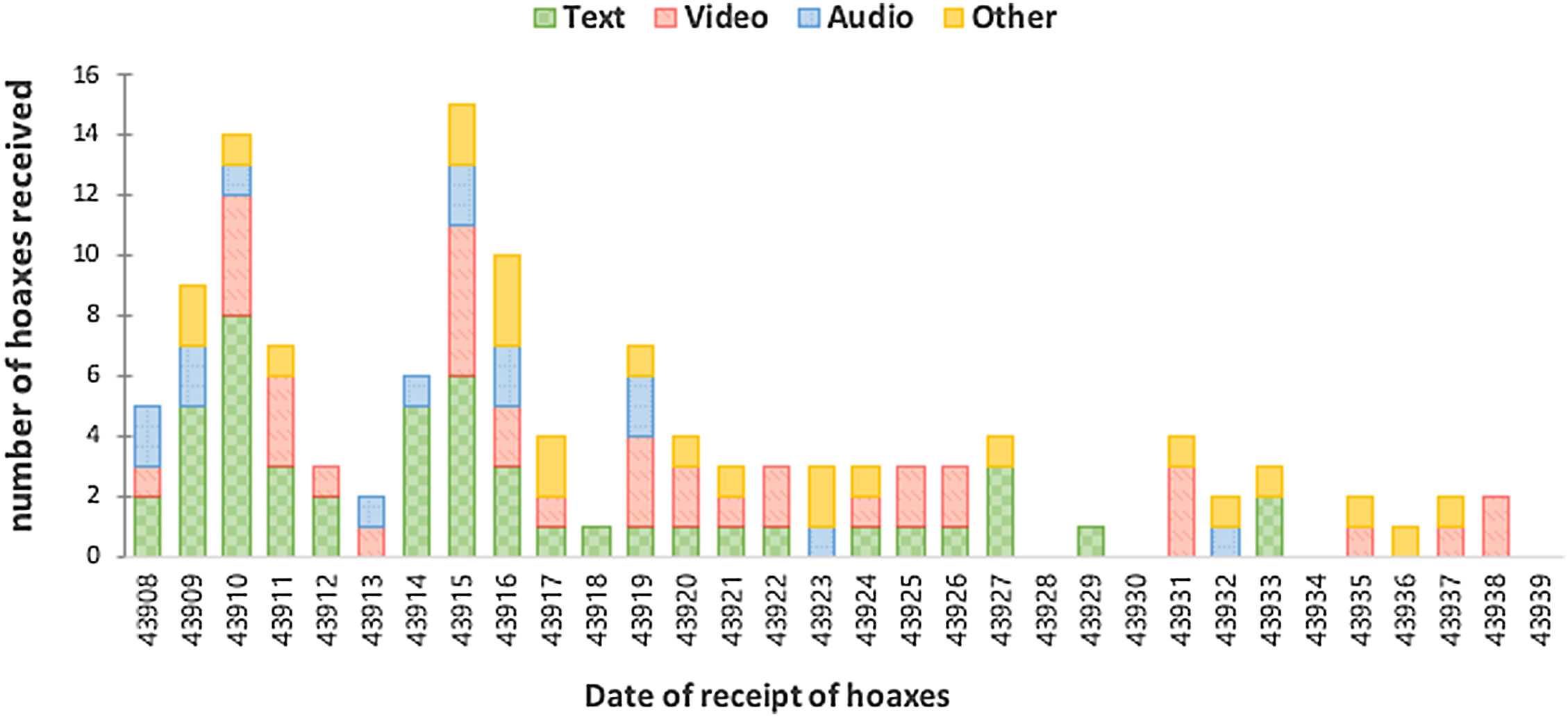
RESULTSThe subsample of 126 hoaxes selected for study accounted for 21.6 per cent of the corpus of verified hoaxes during the period (584). As to their format, 38 videos, 15 audios, 49 text threads and 24 miscellaneous documents were identified (photographs, infographics, pamphlets, screenshots of Facebook, Twitter or other social networking sites, links, etc.). There was a greater probability of receiving hoaxes about the prevention and/or cure of COVID-19 during the first 15 days of lockdown (see Graph 1). Most of the validated hoaxes received were in text thread (39 per cent) or video (30 per cent) format. (Figure 2)

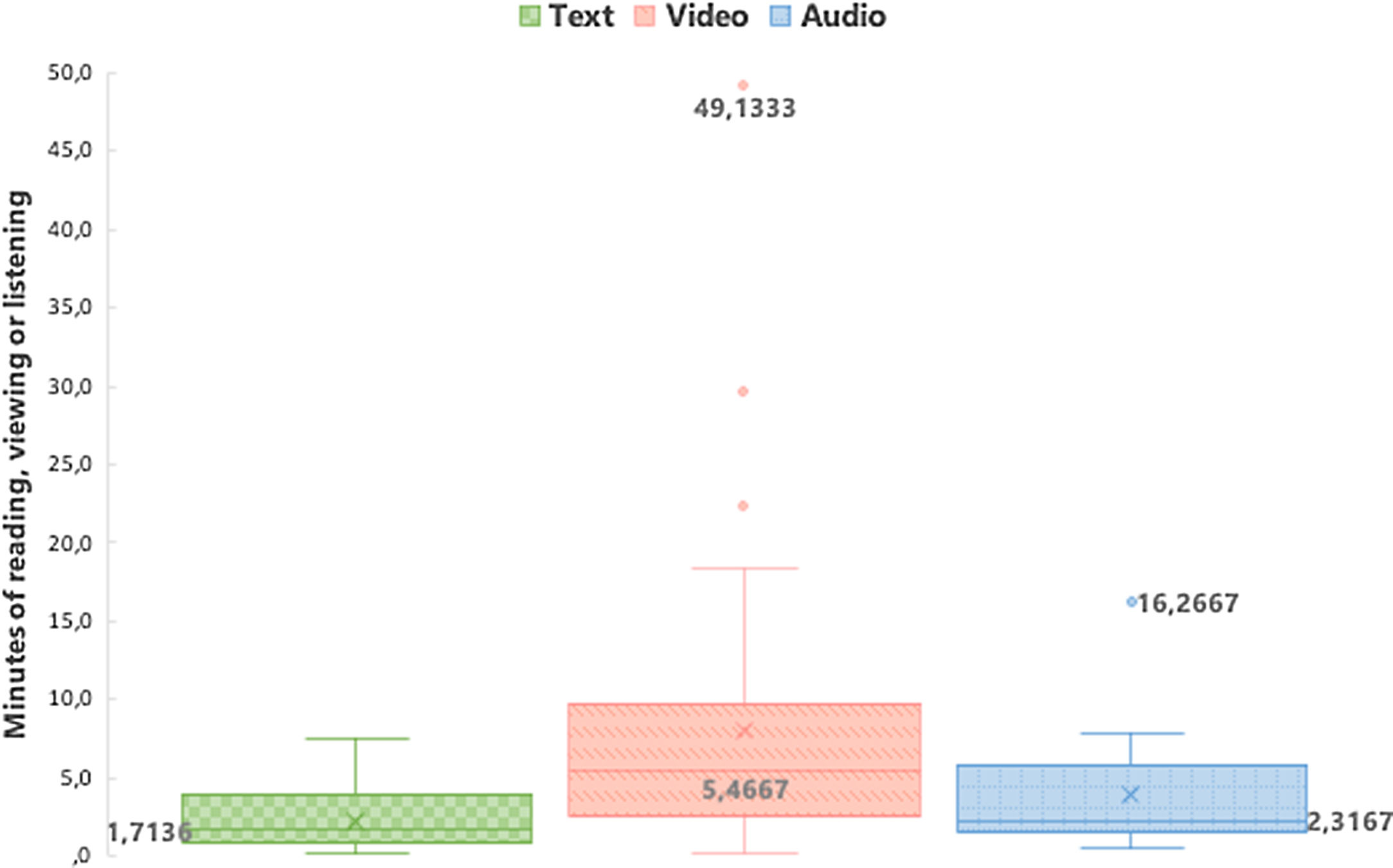
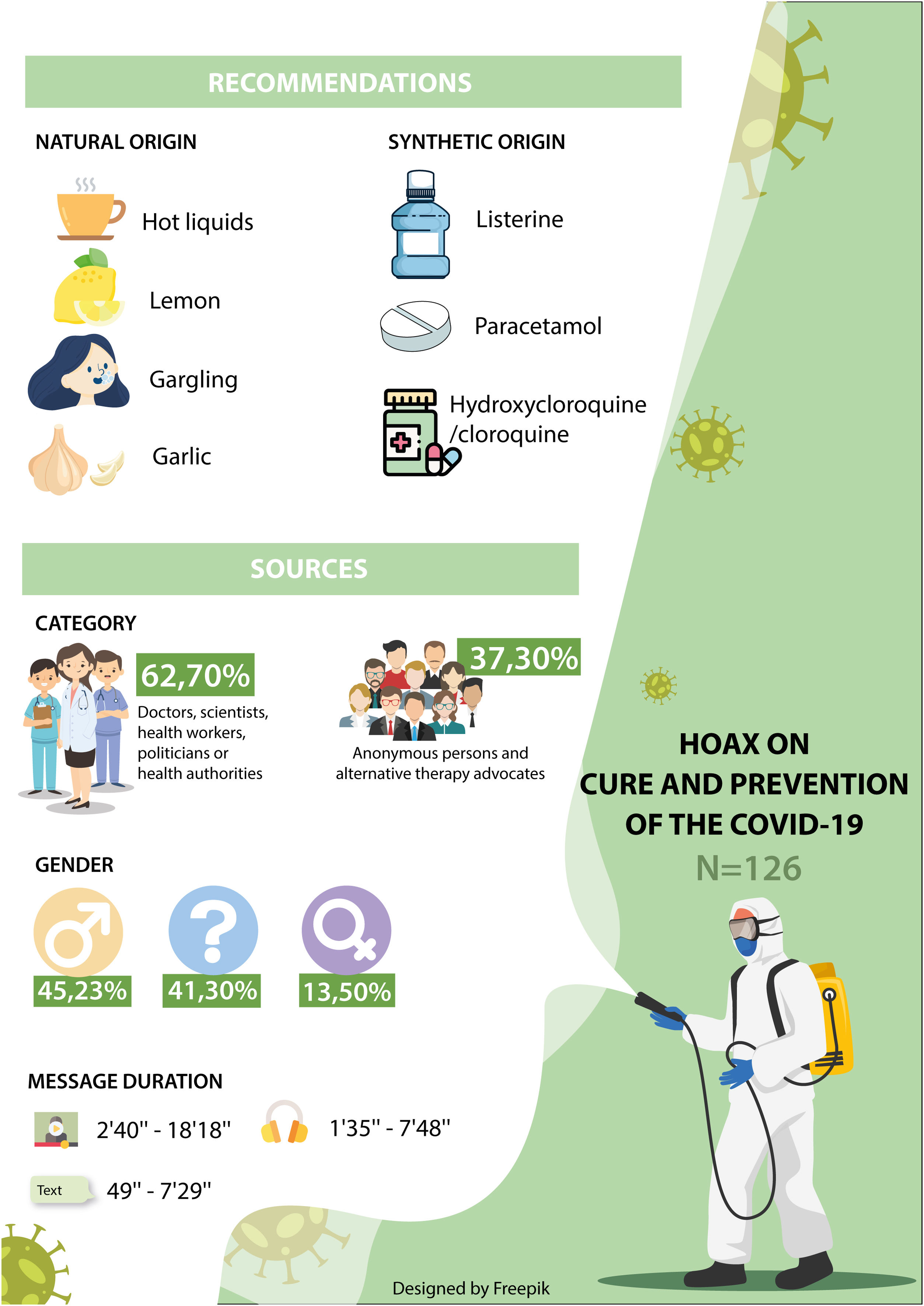
Message content was longer than usual. Most of the shared videos and audios lasted between 2’ 40” and 18’ 18” and 1’ 35” and 7’ 48”, respectively. The approximate time that would be required to read most of the text threads