




To examine the effects of common mental disorders and physical conditions on role functioning in Spain.
MethodsCross-sectional study of the general adult population of Spain (n = 2,121). Non-psychotic mental disorders were assessed with the Composite International Diagnostic Interview (CIDI 3.0) and physical conditions with a checklist. The role functioning dimension of the WHO-Disability Assessment Schedule (WHODAS) was used to asses the number of days in the past month in which respondents were fully or partially limited to perform daily activities. Generalized linear models were used to estimate individual-level associations of specific conditions and role functioning, controlling for co-morbidity. Societal level estimates were calculated using population attributable risk proportions (PARP).
ResultsMental disorders and physical conditions showed similar number of days with full role limitation (about 20 days per year); in contrast mental disorders were responsible for twice as many days with partial role limitation than physical conditions (42 vs 21 days, respectively). If the population were entirely unexposed to mental and physical conditions, days with full limitation would be reduced by 73% and days with partial limitation by 41%.
ConclusionsCommon health conditions in Spain are associated with considerably more days with role limitation than other Western countries. There is need of mainstreaming disability in the Spanish public health agenda in order to reduce role limitation among individuals with common conditions.
Analizar la discapacidad funcional de trastornos mentales y físicos frecuentes en España.
MétodosEstudio transversal de la población general adulta de España (n = 2121). La evaluación de trastorno mental no psicótico se hizo con la Entrevista Diagnóstica Internacional Compuesta. Los trastornos físicos fueron autorreportados a partir de una lista estandarizada. La dimensión de actividades de la vida diaria de WHO-Disability Assessment Schedule (discapacidad funcional) se utilizó para evaluar el número de días del mes pasado en que los/as participantes presentaron una limitación total o parcial para realizar actividades de la vida diaria. Se ajustaron modelos lineales generalizados para estimar las asociaciones individuales entre trastornos y discapacidad funcional, controlando por comorbilidad. En el ámbito social, se calcularon las proporciones del riesgo atribuible poblacional (PARP).
ResultadosLos trastornos mentales y físicos mostraron igual número de días con discapacidad funcional total (20 días/año). En cambio, los trastornos mentales se asociaron al doble de días con discapacidad funcional parcial que los trastornos físicos (42 frente a 21 días, respectivamente). Si la población no estuviera expuesta a los trastornos mentales y físicos frecuentes, los días con discapacidad funcional total se reducirían un 73% y los días con discapacidad funcional parcial un 41%.
ConclusionesLos trastornos mentales y físicos frecuentes están asociados con un mayor número de días con discapacidad funcional en España que en otros países occidentales. Es necesario incorporar la discapacidad en la agenda de salud pública española con el fin de reducir la limitación funcional entre los individuos con trastornos frecuentes.
Efforts for improving the measure of the burden of diseases are needed for setting priorities on resource allocation. Along with traditional indicators of health status (morbidity and mortality), disability has become an important indicator of burden.1 Disability is “the difficulty in functioning at the body, person, or societal levels, in one or more life domains, as experienced by an individual with a health condition in interaction with contextual factors”.2 Around 15% of the world's population experiences disability.3 One major component of the economic costs of disability is loss of labour productivity, as a result of work absences or reduced work.3 Data on disability-related productivity losses are scarce and difficult to obtain. In Canada,4 the total indirect cost attributable to short and long-term disability was around 42 billion dollars in 1998, the 6.7% of Canada's GDP.
Common conditions, including mental disorders, are important determinants of disability, but the interrelation between disorders and disability is complex. High prevalence of a health condition does not always mean high associated disability. In 2004, in Australia,5 arthritis was the most prevalent condition and the one with the highest proportion of disability, while autism was causing the highest impact on activity limitation, though it had the lowest prevalence rate. The number of co-occurring disorders, co-morbidities, is also important when considering the relationship between health conditions and disability. Recently, two reports6,7 from the World Mental Health Surveys showed that controlling by co-morbid conditions and their specific severity weights, mental and physical conditions yielded substantial full and partial limitation for performing activities of daily living worldwide. Marked differences by country level income were observed: while in high income countries, health conditions have a large effect on partial role limitation; in low and medium income countries a substantial impact on full role limitation was reported. The authors hypothesised on differences in prevalence rates of conditions as well as differences in welfare states as possible explanations of such cross-national differences.
