




To validate the Brazilian version of the Short Assessment of Health Literacy in Portuguese-speaking Adults (SAHLPA), a 50-item test proposed as a particularly helpful instrument to assess health literacy in people with limited skills, in the Portuguese population.
MethodsWe used the standard procedure for cultural adaptation and administered the instrument to 249 participants. We examined construct validity using groups with expectedly increasing levels of health literacy (laypersons from the general population, engineering researchers, health researchers, and physicians), and through association with age and educational attainment, dichotomizing scores at the median of the layperson's group.
ResultsExploratory factor analysis revealed the instrument was one-dimensional and justified reduction to 33 items. SAHLPA-33 displayed adequate reliability (Cronbach's α = 0.73). The frequency of limited health literacy was highest among laypersons and lowest among physicians (p <0.001; p for trend <0.001). The proportion of participants with limited health literacy decreased with increasing education attainment (age- and sex-adjusted p for trend <0.001). Limited health literacy also tended to decrease with age, although the association was non-significant (sex- and education-adjusted p for trend = 0.067).
ConclusionWe culturally adapted a brief and simple instrument for health literacy assessment, and showed it was valid and fairly reliable. In Portuguese low-literate adults, SAHLPA-33 fills the gap in health literacy assessment instruments, and may be used to guide communication strategies with vulnerable patients and communities.
Validar la versión brasileña del Short Assessment of Health Literacy inPortuguese-speakingAdults (SAHLPA), una prueba de 50 ítems que ha sido propuesta como una herramienta particularmente útil para evaluar la alfabetización en salud en personas con bajas competencias, en la población portuguesa.
MétodosSe usó el procedimiento habitual para la adaptación cultural. El instrumento fue administrado a 249 participantes. Se evaluó la validez de constructo utilizando grupos con niveles esperados crecientes de alfabetización en salud (personas no cualificadas de la población general, investigadores en el área de la ingeniería, investigadores en salud y médicos) y a través de la asociación con la edad y la escolaridad, dicotomizando las puntuaciones por la mediana de las del grupo de la población general.
ResultadosEl análisis factorial exploratorio reveló que el instrumento era unidimensional y así ha sido reducido a 33 ítems. El SAHLPA-33 reveló una consistencia interna aceptable (α de Cronbach = 0,73). La frecuencia de alfabetización en salud limitada fue más elevada en la población general y menor en los médicos (p <0,001; p para la tendencia <0,001). La proporción de participantes con alfabetización en salud limitada disminuyó con el aumento de la escolaridad (p para la tendencia ajustada por edad y sexo <0,001). La alfabetización en salud también tendió a disminuir con la edad, aunque la asociación no era significativa (p para la tendencia ajustada por sexo y escolaridad = 0,067).
ConclusiónSe adaptó un instrumento simple y rápido para evaluar la alfabetización en salud individual y se mostró que era válido y razonablemente fiable. En los adultos portugueses con bajo nivel de alfabetización, SAHLPA-33 llena el vacío en instrumentos de evaluación de alfabetización en salud. Puede utilizarse para guiar estrategias de comunicación con personas y comunidades vulnerables.
Individual health literacy has been defined as “the degree to which people are able to access, understand, appraise and communicate information to engage with the demands of different health contexts to promote and maintain health across the life-course”.1 Limited health literacy has been linked to various adverse outcomes, including higher mortality, and is more common among the elderly, immigrants, and those with lower levels of education.2–5
In the past three decades, numerous instruments have been developed to screen for limited individual health literacy in research or clinical settings.6 The most widely used include the 66-item Rapid Estimate of Adult Literacy in Medicine7 (REALM), and the full and short versions of the Test of Functional Health Literacy in Adults (TOFHLA8 and STOFHLA9).3 Most of them were originally developed in English and are being adapted to other languages and populations.6 The REALM10 is a 125-item instrument developed as a fast screening tool to identify patients with limited abilities to read common medical and lay terms for body parts and illnesses. It presents words in ascending order of difficulty and is based on the idea that patients having trouble reading and pronouncing words probably will have issues with reading comprehension. The most commonly used is the reduced 66-item version7 that is frequently used to estimate patient reading levels (converting raw scores into grade equivalents) and tailor communication with patients accordingly.
In languages with very high letter to sound (phoneme-grapheme) correspondence, such as Spanish and Portuguese, the adaptation of health literacy assessment instruments based on word recognition and pronunciation, such as the REALM, is hindered by their inability to discriminate between health literacy and ability to read.11,12 The Short Assessment of Health Literacy for Spanish-speaking Adults (SAHLSA)13 was designed to overcome this issue by incorporating word comprehension. It has been adapted to Portuguese and validated in the Brazilian population as the Short Assessment of Health Literacy for Portuguese-speaking Adults (SAHLPA).14 These instruments have been proposed as less intimidating alternatives to assess health literacy in a clinical setting, and particularly helpful in assessing health literacy in the population groups most vulnerable to limited health literacy.13
In Portugal, limited health literacy has been estimated to affect between 4915 and 73%16 of the population. There is a lack of health literacy instruments designed specifically for low-literate populations that can be used to tailor health education interventions, as well as to study the impact of this social determinant of health.17 Because of its characteristics, brevity and ease of administration, we aimed to culturally adapt and validate SAHLPA in the Portuguese population.
