





Qualitative methods may help to understand features related to health urban inequalities as a way to include citizens’ perceptions of their neighbourhoods in relation to their health-related behaviours. The aim of this article is to describe the methods and design of a qualitative urban health study.
MethodsThe Heart Healthy Hoods (HHH) analyses cardiovascular health in an urban environment using mixed methods: electronic health records, quantitative individual questionnaires, physical examination, semi-structured Interviews (SSIs), focus groups (FGs) and participatory technics such as photovoice. This article focuses on the HHH qualitative methods and design. A case study was used to select three neighbourhoods in Madrid with different socioeconomic levels: low, medium, and high. The selection process for these three neighbourhoods was as follows: classification of all Madrid's neighbourhoods (128) according to their socioeconomic level; after ranking this classification, nine neighbourhoods, three by socioeconomic level, were short-listed; different urban sociology criteria and non-participant observation were used for the final selection of three neighbourhoods. After selecting the three neighbourhoods, thirty SSIs were held with residents and six SSIs were held with key informants. Finally, twenty-nine FGs will be conducted over the course of 8 months, between May and December of 2018.
ConclusionsSystematization in the selection of neighbourhoods and the use of adequate techniques are essential for the qualitative study of urban health inequalities.
La metodología cualitativa puede ayudar a entender aspectos relacionados con las desigualdades en salud urbana, incluyendo la percepción de los ciudadanos de su barrio en relación con los comportamientos relacionados con su salud. El objetivo de este artículo es describir los métodos y el diseño de un estudio cualitativo sobre salud urbana.
MétodoHeart Healthy Hoods (HHH) es un estudio que analiza la salud cardiovascular en un ámbito urbano, utilizando métodos mixtos: registros electrónicos de salud, cuestionarios individuales cuantitativos, exploraciones físicas, entrevistas semiestructuradas (ESE), grupos de discusión (GD) y técnicas participativas como el fotovoz. Este artículo se centra en los métodos y el diseño de la fase cualitativa del HHH. Se aplicó un estudio de caso, seleccionando tres barrios de Madrid con diferente nivel socioeconómico: bajo, medio y alto. El proceso de selección para estos tres barrios fue el siguiente: clasificación de todos los barrios de Madrid (128) según su nivel socioeconómico; tras graduar la clasificación se seleccionaron nueve barrios de Madrid, tres por nivel socioeconómico; se utilizaron diferentes criterios de sociología urbana y observación no participante para la selección final de tres barrios. Tras la elección de los tres barrios, se realizaron 30 ESE a vecinos y 6 ESE a informantes clave. Finalmente, se están organizando 29 GD con vecinos durante 8 meses, entre mayo y diciembre de 2018.
ConclusionesLa sistematización en la selección de barrios y la utilización de las técnicas adecuadas son fundamentales para el estudio cualitativo de las desigualdades en el entorno urbano.
The study of the urban environment and cardiovascular health is a recurrent topic in recent years in public health and urban sociology.1,2 The new dynamics of city life have been shaped by external factors such as globalization, the impact of technologies, deregulation, and new communications.3,4 These dynamics have led to changes such as “urban outsourcing”, a phenomenon whereby city centers have become the setting for offices, businesses, services and shops.5 Another phenomenon caused by the new dynamics is “gentrification”.6,7 We assume the concept of “gentrification” of Neil Smith6 which is briefly defined as the transformation of inner-city working-class neighborhoods into middle-and upper-middle class neighborhoods.
