




To explore university health science students’ intimate partner violence tolerance and sexist attitudes and to examine their trend throughout the academic years.
MethodsCross-sectional study of students of both sexes of the degrees of medicine, nursing, and psychology from three selected Spanish universities (n = 1,322). Data were collected anonymously using two validated scales: the Dating Violence Questionnaire (DVQ-R) and the Gender Role Attitudes Scale (GRAS). Logistic regressions were used to compare tolerance toward violence and sexist attitudes across the degrees. The evolution of these variables throughout different academic courses was assessed.
ResultsOf the sample, 62.8% were tolerant towards intimate partner violence. The percentage of tolerant students was significantly higher in Psychology (75.9%) than in Nursing (57.7%) and Medicine Degrees (60.3%). A higher percentage of sexist students was also found in psychology students (80.8%) than in nursing (62.2%) and medicine students (62.7%). Compared to the first-year students, female medicine students of the last courses were less tolerant to intimate partner violence (p-trend <0.001), and male medicine students had less sexist attitudes (p-trend = 0.002).
ConclusionsTolerance of intimate partner violence and sexist attitudes were very high, especially among psychology students. These indicators were significantly better among medicine students of higher courses, suggesting a positive effect of medical training. Intimate partner violence in the university education of the future health professionals should be addressed.
.
Explorar la tolerancia de la violencia en la pareja y las actitudes sexistas en estudiantes universitarios/as de ciencias de la salud, y estudiar su tendencia a lo largo de los cursos.
MétodoEstudio transversal en estudiantes de ambos sexos de medicina, enfermería y psicología de tres universidades españolas (n = 1322). Se utilizaron dos escalas validadas y anónimas: Cuestionario de Violencia entre Novios-Revisado (DVQ-R) y Escala de Actitudes de Rol de Género (EARG). Mediante regresiones logísticas se compararon la tolerancia al abuso y las actitudes sexistas entre titulaciones, y se estudió su evolución a lo largo de la formación académica.
ResultadosEl 62,8% se mostraron tolerantes ante la violencia en la pareja. El porcentaje de estudiantes tolerantes fue significativamente más elevado en psicología (75,9%) que en enfermería (57,7%) y medicina (60,3%). También se encontró un mayor porcentaje de estudiantes sexistas en psicología (80,8%) que en enfermería (62,2%) y medicina (62,7%). En comparación con estudiantes de nuevo acceso, las estudiantes de medicina de los últimos cursos fueron menos tolerantes a la violencia (p <0,001) y los estudiantes de medicina varones tuvieron menos actitudes sexistas (p = 0,002).
ConclusionesLa tolerancia de la violencia en la pareja y las actitudes sexistas fueron muy elevadas, especialmente en psicología. Estos indicadores fueron significativamente mejores en estudiantes de medicina de los cursos superiores, lo que sugiere un efecto positivo de la formación médica. Se debería mejorar el abordaje de la violencia en la pareja en la formación universitaria de los/las futuros/as profesionales sanitarios/as.
The prevalence of intimate partner violence (IPV) in youth dating is very high, even higher than in adulthood.1,2 Although psychological IPV is its most frequent expression,3,4 other forms of more direct and recognizable IPV, like physical or sexual IPV, are also common among youth.2,4 Furthermore, as some violent behaviors are often not properly perceived by victims, these figures may be higher.5,6 According to data from the Spanish Government, one out of every three women does not identify controlling behavior as abusive.7 Many young people even justify acts of violence as play or a joke, or they mistakenly interpret them according to romantic sexist ideals,8,9 presenting high IPV-tolerance.10,11 Tolerance of violent behavior and gender role attitudes have been associated with the difficulty of recognizing abuse.12,13
Health professionals —mainly doctors, nurses, and psychologists— play a central role in identifying and addressing IPV. Victims of abuse consider health professionals as necessary support persons.14 Therefore, the comprehensive approach to IPV from the healthcare system has little chance of success if practitioners are not suitably trained to recognize violence and are sufficiently sensitive to its relevance.15 Given that training in IPV is known to increase its recognition and improve attitudes and skills for its treatment,16,17 beginning this training during university studies seems reasonable. However, the development of IPV-related skills and content are poorly covered in health sciences curricula, both internationally18 and in Spain.19,20
To date, no prior study has compared IPV-tolerance and gender role attitudes of future health professionals. Furthermore, we found no studies addressing differences in IPV-tolerance and gender role attitudes among students of consecutive academic courses. Therefore, the objectives were to explore the differences in IPV-tolerance and sexist attitudes among medicine, nursing, and psychology students from three Spanish universities, and to study the evolution of these indicators, comparing students of consecutive academic courses.