Contextual factors (e.g., technology, attitudes, health services, legislation and policies) have a huge impact on the experience and in the extent of disability.3 In 2002, Spain reported one of the lowest prevalence percentages of disability in Europe, with 8.7% of the working-age population reporting disability.8 Recently, the burden of disease in Spain was measured.9 Neurological and mental disorders, malignant neoplasms, and cardiovascular disease, were the leading causes of DALYs (i.e., disability-adjusted life years). While comparative illness burden estimates are valuable for health planners, two important limitations can be underlined. First, valuation of the burdens of different conditions relies, basically, on experts’ judgments of vignettes10,11 rather than on the individual perception of s/he's own disability. Second, vignettes represents single conditions rather than realistic cases with a number of morbidities.12
Here we examine the effects of common conditions on number of days with either full or partial role limitation by using the Spanish data from the World Mental Health Survey (ESEMeD-Spain), which collected information on prevalence of mental disorders and correlates, along with information on physical conditions and disability.
MethodsSurvey methods and sampleThe ESEMeD-Spain study was a country representative cross-sectional household survey of non-institutionalized adult population using a stratified, probability sampling without replacement design. Final sample comprised 5,473 respondents (+18 years), with a response rate of 78.6%. Data collection was conducted between 2001-2002. Response burden was reduced using a two-part interview. Part 1 included the core diagnostic assessment of mood and anxiety disorders and was administered to the whole sample. Part 2 (n=2,121) was administered to respondents with a certain number of mood and anxiety symptoms and to random 25% of those who have not, and included questions about correlates, additional mental disorders and information on physical conditions. Part 2 individuals were weighted by the inverse of probability selection to adjust for differential sampling, and therefore provide data representative of the target adult general population. A more detailed description of sampling methods has been provided elsewhere.13 This study was based on data from part 2 sample.
Measurements- 1.)
Mental disorders
Mental disorders were assessed using the WHO Composite International Diagnostic Interview (CIDI), version 3.0, a fully structured lay-administered interview designed to generate diagnoses of common mental disorders according to the definitions and criteria of both the International Classification of Diseases, 10th revision (ICD-10); and Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV).14 Seven mental disorders were included and grouped into two categories: major depression episode and any anxiety disorder (generalised anxiety disorder, panic and/or agoraphobia, post-traumatic stress disorder, social phobia and specific phobia). To increase recall accuracy only disorders present in the 12-months before the interview were considered.
- 2.)
Physical conditions
Physical conditions were assessed with a checklist based on the U.S. National Health Interview Survey list.15 Respondents were asked to report whether they ever had a number of symptom-based conditions (e.g., headaches) and whether a health professional ever told them they had a series of silent conditions (e.g., hypertension). Physical conditions had to be present in the previous 12 months. Eight conditions or groups of conditions were included: arthritis, chronic pain (back or neck pain), cardiovascular disorders (heart attack, heart disease, hypertension and stroke), diabetes, digestive disorders (stomach or intestine ulcer or irritable bowel disorder), severe headaches or migraines, respiratory disorders (seasonal allergies, asthma, chronic obstructive pulmonary disease, emphysema), and insomnia.
- 3.)
Role functioning
Role functioning was assessed with the modified version of the WHO Disability Assessment Schedule version 2.0 (WHODAS).16 Respondents were asked about the number of days in the last 30 days, in which they were totally unable to carry out their daily life activities (full role limitation) or they were able to perform their daily life activities, but partially (partial role limitation). These numbers were then projected to the whole year by multiplying by twelve. Respondents informed on both (i.e. with full and/or with partial role limitation), except for those respondents who declared to be totally unable to perform daily activities in all previous 30 days, for whom information on the number of days with partial limitation was not collected. Further details on the collection of days with partial role limitation along with information on its construction can be found elsewhere.7
We used multiple regression analysis to assess the joint predictability of mental disorders and physical conditions when using the number of days with full and partial role limitation, controlling for age, sex, employment status, and education. Since co-morbidity among conditions was frequent, the model that provided the best fit for each of the two dependent variables included the common conditions considered, the covariates, the number of conditions starting by two (to avoid colinearitiy) and interaction terms between the number of conditions and each condition.