The analysis of urban setting and its relationships with cardiovascular health leads to the study of inequality in health in the cities, which is based mainly on an analysis of the distinctive features of city neighborhoods. Several studies have confirmed the existence of health inequalities in urban settings.8–10
The main risk factors of cardiovascular diseases involve physical inactivity, diet, harmful alcohol consumption, and smoking.9 The relationship between city neighborhoods and these risk factors of cardiovascular health has been previously studied.11,12
We emphasize the main research studies which have been conducted using a qualitative method applied to the analysis of health inequalities regarding cardiovascular risk factors in an urban environment.13–16 Qualitative research in this area has been based either on one single cardiovascular risk factor or on a specific group, i.e., physical inactivity or Latin women.13,14 It is important to emphasize that previous qualitative studies are designed for the later use of quantitative questionnaires15 or have focused only on poverty and social exclusion.16
In short, qualitative studies are necessary to analyze the four main dimensions in the risk of cardiovascular and chronic diseases from the perspective of health inequalities in urban settings. This approach will facilitate the understanding of structural factors explaining health inequalities as well as the understanding of multiple behaviors in context. In addition, the use of qualitative methods must be accompanied by a suitable design allowing a relevant selection of different socioeconomic areas. This design is fundamental for making suitable comparisons between neighborhoods.
Within this framework, the study objective is to describe the design, methods and qualitative technics used to understand urban cardiovascular health inequalities in the Heart Healthy Hoods (HHH) Project.
MethodThe methodological design of the qualitative study is an ancillary study of the HHH Project. The HHH Project was funded by the European Research Council as a starting grant in 2013 and will be conducted until 2019. The main goal of the HHH study is to understand the physical and social elements impacting upon city residents’ cardiovascular health. The HHH Project uses different techniques such as analysis of electronic health records, questionnaires, physical examination, semi-structured Interviews (SSIs), focus groups (FGs) and participatory technics as photovoice.11,17–20
Photovoice is a participatory action research method used to reflect reality and empower the residents through photography. Within the HHH project this technic has been used for understanding key determinants of the urban environment influencing residents’ health from a residents’ perspective.18
Design of the HHH qualitative studyThe city of Madrid (Spain) is administratively organized into 21 districts and 128 neighborhoods. We decided to include as the study setting three neighborhoods exemplifying (every one of them) the different socioeconomic levels in the city: high, medium and low. We could consider this design as a case study approach similar to the single case-design, type 2, embedded (multiple units of analysis).21 The following steps were taken to finally select these three neighborhoods:
- •
Classification of all Madrid neighborhoods (128) according to socioeconomic level. An ad hoc index was created for this classification. A low value in this index represents neighborhoods with low socioeconomic level, while a higher value represents neighborhoods with high socioeconomic level. We considered seven indicators to represent the demographic and socioeconomic structure of Madrid neighborhoods. We calculated percentages for all the indicators as follows: 1) percentage of the population registered as unemployed over the whole population aged between 16 and 64; 2) percentage of people registered with the Social Security (SS) system with temporary contracts; 3) percentage of people registered with the SS system with part-time contracts; 4) percentage of people registered with the SS system without a university degree, such as office workers and laborers; 5) percentage of the population over the age of 25 who “do not know how to read or write, without formal studies or primary education”; 6) percentage of the population born in a foreign country; and 7) percentage of households with a single parent and one or more children. All these data have been gathered from the Local Government of Madrid's website.22
- •
To build the index, we standardized each indicator using Z-scores and performed an unweighted linear addition obtaining an index for each neighborhood. The Z-scores standardization is calculated by subtracting to each data its average and dividing it by the standard deviation. With each standardization a new indicator is obtained with an average equal to 0 and a variance equal to 1. Next, we stratified Madrid neighborhoods into tertiles; the first tertile included neighborhoods with a high socioeconomic level. The third tertile included the neighborhood with a low socioeconomic level.
- •
After building the classification according to the above criteria, nine neighborhoods were short-listed according to their socioeconomic level (three neighborhoods by tertile):
- •
High socioeconomic level (tertile 1): Fuentelarreina (Fuencarral-El Pardo district); Nueva España (Chamartín district); El Viso (Chamartín district).
- •
Medium socioeconomic level (tertile 2): Palacio (Centro district); Apóstol Santiago (Hortaleza district); El Pilar (Fuencarral-El Pardo district).
- •
Low socio-economic level (tertile 3): San Cristóbal (Villaverde district); San Diego (Puente de Vallecas district); Pradolongo (Usera district).
