



Evaluar el acceso a jeringas estériles y su asociación con prácticas de inyección de riesgo en Madrid y Barcelona.
Material y métodoEstudio transversal en la comunidad de 465 jóvenes que se inyectan heroína, realizado entre 2001 y 2003, mediante entrevista asistida por ordenador.
ResultadosUn 4,2% no obtuvo jeringas estériles gratuitas en los últimos 12 meses. En Madrid, el 32,1% obtuvo todas las jeringas estériles gratis (TJEG), frente al 44,6% de Barcelona (p < 0,01). No compartir (no utilizar jeringas ajenas usadas o droga diluida en las usadas por otros) se asoció con obtener TJEG (odds ratio [OR] = 1,69) e inyectarse esporádicamente (OR = 1,83). No reutilizar las jeringas propias se asoció con las mismas variables (OR = 4,02 y OR = 2,50, respectivamente).
ConclusionesEn Madrid y Barcelona el acceso a jeringas estériles es muy elevado, aunque con modelos diferentes. Debe facilitarse la obtención de todas las jeringas estériles gratis, especialmente entre los jóvenes que se inyectan con mayor frecuencia.
To evaluate access to sterile syringes and its association with injection risk behaviour in Madrid and Barcelona.
Materials and methodsCross-sectional community study by computer-assisted personal interview in 465 young heroin injectors between 2001 and 2003.
ResultsSome 4.2% had not obtained any free sterile syringes in the previous 12 months. In Madrid 32.1% had obtained all their sterile syringes free of charge (ASSF), versus 44.6% in Barcelona (p < 0.01). Not sharing (not using syringes used by someone else and not front/backloading) was associated with obtaining ASSF (OR = 1.69) and with sporadic injection (OR = 1.83). Not reusing one’s own syringes was associated with the same two variables (OR = 4.02 and OR = 2.50, respectively).
ConclusionsAccess to sterile syringes is very high in Madrid and Barcelona, although the 2 cities have different approaches. The acquisition of all syringes free of charge should be facilitated, especially among frequent injectors.
Over the last 15 years, a growing number of initiatives have facilitated the provision of sterile syringes to drug injectors in Spain, primarily syringe exchange programmes (SEPs) and subsidised sales in pharmacies. The SEPs have branched out to new locations1, and some injectors obtain their supplies through these programmes and subsequently sell them2 (satellite distributors – SDs)3. However, the development of the SEPs has not been geographically homogeneous: in 2003 there were 254 SEPs with 1,560 exchange points (EPs) (each location or site where syringe exchange takes place), 799 of which (51.2%) were in Catalonia and 66 (4.2%) in the Community of Madrid1. Moreover, 664 pharmacies in Catalonia had an SEP, versus only 12 pharmacies in the Community of Madrid1. Free syringes could be obtained only in the SEPs and there were no subsidised sales.
In other countries, SDs have been shown to improve access to sterile syringes in certain places or at certain times4,5 although these informal resources are associated with a greater risk of HIV infection than the use of more structured programmes4. The extent of SEP coverage is critical to assuring their effectiveness6.
The aim of this work is to describe the differences in access to sterile syringes among injectors in Madrid and Barcelona and to study sterile syringe access as a predictor of safer injection practices that may prevent the transmission of bloodborne infections.
Materials and methodsThe methodology used in the ITINERE cohort has previously been described in detail7. Independently of the social services, 991 young adults (18-30 years old) were recruited in the cities of Madrid, Barcelona and Seville between April 2001 and December 2003. All participants had used heroin on at least 12 days in the previous 12 months and on at least 1 day in the previous 3 months. The present analysis was restricted to the 465 participants from Madrid and Barcelona who had injected the drug in the previous 12 months and who answered three pre-coded questions: 1) Of all the sterile syringes you have used in the last 12 months, how many did you obtain free of charge? 2) From what kind of organization or service did you obtain the most free syringes in the last 12 months? 3) Where did you buy most of the syringes you purchased during this same time period? The 2.5% of injection drug users who did not respond were excluded. Their profile did not differ significantly from the rest of the population in terms of the main variables. The questionnaire7 was computer-assisted. Dried blood spot samples were also analysed (HIV, HCV).