MethodsOriginal instrumentThe SAHLPA is the Brazilian adapted version of the SAHLSA. SAHLSA is a new instrument based on the 66-item REALM10 supplemented by a simple comprehension test. An expert panel using the Delphi method developed two simple terms to match each REALM medical term: a key (a word with similar meaning) and a distractor (a word unrelated to the medical term). The resulting instrument consists of 50 medical terms the participants are requested to read aloud and associate with one of two word options. Participants are shown 50 laminated flash cards, each with a medical term in boldface on top and a key and distractor at the bottom. Because the key and distractor are used to test comprehension, participants are asked not to guess and to answer “Don’t know” if they don’t know the correct association. To answer correctly, the participants must both correctly pronounce the medical term and match it to the key. The score is calculated as the sum of all correct answers and varies between 0 and 50. It was validated in a convenience sample of 201 Spanish-speaking adults living in the United States. It takes 3-6minutes to complete.
SAHLPA was validated in a convenience sample of 226 Brazilian adults over the age of 60. Construct validity was assessed through correlation with formal education, self-reported functional literacy and global cognitive testing. The cut-off point for inadequate health literacy was defined by the inability to fully understand a medical prescription by a sub-sample of the participants and was ≤42 for the 50-item version and ≤14 for the short version (SAHLPA-18). Both the full (50-items) and reduced versions (18-items) showed good psychometric properties (Cronbach's α = 0.93 and 0.90, respectively) and high correlation (>0.60) with the variables used for construct validity testing. The full version takes 3-6minutes to administer and the short one 1-2minutes.
Cultural adaptation of SAHLPA to European PortugueseWe used the standard procedure for instrument adaptation to other populations.18 An expert committee (with backgrounds in family medicine, internal medicine, pharmacy, psychology, and sociology) culturally adapted the Brazilian Portuguese SAHLPA into European Portuguese, ensuring semantic and item equivalence. To preserve semantic equivalence, some words were altered: “recreação” was replaced by “lazer”, “similar” by “semelhante”, “matrimônio” by “casamento”, “coceira” by “coçar”, “tranquilo” by “calmo”. Other words were changed to match the correct spelling used in Portugal and accommodate spelling differences between Brazil and the other Portuguese speaking countries: “estresse” was replaced by “stress”, “Papanicolaou” by “Papanicolau”, “dolorido” by “dorido” and “contraceptivo” by “contracetivo” (Table 1). Items were otherwise considered culturally and socially equivalent. In addition, two native Portuguese speakers proficiently fluent in Spanish translated SAHLSA independently and merged the translations into a single European Portuguese version. Next, two native Spanish speakers, proficient