



To describe the influence of socioeconomic characteristics on the choice of the contraceptive method used among women in Spain in 2006.
MethodsThis is a cross-sectional study of women aged 15-49 who reported the contraceptive method used during the first sexual intercourse (n = 3352) and during the 4 weeks prior to the interview (n = 2672). Data were analyzed taking into account women's socioeconomic characteristics.
ResultsThe mostly used method during the first sexual intercourse was the condom. Women from developing countries more frequently used the pill than native-born Spanish women. The condom was also the most commonly used method in the 4 weeks prior to the interview. The use of other contraceptive methods increased with age. Being older and having children were both associated with an increased use of permanent methods.
ConclusionsThe choice of a specific contraceptive method seems to be more strongly influenced by women's stage of life than by socioeconomic characteristics.
Describir la influencia de las características socioeconómicas en la elección del método anticonceptivo utilizado por las mujeres en España en 2006.
MétodosEstudio transversal de las mujeres de 15-49 años de edad que declararon el método anticonceptivo utilizado en la primera relación sexual (n = 3352) y durante las cuatro últimas semanas (n = 2672), teniendo en cuenta sus características socioeconómicas.
ResultadosEl preservativo fue el método más utilizado durante la primera relación sexual. Las mujeres de países en vías de desarrollo usaron más frecuentemente la píldora que las autóctonas. El preservativo fue también el método más utilizado durante las cuatro últimas semanas. El uso del resto de los métodos aumenta con la edad. Tener una edad más alta e hijos se asoció con un mayor uso de métodos permanentes.
ConclusionesLa elección de un método anticonceptivo concreto parece estar más influenciada por el ciclo vital de la mujer que por sus características socioeconómicas.
Several studies have highlighted the factors that influence women's use of contraception. Women of lower socioeconomic positions use contraception less and use less effective contraceptive methods, having the highest risk of unintended pregnancy.1,2 It has been observed that different countries in Europe not only have differences in the prevalence of the use of contraception but also in the forms of contraception used.1–3A recent study showed that 70% of sexually active women in Spain aged 15-49 years used contraception during their first intercourse and 78% used it during the four weeks prior to the interview.4 This same study showed that women's characteristics such as age, level of education, country of origin, religiousness and age at first intercourse influence the use of contraception at first intercourse, and that in the case of the use of contraception during the last four weeks characteristics such as living with a partner, having children and having used contraception at first intercourse appear to be more relevant.
The condom, followed by the pill, were the methods used most, both in their first intercourse and during their most recent sexual intercourse, in Spain,4,5 but it is not known if women's socioeconomic characteristics have an influence on their decision to use a specific contraceptive method.
In this context, the aim of the present study was to describe the influence of women's socioeconomic characteristics on the choice of the contraceptive method used among women in Spain in 2006.
MethodsThis is a population-based cross-sectional study of non-institutionalised women aged 15-49 years in Spain in 2006.
The source of information was the 2006 fecundity interview developed by the Centro de Investigaciones Sociológicas. From an initial sample of 9737 interviewees, we selected women aged 15-49 years who reported the contraceptive method used during their first sexual intercourse (n = 3352) and during the four weeks prior to the interview (n = 2672). Full details of the survey have been reported elsewhere.4
Two dependent variables were analyzed, the contraceptive method used during first sexual intercourse and during sex in the four weeks prior to the interview. After having reported using contraception, women were asked if they used any of the following methods: condom, pill, withdrawal, injection, intrauterine device (IUD), emergency contraception, periodic abstinence, male sterilization, female sterilization, cream/foam spermicides or sponge, diaphragm, any other method. We selected women who had used a single method and compared these methods both individually and in groups of methods: condom/pill; condom/pill/IUD; ineffective (withdrawal, periodic abstinence and cream/foam spermicides or sponge)/effective (all the other methods of the previous list except the category ‘any other method’, as we do not know the effectiveness of the methods included in that category); permanent (male and female sterilization)/reversible (methods defined previously as effective).
Details of the selection of independent variables and explanation about categories have been reported previously.4 The variables used in the analysis of first sexual intercourse were: level of education, country of origin, religiousness and age at first intercourse; and during the four weeks prior to the interview: all the variables mentioned above, living with partner, number of children and use of contraception at first intercourse. All analyses were stratified by age.