was estimated between 49” and 7’ 29”, taking into account an average reading rate of 160 words per minute.30 Nonetheless, there were also a number of very long videos and audios lasting around 49” and 16”, respectively (see Graph 2). (Figure 3)

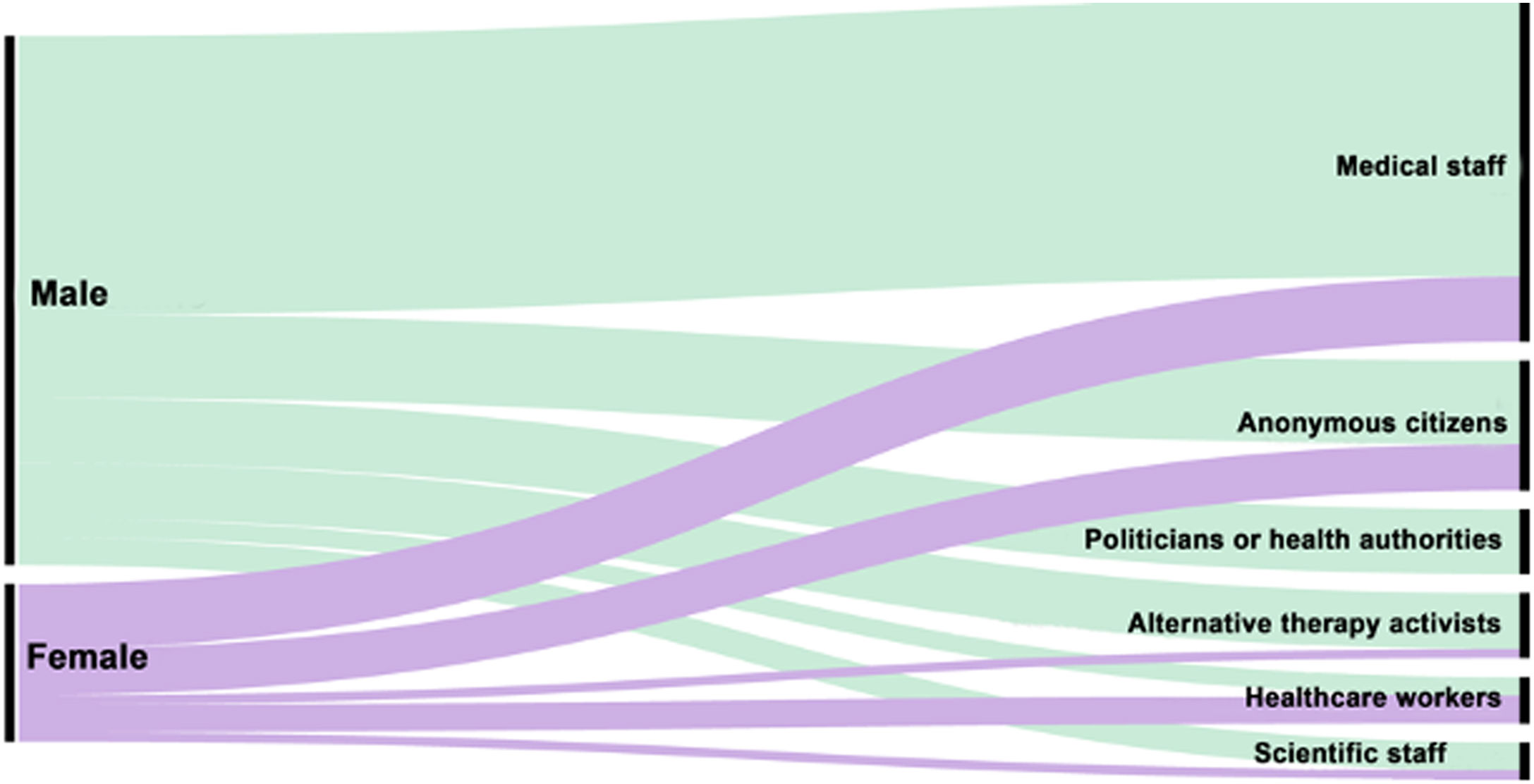
In most of these hoaxes, the actant and the source of information on the recommendation made were purportedly medical workers (36.5 per cent) or anonymous citizens (30.9 per cent). Politicians or health authorities were the actants in 12.7 per cent of the messages, followed by scientists (9.5 per cent), alternative therapy activists (6.3 per cent) and, finally, other categories of health personnel (3.9 per cent). Based on the identification of the actant, 61.9 per cent of the hoaxes did reveal the name and surname of the information source. Specifically, 34.1 per cent offered basic information and 27.8 per cent, complete information. It should be noted that more than a third