in Portuguese, independently back-translated this version. They arrived at a consensus back-translated version, which was then revised and compared to the original by the committee, resolving any discrepancies between the two versions. This translated second European Portuguese version was then compared with the Brazilian one and with the first translation to European Portuguese. No additional changes were made. Because of word pronunciation differences between regions in Portugal, all but overtly inappropriate accents (e.g. ignoring written accents) were accepted as correct.
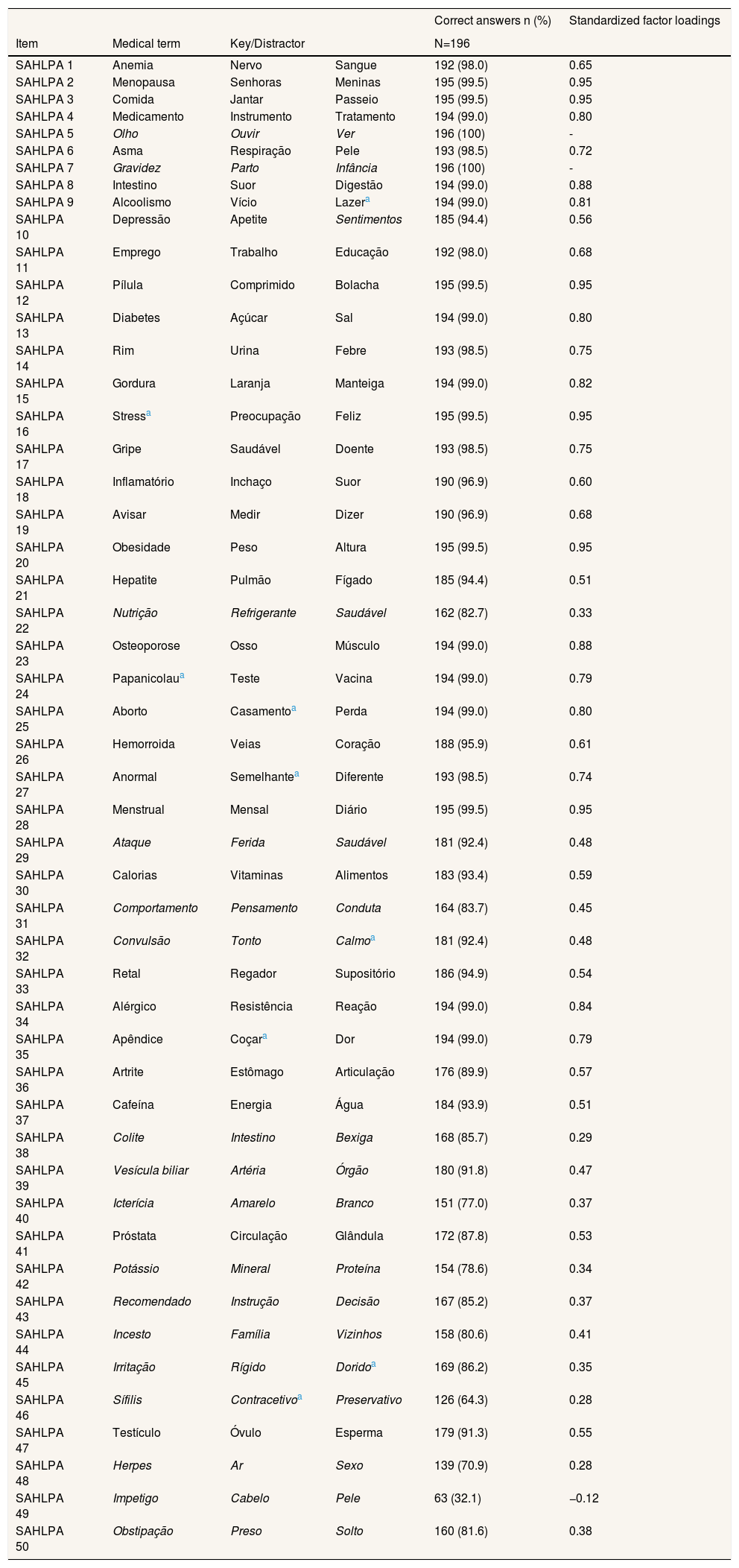
Correct answers per item and standardized factor loadings in exploratory factor analysis.
| Correct answers n (%) | Standardized factor loadings | ||||
|---|---|---|---|---|---|
| Item | Medical term | Key/Distractor | N=196 | ||
| SAHLPA 1 | Anemia | Nervo | Sangue | 192 (98.0) | 0.65 |
| SAHLPA 2 | Menopausa | Senhoras | Meninas | 195 (99.5) | 0.95 |
| SAHLPA 3 | Comida | Jantar | Passeio | 195 (99.5) | 0.95 |
| SAHLPA 4 | Medicamento | Instrumento | Tratamento | 194 (99.0) | 0.80 |
| SAHLPA 5 | Olho | Ouvir | Ver | 196 (100) | - |
| SAHLPA 6 | Asma | Respiração | Pele | 193 (98.5) | 0.72 |
| SAHLPA 7 | Gravidez | Parto | Infância | 196 (100) | - |
| SAHLPA 8 | Intestino | Suor | Digestão | 194 (99.0) | 0.88 |
| SAHLPA 9 | Alcoolismo | Vício | Lazera | 194 (99.0) | 0.81 |
| SAHLPA 10 | Depressão | Apetite | Sentimentos | 185 (94.4) | 0.56 |
| SAHLPA 11 | Emprego | Trabalho | Educação | 192 (98.0) | 0.68 |
| SAHLPA 12 | Pílula | Comprimido | Bolacha | 195 (99.5) | 0.95 |
| SAHLPA 13 | Diabetes | Açúcar | Sal | 194 (99.0) | 0.80 |
| SAHLPA 14 | Rim | Urina | Febre | 193 (98.5) | 0.75 |
| SAHLPA 15 | Gordura | Laranja | Manteiga | 194 (99.0) | 0.82 |
| SAHLPA 16 | Stressa | Preocupação | Feliz | 195 (99.5) | 0.95 |
| SAHLPA 17 | Gripe | Saudável | Doente | 193 (98.5) | 0.75 |
| SAHLPA 18 | Inflamatório | Inchaço | Suor | 190 (96.9) | 0.60 |
| SAHLPA 19 | Avisar | Medir | Dizer | 190 (96.9) | 0.68 |
| SAHLPA 20 | Obesidade | Peso | Altura | 195 (99.5) | 0.95 |
| SAHLPA 21 | Hepatite | Pulmão | Fígado | 185 (94.4) | 0.51 |
| SAHLPA 22 | Nutrição | Refrigerante | Saudável | 162 (82.7) | 0.33 |
| SAHLPA 23 | Osteoporose | Osso | Músculo | 194 (99.0) | 0.88 |
| SAHLPA 24 | Papanicolaua | Teste | Vacina | 194 (99.0) | 0.79 |
| SAHLPA 25 | Aborto | Casamentoa | Perda | 194 (99.0) | 0.80 |
| SAHLPA 26 | Hemorroida | Veias | Coração | 188 (95.9) | 0.61 |
| SAHLPA 27 | Anormal | Semelhantea | Diferente | 193 (98.5) | 0.74 |
| SAHLPA 28 | Menstrual | Mensal | Diário | 195 (99.5) | 0.95 |
| SAHLPA 29 | Ataque | Ferida | Saudável | 181 (92.4) | 0.48 |
| SAHLPA 30 | Calorias | Vitaminas | Alimentos | 183 (93.4) | 0.59 |
| SAHLPA 31 | Comportamento | Pensamento | Conduta | 164 (83.7) | 0.45 |
| SAHLPA 32 | Convulsão | Tonto | Calmoa | 181 (92.4) | 0.48 |
| SAHLPA 33 | Retal | Regador | Supositório | 186 (94.9) | 0.54 |
| SAHLPA 34 | Alérgico | Resistência | Reação | 194 (99.0) | 0.84 |
| SAHLPA 35 | Apêndice | Coçara | Dor | 194 (99.0) | 0.79 |
