



To analyze the construct validity and the internal consistency of the 12-item Bem Sex Role Inventory (BSRI-12) questionnaire and to study the association between gender stereotypes and sexual risk practices in men who have sex with men (MSM).
MethodsCross-sectional study of 601 MSM who voluntarily and anonymously responded to an online survey on risk practices and gender stereotypes. The BSRI-12 was used to obtain gender stereotypes (masculine, feminine, undifferentiated and androgynous). For data analysis, exploratory factor analysis (EFA) of the BSRI-12 and logistic regression were performed.
ResultsTwo main factors (Cronbach alpha 0.95 and 0.81) were obtained from the EFA. Using the androgynous roles as the reference category, we found lower odds of engaging in unprotected anal intercourse (UAI) among those who endorse feminine roles (OR: 0.53; 95%CI: 0.29-0.95). Endorsing masculine roles with alcohol consumption (OR: 1.92; 95%CI: 1.15-3.20) or the undifferentiated when not knowing the partner's serological status (OR: 1.55; 95%CI: 1.02-2.35) were associated with higher odds of UAI compared to those endorsing the androgynous roles. Undifferentiated participants also perform receptive UAI using poppers (OR: 2.19; 95%CI: 1.24-3.87), and insertive UAI not knowing the serological status of the sexual partner (OR: 1.69; 95%CI: 1.04-2.76) compared to androgynous participants.
ConclusionThe BSRI is a valid and consistent instrument for identifying gender stereotypes in MSM. A greater proportion of participants within the undifferentiated and the masculine category engage in risk practices with the influence of substance consumption and unawareness of their sexual partner's serological status. The information obtained may be useful to define intervention and prevention programs.
Analizar la validez de constructo y la consistencia interna del cuestionario Bem Sex Role Inventory (BSRI-12) y estudiar la asociación entre estereotipos de género y prácticas sexuales de riesgo en hombres que tienen sexo con hombres (HSH).
MétodosEstudio transversal con 601 HSH que de manera anónima y voluntaria respondieron a un cuestionario online sobre prácticas de riesgo y estereotipos de género. Se utilizó el cuestionario BSRI-12 sobre estereotipos de género (masculino, femenino, indiferenciado y andrógino). Se realizó un análisis factorial exploratorio (AFE) del BSRI-12 y regresión logística.
ResultadosSe obtuvieron dos factores principales (alfa de Cronbach: 0,95 y 0,81). Utilizando el rol andrógino como categoría de referencia, encontramos menores odds ratios (OR) de realizar penetración anal sin condón (PASC) entre aquellos pertenecientes a roles femeninos (OR: 0,53; intervalo de confianza del 95% [IC95%]: 0,29-0,95). Los roles masculinos con consumo de alcohol (OR: 1,92; IC95%: 1,15-3,20) y los indiferenciados con desconocimiento del estado serológico de la pareja (OR: 1,55; IC95%: 1,02-2,35) se asociaron con mayores OR de PASC en comparación con los roles andróginos. Los indiferenciados realizaron más PASC usando popper (OR: 2,19; IC95%: 1,24-3,87) y PASC insertiva con desconocimiento del estado serológico de la pareja sexual (OR: 1,69; IC95%: 1.04-2.76) en comparación con los andróginos.
ConclusiónEl BSRI es un instrumento consistente y válido para identificar estereotipos de género en los HSH. Los participantes de las categorías indiferenciado y masculino realizan más prácticas de riesgo bajo la influencia de sustancias y desconociendo el estado serológico de las parejas. La información obtenida es útil para definir programas de intervención y prevención.