We performed a descriptive analysis using the Chi-squared test. Bivariate, multivariate and multinomial logistic regression models were fitted, and crude and adjusted odds ratios (aOR) with 95% confidence intervals (95%CI) were calculated for each group of age. Final adjusted models include all independent variables.
All statistical analyses were performed using STATA, version 10.1. Missing values were excluded from the analysis.
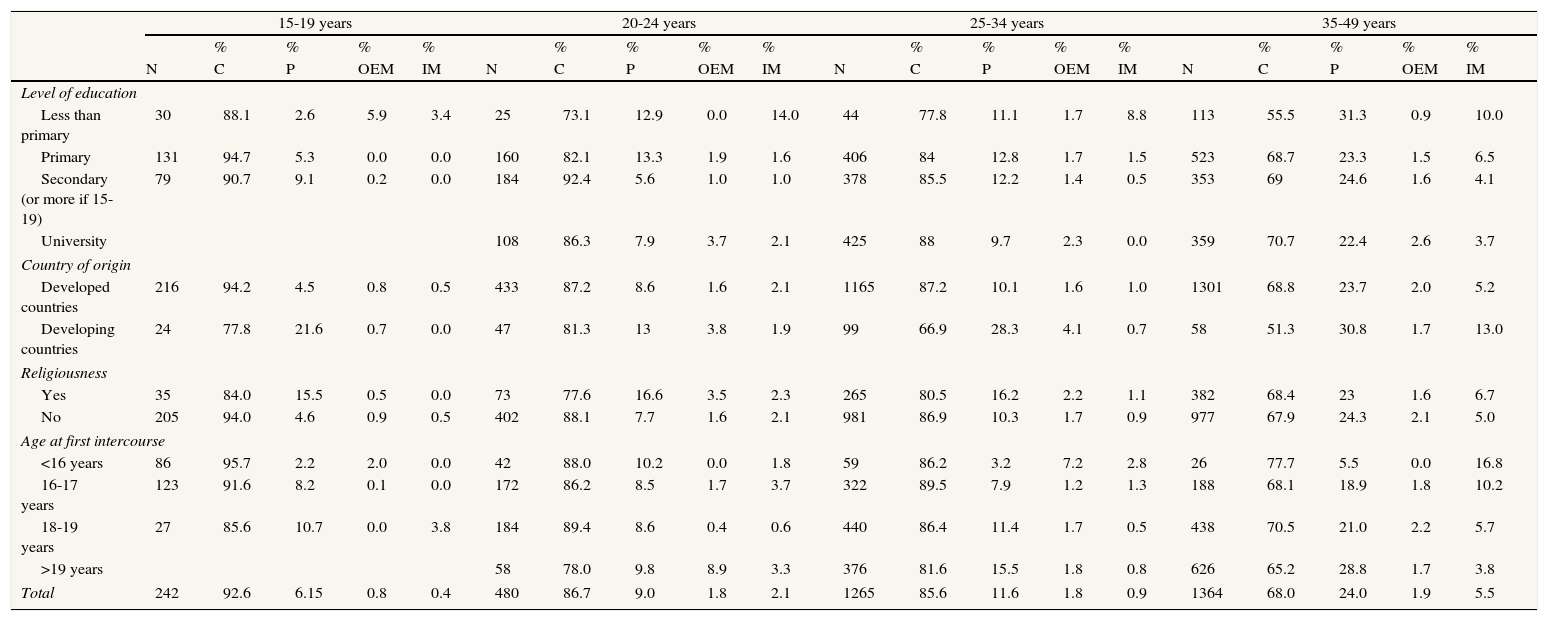
ResultsTable 1 shows the prevalence of the most common contraceptive methods used during the first sexual intercourse stratified by variables of interest. Male condom was the method most commonly used in all ages (92.6% in 15-19, 86.7% in 20-24, 85.6% in 25-34 and 68% in 35-49). Women who did not use condom mostly used the pill, and the rest of methods are practically not used. The only variable associated with the choice of a contraceptive method was country of origin (data not shown). Women from developing countries aged 15-19 (aOR = 0.11; 95%CI: 0.02-0.58) and 25-34 (aOR = 0.35; 95%CI: 0.19-0.66) used the pill more than the condom, compared to women of the same age from developed countries.