Since the dependent variables were highly skewed, Generalized Linear Models (GLM) were estimated using ordinary least squares regression. For the full limitation variable the GLM with a log link function and variance proportional to the mean was used as it was the optimal specification. As for the partial limitation model, we used a Gamma-like log-link.17
The predictive effect of a condition on the dependent variables was distributed across a number of coefficients. In order to produce a single term, we estimated first the predicted value of the outcome for each respondent from the coefficients in the final model (base estimate) and then repeated this exercise in modified form nine different times, each time assuming that one of the nine conditions no longer existed (restricted estimate). The individual-level effect of each condition on the outcomes was the mean difference between both estimates among those with the condition. This mean difference is called the additional number of days with either limitation. For societal effects, they were estimated using population attributable risk proportions (PARPs), an indicator interpreted as the proportion of days with either full or partial role limitation that might be reduced when a specific condition is removed from the general population. Estimates of both role functioning variables were calculated based on the actual data, and then under the counterfactual assumption that the condition in question had been removed from the population. We averaged these two estimates across the entire population and computed the percentage difference between them.6,7 Models coefficients are displayed in a supplementary file.
Taylor series linearization method18 implemented in SUDAAN19 to obtain accurate estimates of standard errors and p-values was applied. Standard errors of the individual- and societal-level effects were obtained via Jackknife Resampling.
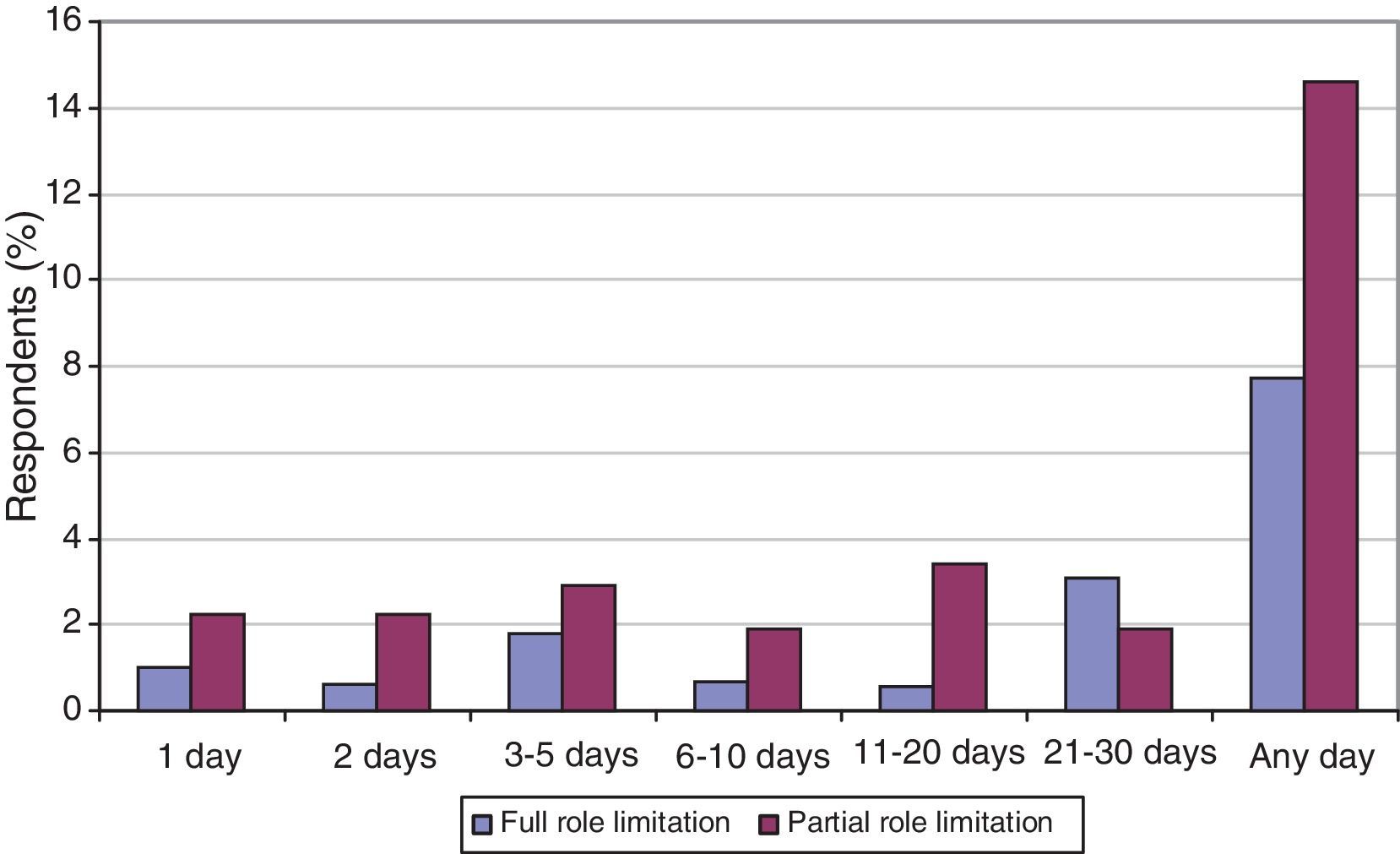
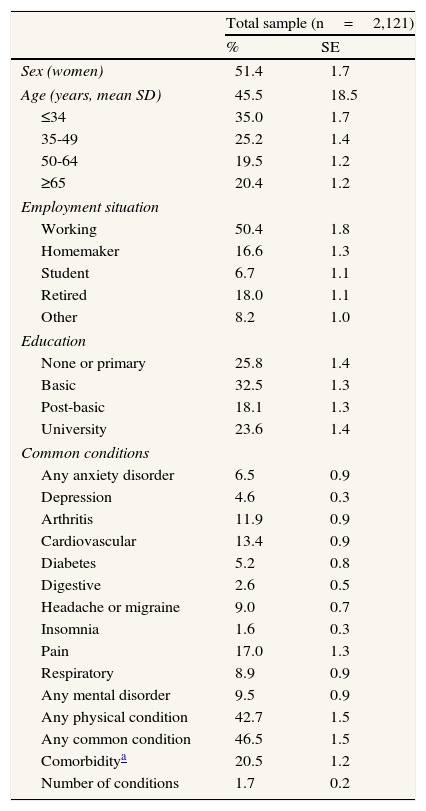
ResultsSocio-demographic characteristics of the ESEMeD-Spain sample are shown in Table 1. The average age of respondents was 45.5 (SE=18.5), and women represented 51.4% (SE=1.7%). About one in two respondents (50.4%) were working at the time of the interview. Almost two-thirds (58.3%) of the sample has reached basic education. Nearly half of the sample (47.1%) had at least one common