| SAHLPA 36 | Artrite | Estômago | Articulação | 176 (89.9) | 0.57 |
| SAHLPA 37 | Cafeína | Energia | Água | 184 (93.9) | 0.51 |
| SAHLPA 38 | Colite | Intestino | Bexiga | 168 (85.7) | 0.29 |
| SAHLPA 39 | Vesícula biliar | Artéria | Órgão | 180 (91.8) | 0.47 |
| SAHLPA 40 | Icterícia | Amarelo | Branco | 151 (77.0) | 0.37 |
| SAHLPA 41 | Próstata | Circulação | Glândula | 172 (87.8) | 0.53 |
| SAHLPA 42 | Potássio | Mineral | Proteína | 154 (78.6) | 0.34 |
| SAHLPA 43 | Recomendado | Instrução | Decisão | 167 (85.2) | 0.37 |
| SAHLPA 44 | Incesto | Família | Vizinhos | 158 (80.6) | 0.41 |
| SAHLPA 45 | Irritação | Rígido | Doridoa | 169 (86.2) | 0.35 |
| SAHLPA 46 | Sífilis | Contracetivoa | Preservativo | 126 (64.3) | 0.28 |
| SAHLPA 47 | Testículo | Óvulo | Esperma | 179 (91.3) | 0.55 |
| SAHLPA 48 | Herpes | Ar | Sexo | 139 (70.9) | 0.28 |
| SAHLPA 49 | Impetigo | Cabelo | Pele | 63 (32.1) | −0.12 |
| SAHLPA 50 | Obstipação | Preso | Solto | 160 (81.6) | 0.38 |
A pilot version was administered to a sample of six people (that included men and women between the ages of 15 and 65) and the instructions wording was adjusted for clarity.
Sample and recruitmentThe adapted version of the instrument was administered to a convenience sample of 249 people, as part of a validation study of individual health literacy instruments in the Portuguese population.12 Participants were recruited from four different groups: physicians from public hospitals and primary care health centres (n = 53), health researchers from a research institute in public health (n = 45), researchers from areas unrelated to health from an engineering faculty (n = 50), and laypersons from the general population users of a primary care health centre (n = 101). We followed the administration instructions of the original instrument, i.e., participants were shown the laminated flash cards by a trained interviewer and were asked to read the bolded term out loud and to choose the associated term from the bottom two options.
Eligibility criteria for the participants were age over 18 years and ability to speak and read Portuguese. Potential participants with impaired vision were excluded.
Statistical analysisParticipant characteristics are described using frequencies and median [25th-75th percentiles (P25-P75)] as appropriate, by validation group, for sex and age, and compared across the groups using the χ2 test for sex and the Kruskal-Wallis for age.
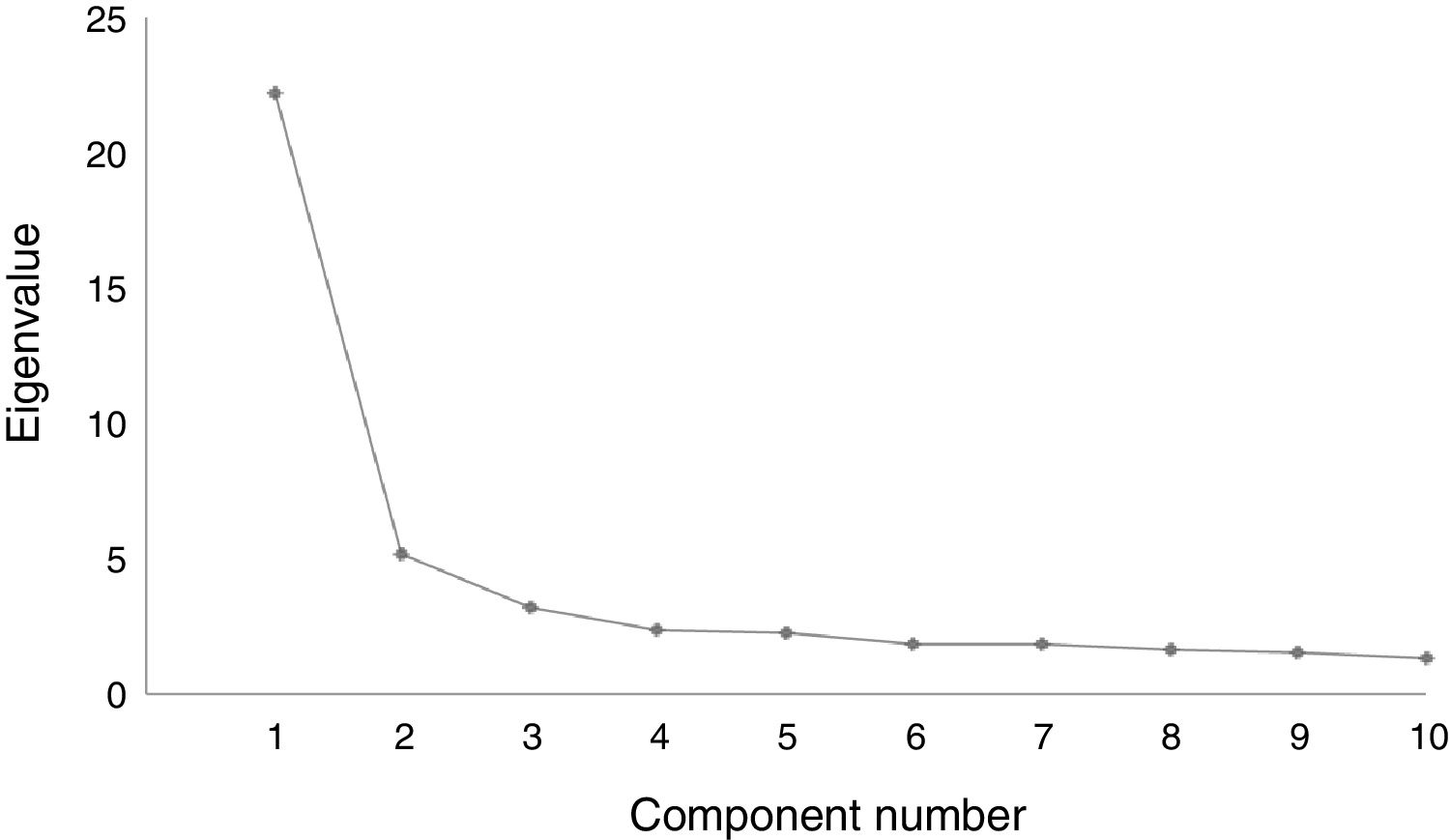
Exploratory factor analysis (by common factor analysis) was performed on the 50 items and visual analysis of the scree plot was used to evaluate homogeneity (i.e., to verify there was a single latent factor measuring reading skills and comprehension). An item was considered to load in a certain factor when it showed an absolute factor loading higher than 0.5. Items with clear ceiling effects (100% participants answering correctly) and items with loadings <0.5 were removed from the instrument. Cronbach's alpha with 95% confidence interval (95%CI) was used