of the hoaxes (38.1 per cent) did not contain any information on the identity of their source. Regarding the narrative voice, there were no statistically significant differences between the use of the first or the third person, with 42.9 per cent of hoaxes being narrated in the former and 49.2 per cent in the latter (7.9 per cent not applicable). However, there were indeed statistically significant differences with respect to the sex of the actant, 45.2 per cent being male and 13.5 per cent female (41.3 per cent being unknown). (Figure 4)

As to those hoaxes in which the gender and profession of the actants were mentioned (see Graph 3), 52 per cent of the men professed to be medical workers, versus 41.2 per cent of the women. By and large, 29.4 per cent of the women did not identify themselves and were classified as anonymous citizens, versus 15.8 per cent of the men. The only category in which women outnumbered men (17.6 and 3.5 per cent, respectively) was that of healthcare workers. Moreover, none of the women introduced themselves as politicians or belonging to a health authority, whereas 12.28 per cent of the men identified themselves as such. Although the hoaxes were based on misleading, false or out-of-context interpretations of the official information disseminated by the health authorities, most of them were not aimed as discrediting them (94.4 per cent). As a matter of fact, only seven messages (5.6 per cent) openly criticised the Western healthcare system, five of which contained technical jargon and four of which were sent by alternative therapy activists. In the main, the hoaxes employed mostly non-technical language aimed at the general public (75.4 per cent), while 24.6 per cent resorted to technical jargon as a discursive strategy, widely used in advertising, to make them seem more credible.31,32
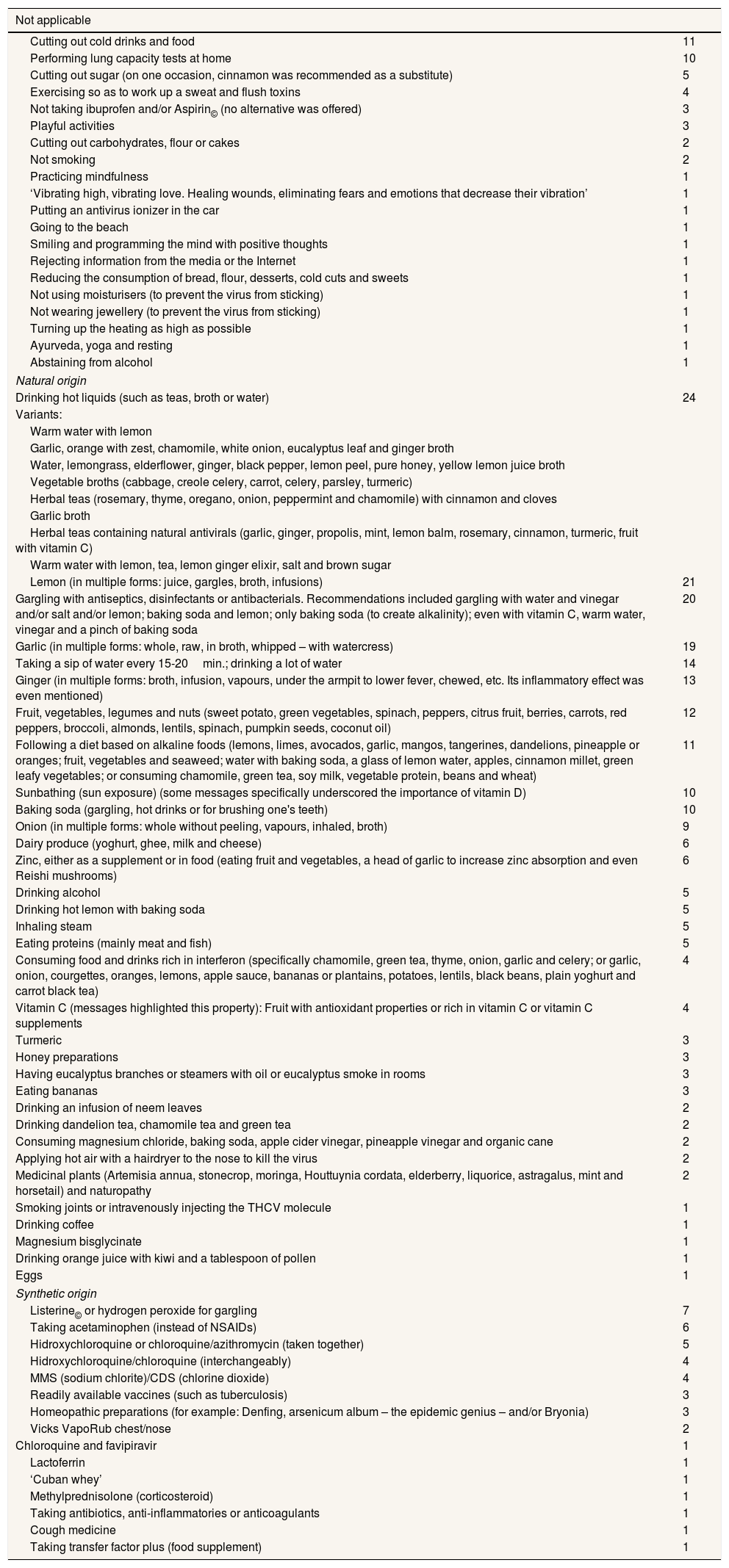
Regarding the thematic core of the hoaxes, the prevention of infection by SARS-CoV-2 was the only issue addressed in 50.8 per cent of them. Those focusing instead on cures for COVID-19 represented 31.7 per cent of the subsample. The hoaxes pursuing both of the aforementioned objectives accounted for 7.9 per of the total. And, lastly, those that solely offered recommendations on how to avoid a severe clinical profile associated with COVID-19 represented 9.5 per cent. At a second level of classification, the hoaxes, in addition to spreading erroneous information on preventing and/or curing COVID-19, promoted the consumption of certain substances (61.5 per cent of the subsample) or taking specific action (32.1 per cent). Regarding the consumption of certain substances, 58.9 per cent were natural (e.g. lemons and ginger) and 32.1 per cent were synthetic (e.g. drugs). While as to taking specific action to prevent infection by SARS-CoV-2, examples classified by the origin of the recommended substances are shown in Table 2.