MethodStudy design and participantsCross-sectional study among male and female students of the degrees of medicine, nursing, and psychology from three Spanish universities (Universities of Oviedo, Extremadura and Seville), selected according to the availability of a member of the research team. Inclusion criteria were ≥18 years and having been in a dating relationship for at least one month. In order to compare the degrees, students in fifth and sixth course of the medicine degree were excluded. We surveyed 1,430 students who met selection criteria, 905 from the University of Oviedo, 411 from the University of Extremadura, and 114 from the University of Seville. Medicine students represented 38.8% of the sample (n = 555), nursing students 37.0% (n = 529), and psychology students 24.2% (n = 346). Considering all the students registered in the selected health science degrees, response rates were 54.3% in medicine, 50.2% in nursing, and 23.6% in psychology. Overall response rate was 40.3%.
All participants gave passive informed consent (questionnaire instructions indicated implicit consent by completion and return of the form). The study received approval of the universities and of the Committee of Research Ethics of Asturias (Spain).
Data collection and study variablesStudents’ information was obtained through a questionnaire administered in the classrooms between December 2016 and March 2017. Previously, we explained the aims of the study and the anonymous and voluntary nature of participation. Students who had a history of more than one dating relationship were asked to respond with reference to the most problematic relationship. The questionnaire measured IPV-tolerance and sexist attitudes using two scales.
On the one hand, the Perceived Disturbance Scale included in the Dating Violence Questionnaire (DVQ-R), which assesses the level of annoyance about 20 violent behaviors on a five-point scale (not at all = 0, not much = 1, somewhat = 2, quite a bit = 3, and very much = 4) (see Table I of the online Appendix).21 These behaviors are grouped into five forms of IPV: detachment, humiliation, coercion, physical abuse, and sexual abuse. Subsequently, given that perceived annoyance about violent behaviors can be considered the opposite of their tolerance, the scale was inverted. Thereby, higher scores indicated higher IPV-tolerance. Then, options “not at all”, “not much” or “somewhat” were globally considered as “IPV-tolerant”. Following a zero-tolerance