The statistical significance of the differences was evaluated with the Chi square test for qualitative variables and by analysis of variance with subsequent comparisons with Scheffé's test for quantitative variables. Two dependent variables were explored separately in the logistic regression: «sharing» - injecting with used syringes or front/backloading (i.e., employing a used syringe to prepare the drug solution, which is then divided into one or more syringes for injection) and «reusing one's own syringes» - because these practices involve very different risks of transmitting infections and to avoid problems of co-linearity.
ResultsMost respondents were men (73.4%), born in Spain (84.9%), and without regular employment (69.2%); their mean age was 25.8 years (95% CI 25.5-26.1) and mean duration of injecting drug use was 6.5 years (95% CI 6.0-6.91). Some 86.5% had injected in the last 30 days. Injection in prívate places, such as flats or houses, was more frequent in Barcelona (19.3%) than in Madrid (11.4%), where it more often took place in open places (sites of drug sales or consumption, public squares, abandoned houses or similar places) (p < 0.05).
Only 4.2% (20) had not obtained any free sterile syringes in the last 12 months, 1.9% in Barcelona and 7.4% in Madrid (p < 0.01). These injectors differed from the rest of the sample in that they were more frequently women (45.0% vs. 25.8%; p=0.058) and sporadic users (61.1% vs. 22.8%; p < 0.001), and they less often injected in places where drugs are sold or consumed (10.0% vs. 63.8%; p < 0.001).
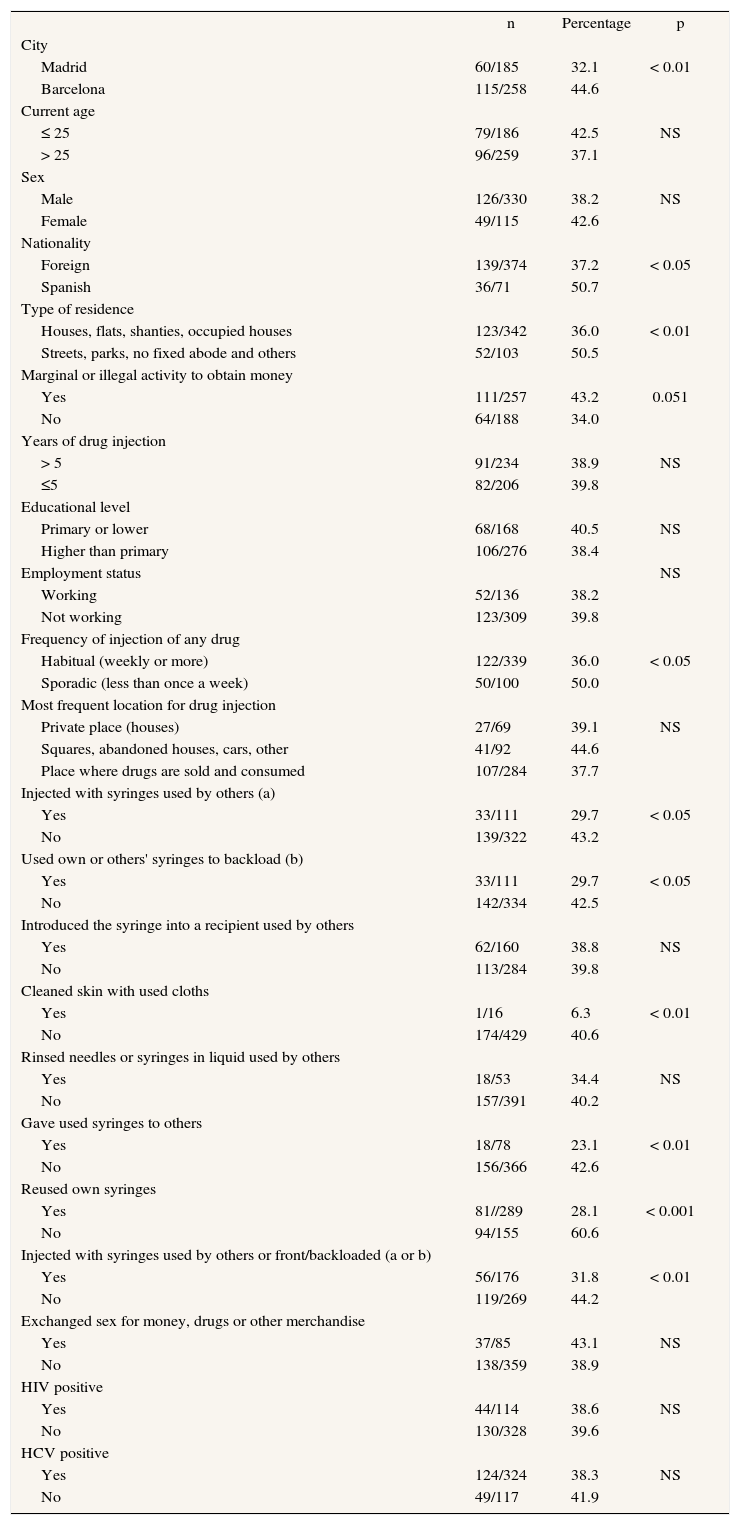
The way syringes were acquired - either all sterile syringes free of charge (ASSF) through SEPs or free plus purchased sterile syringes - was significantly associated with the city of residence. The proportion of drug users who obtained ASSF was smaller in Madrid than in Barcelona (table 1). In Barcelona, 62.8% obtained most of their free syringes from SEPs located in buses or vans, 20.5% from SEPs in pharmacies, 7.8% from SEPs at fixed locations, 5.7% through streetbased social workers or educators and 