Sexually transmitted infections continue to spread in men who have sex with men (MSM) globally1 and various authors consider them to be under-diagnosed.2 It is necessary to identify factors associated to sexual risk practices engagement in these men. The most studied risk practices in MSM have been unprotected anal intercourse (UAI), both receptive and insertive3 and bareback or intentional and premeditated condomless anal intercourse.4,5 Currently, other practices such as oral sex, rimming or sex toys are being considered.6
Different variables have been found associated to risk practices among MSM such as drug consumption,7 knowledge of sexual partner's serological status,8 depression,9 and socio-economic characteristics.10 Recent studies have highlighted that being a man is used to justify the engagement in risk practices, since it is socially accepted that men have more need for sex, supporting the idea that masculinity plays an essential role in said practices in MSM.11
The sex-gender system is a structure that places people within limits, expected behaviors and demands regarding distinctions that culture establish based on biological characteristics. This dichotomous system (man/woman) influences the subjectivities, organizes social interactions, institutions and people's lives, as well as their sexuality, their practices and their ways of relating. Gender is taken as a socially accepted strategy to legitimize social inequalities12 and specifies the roles to be carried out, being considered a determinant of health,13 since it conditions access to health services, the type of prevention and health promotion campaigns, diagnostic and therapeutic efforts, cares and care planning.14
Zeglin5 found the consumption of drugs in those men that fit within the demands of traditional norms of masculinity7 which has been identified as a determinant of risk behavior in various populations of MSM.15,16 Since the hegemonic model reports more benefits in social and sexual intercourses, if the relationship does not fit with hegemonic model, the MSM sometimes develop hypermasculinization behaviors to achieve greater legitimacy.17,18 To better understand how people construct their sexual relationships, some studies highlighted the importance of breaking the gender dichotomy. Gender relational approach proposed by Connell19 suggests studying masculinity as a changing, dynamic and multidimensional fact. More research is needed about how non-hegemonic masculinities play with regard to how men build their gender identity, while this situation is managed in the gendered social relations and sexual intercourses, even rejecting traditional norms of masculinity and shaping alternative masculinities, which face gender structure impositions.20 This could be one starting point for analyze whether the different gender stereotypes are associated with sexual risk practices in MSM.
Some masculinity/femininity scales are associated with differences in psychological traits as a function of masculinity/femininity: emotional empathy, assertiveness, achievement and affiliation motivation, and social communication skills. It is difficult to find instruments that allow researchers to apply a quantitative methodology that could give a vision of how the gender stereotypes are distributed in the population of MSM. The Bem Sex Role Inventory (BSRI),21 a questionnaire based on stereotypes, which are perceived socially as masculine (instrumental traits) or feminine (expressive traits) and that contributes other possibilities such as androgynous (both instrumental and expressive) and undifferentiated (lack of both instrumental and expressive), may be used in order to analyze the perceptions of MSM in relation to gender stereotypes. This tool will allow us to relate the results based on the gender relational approach and to identify the diverse relations between masculinities: hegemony, complicity, subordination and marginalization17 according to the categories of the BSRI questionnaire. Taking into account that no measurement tools have been found to analyze the gender stereotypes in MSM further than the traditional masculinity,22 in this study the hypothesis proposed is that BSRI is a valid tool for identifying the gender stereotypes in MSM and will allow us to analyze the different forms of constructing sexual affective relations among MSM. It has been shown that the commitment to hegemonic values determines the risk practices engagement, but it remains to analyze those situations that they have when they are placed in lower positions of this hierarchy of masculinities explained by the gender relational approach.
The aim of this study is to analyze the validity of the construct and the internal consistency of the BSRI questionnaire in our population of MSM and to study the association between the gender stereotypes and sexual risk practices.
MethodsA cross-sectional study in 601 MSM who voluntarily and anonymously responded to an online survey on sexual risk practices and gender stereotypes was conducted. For the data collection, a questionnaire based on other studies on the same subject was designed23 and the abbreviated BSRI-12 items initially developed among university students from Spain24 and validated in Hispanic population25–27 was used. It was posted on a website and spread through social networks such as Facebook, and lesbian, gay, transgender, bisexual, intersexual and queer (LGBTIQ) organizations, OMSIDA Zaragoza and state coordinator of HIV-AIDS organizations (CESIDA). The questionnaires were available from June 2014 to January 2015. Inclusion criteria were to be a man who had sex with a man in the last 12 months. Participants were informed about the scope of this research. The study meets the requirements of Law 14/2007 of 3 July Biomedical Research and the Ethics Committee for Clinical Research of Aragon approved the research.
Gender stereotype variable, categorized into feminine, masculine, androgynous and undifferentiated was measured according to BSRI-12. The masculine traits refer to the aspects of self-confidence and of the establishment and achievement of goals, while the feminine traits refer to aspects of affection, expression and concern for the welfare of others. The BSRI also contributes the androgynous category, when both the masculine and the feminine traits score high on the questionnaire, and the undifferentiated category, when both give low scores. Participants were asked to describe how they perceived themselves, from 1 to 7 (totally agree-totally disagree) each one of the twelve items in the questionnaire.