condition. Anxiety disorders were the most prevalent mental disorder (6.5%) while back/neck pain (17.0%) was the most prevalent physical condition. One fifth of the total sample had two or more conditions, with average of 1.7 conditions. Figure 1 shows the monthly distribution of days with full and partial role limitation. Overall, 7.7% of the sample had at least one day with full role limitation while double the respondents (14.2%) had at least one day with partial role limitation.
Characteristics of the ESEMeD-Spain sample (n=2,121).
| Total sample (n=2,121) | ||
| % | SE | |
| Sex (women) | 51.4 | 1.7 |
| Age (years, mean SD) | 45.5 | 18.5 |
| ≤34 | 35.0 | 1.7 |
| 35-49 | 25.2 | 1.4 |
| 50-64 | 19.5 | 1.2 |
| ≥65 | 20.4 | 1.2 |
| Employment situation | ||
| Working | 50.4 | 1.8 |
| Homemaker | 16.6 | 1.3 |
| Student | 6.7 | 1.1 |
| Retired | 18.0 | 1.1 |
| Other | 8.2 | 1.0 |
| Education | ||
| None or primary | 25.8 | 1.4 |
| Basic | 32.5 | 1.3 |
| Post-basic | 18.1 | 1.3 |
| University | 23.6 | 1.4 |
| Common conditions | ||
| Any anxiety disorder | 6.5 | 0.9 |
| Depression | 4.6 | 0.3 |
| Arthritis | 11.9 | 0.9 |
| Cardiovascular | 13.4 | 0.9 |
| Diabetes | 5.2 | 0.8 |
| Digestive | 2.6 | 0.5 |
| Headache or migraine | 9.0 | 0.7 |
| Insomnia | 1.6 | 0.3 |
| Pain | 17.0 | 1.3 |
| Respiratory | 8.9 | 0.9 |
| Any mental disorder | 9.5 | 0.9 |
| Any physical condition | 42.7 | 1.5 |
| Any common condition | 46.5 | 1.5 |
| Comorbiditya | 20.5 | 1.2 |
| Number of conditions | 1.7 | 0.2 |

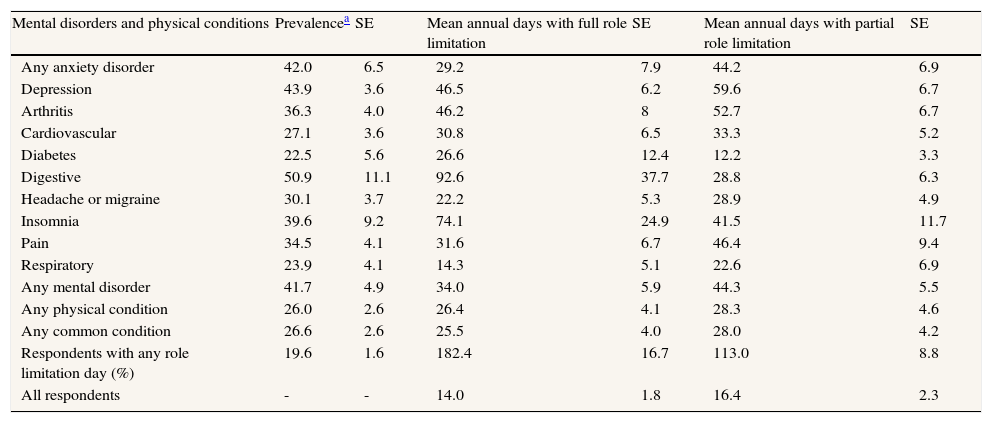
Table 2 shows the prevalence estimates of respondents with role limitations. About 42% of those respondents with mental disorders reported having role limitations. Among those with physical conditions, the figure was about 26%. Digestive, depression and anxiety were the conditions with the highest proportion of respondents with role limitation. Considerable differences in the number of days with full role limitation were observed across conditions. Respondents with any mental disorder reported a large number of days with full role limitation than those with physical conditions (34 vs 26, respectively). Digestive disorders, insomnia, depression and arthritis were the conditions with the highest number of days with full role limitation per year (93, 74, 47, and 46, respectively). Partial role limitation estimates were almost twice in respondents with mental disorders than with physical conditions (44 vs 28, respectively). Depression, arthritis, pain, and anxiety disorders were the conditions with the highest number of days with partial role limitation per year (60, 53, 46, and 44, respectively). Overall 20% of the sample reported to have had some day with role limitation.