3.1% in other ways. In Madrid, the respective percentages were 82.5%, 0.5%, 8.7%, 2.7% and 5.5% (p < 0.001). Of those who had purchased syringes in the 12 months before the interview (286), 51.7% had bought them primarily in pharmacies and 48% in the street (67% and 32.4%, respectively, in Barcelona, vs. 34.8% and 65.2% in Madrid, p < 0.001). Obtaining ASSF was also significantly and positively associated with being Spanish, not having a fixed abode, injecting drugs sporadically and not exhibiting most of the injection risk behaviour investigated.
Proportion of young drug injectors who obtain all their sterile syringes free of charge, according to variables related with sociodemographics, injection, sexual behaviour and serological status (HIV, HCV). Itínere Project, 2001-03
| n | Percentage | p | |
| City | |||
| Madrid | 60/185 | 32.1 | < 0.01 |
| Barcelona | 115/258 | 44.6 | |
| Current age | |||
| ≤ 25 | 79/186 | 42.5 | NS |
| > 25 | 96/259 | 37.1 | |
| Sex | |||
| Male | 126/330 | 38.2 | NS |
| Female | 49/115 | 42.6 | |
| Nationality | |||
| Foreign | 139/374 | 37.2 | < 0.05 |
| Spanish | 36/71 | 50.7 | |
| Type of residence | |||
| Houses, flats, shanties, occupied houses | 123/342 | 36.0 | < 0.01 |
| Streets, parks, no fixed abode and others | 52/103 | 50.5 | |
| Marginal or illegal activity to obtain money | |||
| Yes | 111/257 | 43.2 | 0.051 |
| No | 64/188 | 34.0 | |
| Years of drug injection | |||
| > 5 | 91/234 | 38.9 | NS |
| ≤5 | 82/206 | 39.8 | |
| Educational level | |||
| Primary or lower | 68/168 | 40.5 | NS |
| Higher than primary | 106/276 | 38.4 | |
| Employment status | NS | ||
| Working | 52/136 | 38.2 | |
| Not working | 123/309 | 39.8 | |
| Frequency of injection of any drug | |||
| Habitual (weekly or more) | 122/339 | 36.0 | < 0.05 |
| Sporadic (less than once a week) | 50/100 | 50.0 | |
| Most frequent location for drug injection | |||
| Private place (houses) | 27/69 | 39.1 | NS |
| Squares, abandoned houses, cars, other | 41/92 | 44.6 | |
| Place where drugs are sold and consumed | 107/284 | 37.7 | |
| Injected with syringes used by others (a) | |||