Prevalence of the contraceptive methods most commonly used during the first experience of sexual intercourse, stratified by selected variables, Spain, 2006.
| 15-19 years | 20-24 years | 25-34 years | 35-49 years | |||||||||||||||||
| % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | |||||
| N | C | P | OEM | IM | N | C | P | OEM | IM | N | C | P | OEM | IM | N | C | P | OEM | IM | |
| Level of education | ||||||||||||||||||||
| Less than primary | 30 | 88.1 | 2.6 | 5.9 | 3.4 | 25 | 73.1 | 12.9 | 0.0 | 14.0 | 44 | 77.8 | 11.1 | 1.7 | 8.8 | 113 | 55.5 | 31.3 | 0.9 | 10.0 |
| Primary | 131 | 94.7 | 5.3 | 0.0 | 0.0 | 160 | 82.1 | 13.3 | 1.9 | 1.6 | 406 | 84 | 12.8 | 1.7 | 1.5 | 523 | 68.7 | 23.3 | 1.5 | 6.5 |
| Secondary (or more if 15-19) | 79 | 90.7 | 9.1 | 0.2 | 0.0 | 184 | 92.4 | 5.6 | 1.0 | 1.0 | 378 | 85.5 | 12.2 | 1.4 | 0.5 | 353 | 69 | 24.6 | 1.6 | 4.1 |
| University | 108 | 86.3 | 7.9 | 3.7 | 2.1 | 425 | 88 | 9.7 | 2.3 | 0.0 | 359 | 70.7 | 22.4 | 2.6 | 3.7 | |||||
| Country of origin | ||||||||||||||||||||
| Developed countries | 216 | 94.2 | 4.5 | 0.8 | 0.5 | 433 | 87.2 | 8.6 | 1.6 | 2.1 | 1165 | 87.2 | 10.1 | 1.6 | 1.0 | 1301 | 68.8 | 23.7 | 2.0 | 5.2 |
| Developing countries | 24 | 77.8 | 21.6 | 0.7 | 0.0 | 47 | 81.3 | 13 | 3.8 | 1.9 | 99 | 66.9 | 28.3 | 4.1 | 0.7 | 58 | 51.3 | 30.8 | 1.7 | 13.0 |
| Religiousness | ||||||||||||||||||||
| Yes | 35 | 84.0 | 15.5 | 0.5 | 0.0 | 73 | 77.6 | 16.6 | 3.5 | 2.3 | 265 | 80.5 | 16.2 | 2.2 | 1.1 | 382 | 68.4 | 23 | 1.6 | 6.7 |
| No | 205 | 94.0 | 4.6 | 0.9 | 0.5 | 402 | 88.1 | 7.7 | 1.6 | 2.1 | 981 | 86.9 | 10.3 | 1.7 | 0.9 | 977 | 67.9 | 24.3 | 2.1 | 5.0 |
| Age at first intercourse | ||||||||||||||||||||
| <16 years | 86 | 95.7 | 2.2 | 2.0 | 0.0 | 42 | 88.0 | 10.2 | 0.0 | 1.8 | 59 | 86.2 | 3.2 | 7.2 | 2.8 | 26 | 77.7 | 5.5 | 0.0 | 16.8 |
| 16-17 years | 123 | 91.6 | 8.2 | 0.1 | 0.0 | 172 | 86.2 | 8.5 | 1.7 | 3.7 | 322 | 89.5 | 7.9 | 1.2 | 1.3 | 188 | 68.1 | 18.9 | 1.8 | 10.2 |
| 18-19 years | 27 | 85.6 | 10.7 | 0.0 | 3.8 | 184 | 89.4 | 8.6 | 0.4 | 0.6 | 440 | 86.4 | 11.4 | 1.7 | 0.5 | 438 | 70.5 | 21.0 | 2.2 | 5.7 |
| >19 years | 58 | 78.0 | 9.8 | 8.9 | 3.3 | 376 | 81.6 | 15.5 | 1.8 | 0.8 | 626 | 65.2 | 28.8 | 1.7 | 3.8 | |||||
| Total | 242 | 92.6 | 6.15 | 0.8 | 0.4 | 480 | 86.7 | 9.0 | 1.8 | 2.1 | 1265 | 85.6 | 11.6 | 1.8 | 0.9 | 1364 | 68.0 | 24.0 | 1.9 | 5.5 |
C: condom; P: pill; OEM: other effective methods; IM: ineffective methods.
