



A large volume of public health literature has shown how the social and physical features of a neighbourhood affect residents’ health, and how they contribute to health inequalities. In this article, we argue that citizens, researchers, policy makers and health professionals should engage in creating a common, policy-relevant neighbourhood and health agenda to effectively improve population health and reduce health inequalities. We discuss four critical processes for advancing this neighbourhood and health agenda: 1) citizen participation and community empowerment; 2) policy making; 3) producing relevant research; and 4) how to best communicate between stakeholders. Various methodologies and experiences currently exist to secure and promote citizen participation. Sufficient funding of research projects and specific policies, as well as continued communication strategies among stakeholders, are necessary elements of this neighbourhood and health agenda. Establishing collaborative and sustained relationships between citizens, policy makers, health professionals and researchers at local and higher political levels is a challenging but necessary step. Developing participatory action research and local participatory policy efforts are important steps towards developing a policy- relevant neighbourhood and health agenda.
Numerosos ejemplos de la literatura en salud pública han puesto de manifiesto el impacto de las características sociales y físicas del barrio sobre el estado de salud de las personas residentes, así como su influencia sobre las desigualdades en salud. En este artículo de posicionamiento sostenemos que ciudadanía, personas investigadoras, decisoras políticas y profesionales de la salud deberían involucrarse en construir una estrategia común en barrios y salud, que promueva mejorar la salud de la población y que disminuya de manera efectiva las desigualdades en salud. Para ello identificamos y discutimos cuatro procesos críticos necesarios para avanzar en esta agenda de barrios y salud: 1) la participación y el fortalecimiento de la comunidad; 2) la elaboración de políticas locales; 3) la realización de investigaciones relevantes; y 4) la comunicación entre estos agentes. Existen diferentes metodologías y experiencias que fomentan y promueven la participación y el fortalecimiento de la ciudadanía. A su vez, se requiere una financiación suficiente de proyectos de investigación, políticas específicas y la puesta en marcha de estrategias continuas de comunicación. Establecer relaciones colaborativas a largo plazo, tanto de ámbito local como a niveles superiores, entre ciudadanía, decisores/as políticos/as, expertos/as e investigadores/as es un paso difícil, pero necesario. Desarrollar proyectos de investigación-acción-participación y políticas locales participativas es un paso fundamental para desarrollar una estrategia de barrios saludables políticamente relevante.
The powerful role of the social determinants of health in shaping population health across diverse health outcomes, populations or settings has been vastly acknowledged. The notion that the neighborhood where you live has consequences for your health is also far from new. From Engels studies on mortality in suburban areas in Liverpool,1 to the concept of “walkable neighborhood” and the use of complex systems, research on neighborhoods and health has evolved in many ways, especially in the last 20 years.2,3 Publications linking neighborhood factors to health have grown exponentially. From 1993 to 2014, Oakes et al.2 found 1170 empirically focused research articles focusing on neighborhoods and health.
Some of the seminal work on neighborhoods and health research includes the work of Diez-Roux et al.4 In 1997, she suggested that living in deprived neighborhoods was independently associated with increased prevalence of heart disease using data from large cardiovascular cohort studies. Following these research findings, debates on the strength of the evidence and calls for new analytical and theoretical approaches have appeared in the social epidemiology and urban health literature.5 Moreover, in 2002, the book Neighborhoods and Health, edited by Ichiro Kawachi and Lisa Berman was released, with a second edition in 2018.3 Several approaches on neighborhood differences and effects of health (placed in non-US settings) have appeared in the last decades in public health journals.6,7 Currently, this research has lead us to ask once again: how should we continue advancing this relevant public health field, and how do we act to improve population health?