As independent variables, socioeconomic data were included age: up to 24 years, 25 to 49, and over 49 years; educational level: up primary (12 years), secondary (12-18) and university (over 18 years); employment status: employed, unemployed, students or pensioners; monthly income level: less than 700 €, between 700-1200 € and over 1200 €; and living situation: a couple, alone, others. Place of origin variable registering Europe, North and South America and Canada was also included and it was dichotomized into European and others.
Sexual risk practices were included: receptive and insertive unprotected anal intercourse (RUAI/IUAI) according to seroconcordant, serodiscordant or unknown serological status of the sexual partner. Other practices such as bareback (intentional and premeditated condomless anal intercourse), oral sex, rimming and sex toys were also included. The variables concerning sexual risk practices and substance consumption (cannabis, cocaine, poppers and alcohol) were answered: never, sometimes and usually, which were dichotomized into never and sometimes/usually.
To assess the BSRI-12 construct validity in MSM, an exploratory factor analysis of main components was performed. We use varimax rotation because no correlation between factors was found and this method is more robust, easier to explain and reproduce.28 To ascertain the applicability of such factor analysis in our population, it was considered that the Bartlett Sphericity test was significant (p<0.05) and the measure of sampling adequacy Kaiser-Meyer-Olkin (KMO), higher than 0.75.29
Once the factor analysis was performed, we included those factors with eigenvalues greater than 1.30 To assign items to factors, factor loadings equal or greater than 0.5 were considered. To assess the internal consistency of the factors, Cronbach's alpha coefficients for each of them were valued, requiring those higher than 0.7531 to be assessed.
The factorial analysis showed two well differentiated factors: factor 1, corresponded with the characteristics of feminine category, and factor 2, which matched the characteristics of masculine. Then the scores of each of the two factors separately, were dichotomized by the median value, thus considering both scores together, the four categories of the variable gender role proposed21 were generated: feminine (score over the median in factor 1 and below the median in factor 2); masculine (over the median in factor 2 and below in factor 1); androgynous (over the median in both factors); and undifferentiated (below the median in both factors).
To analyze the relationship between gender stereotype and the rest of variables, logistic regression models were constructed for each variable using the androgynous roles as the reference category, following the contributions of the Bem model that indicates that it is this category that shows better results in health and that therefore it could be expected, greater protection to sexual risk practices engagement. Among the estimators obtained the odds ratio (OR) was taken into account with its 95% confidence interval (95%CI). The required level of significance was p<0.05 and the statistical packaged used was SPSS-22.
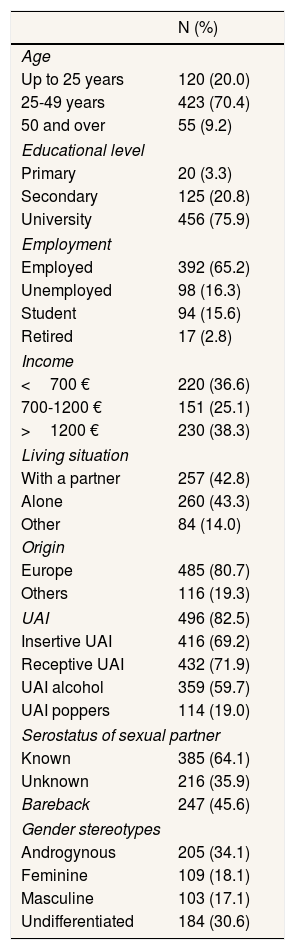
ResultsA total of 601 MSM aged 16 to 69 with an average of 34 years (standard deviation: 10.50) participated in the study. As shown in Table 1, the majority of participants had university studies and they were working, earning more than 1200 € per month, lived in pairs or alone and were mostly European. The majority performed UAI and also performed it under the effects of the alcohol. From de total data, 46% performed bareback and 36% were unaware of their partner's HIV status.
Socio-demographic data of the total sample.
| N (%) | |
|---|---|
| Age | |
| Up to 25 years | 120 (20.0) |
| 25-49 years | 423 (70.4) |
| 50 and over | 55 (9.2) |
| Educational level | |
| Primary | 20 (3.3) |
| Secondary | 125 (20.8) |
| University | 456 (75.9) |
| Employment | |
| Employed | 392 (65.2) |
| Unemployed | 98 (16.3) |
| Student | 94 (15.6) |
| Retired | 17 (2.8) |
| Income | |
| <700 € | 220 (36.6) |
| 700-1200 € | 151 (25.1) |
| >1200 € | 230 (38.3) |
| Living situation | |
| With a partner | 257 (42.8) |
| Alone | 260 (43.3) |
| Other | 84 (14.0) |
| Origin | |
| Europe | 485 (80.7) |
| Others | 116 (19.3) |
| UAI | 496 (82.5) |
| Insertive UAI | 416 (69.2) |
| Receptive UAI | 432 (71.9) |
| UAI alcohol | 359 (59.7) |
| UAI poppers | 114 (19.0) |
| Serostatus of sexual partner | |
| Known | 385 (64.1) |
| Unknown | 216 (35.9) |
| Bareback | 247 (45.6) |
| Gender stereotypes | |
| Androgynous | 205 (34.1) |
| Feminine | 109 (18.1) |
| Masculine | 103 (17.1) |
| Undifferentiated | 184 (30.6) |
UAI: unprotected anal intercourse; bareback: intentional and premeditated condomless anal intercourse.