- •
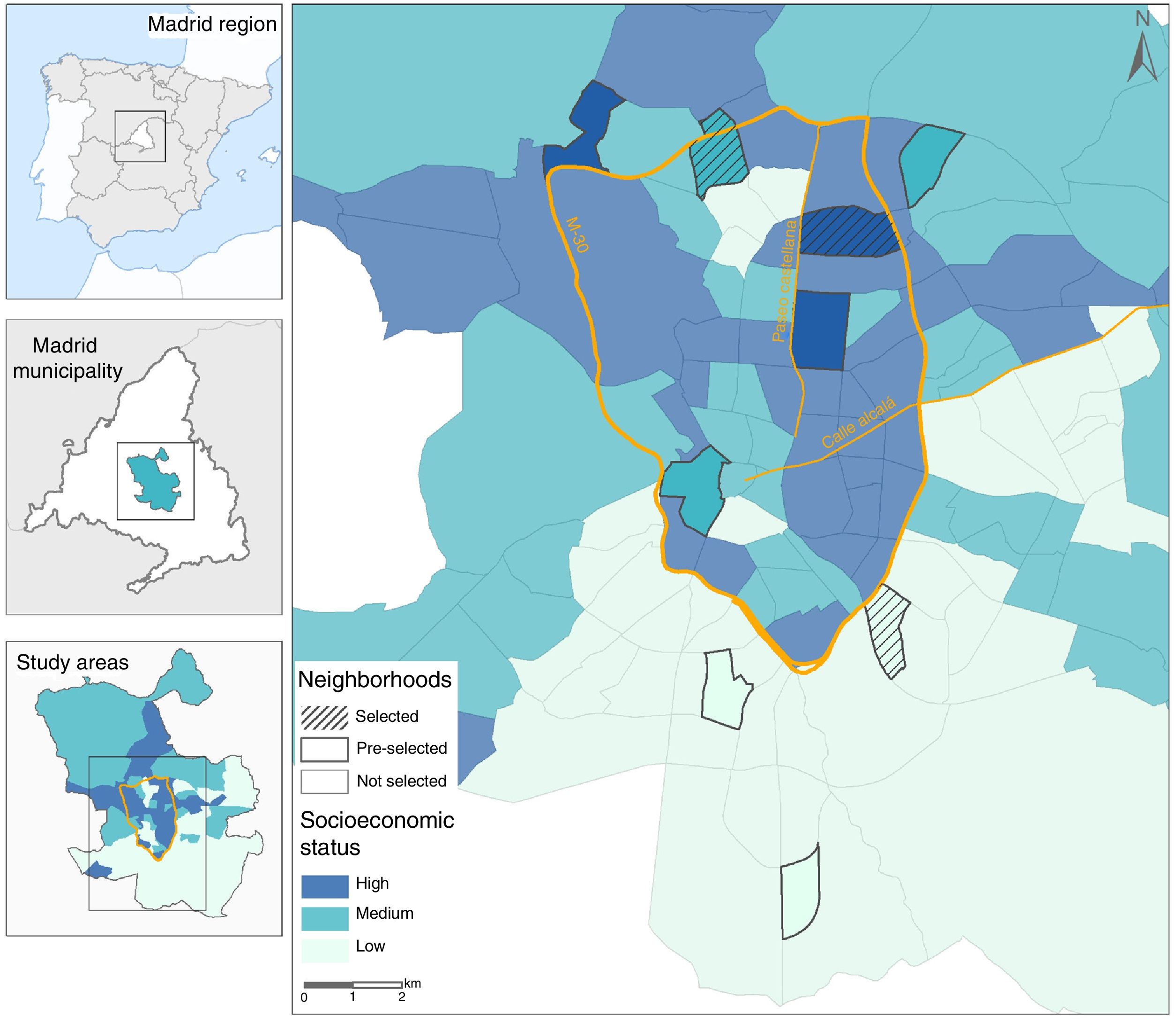
Madrid districts, as well as the location of the nine selected neighborhoods, are shown in Figure 1. The following urban sociology criteria were used for the final selection of the three neighborhoods:
- •
Social heterogeneity in the neighborhood. Social homogeneity will allow us to detect differences in lifestyles between neighborhoods. Even accepting that within each neighborhood there are differences in social structure, studying neighborhoods with high social polarization could lead to the mixture of very different discourses, and limited representation with respect to each neighborhood. The selection of the three neighborhoods should therefore reduce heterogeneity as far as possible.