Totals may differ from the sum of categories because of missing values and sample weights. The percentages may not sum to 100 because the category ‘any other method’ of contraception is not included.
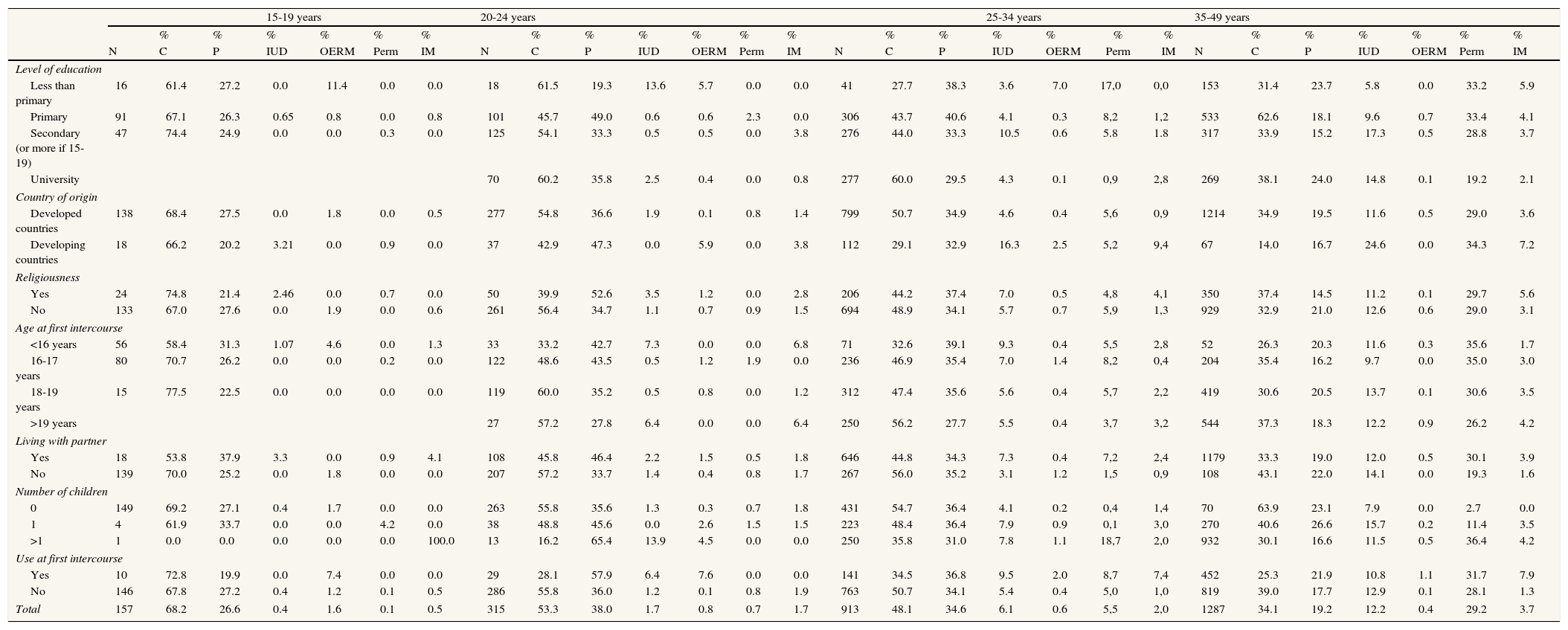
Table 2 shows the prevalence of the contraceptive methods used most commonly during the four weeks prior to the interview stratified by variables of interest. The contraceptive method used varies depending on age. Condom is the most common method in all ages (68.2% in women aged 15-19, 53.3% in 20-24, 48.1% in 25-34 and 34.1% in 35-49). In women aged 15-24 the majority of those who did not use the condom used the pill, and no socioeconomic variable was associated with the choice between them (data not shown). Among women aged 25-49, the pill is also the second most commonly used method, and the use of IUD and specially permanent methods increases. Women aged 25 to 49 showed no differences in the choice of a reversible method, using mainly condom, pill or IUD, but there were differences in the use of a reversible method compared to a permanent one. Older women (aOR = 2.28; 95%CI: 1.39-3.75 for women aged 35-49 compared to those aged 25-34) and those with children (aOR = 3.95; 95%CI: 1.12-13.9 for women with one children compared to women without children) are the ones who used permanent methods more after adjusting for all independent variables (data not shown).