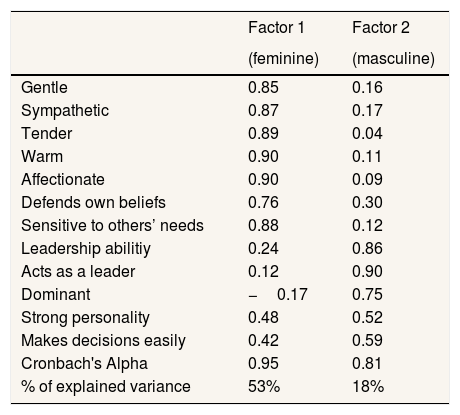
It is possible to perform an exploratory factor analysis, since the Bartlett Sphericity testis significant (p<0.01) and the measure of sampling adequacy Kaiser-Meyer-Olkin (KMO) of 0.90. From this analysis, two main factors were drawn, both with eigenvalues greater than 1. The first factor “feminine” included those items: gentle, sympathetic, tender, warm, affectionate, sensitive and defends own beliefs, with a score between 0.76 and 0.90, accounting for 53% of the total variance and Cronbach's alpha of 0.95. The second factor “masculine” included items: leadership abilities, acts as a leader, dominant, strong personality and makes decisions easily, that scored between 0.59 and 0.90, accounting for 18% of the total variance and Cronbach's alpha coefficient of 0.81. Masculine traits have low saturations in factor 1 “feminine” and, conversely, feminine traits score low on factor 2 “masculine” (Table 2).
Rotated matrix component. Factor analysis.
| Factor 1 | Factor 2 | |
|---|---|---|
| (feminine) | (masculine) | |
| Gentle | 0.85 | 0.16 |
| Sympathetic | 0.87 | 0.17 |
| Tender | 0.89 | 0.04 |
| Warm | 0.90 | 0.11 |
| Affectionate | 0.90 | 0.09 |
| Defends own beliefs | 0.76 | 0.30 |
| Sensitive to others’ needs | 0.88 | 0.12 |
| Leadership abilitiy | 0.24 | 0.86 |
| Acts as a leader | 0.12 | 0.90 |
| Dominant | −0.17 | 0.75 |
| Strong personality | 0.48 | 0.52 |
| Makes decisions easily | 0.42 | 0.59 |
| Cronbach's Alpha | 0.95 | 0.81 |
| % of explained variance | 53% | 18% |
KMO for the adequacy of the sample: 0.90.
p-value of Barlett sphericity test:<0.01.
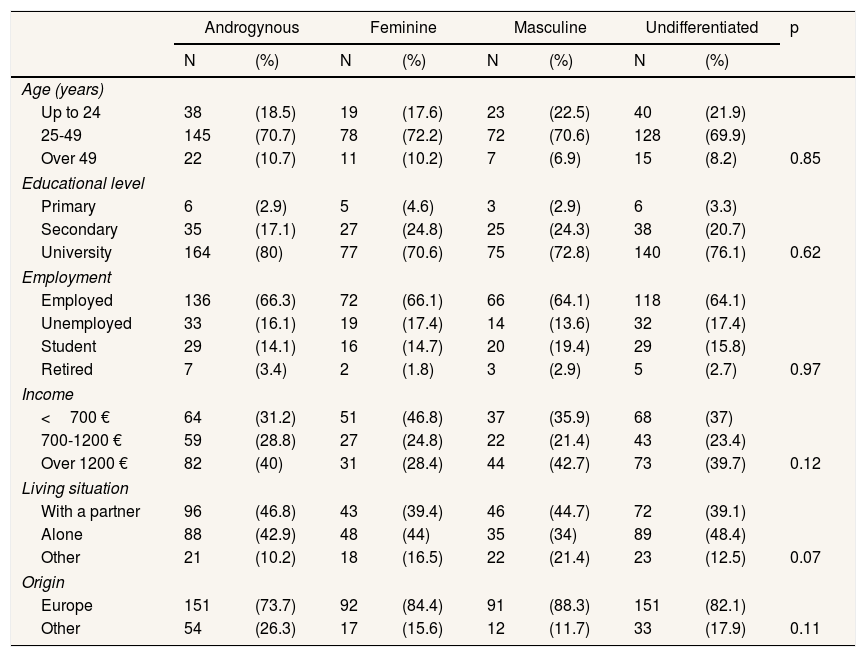
After classifying the participants according to gender stereotypes, the androgynous category (34.1%) was predominant, followed by the undifferentiated (30.6%), feminine (18.1%) and masculine (17.1%). There were no statistically significant differences between gender stereotypes and socio-demographic characteristics (Table 3).