One possible answer is to shift the current neighborhoods and health agenda to a more inclusive paradigm, including the concerns and views of important stakeholders as citizens, academic researchers, health professionals and policy makers at the local and higher levels.8 By adopting a ‘bottom-up’ approach, this future agenda would deepen our current understanding of how to respond to relevant public health issues in a more culturally appropriately and effective manner. Following this approach, it is relevant to acknowledge the principles of Participatory Action Research and its deep roots in Latin America with the models and experiences of community social development by Marco Marchionni.9 Also relevant is the work developed in the UK working on empowerment processes and resilient communities by Porroche-Escudero et al.10 among others. Several of these ideas have been included in the concept of citizen science that is currently gaining momentum in Europe's research and funding agenda.
Citizen science is the involvement of the public in scientific research. Thereby, citizen science represents a research paradigm shift, in that it engages lay people in the research process —either as contributors, collaborators or co-creators.11 Scientific methodologies and studies become tools at the service of communities in order to promote much needed social changes to improve population health. Engaging citizens into processes focusing on neighborhoods’ health determinants (e.g. barriers and facilitators of healthy food access), leads to actions to collectively advocate for local environmental- and policy-level changes (e.g. to support healthy eating). This approach has shown to be a relevant methodology in several settings,12,13 specifically when these processes can be conducted in collaboration with local policy-makers.14 Moreover, previous studies have shown that there is a mismatch between the expert view and the target group perceptions (e.g. residents).15 The mismatch between what residents perceive as problems and solutions and what we researchers study is of paramount relevance when intervening from a public health perspective. This mismatch has been also studied in Madrid when studying environmental influences on residents’ dietary patterns.16
We acknowledge that actions leading to population health improvement and the reduction of health inequalities in cities and neighborhoods may not always include the participation of public health researchers. Many different political and civil society movements in cities and neighborhoods have their focus on population health. Nevertheless, the inclusion of well-trained researchers and the use of methodologically sound participatory approaches will confirm the evaluation, reproducibility and the possibility of sharing successful experiences at international levels.
Therefore, we consider that engaging citizens and empowering communities are key components in the development of a more relevant neighborhoods and health agenda. Engaging citizens would foster ‘knowledge democracy’ and strengthen urban health including both scientific and lay knowledge in a continued and well established dialogue with relevant stakeholders.17 We acknowledge the large potential of these participatory approaches in a policy relevant neighborhoods and health agenda that warrants further exploration and development.