List of specific suggestions to prevent or cure COVID-19 classified by the origin of the recommended substances.
| Not applicable | |
|---|---|
| Cutting out cold drinks and food | 11 |
| Performing lung capacity tests at home | 10 |
| Cutting out sugar (on one occasion, cinnamon was recommended as a substitute) | 5 |
| Exercising so as to work up a sweat and flush toxins | 4 |
| Not taking ibuprofen and/or Aspirin© (no alternative was offered) | 3 |
| Playful activities | 3 |
| Cutting out carbohydrates, flour or cakes | 2 |
| Not smoking | 2 |
| Practicing mindfulness | 1 |
| ‘Vibrating high, vibrating love. Healing wounds, eliminating fears and emotions that decrease their vibration’ | 1 |
| Putting an antivirus ionizer in the car | 1 |
| Going to the beach | 1 |
| Smiling and programming the mind with positive thoughts | 1 |
| Rejecting information from the media or the Internet | 1 |
| Reducing the consumption of bread, flour, desserts, cold cuts and sweets | 1 |
| Not using moisturisers (to prevent the virus from sticking) | 1 |
| Not wearing jewellery (to prevent the virus from sticking) | 1 |
| Turning up the heating as high as possible | 1 |
| Ayurveda, yoga and resting | 1 |
| Abstaining from alcohol | 1 |
| Natural origin | |
| Drinking hot liquids (such as teas, broth or water) | 24 |
| Variants: | |
| Warm water with lemon | |
| Garlic, orange with zest, chamomile, white onion, eucalyptus leaf and ginger broth | |
| Water, lemongrass, elderflower, ginger, black pepper, lemon peel, pure honey, yellow lemon juice broth | |
| Vegetable broths (cabbage, creole celery, carrot, celery, parsley, turmeric) | |
| Herbal teas (rosemary, thyme, oregano, onion, peppermint and chamomile) with cinnamon and cloves | |
| Garlic broth | |
| Herbal teas containing natural antivirals (garlic, ginger, propolis, mint, lemon balm, rosemary, cinnamon, turmeric, fruit with vitamin C) | |
| Warm water with lemon, tea, lemon ginger elixir, salt and brown sugar | |
| Lemon (in multiple forms: juice, gargles, broth, infusions) | 21 |
| Gargling with antiseptics, disinfectants or antibacterials. Recommendations included gargling with water and vinegar and/or salt and/or lemon; baking soda and lemon; only baking soda (to create alkalinity); even with vitamin C, warm water, vinegar and a pinch of baking soda | 20 |
| Garlic (in multiple forms: whole, raw, in broth, whipped – with watercress) | 19 |
| Taking a sip of water every 15-20min.; drinking a lot of water | 14 |
| Ginger (in multiple forms: broth, infusion, vapours, under the armpit to lower fever, chewed, etc. Its inflammatory effect was even mentioned) | 13 |
| Fruit, vegetables, legumes and nuts (sweet potato, green vegetables, spinach, peppers, citrus fruit, berries, carrots, red peppers, broccoli, almonds, lentils, spinach, pumpkin seeds, coconut oil) | 12 |
| Following a diet based on alkaline foods (lemons, limes, avocados, garlic, mangos, tangerines, dandelions, pineapple or oranges; fruit, vegetables and seaweed; water with baking soda, a glass of lemon water, apples, cinnamon millet, green leafy vegetables; or consuming chamomile, green tea, soy milk, vegetable protein, beans and wheat) | 11 |
| Sunbathing (sun exposure) (some messages specifically underscored the importance of vitamin D) | 10 |
| Baking soda (gargling, hot drinks or for brushing one's teeth) | 10 |
| Onion (in multiple forms: whole without peeling, vapours, inhaled, broth) | 9 |
| Dairy produce (yoghurt, ghee, milk and cheese) | 6 |
| Zinc, either as a supplement or in food (eating fruit and vegetables, a head of garlic to increase zinc absorption and even Reishi mushrooms) | 6 |
| Drinking alcohol | 5 |
| Drinking hot lemon with baking soda | 5 |
| Inhaling steam | 5 |
| Eating proteins (mainly meat and fish) | 5 |