Categories of gender stereotypes and socio-economic variables.
| Androgynous | Feminine | Masculine | Undifferentiated | p | |||||
|---|---|---|---|---|---|---|---|---|---|
| N | (%) | N | (%) | N | (%) | N | (%) | ||
| Age (years) | |||||||||
| Up to 24 | 38 | (18.5) | 19 | (17.6) | 23 | (22.5) | 40 | (21.9) | |
| 25-49 | 145 | (70.7) | 78 | (72.2) | 72 | (70.6) | 128 | (69.9) | |
| Over 49 | 22 | (10.7) | 11 | (10.2) | 7 | (6.9) | 15 | (8.2) | 0.85 |
| Educational level | |||||||||
| Primary | 6 | (2.9) | 5 | (4.6) | 3 | (2.9) | 6 | (3.3) | |
| Secondary | 35 | (17.1) | 27 | (24.8) | 25 | (24.3) | 38 | (20.7) | |
| University | 164 | (80) | 77 | (70.6) | 75 | (72.8) | 140 | (76.1) | 0.62 |
| Employment | |||||||||
| Employed | 136 | (66.3) | 72 | (66.1) | 66 | (64.1) | 118 | (64.1) | |
| Unemployed | 33 | (16.1) | 19 | (17.4) | 14 | (13.6) | 32 | (17.4) | |
| Student | 29 | (14.1) | 16 | (14.7) | 20 | (19.4) | 29 | (15.8) | |
| Retired | 7 | (3.4) | 2 | (1.8) | 3 | (2.9) | 5 | (2.7) | 0.97 |
| Income | |||||||||
| <700 € | 64 | (31.2) | 51 | (46.8) | 37 | (35.9) | 68 | (37) | |
| 700-1200 € | 59 | (28.8) | 27 | (24.8) | 22 | (21.4) | 43 | (23.4) | |
| Over 1200 € | 82 | (40) | 31 | (28.4) | 44 | (42.7) | 73 | (39.7) | 0.12 |
| Living situation | |||||||||
| With a partner | 96 | (46.8) | 43 | (39.4) | 46 | (44.7) | 72 | (39.1) | |
| Alone | 88 | (42.9) | 48 | (44) | 35 | (34) | 89 | (48.4) | |
| Other | 21 | (10.2) | 18 | (16.5) | 22 | (21.4) | 23 | (12.5) | 0.07 |
| Origin | |||||||||
| Europe | 151 | (73.7) | 92 | (84.4) | 91 | (88.3) | 151 | (82.1) | |
| Other | 54 | (26.3) | 17 | (15.6) | 12 | (11.7) | 33 | (17.9) | 0.11 |
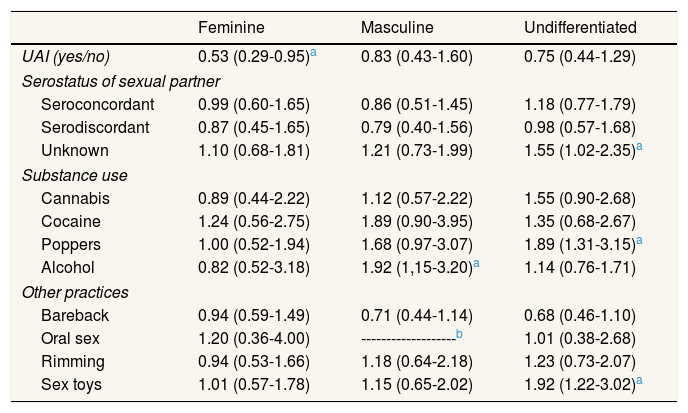
As shown in Table 4, belonging to the feminine category acts as a protective factor (OR: 0.53; 95%CI: 0.29-0.95) when performing UAI compared to those belonging to the androgynous. Participants included in the masculine category were 1.92 times more likely to perform UAI under the influence of alcohol (95%CI: 1.15-3.20). Those within the undifferentiated category are 1.55 times more likely to perform this practice unknowing the serological status of their partner (95%CI: 1.02-2.35) and also to perform it using popper (OR: 1.89; 95%CI: 1.31-3.15). Those belonging to the undifferentiated category also have a higher risk of using unprotected sex toys (OR: 1.92; 95%CI: 1.22-3.02).