Reported days with full and partial role limitation: prevalence and mean number of days per year, according to common conditions (ESEMeD-Spain).
| Mental disorders and physical conditions | Prevalencea | SE | Mean annual days with full role limitation | SE | Mean annual days with partial role limitation | SE |
| Any anxiety disorder | 42.0 | 6.5 | 29.2 | 7.9 | 44.2 | 6.9 |
| Depression | 43.9 | 3.6 | 46.5 | 6.2 | 59.6 | 6.7 |
| Arthritis | 36.3 | 4.0 | 46.2 | 8 | 52.7 | 6.7 |
| Cardiovascular | 27.1 | 3.6 | 30.8 | 6.5 | 33.3 | 5.2 |
| Diabetes | 22.5 | 5.6 | 26.6 | 12.4 | 12.2 | 3.3 |
| Digestive | 50.9 | 11.1 | 92.6 | 37.7 | 28.8 | 6.3 |
| Headache or migraine | 30.1 | 3.7 | 22.2 | 5.3 | 28.9 | 4.9 |
| Insomnia | 39.6 | 9.2 | 74.1 | 24.9 | 41.5 | 11.7 |
| Pain | 34.5 | 4.1 | 31.6 | 6.7 | 46.4 | 9.4 |
| Respiratory | 23.9 | 4.1 | 14.3 | 5.1 | 22.6 | 6.9 |
| Any mental disorder | 41.7 | 4.9 | 34.0 | 5.9 | 44.3 | 5.5 |
| Any physical condition | 26.0 | 2.6 | 26.4 | 4.1 | 28.3 | 4.6 |
| Any common condition | 26.6 | 2.6 | 25.5 | 4.0 | 28.0 | 4.2 |
| Respondents with any role limitation day (%) | 19.6 | 1.6 | 182.4 | 16.7 | 113.0 | 8.8 |
| All respondents | - | - | 14.0 | 1.8 | 16.4 | 2.3 |
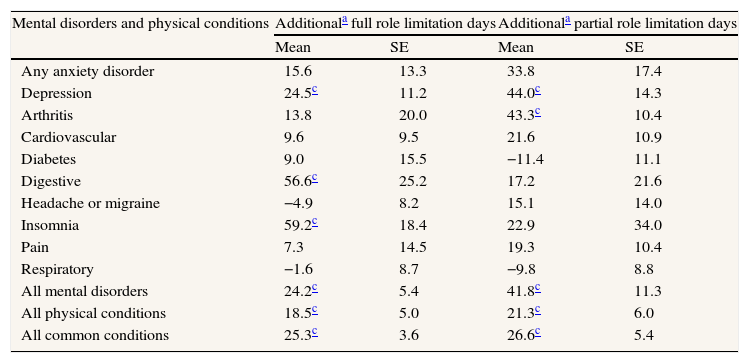
Table 3 shows the additional number of days with full role limitation among respondents with common conditions, when compared to individual not having each of the individual conditions considered per year. Insomnia showed the highest mean number of additional days with full role limitation (59), followed by digestive disorders (57), and depression (25). On the other hand, depression (44), arthritis (43) and anxiety disorders (34) had the highest number of additional days with partial role limitation. Respondents with mental disorders had almost twice as much days with partial role limitation (42) than days with full role limitation (24). Those with physical conditions, on the other hand, had similar number of days for both types of role limitation (19 full and 21 partial role limitation).