to measure internal consistency. Physicians were excluded from these analyses, since they are not part of the target population of the instrument. The global goodness of fit of the underlying model was evaluated using the comparative fit index (CFI) recommended for sample sizes below 250, and the root mean square error of approximation (RMSEA) with 90%CI. We considered the model had good fit when the CFI was higher than 0.95 and the RMSEA was lower than 0.06.19
To assess construct validity we assumed that physicians would score highest on the health literacy test, followed by health researchers, people with a similar academic degree in areas unrelated to health, and finally by laypersons from the general population. Raw scores were compared across these validation groups with the Kruskal-Wallis test, complemented by pairwise comparisons, with a Bonferroni correction to adjust p-values for multiple comparisons. To further test construct validity, SAHLPA scores were also dichotomized at the median of the laypersons subsample into adequate health literacy (scores at or above the median) and limited health literacy. Fisher's exact test was used to compare proportions of limited health literacy across validation groups, with a test for linear trend. Logistic regression was used to calculate odds ratios (OR) and 95%CI to compare the odds of limited health literacy across age and education groups. Physicians were excluded from the regression analyses, since the instrument was not developed to assess them. A sensitivity analysis was performed restricting the regression analysis to the laypersons subsample. Two-sided p values less than 0.05 were considered to define a statistically significant result.
Exploratory factor analysis models were fitted using MPlus (V.5.2; Muthen & Muthen, Los Angeles, California, USA). All other statistical analyses were performed using STATA11®.
Ethics review and consentThe present investigation was carried out in accordance with the Code of Ethics of World Medical Association and the Declaration of Helsinki, and approved by the Ethics Committee of Centro Hospitalar de São João and the National Committee for Data Protection. Both the authors of SAHLSA and SAHLPA authorised the adaptation and validation of the instrument in the Portuguese population. Each participant provided written informed consent.
ResultsCharacteristics of the sample are summarized in Table 2. Women made up the majority of respondents in all validation groups except for the group of engineering researchers (p <0.001). Engineering researchers and laypersons from the general population were older (p <0.001).
Characteristics of the sample by validation group.
| Physicians(n = 53) | Health researchers(n = 45) | Engineering researchers(n = 50) | General population(n = 101) | p | |
|---|---|---|---|---|---|
| Women, n (%) | 34 (64.2) | 37 (82.2) | 6 (12.0) | 64 (63.4) | <0.001a |
| Age in years, median (P25-P75) | 30.0 (27.0-34.0) | 28.0 (26.0-31.0) | 48.5 (31.0-53.0) | 42.0 (34.0-58.0) | <0.001b |
P25-P75: 25th percentile-75th percentile.