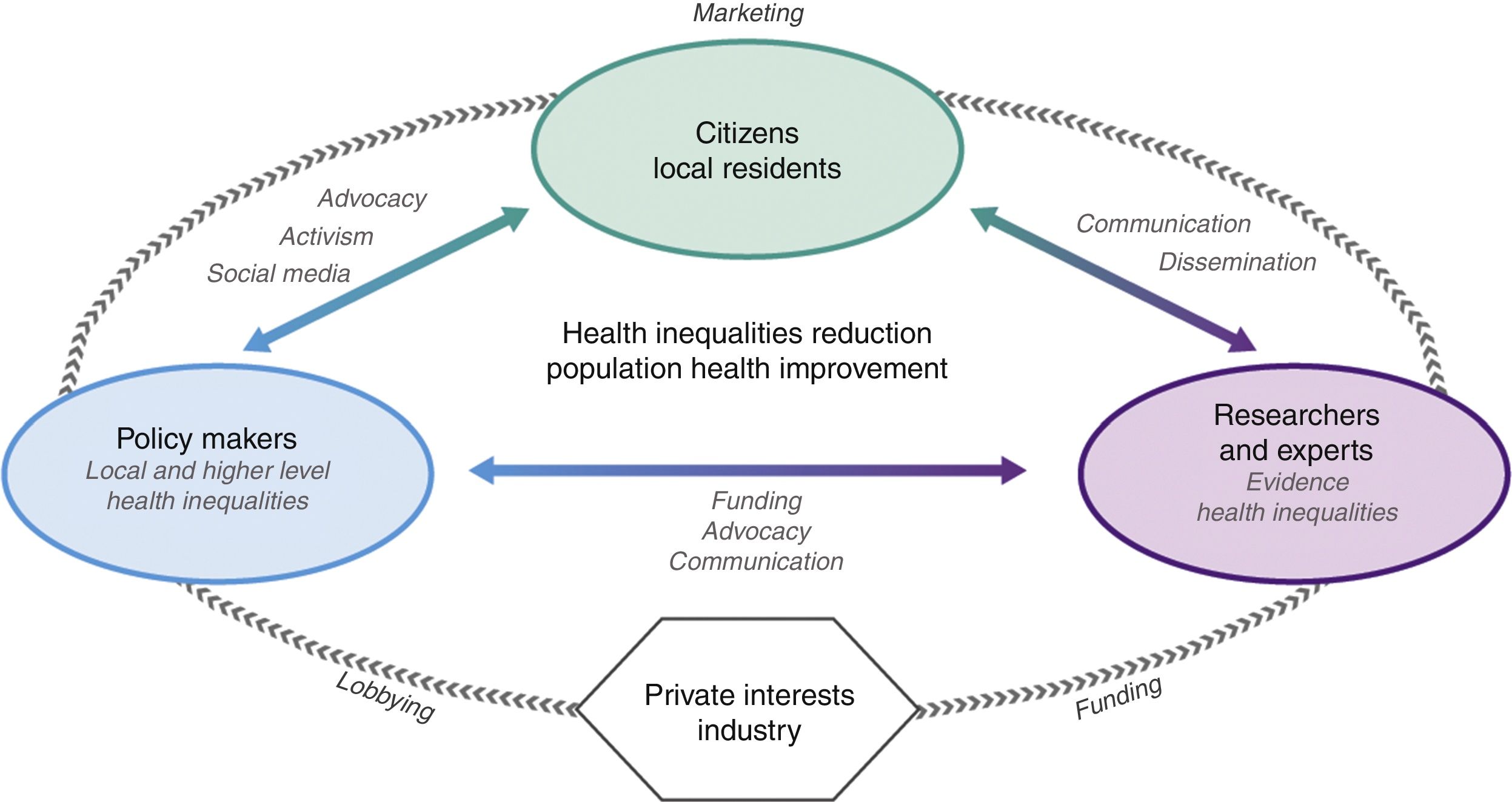
In this article we argue that citizens, policy makers, health professionals and researchers should be aligned to support a relevant neighborhoods and health agenda. Reframing the current agenda towards this new paradigm may effectively improve population health and help reducing health inequalities. We argue that the different stakeholders (citizens, policy makers, health professionals and researchers), as shown in Figure 1, depict the action model and elements required to build a relevant neighborhoods and health agenda.

As shown in Figure 1, we also acknowledge the existence of an important fourth stakeholder: the industry and private interests (e.g. car industry), which relate through lobbying, funding and marketing campaigns to all others three stakeholders. In this context, we argue that a deep understanding of their interests, strategies, and presence is essential. However, their involvement in building this new agenda is not warranted, given that their main interests may not relate neither to improving population health, nor to reduce health inequalities, probably just the contrary. In the next paragraphs, we will discuss four key processes for building this relevant neighborhoods and health agenda: 1) citizen participation, 2) policy making, 3) producing relevant research, and finally 4) effective communication between relevant stakeholders.
Citizen participation and community empowermentCitizen participation, also named community engagement in the literature, is increasingly supported in government policies to promote health. Two recent articles18,19 have highlighted different benefits (such as enhanced social capital or improved self-efficacy) for citizens participating in participatory action research projects. Citizen participation may be very useful in order to achieve population health improvements outside scientific processes. Other authors have developed different frameworks and models to establish and generate effective community participation and community empowerment beyond research. Yet, it is essential to test and adapt these models to integrate intervention activities into community networks.
Enhancing citizen participation can create a sense of public ownership of research and political processes, contributing to the democratization of this new neighborhoods and health agenda.8 However, the engagement of citizens in research and political processes is extremely challenging. While different ways of articulating this collaboration exist (e.g. intersectorial health councils), it should be noted that sometimes ongoing participation processes are not connected to each other. Further, duplicities can occur between different sectors, generating dysfunctional processes (e.g. within different departments at the local level). As such, there is a need to offer new ways of ensuring citizen participation, and to mobilize residents within community processes.