Additional yearly days with full and with partial role limitation among individuals with selected common condition (“individual effect”) (ESEMeD-Spain).
| Mental disorders and physical conditions | Additionala full role limitation days | Additionala partial role limitation days | ||
| Mean | SE | Mean | SE | |
| Any anxiety disorder | 15.6 | 13.3 | 33.8 | 17.4 |
| Depression | 24.5c | 11.2 | 44.0c | 14.3 |
| Arthritis | 13.8 | 20.0 | 43.3c | 10.4 |
| Cardiovascular | 9.6 | 9.5 | 21.6 | 10.9 |
| Diabetes | 9.0 | 15.5 | −11.4 | 11.1 |
| Digestive | 56.6c | 25.2 | 17.2 | 21.6 |
| Headache or migraine | −4.9 | 8.2 | 15.1 | 14.0 |
| Insomnia | 59.2c | 18.4 | 22.9 | 34.0 |
| Pain | 7.3 | 14.5 | 19.3 | 10.4 |
| Respiratory | −1.6 | 8.7 | −9.8 | 8.8 |
| All mental disorders | 24.2c | 5.4 | 41.8c | 11.3 |
| All physical conditions | 18.5c | 5.0 | 21.3c | 6.0 |
| All common conditions | 25.3c | 3.6 | 26.6c | 5.4 |
The term additional days is referring to the mean of the difference between the estimated effect obtained from individuals with a particular condition and the effect that would have been obtained if these same individuals wouldn’t have that condition.
bAll models adjusted by age, age squared, sex, employment situation, number of conditions (≥ 2) and interaction terms between numbers and conditions.
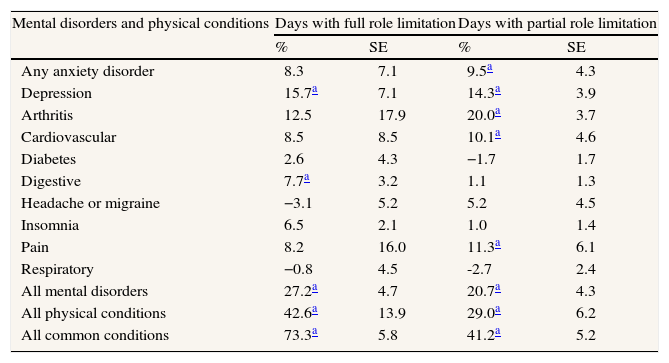
In Table 4, PARPs of days with full and partial limitation for each condition are shown. Overall, all common conditions accounted for 73% of all days with full role limitation and 41% of all days with partial role limitation. Depression contributed to a similar proportion in both functioning outcomes (16% in full role limitation and 14% in partial role limitation). Arthritis (20%) yielded the highest attributable proportion in partial role limitation.
Population attributable risk proportions (PARP) of the number of days with full and with partial role limitation due to common conditions (“societal effect”) (ESEMeD-Spain).
| Mental disorders and physical conditions | Days with full role limitation | Days with partial role limitation | ||
| % | SE | % | SE | |
| Any anxiety disorder | 8.3 | 7.1 | 9.5a | 4.3 |
| Depression | 15.7a | 7.1 | 14.3a | 3.9 |
| Arthritis | 12.5 | 17.9 | 20.0a | 3.7 |
| Cardiovascular | 8.5 | 8.5 | 10.1a | 4.6 |
| Diabetes | 2.6 | 4.3 | −1.7 | 1.7 |
| Digestive | 7.7a | 3.2 | 1.1 | 1.3 |
| Headache or migraine | −3.1 | 5.2 | 5.2 | 4.5 |
| Insomnia | 6.5 | 2.1 | 1.0 | 1.4 |
| Pain | 8.2 | 16.0 | 11.3a | 6.1 |
| Respiratory | −0.8 | 4.5 | -2.7 | 2.4 |
| All mental disorders | 27.2a | 4.7 | 20.7a | 4.3 |
| All physical conditions | 42.6a | 13.9 | 29.0a | 6.2 |
| All common conditions | 73.3a | 5.8 | 41.2a | 5.2 |
Common mental disorders and physical conditions accounted for a substantial proportion of days with full and with partial role limitation. While Spain showed a similar pattern of role limitation due to common conditions, the estimates are considerably higher than comparable data for high income countries.6,7,20 Mental and physical conditions contributed to a similar number of days with full role limitation (around 20 days per year), in contrast with partial role limitation, where mental disorders were responsible for twice the number of days than physical conditions (42 vs 21 days, respectively). This study extends the evidence that mental disorders contribute to substantial productivity losses, specifically through reduced daily performance.21–24 Overall, from a societal perspective, all nine conditions accounted for almost three-quarters of the total number of days with full role limitation, also much higher proportion than that reported for other developed countries.