The scree plot curve inflected at the first component, revealing a single dimension of the instrument (Fig. 1). This dimension explained 44,4% of the total variance. The global fit of the underlying model was good (CFI = 0.97 and RMSEA = 0.037; 90%CI: 0.030-0.043). Two items (SAHLPA 5 e 7) were removed because of a ceiling effect and 15 items because they had factor loadings below 0.5 (Table 1). The final version contained 33 items (SAHLPA-33) (see Appendix online to this article). SAHLPA-33 showed an adequate degree of reliability, with a Cronbach's alpha of 0.73 (95%CI: 0.68-0.78).

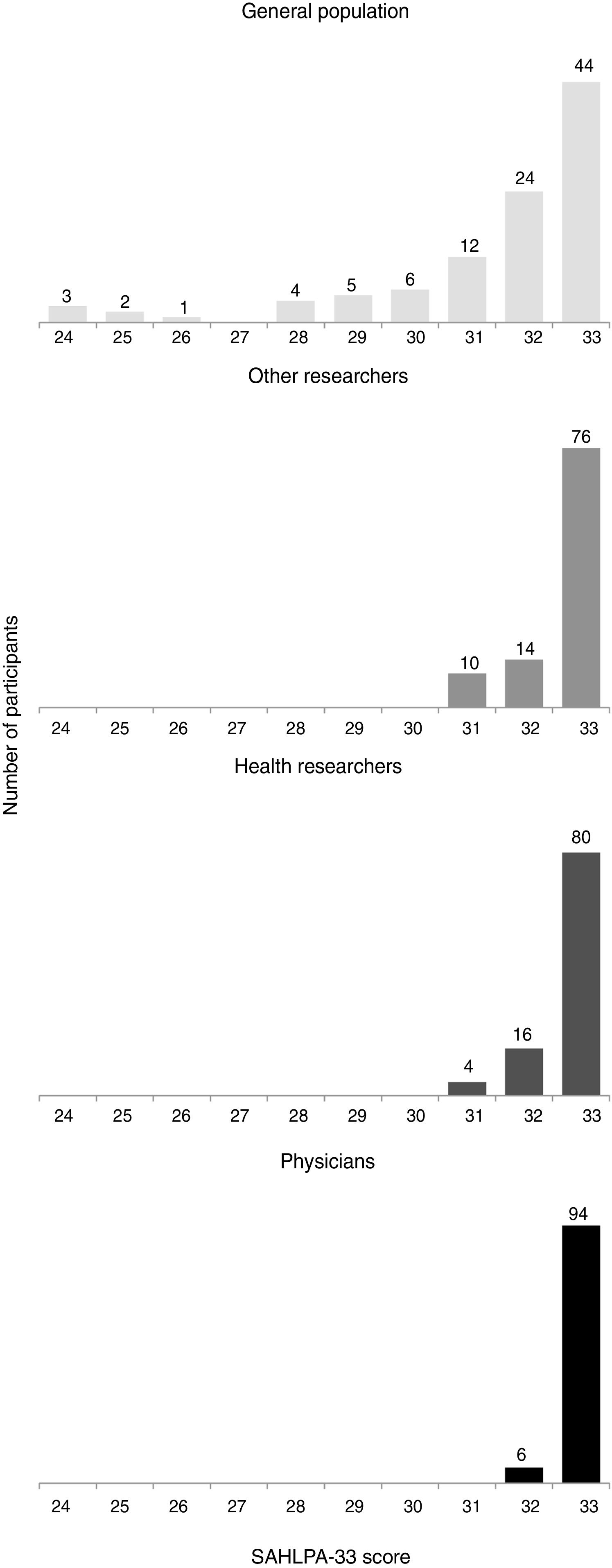
The distributions of SAHLPA-33 scores were left skewed and with positive kurtosis in all validation groups, but with different distribution shapes (Fig. 2). The scores ranged from 24 to 33 in the general population subsample, 31 to 33 for researchers and 32 to 33 for physicians.

There was a statistically significant difference in mean ranks of SAHLPA-33 scores between the four validation groups (p <0.001), with the group of laypersons from the general population exhibiting a lower mean rank of scores than the other groups (all p <0.001), and the group of engineering researchers showing a lower rank of scores than physicians (p = 0.042).