Categories of gender stereotypes and unprotected anal intercourse according to serostatus, substance use and other risk practices in men who have sex with men. Logistic regression.
| Feminine | Masculine | Undifferentiated | |
|---|---|---|---|
| UAI (yes/no) | 0.53 (0.29-0.95)a | 0.83 (0.43-1.60) | 0.75 (0.44-1.29) |
| Serostatus of sexual partner | |||
| Seroconcordant | 0.99 (0.60-1.65) | 0.86 (0.51-1.45) | 1.18 (0.77-1.79) |
| Serodiscordant | 0.87 (0.45-1.65) | 0.79 (0.40-1.56) | 0.98 (0.57-1.68) |
| Unknown | 1.10 (0.68-1.81) | 1.21 (0.73-1.99) | 1.55 (1.02-2.35)a |
| Substance use | |||
| Cannabis | 0.89 (0.44-2.22) | 1.12 (0.57-2.22) | 1.55 (0.90-2.68) |
| Cocaine | 1.24 (0.56-2.75) | 1.89 (0.90-3.95) | 1.35 (0.68-2.67) |
| Poppers | 1.00 (0.52-1.94) | 1.68 (0.97-3.07) | 1.89 (1.31-3.15)a |
| Alcohol | 0.82 (0.52-3.18) | 1.92 (1,15-3.20)a | 1.14 (0.76-1.71) |
| Other practices | |||
| Bareback | 0.94 (0.59-1.49) | 0.71 (0.44-1.14) | 0.68 (0.46-1.10) |
| Oral sex | 1.20 (0.36-4.00) | -------------------b | 1.01 (0.38-2.68) |
| Rimming | 0.94 (0.53-1.66) | 1.18 (0.64-2.18) | 1.23 (0.73-2.07) |
| Sex toys | 1.01 (0.57-1.78) | 1.15 (0.65-2.02) | 1.92 (1.22-3.02)a |
UAI: unprotected anal intercourse.
Reference value: androgynous.
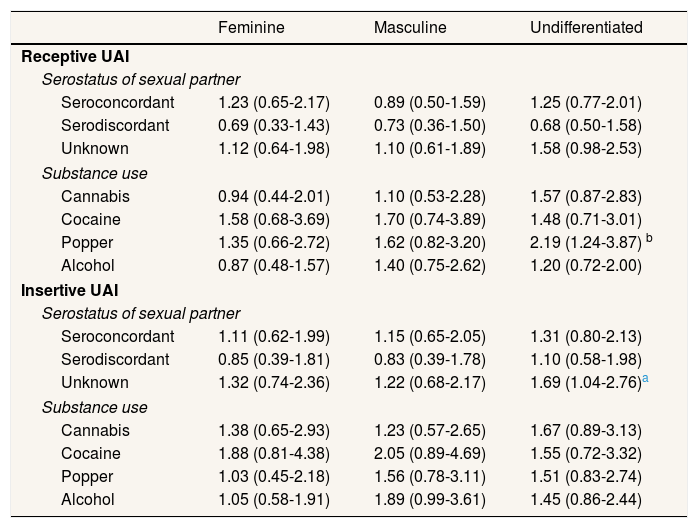
Analyzing the differences between gender categories and IUAI/RUAI (Table 5), we observe that those belonging to the undifferentiated category are those most likely to perform RUAI under the effects of popper (OR: 2.19; 95%CI: 1.24-3.87) and to perform IUAI unknowing the serological status of the sexual partner (OR: 1.69; 95%CI: 1.04-2.76).