| Consuming food and drinks rich in interferon (specifically chamomile, green tea, thyme, onion, garlic and celery; or garlic, onion, courgettes, oranges, lemons, apple sauce, bananas or plantains, potatoes, lentils, black beans, plain yoghurt and carrot black tea) | 4 |
| Vitamin C (messages highlighted this property): Fruit with antioxidant properties or rich in vitamin C or vitamin C supplements | 4 |
| Turmeric | 3 |
| Honey preparations | 3 |
| Having eucalyptus branches or steamers with oil or eucalyptus smoke in rooms | 3 |
| Eating bananas | 3 |
| Drinking an infusion of neem leaves | 2 |
| Drinking dandelion tea, chamomile tea and green tea | 2 |
| Consuming magnesium chloride, baking soda, apple cider vinegar, pineapple vinegar and organic cane | 2 |
| Applying hot air with a hairdryer to the nose to kill the virus | 2 |
| Medicinal plants (Artemisia annua, stonecrop, moringa, Houttuynia cordata, elderberry, liquorice, astragalus, mint and horsetail) and naturopathy | 2 |
| Smoking joints or intravenously injecting the THCV molecule | 1 |
| Drinking coffee | 1 |
| Magnesium bisglycinate | 1 |
| Drinking orange juice with kiwi and a tablespoon of pollen | 1 |
| Eggs | 1 |
| Synthetic origin | |
| Listerine© or hydrogen peroxide for gargling | 7 |
| Taking acetaminophen (instead of NSAIDs) | 6 |
| Hidroxychloroquine or chloroquine/azithromycin (taken together) | 5 |
| Hidroxychloroquine/chloroquine (interchangeably) | 4 |
| MMS (sodium chlorite)/CDS (chlorine dioxide) | 4 |
| Readily available vaccines (such as tuberculosis) | 3 |
| Homeopathic preparations (for example: Denfing, arsenicum album – the epidemic genius – and/or Bryonia) | 3 |
| Vicks VapoRub chest/nose | 2 |
| Chloroquine and favipiravir | 1 |
| Lactoferrin | 1 |
| ‘Cuban whey’ | 1 |
| Methylprednisolone (corticosteroid) | 1 |
| Taking antibiotics, anti-inflammatories or anticoagulants | 1 |
| Cough medicine | 1 |
| Taking transfer factor plus (food supplement) | 1 |
With respect to those hoaxes that prompted a specific action to prevent infection by the SARS-CoV-2 coronavirus, they accounted for 38.5 per cent of the subsample. Examples of these actions can be found in Table 2, where the suggestions classified by the origin of the recommended substances are shown.
There was a wide variety of recommendations that have been grouped under the concept of ‘not applicable’ because they were unrelated to the other two categories. These featured cutting out cold food or drinks and performing lung capacity tests at home. As to the natural substance category, consuming hot drinks (such as tea, infusions, broths, etc.), drinking warm water with garlic and lemon and gargling with disinfectants stood out. Regarding the synthetic substance category, taking the antimalarials chloroquine and hydroxychloroquine, alone or together with antibiotics or antivirals, gargling with Listerine© or oxygen peroxide, taking paracetamol (instead of NSAIDs) and MMS were among the most frequent recommendations. The main results of this exploratory study are shown in Image 1. (Figure 5)
DISCUSSION
This exploratory study has shown that the sheer number of hoaxes about COVID-19 disseminated via WhatsApp coincides with the phenomenon known as infodemic, as other authors have contended.1–5 Approximately one in five hoaxes recommended the consumption of some or other substance, both natural and synthetic, as well as taking a number of specific actions. Some of these hoaxes had the potential to exacerbate the saturation of health systems owing to the side effects of putting into practice their recommendations. For example, the recorded side effects of some of the preventive or curative techniques recommended include burns or poisoning, as a result of consuming substances like chlorine dioxide, among others.