| Yes | 33/111 | 29.7 | < 0.05 |
| No | 139/322 | 43.2 | |
| Used own or others' syringes to backload (b) | |||
| Yes | 33/111 | 29.7 | < 0.05 |
| No | 142/334 | 42.5 | |
| Introduced the syringe into a recipient used by others | |||
| Yes | 62/160 | 38.8 | NS |
| No | 113/284 | 39.8 | |
| Cleaned skin with used cloths | |||
| Yes | 1/16 | 6.3 | < 0.01 |
| No | 174/429 | 40.6 | |
| Rinsed needles or syringes in liquid used by others | |||
| Yes | 18/53 | 34.4 | NS |
| No | 157/391 | 40.2 | |
| Gave used syringes to others | |||
| Yes | 18/78 | 23.1 | < 0.01 |
| No | 156/366 | 42.6 | |
| Reused own syringes | |||
| Yes | 81//289 | 28.1 | < 0.001 |
| No | 94/155 | 60.6 | |
| Injected with syringes used by others or front/backloaded (a or b) | |||
| Yes | 56/176 | 31.8 | < 0.01 |
| No | 119/269 | 44.2 | |
| Exchanged sex for money, drugs or other merchandise | |||
| Yes | 37/85 | 43.1 | NS |
| No | 138/359 | 38.9 | |
| HIV positive | |||
| Yes | 44/114 | 38.6 | NS |
| No | 130/328 | 39.6 | |
| HCV positive | |||
| Yes | 124/324 | 38.3 | NS |
| No | 49/117 | 41.9 |
HIV: Human immunodeficiency virus; HCV: Hepatitis C virus; NS: no statistical significance (p > 0.05).
All practices refers to the last 12 months.
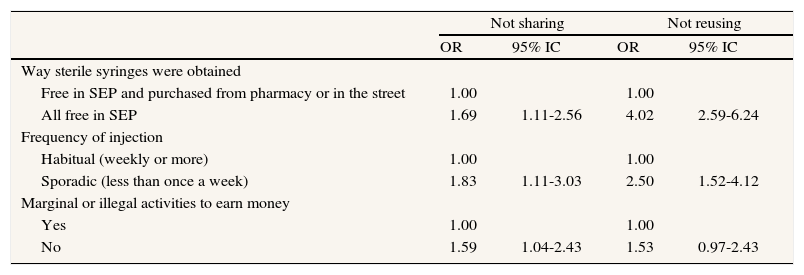
After adjusting for city, sociodemographic variables (sex, age, country of birth, educational level, employment status and type of residence), frequency of injection, years of injection, HIV and HCV status, prostitution and way of obtaining sterile syringes, «not sharing» (not injecting with used syringes and not front/backloading in syringes used by others) was associated with obtaining ASSF (OR = 1.69; 95% CI 1.11-2.56) and sporadic injection (OR = 1.83; 95% CI 1.11-3.03). Not reusing one's own syringes was associated with the same variables (OR = 4.02; 95% CI 2.59-6.24; and OR = 2.50; 1.52-4.12, respectively) (table 2). Among those who purchased syringes, a significant association was seen between not reusing and buying most syringes in the street (OR = 1.85 95% CI 1.02-3.34). Not sharing was not associated with the way syringes were purchased.