Back in 1978, the conference of Alma-Ata (during the International Conference on Primary Health Care, organized by the World Health Organization) already established citizen participation as a right and duty in planning and implementing health care. In Spain, the Spanish Constitution (1978) also acknowledges citizens’ participation as a fundamental right. However, as stated by Rowbotham et al.8, it is key to engage citizens of different backgrounds and socioeconomic positions, to ensure that the potential benefits of their participation (and their suggested interventions) «do not disproportionately benefit those who are already better off». Thereby, we argue that including those residents with the greatest need to make their voices heard, will reduce health inequalities.
In this context, we argue that citizens’ participation will narrow the gap between researchers, policy makers, health professionals and citizens, and increase the support for public health interventions and policies. Thereby, citizen participation will have positive effects on neighbourhoods and health by contributing to include new knowledge and ideas for different processes of intervening in any given neighbourhood provided by participating citizens. As an example, the Health Observatory in Asturias, part of the public health administration in this Autonomous Community in Spain, launched an action guide on community health in 2016 (publicly available at https://goo.gl/hyqGyW) building on previous regional and national experiences. At the Spanish National level, a Community Health Alliance has been founded to coordinate and visualize local and regional efforts in this area.
Policy makingAs Oliver20 stated back in 2006, «science can identify solutions to pressing public health problems, but only politics can turn most of those solutions into reality». He argued that there are many reasons why population health is a political issue. First, individual and institutional actions often produce effects that can be harmful. Compensating these effects requires taking political decisions about when and how to impose restraints. Second, governments are supposed to identify and satisfy a variety of physical and social society needs. Third, protecting public health involves values and moral judgments, which are less a matter of scientific facts, yet a matter of political organization.21 These values can promote the inclusion of some public health policies in the political agenda. Fourth, a healthy population and workforce is vital to economic growth and social order.
Humphreys and Piot22 also argued that scientific evidence alone is not sufficient basis for health policy because science also has limits in health policy decision making. Therefore, it is also important to take into account government and societal values. In this context, social inequalities in health, as also the different actions implemented to reduce them, can be more or less prioritized (depending on these government and societal values). Moreover, the root causes of health inequalities are hardly known by city policymakers,23 and health policy documents of cities sometimes do not address these causes, because there are mainly focused in targeted interventions.24
One of the strategies to tackle health inequalities is to implement neighborhood-level policies, addressing more resources to those neighborhoods in greater need. It is worth mentioning that neighborhood health inequalities are due to the persistence of structural inequalities due to political decision making, available neighborhood equipment, economic development within the neighborhood, as well as residents’ demographic characteristics.25 Governments that have social justice as a priority will include more easily health inequalities in the political agenda, assigning a specific budget to tackle them.
As an example, we should note that the movement of ‘indignados’ that occurred in Spain after May 2011, criticizing the current economic model26 was important to situate inequalities as a relevant and current problem in our societies and therefore very visible in our cities. As an example, the political parties ‘Barcelona en Comú’ and ‘Ahora Madrid’, that won the elections in 2015 in the cities of Barcelona and Madrid, respectively, are political parties directly emerging from the ‘indignados’ movement of May 2011. ‘Barcelona en Comú’ and ‘Ahora Madrid’ have included social and health inequalities in the focus of their political agenda. As such, several measures have been implemented to reduce social inequalities and consequently health inequalities. It is important to acknowledge that local policies may be influenced by regional, national and supranational, e.g. European-level policies.
Producing relevant researchHigh quality urban health research studies can help developing a neighborhoods and health agenda aimed to significantly reduce health inequalities and improve population health in our cities. Sound research projects need to receive sufficient funds form independent science agencies. This is a crucial starting point for conducting good and impactful research. Participatory urban health research may add innovative processes and will definitely help giving voice to relevant knowledge stemming from citizens.