- •
Gentrification processes in the city. The gentrification process is taking place in cities like Madrid, modifying the social structure of some neighborhoods.21,23 Gentrification is not one of the indicators used in the classification of neighborhoods, but the authors contend that this process should be considered when selecting the three neighborhoods.
- •
Previous research in some of the nine neighborhoods selected. There is one neighborhood called San Cristóbal that is being analyzed by the HHH project team through the photovoice technique in dimensions such as diet24 or physical activities. The reason for not studying San Cristóbal from a qualitative point of view is that residents could discover the objectives and content of the HHH project, possibly triggering the phenomenon called “Social Desirability”.25
- •
Identification with the neighborhood. In the chosen neighborhoods, their residents must feel identified with their neighborhood and their administrative definitions. If the identification with the neighborhood is not fitting to its administrative definition, it would be difficult to find a discourse on that neighborhood.
- •
In addition, non-participant observation technique26 was applied in the nine neighborhoods short-listed. This technique was useful27 for a better understanding of the neighborhoods, i.e., adding information to that provided by the indicators, for instance, to know the type of persons who use parks and the type of activities. A guide for non-participant observation was used and can be seen in the online Appendix of the article.

Once the three neighborhoods have been selected, SSIs were held with residents and key informants, i.e., school principals and health professionals in each one of the three neighborhoods selected. The key informants would help explain the dynamics related to all four health dimensions in every neighborhood: alcohol, tobacco, physical activity and diet. The FGs will be conducted during the course of 8 months, between May and December of 2018.
The authors have decided to use methodological triangulation28 choosing SSIs and FGs as the main techniques because both techniques shed light on the relationship between local residents and their neighborhoods. The SSIs reveal an individual life plan related to the four dimensions studied (tobacco and alcohol consumption, physical activity and diet) and their relationship with the neighborhood.29 The FGs (in this case and to avoid problems in the understanding, the authors consider to FGs similar to “discussion groups” according to the Latin-American tradition30) help to understand how the neighborhood is perceived collectively, and the behaviors related to the four dimensions according to the different collectives, i.e., migrants, pensioners, etc.31
Both SSIs and FGs involving residents have been designed according to specific profiles determined by the following criteria: sex, age, education level, number of children, labor situation, income, family responsibility related to children or grandchildren, years of living in the neighborhood, immigration, tobacco consumption (smoker, ex-smoker, smoker who has participated in health programs to quit smoking), alcohol consumption (occasional drinker or regular drinker), and participation in fitness programs. In the high socioeconomic level neighborhood immigrants were not included. This decision is due to the fact that the highest percentage of immigrants in Madrid live in low and medium socioeconomic level neighborhoods and their impact on these kinds of neighborhoods can be very relevant. A pilot study, conducted between January 2014 and January 2015 in a middle-low socioeconomic neighborhood in Madrid32, helped defining the residents’ profiles to be interviewed and the profile of FGs participants. These profiles are shown in the online Appendix (tables 2 and 3).
Selected neighborhoodsOut of the nine neighborhoods short-listed, three were finally selected for an in-depth study or case study: low socio-economic level: San Diego (Puente de Vallecas district); medium socio-economic level: El Pilar (Fuencarral-El Pardo district); high socio-economic level: Nueva España (Chamartín district)
The three finally selected neighborhoods are shown in Figure 1.
Distribution of semi-structured interviews and focus groups in the selected neighborhoodsA total of thirty SSIs were held, twenty-nine FGs will be conducted with residents, and six SSIs were held with key informants. Table 1 shows the distribution of SSIs and FGs organized in the three neighborhoods in regard to the health dimensions under study.