Factors associated with not sharing syringesa, or not reusing one's own syringes among young heroin injectors. Itínere Project, 2001-03. Multivariate logistic regression analysis
| Not sharing | Not reusing | |||
| OR | 95% IC | OR | 95% IC | |
| Way sterile syringes were obtained | ||||
| Free in SEP and purchased from pharmacy or in the street | 1.00 | 1.00 | ||
| All free in SEP | 1.69 | 1.11-2.56 | 4.02 | 2.59-6.24 |
| Frequency of injection | ||||
| Habitual (weekly or more) | 1.00 | 1.00 | ||
| Sporadic (less than once a week) | 1.83 | 1.11-3.03 | 2.50 | 1.52-4.12 |
| Marginal or illegal activities to earn money | ||||
| Yes | 1.00 | 1.00 | ||
| No | 1.59 | 1.04-2.43 | 1.53 | 0.97-2.43 |
Not sharing syringes = not injecting with syringes used by others and not front/backloading. Reference period: last 12 months. Both models were adjusted by city, sociodemographic variables, years of injection, HIV and HCV serological status and prostitution. N.° of cases retained in each model = 439. SEP = Syringe exchange programs. CI: confidence interval.
This is the first study of access to sterile syringes in a community sample of drug injectors in Spain. Free sterile syringes were found to be widely accessible in Madrid and Barcelona, which is consistent with the considerable increase in SEPs over the last 15 years1,2. However, there are important differences between the two cities: a smaller proportion obtained ASSF in SEPs in Madrid, where those who purchased syringes most often bought them in the street. Both findings are consistent with the much larger number of EPs in Barcelona8 (141) than in Madrid (27-31; personal communication, Marta Franco) in 2003, and with the small number of pharmacies authorised for syringe exchange in the latter city1. It is possible that the number of syringes provided by the SEPs per year to each injector was not less in Madrid, but that a substantial proportion of syringes reach users through SDs and thus are not free of charge. It may also be that the number of free sterile syringes put into circulation in Madrid was too low to meet the demand. Although it is not easy to estimate coverage when the number of users is unknown, NGOs and local governments should make an effort in this regard. Furthermore, a certain balance should be maintained between structured programmes and informal resources that do not focus on transmitting preventive messages, do not collect used syringes, and do not fully guarantee the sterility of injection material4,9. It may be necessary to seek mechanisms to involve such a widespread resource as SDs in a structured way, as health agents.
In Madrid injection is more frequent in public or open places, and syringes are more often obtained in mobile SEPs. This seems consistent with the existence of a single vehicle-based programme in Barcelona, which in practice is used as a fixed site, and of public places where drugs are sold and consumed in many parts of Madrid. The characteristics of the illegal drug market and the needs of the injector should guide the types of SEPs to be developed, without forgetting that the characteristics or location of the programme may in some measure affect the choice of injection site.
It is logical that a smaller proportion of frequent injectors obtain ASSF; however, this could seriously limit the effectiveness of SEPs10, since those who inject more often have more opportunities to share injection material and to reuse their own. In fact, the regression analysis showed that those who inject fewer times, as well as those who obtain ASSF, have less risk behaviour (not sharing or not reusing). Frequent injectors need to have greater access to ASSF, particularly considering the high prevalence of different ways of sharing injection material3,11 and the high incidence of HIV or HCV in injectors in both cities12. Moreover, among those who buy syringes, access to SDs has a protective effect with regard to reuse of one's own syringes. However, this resource seems to have a limited capacity to prevent sharing of injection material, which would support a greater effect of SEPs as compared to informal resources for HIV prevention4,9.
This study has limitations stemming from its crosssectional design in a difficult-to-access population lacking a clear sampling framework, thus it is difficult to know the extent to which the sample is representative. To reduce socially desired responses, the interviews were not conducted either in treatment centres for drug dependence or in SEPs.
AcknowledgementsThis research was financed primarily by the Fundación para Investigación y la Prevención del Sida en España (FIPSE 3035/99 - Foundation for AIDS Research and Prevention in Spain); the analysis was possible thanks to the support of the Ciber de Epidemiología y Salud Pública.
Our thanks to all the persons and institutions that helped with participant recruitment and follow-up and those that allowed us the use of their premises to conduct the interviews; to Marta Franco of the Agencia Antidroga of the Community of Madrid; and to all those who agreed to participate in ITÍNERE and formed part of the study sample.