policy, which is widely used when referring to several forms of violence or sexism,6,22 students were deemed to be considered IPV-tolerant if they were tolerant of at least one of the behaviors. Although to date, the validation of DVQ-R has only been published with reference to the Victimization Scale —with good internal consistency (Cronbach's alpha: 0.85)21— the satisfactory validity of the Perceived Disturbance Scale could be expected, as both scales use the same items. Moreover, this scale was considered appropriate by consensus of the same panel of experts. Lastly, the Perceived Disturbance Scale has been successfully used in previous research.11
On the other hand, we used the Gender Role Attitudes Scale (GRAS).23 This 20-item scale describes different egalitarian or sexist expressions that people use about the role that men and women play in society according three functions: social, occupational, and family. Each item is rated on a five-point Likert scale ranging from 0 (strongly disagree) to 4 (strongly agree) (see Table II of the online Appendix). Given that sexism can be considered the opposite of gender equality, the scores of items referring to egalitarian expressions were reversed to transform them into sexist attitudes. Subsequently, the options “partially disagree”, “agree” and “strongly agree” were considered as sexist attitudes, and the options “strongly disagree” and “disagree” were considered as egalitarian attitudes. From the perspective of the zero-tolerance policy, students were deemed to have a global sexist attitude when they agreed with at least one sexist attitude considered in of the GRAS. The internal consistency of the GRAS was excellent (Cronbach's alpha: 0.99).23
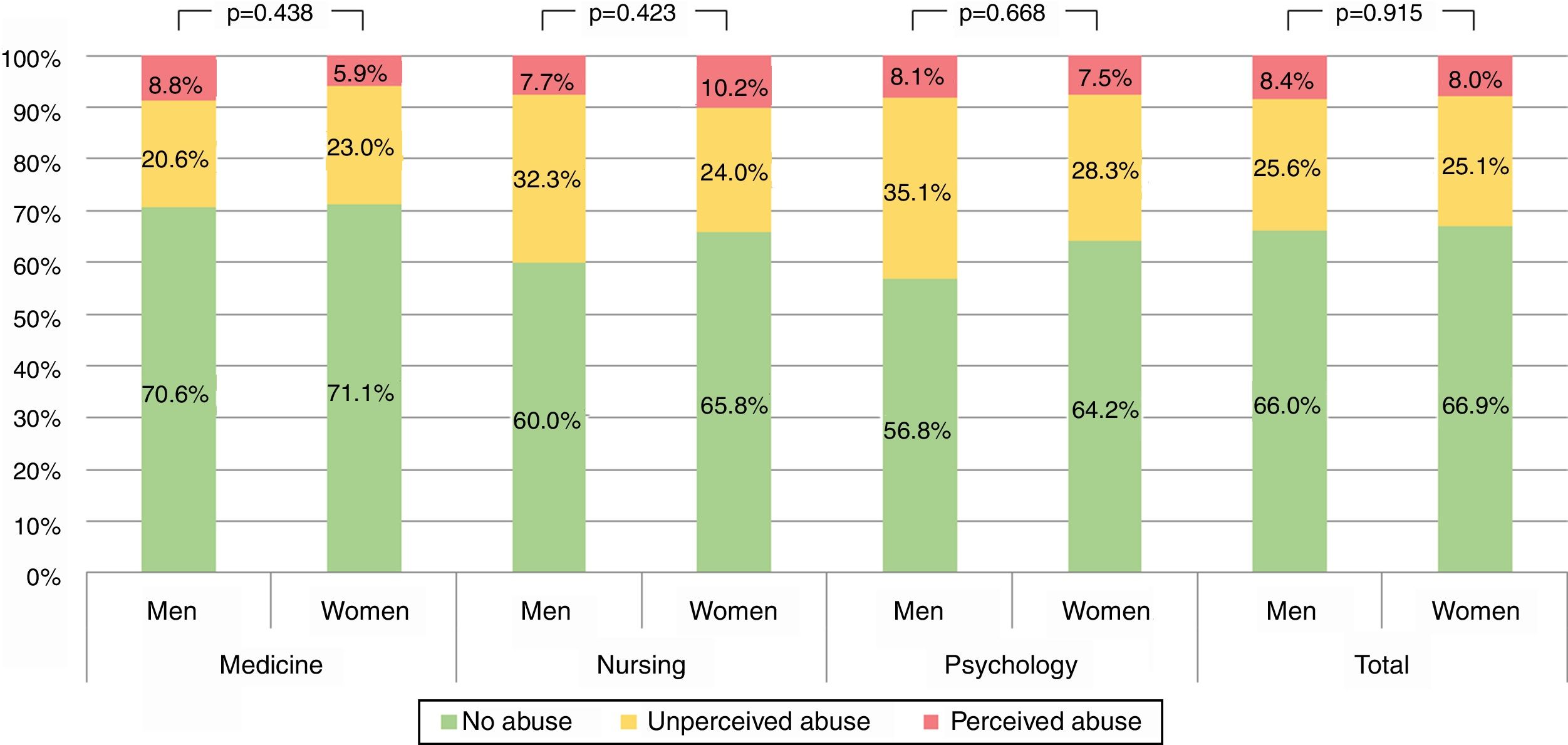
The questionnaire also included potential confounders. Sociodemographic and basic academic data were collected (sex, age, degree, and course). We also studied the perception of abuse, fear, and/or entrapment through three dichotomous (yes/no) self-reported variables. Through these variables we classified students in three levels of perception of abuse: a first group that perceived themselves as abused (i.e., “perceived abuse”); a second group that did not feel abused by their partners but reported being afraid of their partner or having felt trapped during their relationship (i.e., “unperceived abuse”); and a third group made up of youths who claimed not having been abused or feeling afraid or entrapped (i.e., “non-abused”).