Distribution of semi-structured interviews and focus groups to be conducted in the three different socioeconomic level neighborhoods of the Heart Healthy Hoods Qualitative Study by health domains.
| Low socioeconomic level neighborhood | Medium socioeconomic level neighborhood | High socioeconomic level neighborhood |
|---|---|---|
| 2 SSIs with key informants | 2 SSIs with key informants | 2 SSIs with key informants |
| Alcohol and tobacco consumption | ||
| 7FGs5 SSIs | 5 FGs6 SSIs | 2 FGs5 SSIs |
| Physical activity and diet | ||
| 7 FGs5 SSIs | 6 FGs3 SSIs | 2 FGs6 SSIs |
FGs: focus groups; SSIs: semi-structured interviews.
Several qualitative studies have been conducted to analyze the relationship between neighborhoods and health;13–16 nevertheless, none of them have provided a systematic design for selecting neighborhoods through the case study or for implementing SSIs and FGs according to different profiles. This is a fundamental issue when studying urban health inequalities.
We used the case study, type 2, embedded (multiple units of analysis), according to Yin24 because it can be useful to describe and to explain different behaviors related to health and it allows the use of several research techniques.
The authors decided to use SSIs and FGs as qualitative techniques. We emphasize the complementarity of SSIs and FGS, i.e. triangulation. The SSI allows us to focus on analyzing the topic without restricting the discourse of the interviewed person.29 The FGs collect collective discourses in the neighborhood on social practices related to health.31 In addition, non-participant observation was used as a criterion of selection of the studied neighborhoods due to this technique enabling us to include a larger space than participant observation without the obligation of participating.25
The authors ruled out the use of other qualitative research techniques such as participant observation or life story interviews. The participant observation technique takes a long time, and would have made it difficult to find results within the deadline of our project.33 The life story interviews would have favored a deeper understanding of the life plan of the people interviewed, but the versatility of profiles would have been lost with this technique.34
Right after, neighborhood exclusion/inclusion criteria by socio-economic level will be explained.
In the low socioeconomic level San Cristobal (Villaverde district) was excluded because it was being studied by the HHH team through the photovoice technique.18 Many people in San Cristobal may be familiar with the HHH project. An information booklet published by the local government35 and results in the media need to be taken into account. This information could come to social desirability.25 Pradolongo (Usera district) has also been excluded because of its administrative definition. Its identity does not exist as such because its residents think their neighborhood is Usera, but Usera is not a neighborhood but a district (a district is formed by many neighborhoods, in this case by seven neighborhoods). In addition, Pradolongo has a very small and dispersed population compared with the other neighborhoods. There are 16,881 people registered in the census, which could make difficult to find an adequate selection of individuals for a FG who, for instance, do not know each other.
San Diego has been chosen in this socioeconomic level for the following reasons:
- •
It has a traditional identity that dates back a long time. Although it belongs to Puente de Vallecas district (a popular area with the left and with many social movements)36 this neighborhood is not to be confused with others in this district. It is small, but with a high population density (39,323 residents). This large population and its identity would allow studying the neighborhood by itself.
- •
San Diego's characteristics make a paradigmatic low socioeconomic setting: a high percentage of immigrants, a well-established Romany community, high unemployment rate, high percentage of part-time labor, etc. It is the second poorest neighborhood after San Cristóbal.
In the medium socioeconomic level Palacio was excluded for the following reasons:
- •
High percentage of rented accommodation.
- •
High mobility (one of the conditions to being interviewed as a resident is to have been living in the neighborhood for at least five years).
- •
High number of hotels or tourists’ accommodation.
The authors consider this neighborhood could be influenced by the gentrification phenomenon, and so it has not been considered suitable for this kind of study.
Apóstol Santiago was excluded as unsuitable for several reasons:
- •
The first disadvantage relates to identity. People living in this neighborhood did not identify themselves with its administrative boundaries. In the past, a place included in the current Apostol Santiago neighborhood (Manoteras) was the focus of the identity of the residents, this identification continues happening. This phenomenon could cause chaotic discourses (in SSIs and FGs) related to the neighborhood boundaries.