Prevalence of the contraceptive methods most commonly used during the four weeks prior to the survey interview, stratified by selected variables, Spain, 2006.
| 15-19 years | 20-24 years | 25-34 years | 35-49 years | |||||||||||||||||||||||||
| % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | |||||
| N | C | P | IUD | OERM | Perm | IM | N | C | P | IUD | OERM | Perm | IM | N | C | P | IUD | OERM | Perm | IM | N | C | P | IUD | OERM | Perm | IM | |
| Level of education | ||||||||||||||||||||||||||||
| Less than primary | 16 | 61.4 | 27.2 | 0.0 | 11.4 | 0.0 | 0.0 | 18 | 61.5 | 19.3 | 13.6 | 5.7 | 0.0 | 0.0 | 41 | 27.7 | 38.3 | 3.6 | 7.0 | 17,0 | 0,0 | 153 | 31.4 | 23.7 | 5.8 | 0.0 | 33.2 | 5.9 |
| Primary | 91 | 67.1 | 26.3 | 0.65 | 0.8 | 0.0 | 0.8 | 101 | 45.7 | 49.0 | 0.6 | 0.6 | 2.3 | 0.0 | 306 | 43.7 | 40.6 | 4.1 | 0.3 | 8,2 | 1,2 | 533 | 62.6 | 18.1 | 9.6 | 0.7 | 33.4 | 4.1 |
| Secondary (or more if 15-19) | 47 | 74.4 | 24.9 | 0.0 | 0.0 | 0.3 | 0.0 | 125 | 54.1 | 33.3 | 0.5 | 0.5 | 0.0 | 3.8 | 276 | 44.0 | 33.3 | 10.5 | 0.6 | 5.8 | 1.8 | 317 | 33.9 | 15.2 | 17.3 | 0.5 | 28.8 | 3.7 |
| University | 70 | 60.2 | 35.8 | 2.5 | 0.4 | 0.0 | 0.8 | 277 | 60.0 | 29.5 | 4.3 | 0.1 | 0,9 | 2,8 | 269 | 38.1 | 24.0 | 14.8 | 0.1 | 19.2 | 2.1 | |||||||
| Country of origin | ||||||||||||||||||||||||||||
| Developed countries | 138 | 68.4 | 27.5 | 0.0 | 1.8 | 0.0 | 0.5 | 277 | 54.8 | 36.6 | 1.9 | 0.1 | 0.8 | 1.4 | 799 | 50.7 | 34.9 | 4.6 | 0.4 | 5,6 | 0,9 | 1214 | 34.9 | 19.5 | 11.6 | 0.5 | 29.0 | 3.6 |
| Developing countries | 18 | 66.2 | 20.2 | 3.21 | 0.0 | 0.9 | 0.0 | 37 | 42.9 | 47.3 | 0.0 | 5.9 | 0.0 | 3.8 | 112 | 29.1 | 32.9 | 16.3 | 2.5 | 5,2 | 9,4 | 67 | 14.0 | 16.7 | 24.6 | 0.0 | 34.3 | 7.2 |
| Religiousness | ||||||||||||||||||||||||||||
| Yes | 24 | 74.8 | 21.4 | 2.46 | 0.0 | 0.7 | 0.0 | 50 | 39.9 | 52.6 | 3.5 | 1.2 | 0.0 | 2.8 | 206 | 44.2 | 37.4 | 7.0 | 0.5 | 4,8 | 4,1 | 350 | 37.4 | 14.5 | 11.2 | 0.1 | 29.7 | 5.6 |
| No | 133 | 67.0 | 27.6 | 0.0 | 1.9 | 0.0 | 0.6 | 261 | 56.4 | 34.7 | 1.1 | 0.7 | 0.9 | 1.5 | 694 | 48.9 | 34.1 | 5.7 | 0.7 | 5,9 | 1,3 | 929 | 32.9 | 21.0 | 12.6 | 0.6 | 29.0 | 3.1 |
| Age at first intercourse | ||||||||||||||||||||||||||||
| <16 years | 56 | 58.4 | 31.3 | 1.07 | 4.6 | 0.0 | 1.3 | 33 | 33.2 | 42.7 | 7.3 | 0.0 | 0.0 | 6.8 | 71 | 32.6 | 39.1 | 9.3 | 0.4 | 5,5 | 2,8 | 52 | 26.3 | 20.3 | 11.6 | 0.3 | 35.6 | 1.7 |
| 16-17 years | 80 | 70.7 | 26.2 | 0.0 | 0.0 | 0.2 | 0.0 | 122 | 48.6 | 43.5 | 0.5 | 1.2 | 1.9 | 0.0 | 236 | 46.9 | 35.4 | 7.0 | 1.4 | 8,2 | 0,4 | 204 | 35.4 | 16.2 | 9.7 | 0.0 | 35.0 | 3.0 |
| 18-19 years | 15 | 77.5 | 22.5 | 0.0 | 0.0 | 0.0 | 0.0 | 119 | 60.0 | 35.2 | 0.5 | 0.8 | 0.0 | 1.2 | 312 | 47.4 | 35.6 | 5.6 | 0.4 | 5,7 | 2,2 | 419 | 30.6 | 20.5 | 13.7 | 0.1 | 30.6 | 3.5 |