Depression was associated with a remarkably high number of days with partial limitation. This is consistent with other studies where depression was strongly associated with worse performance at work.25,26 In a recent study with a similar methodology to ours20 carried out in the Netherlands, workers had nearly one month per year with a decreased performance due to major depression. Our finding is fairly consistent but still much higher since it is referring to all adult population and not only to employees. In fact, only half of the population was employed by the time of the study. So, it is worth pointing out that a large part of the burden associated to role limitation due to common conditions in general, and depression in particular, is being bear at a personal level in Spain. Although the scope of this study was not to consider functioning from an economic perspective, the enormous amount of days with partial role limitation reported here might have huge costs for society. It is also interesting to consider the healthy worker bias27 as a possible explanation of the large number of days with role limitation in a country with one of the lowest employment rate (62.7%) in Europe. While no causal relationships can be drawn from our cross-sectional data, it is widely known that there is a higher prevalence rate of health conditions, especially mental disorders in the unemployed population.28
A condition with a high prevalence rate, not always means higher disability. Depression and anxiety, despite of its relatively low prevalence rate,13 presented a higher impact on role functioning. This result is consistent with data reported by Gènova-Maleras et al.,9 where mental disorders ranked first as the most burdensome conditions in Spain. But, as mentioned above, burden of disease studies do not take into account co-morbidities. In our study, condition-specific ratings substantially change after the adjustment for co-morbidities. For instance, respondents with cardiovascular diseases had about 30 days with full role limitation and other 30 days with partial role limitation. But, after the adjustment for co-morbidity, both estimates dropped substantially and did not reach statistical significance. The same happened with other burdensome conditions such as pain, diabetes and respiratory diseases, which ranked in the top ten disease categories in the burden of disease study, and in ours, all three had almost none additional day with role limitation, after co-morbidity adjusment. We used interactions between the number of co-morbidities and each condition as the way of adjustment, allowing interactions to vary across conditions but not across particular pairs or higher number of disorders. While it is unlikely that our interaction model is optimal, we believe it is a useful approach to take into account co-morbidity.12
If the population were entirely unexposed to common physical and mental conditions, days with full limitation would be reduced by 73% and days with partial limitation by 41%. Health conditions explained a great proportion of days with full role limitation, but other non-health related factors come to play when referring to partial limitation.29,30 Work-related factors (e.g. shift work, physical work, employment position, among others) together with non work-related characteristics (e.g. family life, financial situation, adverse life events, among others)31 have shown to be relevant in explaining work performance. For instance, the ITSAL project (Immigration, Work and Health, for the Spanish acronym) found that the immigration status was one of the most important predictors of sickness presenteeism in Spain (OR=1.77; 95%CI: 1.24-2.53).32 We speculate that there are contextual factors that modulate the association between common health conditions and work functioning, which might be important to investigate in order to give a complete picture of determinants of lost productivity in Spain.