Data analysisOf the 1430 students surveyed, we excluded 108 with lacking data in some questionnaire items, leaving a final sample of 1322 individuals (534 from medicine, 497 from nursing, and 291 from psychology).
Sex- and age-differences according to degrees were respectively studied by means of the non-parametric chi-square independence test and the independent t-test, using medicine degree as reference. Differences in abuse perception according sex within each degree were analyzed using the non-parametric chi-square independence test. Then, using the zero-tolerance criteria to operationalize IPV-tolerance and sexism, logistic regressions separately by sex were used to compare the estimated crude proportion of IPV-tolerant students and sexist attitudes according to the degree. Moreover, we obtained adjusted proportions derived from predicted probabilities using logit models separately by sex, adding the degree as indicator and the age and perception of abuse (perceived abuse, unperceived abuse, non-abused) as potential confounders. These results are shown for each IPV-tolerance forms and sexism functions. Analogously, crude and adjusted proportions for total IPV-tolerance and total sexism according to the academic course (included in the regression model as categorical variable) were calculated separately by sex and degree. Subsequently, to estimate the evolution of IPV-tolerance and sexist attitudes throughout academic formation, we obtained the p-trend by running analogous regression models but with academic course modelled as a continuous variable (from 1 = first course to 4 = fourth course). Lastly, in order to determine the robustness of our findings, we repeated main analyses using linear regression models and introducing IPV-tolerance and sexism as quantitative variables, both of them ranging from 0 to 80 points (maximum IPV-tolerance/sexism). All analyses were conducted and presented separately for each sex.
Data analysis was performed using STATA v.13. Only values of p <0.05 were considered statistically significant.
ResultsOf the total sample, 1060 were women (80.2%) and 262 were men (19.8%). The percentage of women was higher in the psychology (87.3%; p <0.001) and nursing degrees (86.9%; p <0.001) than in medicine (70.0%). Mean age (± standard deviation) was 21.3 in nursing (± 4.7 years), 20.6 in medicine (± 2.9 years), and 19.5 in psychology (± 1.7 years). Compared to medicine students, mean age was significantly higher in nursing students (p = 0.001) and lower in psychology students (p <0.001).
Regarding students’ perception of abuse, 8.4% men and 8.0% women perceived themselves as abused, whereas 25.6% of men and 25.1% of women were in a situation of unperceived abuse. Unperceived abuse was more frequent in the psychology degree, followed by nursing and medicine (Fig. 1).