Categories of gender stereotypes and receptive and insertive unprotected anal intercourse according to serostatus and substance use in men who have sex with men. Logistic regression.
| Feminine | Masculine | Undifferentiated | |
|---|---|---|---|
| Receptive UAI | |||
| Serostatus of sexual partner | |||
| Seroconcordant | 1.23 (0.65-2.17) | 0.89 (0.50-1.59) | 1.25 (0.77-2.01) |
| Serodiscordant | 0.69 (0.33-1.43) | 0.73 (0.36-1.50) | 0.68 (0.50-1.58) |
| Unknown | 1.12 (0.64-1.98) | 1.10 (0.61-1.89) | 1.58 (0.98-2.53) |
| Substance use | |||
| Cannabis | 0.94 (0.44-2.01) | 1.10 (0.53-2.28) | 1.57 (0.87-2.83) |
| Cocaine | 1.58 (0.68-3.69) | 1.70 (0.74-3.89) | 1.48 (0.71-3.01) |
| Popper | 1.35 (0.66-2.72) | 1.62 (0.82-3.20) | 2.19 (1.24-3.87) b |
| Alcohol | 0.87 (0.48-1.57) | 1.40 (0.75-2.62) | 1.20 (0.72-2.00) |
| Insertive UAI | |||
| Serostatus of sexual partner | |||
| Seroconcordant | 1.11 (0.62-1.99) | 1.15 (0.65-2.05) | 1.31 (0.80-2.13) |
| Serodiscordant | 0.85 (0.39-1.81) | 0.83 (0.39-1.78) | 1.10 (0.58-1.98) |
| Unknown | 1.32 (0.74-2.36) | 1.22 (0.68-2.17) | 1.69 (1.04-2.76)a |
| Substance use | |||
| Cannabis | 1.38 (0.65-2.93) | 1.23 (0.57-2.65) | 1.67 (0.89-3.13) |
| Cocaine | 1.88 (0.81-4.38) | 2.05 (0.89-4.69) | 1.55 (0.72-3.32) |
| Popper | 1.03 (0.45-2.18) | 1.56 (0.78-3.11) | 1.51 (0.83-2.74) |
| Alcohol | 1.05 (0.58-1.91) | 1.89 (0.99-3.61) | 1.45 (0.86-2.44) |
Reference value: androgynous.
UAI: unprotected anal intercourse.
We found that 82.5% of the participants performed UAI and 75.9% were well educated. A study developed in Spain found that 54.8% had UAI and 58.6% had university studies. Although in both cases more than a half of the population performed UAI, we found 27.7% more MSM engaging in UAI than the mentioned study, but it must be taken into account that in our population there were 17.3% more MSM with university studies. Related to these differences, it can be said that in general, our results are consistent with those of the aforementioned study.32
In this study, the BSRI-12 showed construct validity in the identification of “feminine” and “masculine” factors, as the two together explain 71% of the variance with a Cronbach alpha of 0.91. These two factors permit the establishment of the four categories in agreement with the model proposed by Bem,21 and it is therefore considered to be a useful tool to describe the perceptions the MSM have with regard to the gender stereotypes. The results demonstrate the association between gender stereotypes and the engagement in sexual risk practices. Although not statistically significant differences were achieved at all times, clinical and social implications exist.
The BSRI-12 has been used in this study because no specific instruments exist to analyze the gender stereotypes in MSM. This discussion has been structured identifying and relating each one of the BSRI stereotypes, masculine, feminine, androgynous and undifferentiated, with those proposed by Connell, hegemony, subordination, complicity and marginalization.17 Connell's proposal gives us clues to analyze the diversity of relationships among masculinities, which also occurs (as this study contends) in MSM. This it is not a typologization or a series of fixed categories, but an approximation about how power, control and benefits provided by the hegemonic masculinity affect the way in which MSM's sexual practices are developed and how they construct different ways of relating, assuming that masculinities are understood as acts of gender that conform subjectivity, in a dynamic relational arena.17
Belonging to the feminine category acts as a significant protective factor for UAI, which do not coincide with a study carried out in Perú, in which those who assumed feminine stereotypes performed mostly risk practices, since they were considered to be weaker and could not manage the situation in sexual encounters.16 Relations of subordination presented by Connell, place those who fulfill feminine stereotypes at the lowest level of the gender hierarchy and by this fact, enjoy less benefits and less power in relationships.
Contrary to what might be expected, participants within the masculine category were not those who most risk practices performed. But nevertheless, different studies found association between traditional masculinity and risk practices.15,16 Although we did not found this same association, we observed a greater proportion of risk practices in this category when they were performed under the effects of alcohol.33 This traditional masculinity, which responds to cultural ideals about how men should behave, highlighting risk taking among others, has been described by Connell17 as relations of hegemony, it is said close to the hegemonic model of masculinity demands.