LimitationsA number of limitations should be taken into account when interpreting our results. First, only a limited number of common conditions were included in the analysis and some were pooled to form larger disorder groups. Grouping illnesses with different degrees of severity (e.g. hypertension and stroke) may have lead to a less impact on functional disability. Burdensome conditions such as dementia and psychosis were not assessed in the ESEMeD survey. Such conditions cause a great impairment not only to the patients but to their caregivers and their families, so we might have underestimated the number of days with disability. In addition, cancer, neurological disorders, and substance abuse were not considered because they had very low prevalence rates (0.25, SE=0.09; 0.23, SE=0.08; 0.60, SE=0.21, respectively). Future research on this subject should include the above-mentioned conditions along with an expansion and disaggregation of those already included. Second, while mental disorders were assessed with a well-established research method,14 diagnoses of physical conditions were self-reported. There is evidence of good correspondence between self-reported somatic conditions such as diabetes, heart disease and asthma, and general practitioner records.33 Nevertheless, cultural or other socio-demographic variables (e.g., poor health literacy or low education, among others) could have affected our results. Most likely, we have underestimated the effect of physical conditions on role functioning.6 Third, the time frame in which we assessed role functioning was limited to the 30 days before the interview and then the numbers in this recall interval were projected to the whole year improving the comparability with published literature.6,7 This recall period may have missed a severe exacerbation present in the previous year but not in the month prior to the interview, or in the other way round. This recall period may have missed a severe exacerbation present in the previous year but not in the month prior to the interview, or in the other way round. Furthermore, some disorders have a seasonal behaviour (e.g., seasonal allergy) and others may have only one episode in a year (e.g., stroke). But, since large numbers of events were assessed, we expected to cancel out this effect. Anyway, a detailed analysis of the influence of the recall period by disorders may be advisable in future investigations. In addition, it is worth mentioning that the simulation method used to evaluate marginal effects of individual conditions implicitly assumes that the presence versus absence of a single condition can be changed while holding constant all other conditions. This assumption would be plausible if all co-morbid conditions were either causes or risk markers34 of focal conditions. However, in cases where the co-morbid condition is a consequence of the focal condition or where two or more conditions are reciprocally related, the method used here will overestimate the effect of the co-morbid condition, as we exposed before. In addition, some negative estimates and large standard errors are related with small sample size especially in certain conditions. Lastly, data were collected between 2001-2002, thus it is possible that our results do not reflect the current association between role limitation and mental and physical conditions in Spain. However, we are not aware of any more recent report that is as exhaustive and internationally comparable assessing the effect of both mental and physical disorders on role functioning in Spain. Therefore, evidence presented here is currently relevant and allows a better understanding of this subject.
All in all, this is a valid first approach to the effect of common conditions on role functioning using a representative sample of the Spanish population. In addition, public-health societal perspective is used for the first time to give an overall distribution of role limitation cause by common conditions taking into account co-morbidities in Spain.
Cross-national analyses showed a substantial, but comparable impact of mental disorders and physical conditions on partial and full role limitation. Context matters in disability, thus country specific data is needed to know the extent and the experience of disability associated to common health conditions in Spain.
What this study adds to the literatureSpain showed a similar pattern of role limitation due to common health conditions, but estimates are considerably higher than comparable data for high income countries. Mental disorders, despite its relatively low prevalence rate in Spain, were associated with a considerable number of days with partial role limitation. A comprehensive and systematic collection of data on people with role limitation seems necessary as it could allow monitoring role limitation distribution. Such an information system would also allow evaluating the need of effective interventions to reduce role limitation among those with common conditions in Spain.
All authors have participated actively in the study, and have read and approved the submitted manuscript. J.M. Haro and C. García Forero were involved in the conception and design of the study and critically reviewed the manuscript; G. Barbaglia was involved in the conception and design of the study, the analysis and interpretation of data, and she was responsible for drafting the manuscript; N. Durán were involved in the analysis and interpretation of data and critically reviewed the manuscript; G. Vilagut and J. Alonso were involved in the conception and design of the study, the analysis and interpretation of data, and critically reviewed the manuscript. All authors provided final approval for the manuscript submitted.
FundingThis work was supported by the European Commission (QLG5-1999-01042, SANCO 2004123, EAHC 20081308), the Piedmont Region (Italy), Fondo de Investigación Sanitaria, Instituto de Salud Carlos III, Spain (FIS 00/0028-02), Ministerio de Ciencia y Tecnología, Spain (SAF 2000-158-CE), Departament de Salut, Generalitat de Catalunya, Spain, and other local agencies and by an unrestricted educational grant from GlaxoSmithKline. ESEMeD is carried out in conjunction with the World Health Organization World Mental Health (WMH) Survey. The EU Contribution to The World Mental Health (WMH) Surveys Initiative was funded by the Executive Agency for Health and Consumers (EAHC), European Comission (SANCO 2008-1308). G. Barbaglia is supported by Ministerio de Ciencia e Innovación Rio Hortega grant (CM 10-00099). C. García Forero is supported by Ministerio de Ciencia e Innovación FSE grant (JCI-2009-05486).
Conflict of interestNone.
We thank the WMH staff for their assistance with instrumentation, fieldwork, and data analysis. A complete list of WMH funding support and publications can be found at http://www.hcp.med.harvard.edu/wmh. In addition, the authors would like to thanks Ana Boskovic for her contribution to the readability of the manuscript.