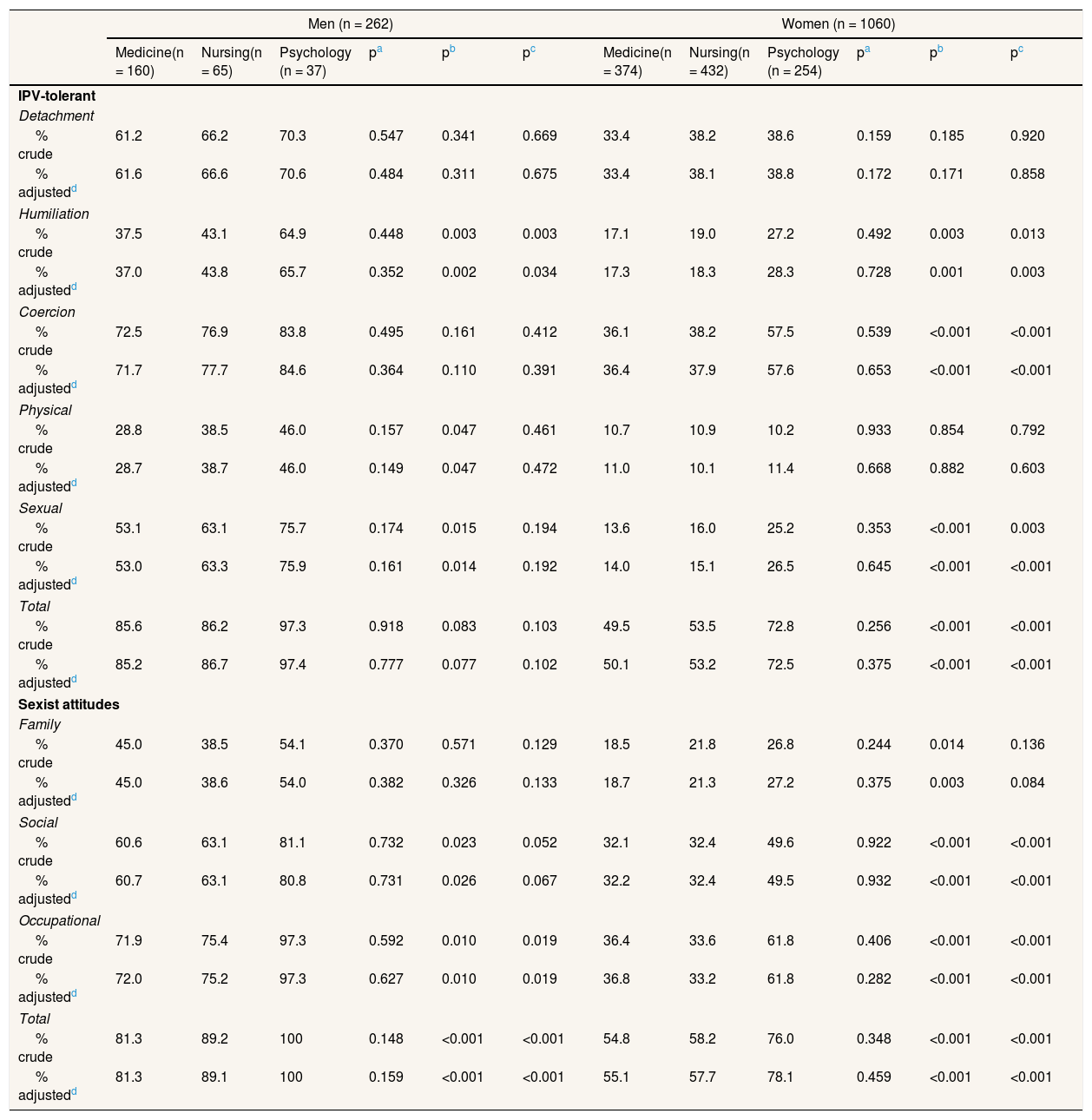
A higher percentage of psychology students were tolerant towards all forms of IPV than were students of medicine and nursing. This was consistent across sexes, despite the lack of statistical power in the men's stratum, except for humiliation (Table 1). Findings regarding sexist attitudes were similar (Table 1).
Estimated proportion of students tolerant to each intimate partner violence and with sexist attitudes using a zero-tolerance criterion according to sex and degree.