- •
It has a social diversity that could make forming the FGs complicated.
- •
Only 16,212 people are registered in the census, which could make it difficult to form FGs without their members knowing each other.
El Pilar was finally selected as the medium neighborhood for the following reasons:
- •
It is the paradigm of a middle-class neighborhood in Madrid. El Pilar reflects the “classic” dynamics of a middle-class neighborhood in Madrid: the moving of the second generation to other parts of the city and a small influx of immigrants has led to an aging population.32
- •
El Pilar has a clear defined identity as a neighborhood.
- •
El Pilar has 45,947 inhabitants, which means it can be studied without any problems.
In the high socio-economic level, Fuentelarreina was excluded for the following reasons:
- •
It has the highest score in the socioeconomic indicators, but it has two very different parts, which were the old Puerta de Hierro area with very luxurious housing and a very high standard of living, and an enclosed residential area with blocks of 5-11 floors built in the 1970s, some of which have a very dilapidated appearance. To mix people from the old Puerta de Hierro area and the enclosed residential area in a FG is not recommended due to the economic differences which would hinder a free-flowing discourse.
- •
It has a problem of numbers, as only 3,203 people live there. This small number of residents would make formation of the FGs difficult.
Nueva España and El Viso neighborhoods (both in Chamartin district) have very similar economic indicators. Finally, Nueva España was selected for three main reasons: there are more people (23,409) than in El Viso (16,847); the socioeconomic indicator is also slightly higher than in El Viso, which probably has a stronger local neighborhood identity, but El Viso is similar to what has happened to Apóstol Santiago, i.e., there was an historic El Viso neighborhood that is now only part of nowadays El Viso, so there is a risk of misunderstanding.
Regarding the limitations of the present study, we acknowledge this is a case study conducted in three neighborhoods with different socioeconomic levels. Therefore, it may not have all the desired representativeness of a large city such as Madrid and there will probably be aspects which we will not be able to consider. Moreover, in spite of our sampling efforts it is very difficult to control the social homogeneity the neighborhoods, especially at a medium socioeconomic level, which could be a handicap for identifying “useful” discourses.
The methods and design of this urban health qualitative study may be useful as a reference and guide for researchers considering a qualitative approach to urban health inequalities. In any research project, as in qualitative research, it is important to follow a rigorous process in the selection of the final settings to be studied and the people whose discourse will be finally analyzed. An accurate and systematic design may allow population studies to incorporate qualitative techniques and case studies into their design for analyzing urban health inequalities.
We consider that this study may help understanding how population health is determined by three dimensions: the place where one lives, the social structure and the collective cultural dimension. Qualitative methodologies allow us to delve into these dimensions, and in turn the dimensions will give us the keys to understanding, for example, why and how in some neighborhoods more physical activity is done and more tobacco and alcohol is consumed than in others. Furthermore, we will be able to understand why and how in some neighborhoods people eat in a different way with respect to others. Therefore, this study might provide useful evidence for the development of urban health policies.
Qualitative methods have been only partially used in urban health research, i.e. poor neighborhoods have been studied applying semi-structured interviews or focus groups. Analyzing, in a qualitative and systematic fashion, neighborhoods of different socioeconomic level to understand urban health inequalities is a novel and necessary approach.
What does this study add to the literature?The present study describes a feasible methodology for investigating health inequalities in large urban settings using a qualitative approach. Qualitative approaches in this research area may shed light complementary to other quantitative and geospatial analyses conducted in the same urban settings as it is the case of the Heart Healthy Hoods project in Madrid (Spain).
Erica Briones-Vozmediano.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsAll the authors made a substantial contribution to the design and execution of this work, as well as to the interpretation of its results. J. Rivera and P. Conde drafted the manuscript, which was critically revised by all the authors, who also approved the final version.
The authors would like to thank Caolán O’Crualaoich for his linguistic assistance on this manuscript, and Daniel Arribas Molero for his collaboration in non-participant observation in the selected neighborhoods in the study.