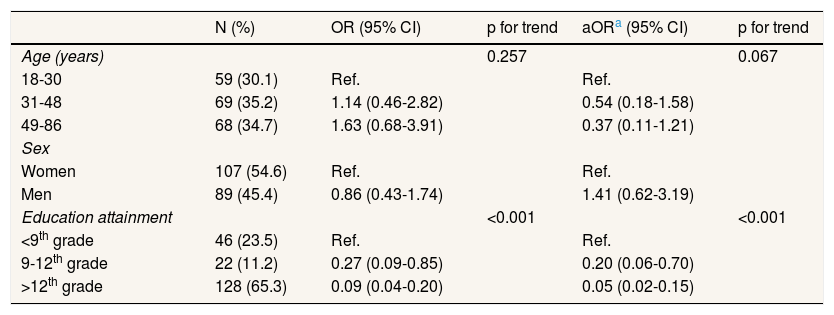
Using health literacy as a binary variable, our data revealed evidence of an association between limited health literacy and validation group (Fisher's test p <0.001; p for trend of the original hypothesis <0.001). In regression analyses, limited health literacy was less common with increasing age, although not significantly (Table 3). There was a negative association between limited health literacy and education attainment (p for trend <0.001). The strongest association was observed for people with education attainment above the twelfth grade; they were significantly less likely to have limited health literacy when compared to people with education attainment below the ninth grade (sex and age-adjusted OR = 0.05; 95%CI: 0.02-0.15).
Odds ratios and 95% confidence intervals (95%CI) for the association between sample characteristics and limited health literacy.
| N (%) | OR (95% CI) | p for trend | aORa (95% CI) | p for trend | |
|---|---|---|---|---|---|
| Age (years) | 0.257 | 0.067 | |||
| 18-30 | 59 (30.1) | Ref. | Ref. | ||
| 31-48 | 69 (35.2) | 1.14 (0.46-2.82) | 0.54 (0.18-1.58) | ||
| 49-86 | 68 (34.7) | 1.63 (0.68-3.91) | 0.37 (0.11-1.21) | ||
| Sex | |||||
| Women | 107 (54.6) | Ref. | Ref. | ||
| Men | 89 (45.4) | 0.86 (0.43-1.74) | 1.41 (0.62-3.19) | ||
| Education attainment | <0.001 | <0.001 | |||
| <9th grade | 46 (23.5) | Ref. | Ref. | ||
| 9-12th grade | 22 (11.2) | 0.27 (0.09-0.85) | 0.20 (0.06-0.70) | ||
| >12th grade | 128 (65.3) | 0.09 (0.04-0.20) | 0.05 (0.02-0.15) |
95%CI: 95% confidence intervals; aOR: adjusted odd ratio; OR: odds ratio.
When considering only the subsample of laypersons, results were similar: there was a significant negative association between limited health literacy and education attainment (p for trend = 0.001) and no significant association with age, although the direction of the association was the same.
DiscussionWe adapted a brief and simple health literacy instrument to European Portuguese, and showed that it was valid and fairly reliable in the Portuguese population. Regarding construct validity, health literacy was significantly associated with health occupation and higher education attainment.
Our results revealed an evident left skew and positive kurtosis in the SAHLPA scores. This asymmetry in scores distribution was more pronounced in our study than in the Brazilian one, which may be explained by the use of a more diverse and literate sample: the average score of the 50-item SAHLPA in our sample was 6 points higher than that found in the Brazilian study, even when considering only the laypersons subsample (43.8; standard deviation [SD] = 4.4 vs. 37.7; SD = 9.0), and 9 points higher when considering the whole sample (46.7; SD = 3.8).14 Furthermore, validation of SAHLPA in the Brazilian population was restricted to patients over 60 years old (mean 74.4 years) and a quarter of the sample (25.7%) had less than 4 years of schooling.14 In contrast, our sample included participants between 18 and 86 years (median 38.5 years), and only 14.8% had less than 4 years of schooling. Hence, our study design oversampled people with higher health literacy, pushing scores to the upper end of the scale.
Our findings show that SAHLPA-33 is fairly reliable. The lower internal consistency (Cronbach's alpha = 0.73), when compared to that of the Brazilian SAHLPA-18 version (Cronbach's alpha = 0.90), could be explained by the lower variability in score distributions, that is known to underestimate the reliability.20
Although two different screening instruments previously validated in the Portuguese population were available,12,16 we decided not to test concurrent validity, because neither of them is considered a gold standard in health literacy assessment. Instead, our strategy relied on examining known-groups validity, that is, administering the instrument to different groups that logically should have different levels of the construct to confirm whether the hypothesized difference was reflected in the scores of the groups.21 Thus, we assumed health literacy would decrease across groups with progressively lower familiarity obtaining and processing health information, in the following order: physicians, health researchers, engineering researchers, laypersons from the general population. Although our data showed a significant trend (p <0.001), the instrument was better at discriminating people in the lower range of the health literacy spectrum, as it was designed to do.10,13
Less educated people tended to have lower health literacy, in accordance with results from previous studies.22
We were not able to find a significant association between limited health literacy and age. The magnitude and direction of this association appears to vary according to the type of assessment instrument used. A recent systematic review found that limited health literacy, when assessed using instruments based on medical vocabulary, such as the REALM (the precursor of SAHLPA), only weakly associates with older age.23 Instruments based on reading comprehension, reasoning, and numeracy skills, such as the NVS or the TOFHLA, in contrast, usually reveal positive associations between limited health literacy and age. The authors argue that crystallized cognitive abilities, such as the ones involved in word recognition and pronunciation, are not affected by aging-related decline, as opposed to those requiring fluid cognitive abilities, more related to reasoning and problem solving. In addition, it is also plausible that as people age and become more exposed to healthcare, their medical vocabulary increases, altering the traditional direction of the association between limited health literacy and age.24 Arguably, our study was underpowered to detect this association.