In Spain, there is a current need for securing sufficient and independent research in order to advance neighborhoods and health research,7,27 which will have implications for the next generations of citizens in a country where 79.8% of the population lived in urban settings in 2016 (according to World Bank population estimates). Researchers may not only produce new and relevant knowledge, but we are also continuously training the next generations of researchers who will produce the necessary knowledge to improve population health in the following decades.
As such, interdisciplinary approaches in neighborhoods and health research are warranted since the relation between cities and health is an extremely complex issue. Experts from different fields of social sciences and public health need to work together in a sustained and integrated fashion. Further, this agenda will benefit from collaborating with media/communication specialists (e.g. journalists, photographers or documentarists). Interdisciplinary and inter-sectorial work is a difficult task given the way that public administrations and academic and research centers are usually organized.
As examples of relevant neighborhoods and health interdisciplinary work that has been conducted in Madrid and Barcelona, respectively, are one on examining alcohol normalization,28 and one evaluating the effects of the Neighborhoods Law on health and health inequalities in Barcelona.29 Interdisciplinary work necessarily leads to the application of different and complementary methodological approaches to study complex problems occurring in neighborhoods in relation to health. These mixed-methods approaches can be successfully applied in public health in order to understand residents’ perspectives on their urban environments determinants.
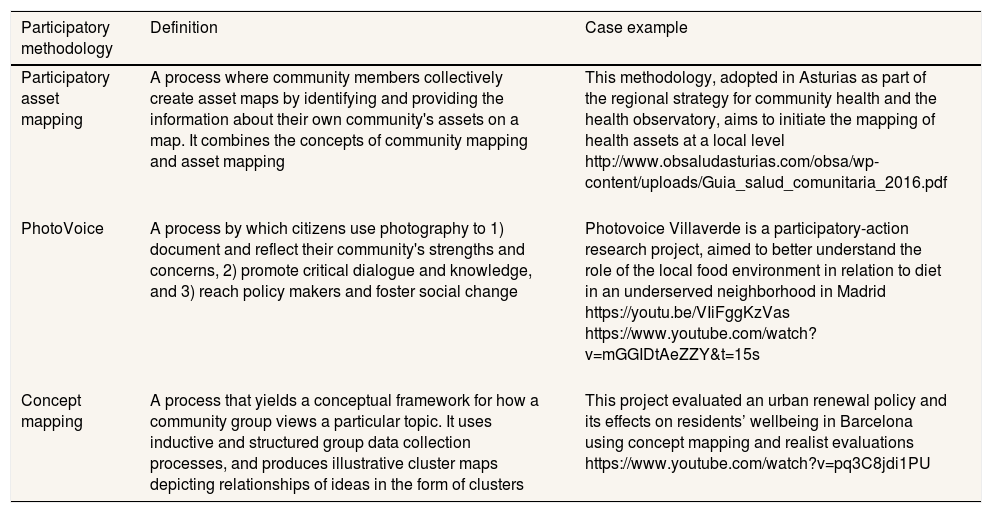
In order to produce policy relevant urban health research30 it is mandatory to disseminate all the scientific results and evidence obtained.31 Evidence should be shared and presented to policy makers, local technicians and practitioners through reports, policy briefs and presentations.32 Research results and evidence also needs to be communicated to citizens and local residents through national and local media as well as specific and relevant social media. In Table 1 we describe several methodologies used by the authors and other public health workers in this area.