| >19 years | 27 | 57.2 | 27.8 | 6.4 | 0.0 | 0.0 | 6.4 | 250 | 56.2 | 27.7 | 5.5 | 0.4 | 3,7 | 3,2 | 544 | 37.3 | 18.3 | 12.2 | 0.9 | 26.2 | 4.2 | |||||||
| Living with partner | ||||||||||||||||||||||||||||
| Yes | 18 | 53.8 | 37.9 | 3.3 | 0.0 | 0.9 | 4.1 | 108 | 45.8 | 46.4 | 2.2 | 1.5 | 0.5 | 1.8 | 646 | 44.8 | 34.3 | 7.3 | 0.4 | 7,2 | 2,4 | 1179 | 33.3 | 19.0 | 12.0 | 0.5 | 30.1 | 3.9 |
| No | 139 | 70.0 | 25.2 | 0.0 | 1.8 | 0.0 | 0.0 | 207 | 57.2 | 33.7 | 1.4 | 0.4 | 0.8 | 1.7 | 267 | 56.0 | 35.2 | 3.1 | 1.2 | 1,5 | 0,9 | 108 | 43.1 | 22.0 | 14.1 | 0.0 | 19.3 | 1.6 |
| Number of children | ||||||||||||||||||||||||||||
| 0 | 149 | 69.2 | 27.1 | 0.4 | 1.7 | 0.0 | 0.0 | 263 | 55.8 | 35.6 | 1.3 | 0.3 | 0.7 | 1.8 | 431 | 54.7 | 36.4 | 4.1 | 0.2 | 0,4 | 1,4 | 70 | 63.9 | 23.1 | 7.9 | 0.0 | 2.7 | 0.0 |
| 1 | 4 | 61.9 | 33.7 | 0.0 | 0.0 | 4.2 | 0.0 | 38 | 48.8 | 45.6 | 0.0 | 2.6 | 1.5 | 1.5 | 223 | 48.4 | 36.4 | 7.9 | 0.9 | 0,1 | 3,0 | 270 | 40.6 | 26.6 | 15.7 | 0.2 | 11.4 | 3.5 |
| >1 | 1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 100.0 | 13 | 16.2 | 65.4 | 13.9 | 4.5 | 0.0 | 0.0 | 250 | 35.8 | 31.0 | 7.8 | 1.1 | 18,7 | 2,0 | 932 | 30.1 | 16.6 | 11.5 | 0.5 | 36.4 | 4.2 |
| Use at first intercourse | ||||||||||||||||||||||||||||
| Yes | 10 | 72.8 | 19.9 | 0.0 | 7.4 | 0.0 | 0.0 | 29 | 28.1 | 57.9 | 6.4 | 7.6 | 0.0 | 0.0 | 141 | 34.5 | 36.8 | 9.5 | 2.0 | 8,7 | 7,4 | 452 | 25.3 | 21.9 | 10.8 | 1.1 | 31.7 | 7.9 |
| No | 146 | 67.8 | 27.2 | 0.4 | 1.2 | 0.1 | 0.5 | 286 | 55.8 | 36.0 | 1.2 | 0.1 | 0.8 | 1.9 | 763 | 50.7 | 34.1 | 5.4 | 0.4 | 5,0 | 1,0 | 819 | 39.0 | 17.7 | 12.9 | 0.1 | 28.1 | 1.3 |
| Total | 157 | 68.2 | 26.6 | 0.4 | 1.6 | 0.1 | 0.5 | 315 | 53.3 | 38.0 | 1.7 | 0.8 | 0.7 | 1.7 | 913 | 48.1 | 34.6 | 6.1 | 0.6 | 5,5 | 2,0 | 1287 | 34.1 | 19.2 | 12.2 | 0.4 | 29.2 | 3.7 |
C: condom; P: pill; IUD: intrauterine device; OERM: other effective reversible methods; Perm: permanent methods; IM: ineffective methods.
Totals may differ from the sum of categories because of missing values and sample weights. The percentages may not sum to 100 because the category ‘any other method’ of contraception is not included.
It has to be remarked that no variable was found associated with the choice of ineffective methods in the adjusted regression models in either of the two moments.
DiscussionDuring first sexual intercourse women mostly used condom at all ages, as has been previously reported in Spain and other European countries.3,4 Only being from a developing country influences prioritising the pill over the condom, as has been shown previously among women from Latin America.6