Regarding natural remedies, such as consuming hot drinks or lemons, in different doses, although they cannot be regarded as dangerous, the confidence that infusions and compound macerations may raise in those putting them to a therapeutic use could have dire consequences, as they might be tempted to delay seeking medical treatment until it is too late. This is related to two attitudes that people show towards the reception of information flows: risk perception33 and confirmation bias.34 In relation to risk perception, people may feel protected by resorting to any of these practices, under the impression they are making a positive decision on their health. On the other hand, confirmation bias occurs when the messages received reinforce already existing attitudes and opinions. Both psychological processes lead to problem denial.
A comprehensive review of the recommendations made in this subsample reveals two types of content. The first forms part of the classic complementary approaches to combat flu and other types of respiratory diseases, such as vitamin C, garlic, honey or nasal irrigation with saline solutions.35 In fact, some of the hoaxes recommended the daily and family use of these substances to prevent and/or cure respiratory infections. In any case, these recommendations always included a conspiracy narrative, with categorical statements or authoritative fallacies, like, for example, the hoax received on 19 March, indicating, ‘If you drink a lot of water and gargle with warm water and salt or vinegar, you’ll eliminate the coronavirus.’
The second type of content recommended the consumption of substances to boost the immune system, to eliminate the virus from the throat, before it reached the lungs, or to alkalinise the body, since drugs such as chloroquine ‘block infection increasing the pH of the endosome’. In this category, the recommendations also included the use of MMS and its variant CDS. For example, the image received on 20 March stating, ‘Bananas cure COVID-19,’ or the anonymous audio that went viral on 18 April, confirming, ‘Scientists know that chloroquine is the only treatment that cures coronavirus; what happens is that there is not enough to go round.’
Regarding the limitations of this study, as self-selection sampling was employed, compiling voluntarily and anonymously received hoaxes, there were no comparable sociodemographic or stratified data. As the hoaxes making up the subsample were only in Spanish, the results cannot be extrapolated to other languages. Another drawback is the lack of data on the attitude of the receivers towards these hoaxes. Nor is there any data on the number of times that these hoaxes were forwarded or on how many people followed their recommendations. Finally, the labeling of a message as a hoax by the fact-checking platform might have led to some bias.
To conclude, an average of approximately four hoaxes with recommendations for taking direct action against COVID-19 were received on a daily basis. As to why these hoaxes spread, one of the reasons might have been due to their appealing nature, the use of home-based strategies and their authoritative medical discourse.
Editor responsible for the articleGonzalo Casino
Transparency statementThe main author, guarantor responsible for the manuscript, affirms this manuscript is an honest, accurate and transparent report of the study. The article sent to Gaceta Sanitaria has not been omitted important aspects of the study. The discrepancies of the research, as planned, have been explained.
Authorship contributionsFour manuscripts contributed intellectually to the manuscript's design and preparation and read and approved the final version before being sent for publishing. Also, we are responsible and guarantors that all aspects that make up the manuscript were reviewed and discussed by us to expose them with the utmost precision and rigour.
Ackno***wledgementsThe authors wish to express their gratitude to the UICC of the University de Valencia, to the SINC Agency (Science Information and News Service), the Instituto Salud Sin Bulos and the Asociación para Proteger al Paciente de Pseudoterapias (APETP) for their collaboration in the dissemination of the study and also for helping us during the collecting of the hoaxes. Likewise, appreciate the cooperation of Maldita.es, a communication medium, the non-profit organisation specialising in data verification, which helped us validate each hoax studied. Finally, we appreciate a lot the translator, Amaia Crespo, for the English version of the article and the graphic designer, Ana Serra, to edit the images.
FundingThis study has been carried out within the European Project “No Rumor Health” (Erasmus + program 2019-1-ES01-KA204- 064037), in which a consortium of three European countries participates (Spain, Poland and Greece).
Conflicts of interestIt doesn’t exit.