Some limitations are worth pointing out. SAHLPA is based on the REALM, a test popularly used to assess health literacy, but centred on reading skills. In fact, the REALM was not designed to assess health literacy but to estimate patient reading levels.7 Some authors have suggested that REALM scores should be treated as a correlate or predictor of health literacy and not as a measure of health literacy per se, because the instrument lacks coverage on three primary content areas of health literacy: comprehension, numeracy, and information seeking/navigation.25 SAHLSA and SAHLPA on the other hand, are seen as new instruments26 because they include comprehension of written health materials and thus have better content validity than the REALM. In addition, as is the case with other instruments that directly test individual abilities, they also do not take into account the abilities to interact, communicate or apply critical thinking, which are now included in definitions of health literacy.27,28 According to more recent guidelines, for adequate assessment of the structural validity (the degree to which scores are an adequate reflection of the dimensionality of the construct to be measured), the recommended sample size should be of at least five participants per item.29 Although we had only 3.92 participants per item, based on theory behind the instrument development and on the high bi-serial correlations between the items, it is highly unlikely the instrument could be multidimensional and assess other health literacy sub-dimensions in addition to the word comprehension sub-dimension.13,14,30 We did not examine test-retest reliability and future studies using SAHLPA in less literate samples should determine it. They should also help determine an appropriate cut-off to use health literacy as a binary variable. Future studies should also investigate the relationship between health literacy and gender, as there is a known gender gap in information seeking behaviour, i.e., women are more likely to engage in information seeking than men.31
An instrument based on the Brazilian SAHLPA-18 has been recently validated in the Portuguese population, adding five items to the shortened instrument, all of them drug-related.32 It is undetermined if the addition of these items significantly increased the difficulty of the instrument, rendering it less appropriate for less literate samples. SAHLPA-33 on the other hand, when compared with two other health literacy measurement instruments (the Newest Vital Sign16 and METER12) using item response theory has shown to have better discrimination and precision at lower levels of respondent ability (unpublished manuscript). Future studies should compare the factor structure between Brazilian and Portuguese populations, with both confirmatory factor analysis and differential item functioning. This comparison should also be done with the abovementioned Portuguese version.
SAHLPA-33 fills the gap in health literacy assessment instruments for Portuguese low-literate adults. In contrast to instruments based on self-assessment questions and more vulnerable to non-response bias,17 it offers an objective way to assess health literacy in this vulnerable group. National and international policies now recognize health literacy as a crucial determinant of health and are focusing on strategies to improve it.33–35 Although this instrument does not assess the health literacy demands imposed on individuals or the resources available to individuals and communities, i.e. their distributed health literacy,36 health literacy research in Portugal is very recent and brief assessment instruments are still useful to increase awareness and advance the field. We hope that the SAHLPA-33 can help support policy makers and clinicians in providing more effective health education, specifically targeted to low health literacy adults.
ConclusionWe have adapted a brief and simple instrument to assess health literacy in the Portuguese population. Future studies with less literate samples are needed to supplement and improve on this validation, before SAHLPA-33 is used to explore associations with health outcomes and to guide health interventions, especially in less literate populations. A cross-cultural validation should also be performed to allow comparisons between Brazilian and Portuguese samples, using SAHLPA-18 and SAHLPA-33. In addition, we recommend complementing it with instruments covering other dimensions of the health literacy construct: access, communication, and critical appraisal of health information to make decisions.
Limited health literacy has been linked to more difficult access to care, increased costs and poorer clinical outcomes. Assessing health literacy directly can enable providers and health organisations to target interventions that improve the health literacy of those with lower health literacy and ultimately their health outcomes.
What does this study add to the literature?SAHLPA may fill the gap in brief health literacy assessment for people with low health literacy in Portugal. Studies with less literate samples are needed to supplement and improve on this validation.
Enrique Castro-Sánchez.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsD. Paiva, A. Azevedo and N. Lunet conceived and designed the study. D. Paiva analyzed the data with support of M. Severo. All authors contributed substantially to the interpretation of the data. D. Paiva drafted the manuscript, which was critically revised by all the authors. All authors approved its final version.
FundingThis study was funded by FEDER through the Operational Programme Competitiveness and Internationalization and national funding from the Foundation for Science and Technology – FCT (Portuguese Ministry of Science, Technology and Higher Education) to the Unidade de Investigação em Epidemiologia - Instituto de Saúde Pública da Universidade do Porto (EPIUnit) (POCI-01-0145-FEDER-006862; Ref. UID/DTP/04750/2013); and the FCT Investigator contract IF/01674/2015 (to SS).
Conflicts of interestThere are no conflicts of interest.
We are grateful to each of the participants and to the institutions Faculdade de Engenharia da Universidade do Porto, Instituto de Saúde Pública da Universidade do Porto and Unidade de Saúde Familiar Monte Murado, for enabling participant recruitment.