Condom is also the method most used in the four weeks prior to the interview, although an increase with age was found in the use of other contraceptive options.4,5 Condom use is higher in Spain than other European countries,1–3 possibly as a result of “safe sex” campaigns implemented to prevent sexually transmitted infections, specially among younger women.1,5 Only being older and having children are associated with choosing a method in recent intercourse, preferring a permanent method to a reversible one.
Recent hormonal methods and long-acting reversible methods could be a good alternative for some specific groups, but they are not commonly used in Spain, or in other European countries, mainly because of a lack of their being offered by professionals.7–9The main limitations of the study are related to design of the survey. Full details have been reported elsewhere.4
Contraceptive counselling is one of the most important factors affecting the choice of a contraceptive method.10–14 There is no information about counselling in the survey, and the different Autonomous Communities could be dealing with counselling in very different ways. It would be necessary to explore regional differences in the choice of the contraceptive method, as differences in the use of contraception have been found at this level.15
To conclude, this study indicates that although socioeconomic characteristics of women are associated with the use of contraception in Spain,4 the choice of a specific contraceptive method seems to be more influenced by the woman's stage of life.5,13
There are inequalities in the use of contraception at first intercourse and during the four weeks prior to the interview in Spain. We do not know if these inequalities are also influencing the choice of a particular contraceptive method.
What this paper adds?The choice of a specific contraceptive method seems to be more influenced by the woman's stage of life than by her socioeconomic characteristics. It would be necessary to explore regional differences in the choice of contraceptive method.
D. Ruiz-Muñoz performed the data analysis, participated in the interpretation of the data and drafted the manuscript. G. Pérez reviewed the analysis, participated in the interpretation of the data and in the drafting of the manuscript. The two authors have read and approved the final version of the manuscript.
FundingProject partially funded by the Plan Nacional I+R+D+I and for the ISCIII 2008-2011 and General Directorate of Evaluation and Research Promotion (reference PI09/90424 PI07/90050).
Conflict of interestNone.
This article forms part of the doctoral dissertation of D. Ruiz Muñoz at the Pompeu Fabra University (UPF) of Barcelona (Spain).