Overview of innovative participatory methods for neighborhoods and health.
| Participatory methodology | Definition | Case example |
|---|---|---|
| Participatory asset mapping | A process where community members collectively create asset maps by identifying and providing the information about their own community's assets on a map. It combines the concepts of community mapping and asset mapping | This methodology, adopted in Asturias as part of the regional strategy for community health and the health observatory, aims to initiate the mapping of health assets at a local level http://www.obsaludasturias.com/obsa/wp-content/uploads/Guia_salud_comunitaria_2016.pdf |
| PhotoVoice | A process by which citizens use photography to 1) document and reflect their community's strengths and concerns, 2) promote critical dialogue and knowledge, and 3) reach policy makers and foster social change | Photovoice Villaverde is a participatory-action research project, aimed to better understand the role of the local food environment in relation to diet in an underserved neighborhood in Madrid https://youtu.be/VIiFggKzVas https://www.youtube.com/watch?v=mGGIDtAeZZY&t=15s |
| Concept mapping | A process that yields a conceptual framework for how a community group views a particular topic. It uses inductive and structured group data collection processes, and produces illustrative cluster maps depicting relationships of ideas in the form of clusters | This project evaluated an urban renewal policy and its effects on residents’ wellbeing in Barcelona using concept mapping and realist evaluations https://www.youtube.com/watch?v=pq3C8jdi1PU |
Methodologies and case studies reported here are shown as example of projects in partnership between the co-authors, community-based organizations and city agencies. For a comprehesive review of participatory methodologies, see Minkler M, Wallerstein N. Introduction to community-based participatory research: new issues and emphases. In: Participatory research for health: from process to outcomes. San Francisco: Jossey Bass; 2008. p. 5-23; and Cornwall A, Jewkes R. What is participatory research? Soc Sci Med. 1995;41:1667-76.
Improving population health and addressing health promotion from a local environment perspective (e.g. neighborhood, district, municipality) requires establishing collaborative relationships between community groups, researchers, health professionals and local representatives. These relationships will facilitate effective responses to health priorities.
Given that each urban context has its own characteristics, these relationships will be very context-specific; however, several investigations have identified several factors that influence whether these collaborative relationships are finally effective. Estacio et al.33 pointed out four basic elements for an effective communication strategy between different stakeholders: patience, perseverance, continuous open communication and learning. These relationships need to be based on respect and trust, allowing each person to contribute with their own skills and knowledge. These different stakeholders —health professionals, researchers, community leaders, lay citizens and local policy makers— contribute to the process using their own and differentiated skills and knowledge. Yet, these skills will not emerge without a respectful and trustful communication environment. Including all these stakeholders will necessarily lead to processes of both confrontation and co-creation. In the same way, Eriksson et al.34 concluded that, in order to close the gap between academia and community, it will be required to: share knowledge about effective methods and instruments, time and specific training, leadership and administrative support, a shared language for concepts and tools, an order and commitment to action.
Within the world of primary health care organization and research, a community orientation is absolutely key when stablishing collaborations within a given territory as those needed in a neighborhoods and health agenda.
Regardless of the local context, it is always necessary to clearly identify both the objective of the process, as well as the roles of each of the participants. It is important to consider that all of these processes will be mediated both by the participants’ roles, and by what Peel and Parker35 coined as the ethos and emotional intelligence of each person. Therefore, it is important to set who leads the “relationship”; the one that should promote a culture of solidarity work for all participants, avoiding imposing the procedures and processes.
ConclusionDeveloping a policy relevant neighborhoods and health agenda will help effectively improving population health and reducing health inequalities in our cities. Establishing collaborative and sustained relationships between citizens, policy makers, health professionals and researchers is a challenging but necessary step toward this public health need.
- •
Advancing the neighborhoods and health agenda requires engaging citizens, policy makers, experts and researcher.
- •
While different methodologies and experiences have proven effective to promote citizen participation, there is a need for securing funding and long-term commitment from all the involved stakeholders.
- •
Existing local government policies and public health citizen science project are important examples of how to engage these different stakeholders in the development of effective and sustainable public health actions.
M. Franco conceived the idea. All the authors contributed substantially in writing and critically revising this article. All authors approved the final version.
FundingJ. Diez, P. Gullón and M. Franco were funded by the European Research Council under the European Union's Seventh Framework Programme (FP7/2007-2013/ERC Starting Grant Heart Healthy Hoods Agreement no. 336893).
Conflicts of interestNone.