Participants who perceive themselves in the undifferentiated category have a higher risk to risk practices engagement under the effects of alcohol and poppers, use sex toys without protection and perform IUAI without knowing their sexual partners’ serological status. We consider that these circumstances place them in a situation of greater vulnerability when compared to the other gender categories. Inequality positions indicated in other studies are being young34 or a migrant,35 identified as factors of vulnerability to risk practices. This category might correspond to marginalization relations in Connell's classification.17 We understand that the negotiation difficulties assigned to the undifferentiated according to Bem's model, and the lack of preventive strategies developed within the above-mentioned contexts, may lead to risk practices engagement within these vulnerability situations.
Differences found in the gender categories compared to the androgynous and the major probability of risk practices engagement found within undifferentiated category, could be understood within the androgyny model expectations,21 which contributes that the undifferentiated have worse health outcomes. Given that there are no publications that used BSRI-12 in MSM, we might suggest that those situations in which other gender categories represent a protection against the risk practices engagement, are showing that in the case of MSM, analysis of gender relations should be reconsidered. This is the case of feminine stereotypes that protect against UAI, RUAI with serodiscordant partners and masculine that protects against bareback or RUAI with serodiscordant partners.
In recent decades, various studies have suggested that the behavior of men has changed and has acquired other traits, which are not exclusive to hegemonic masculinity. It has incorporated features traditionally defined as feminine to be adapted to the demands of changing societies.19 This might explain that even though their feminine traits facilitate their social acceptance, their characteristics of hegemonic masculinity still prevail and lead to hypermasculinization behavior,18 assuming sexual risk practices. Following our interpretation, it would be these who have complicity relations with the hegemonic project.17
Finally, there are no differences between self-perceived gender stereotypes and socio-demographic variables which, according to some authors, may suggest the transnational scope of the gender structure,15,19 as well as how the pressure of the hegemonic model, facilitates the risk practices engagement in MSM.5 It would be interesting to apply similar tools and studies to be able to compare these findings within other cultures.
Among the weaknesses of this study, we may indicate those derived from the cross-sectional design which does not allow the establishment of the cause-effect association, together with those inherent to the data collection, voluntary and via Internet, which means that many MSM will not have had access to it. Future studies using prospective study designs are necessary to examine the longitudinal nature of these associations.
Among the contributions, information from the BSRI-12 allows us to question dichotomous thought regarding gender and facilitates the identification of vulnerability situations determining sexual risk practices in MSM.
Furthermore, this is one of the first studies that we know that takes into account different gender characteristics in MSM, thus it contributes to open a new research field on how it is necessary to question attitudes, behaviors and expectancies related to unhealthy masculinities.20
Results from this study may provide keys for the design of prevention strategies. According to others, items such as the attitudes regarding sexuality and perception of risk practices from a gender perspective11 should be included in order to make programs more effective.
ConclusionsThe BSRI-12 may be a useful instrument for the identification of gender stereotypes in MSM. Compared with the androgynous, those who perceive themselves to be within the undifferentiated category are more vulnerable to risk practices engagement, as well as the influence of factors as knowledge of sexual partners’ serological status, substances consumption and also use sex toys without protection. The information obtained from this study may be useful to better define the strategies of prevention programs.
Editor in chargeMaría del Mar García-Calvente.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
In current studies on sexual risk practices in men who have sex with men, contextual and socioeconomic variables have been identified and recently, also others related to structural factors, highlighting gender and, in particular, traditional norms of masculinity.
What does this study add to the literature?Different gender stereotypes in men who have sex with men exist, which are specifically associated with risk practices, and they also determine conditions for such practices engagement, as substance use.
Preventive programs should incorporate the existence of different gender stereotypes and how they are involved in the establishment of affective-sexual relationships among men.
A. Gasch and C. Tomás designed the study. A. Gasch performed the data collection. A. Gasch, C. Tomás and E. Rubio participated in the data analysis and interpretation. A. Gasch wrote the first version of the article and the three authors reviewed the different versions and performed the critical review with intellectual contributions until they agreed to approve the final version for publication. The three authors are responsible and guarantee that all aspects of the manuscript have been reviewed and discussed in order to be exposed with the utmost precision and integrity.
FundingThis work was supported by project DGA-FSE B124.
Conflicts of interestNone.