| Men (n = 262) | Women (n = 1060) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medicine(n = 160) | Nursing(n = 65) | Psychology (n = 37) | pa | pb | pc | Medicine(n = 374) | Nursing(n = 432) | Psychology (n = 254) | pa | pb | pc | |
| IPV-tolerant | ||||||||||||
| Detachment | ||||||||||||
| % crude | 61.2 | 66.2 | 70.3 | 0.547 | 0.341 | 0.669 | 33.4 | 38.2 | 38.6 | 0.159 | 0.185 | 0.920 |
| % adjustedd | 61.6 | 66.6 | 70.6 | 0.484 | 0.311 | 0.675 | 33.4 | 38.1 | 38.8 | 0.172 | 0.171 | 0.858 |
| Humiliation | ||||||||||||
| % crude | 37.5 | 43.1 | 64.9 | 0.448 | 0.003 | 0.003 | 17.1 | 19.0 | 27.2 | 0.492 | 0.003 | 0.013 |
| % adjustedd | 37.0 | 43.8 | 65.7 | 0.352 | 0.002 | 0.034 | 17.3 | 18.3 | 28.3 | 0.728 | 0.001 | 0.003 |
| Coercion | ||||||||||||
| % crude | 72.5 | 76.9 | 83.8 | 0.495 | 0.161 | 0.412 | 36.1 | 38.2 | 57.5 | 0.539 | <0.001 | <0.001 |
| % adjustedd | 71.7 | 77.7 | 84.6 | 0.364 | 0.110 | 0.391 | 36.4 | 37.9 | 57.6 | 0.653 | <0.001 | <0.001 |
| Physical | ||||||||||||
| % crude | 28.8 | 38.5 | 46.0 | 0.157 | 0.047 | 0.461 | 10.7 | 10.9 | 10.2 | 0.933 | 0.854 | 0.792 |
| % adjustedd | 28.7 | 38.7 | 46.0 | 0.149 | 0.047 | 0.472 | 11.0 | 10.1 | 11.4 | 0.668 | 0.882 | 0.603 |
| Sexual | ||||||||||||
| % crude | 53.1 | 63.1 | 75.7 | 0.174 | 0.015 | 0.194 | 13.6 | 16.0 | 25.2 | 0.353 | <0.001 | 0.003 |
| % adjustedd | 53.0 | 63.3 | 75.9 | 0.161 | 0.014 | 0.192 | 14.0 | 15.1 | 26.5 | 0.645 | <0.001 | <0.001 |
| Total | ||||||||||||
| % crude | 85.6 | 86.2 | 97.3 | 0.918 | 0.083 | 0.103 | 49.5 | 53.5 | 72.8 | 0.256 | <0.001 | <0.001 |
| % adjustedd | 85.2 | 86.7 | 97.4 | 0.777 | 0.077 | 0.102 | 50.1 | 53.2 | 72.5 | 0.375 | <0.001 | <0.001 |
| Sexist attitudes | ||||||||||||
| Family | ||||||||||||
| % crude | 45.0 | 38.5 | 54.1 | 0.370 | 0.571 | 0.129 | 18.5 | 21.8 | 26.8 | 0.244 | 0.014 | 0.136 |
| % adjustedd | 45.0 | 38.6 | 54.0 | 0.382 | 0.326 | 0.133 | 18.7 | 21.3 | 27.2 | 0.375 | 0.003 | 0.084 |
| Social | ||||||||||||
| % crude | 60.6 | 63.1 | 81.1 | 0.732 | 0.023 | 0.052 | 32.1 | 32.4 | 49.6 | 0.922 | <0.001 | <0.001 |
| % adjustedd | 60.7 | 63.1 | 80.8 | 0.731 | 0.026 | 0.067 | 32.2 | 32.4 | 49.5 | 0.932 | <0.001 | <0.001 |
| Occupational | ||||||||||||
| % crude | 71.9 | 75.4 | 97.3 | 0.592 | 0.010 | 0.019 | 36.4 | 33.6 | 61.8 | 0.406 | <0.001 | <0.001 |
| % adjustedd | 72.0 | 75.2 | 97.3 | 0.627 | 0.010 | 0.019 | 36.8 | 33.2 | 61.8 | 0.282 | <0.001 | <0.001 |
| Total | ||||||||||||
| % crude | 81.3 | 89.2 | 100 | 0.148 | <0.001 | <0.001 | 54.8 | 58.2 | 76.0 | 0.348 | <0.001 | <0.001 |
| % adjustedd | 81.3 | 89.1 | 100 | 0.159 | <0.001 | <0.001 | 55.1 | 57.7 | 78.1 | 0.459 | <0.001 | <0.001 |
IPV: intimate partner violence.
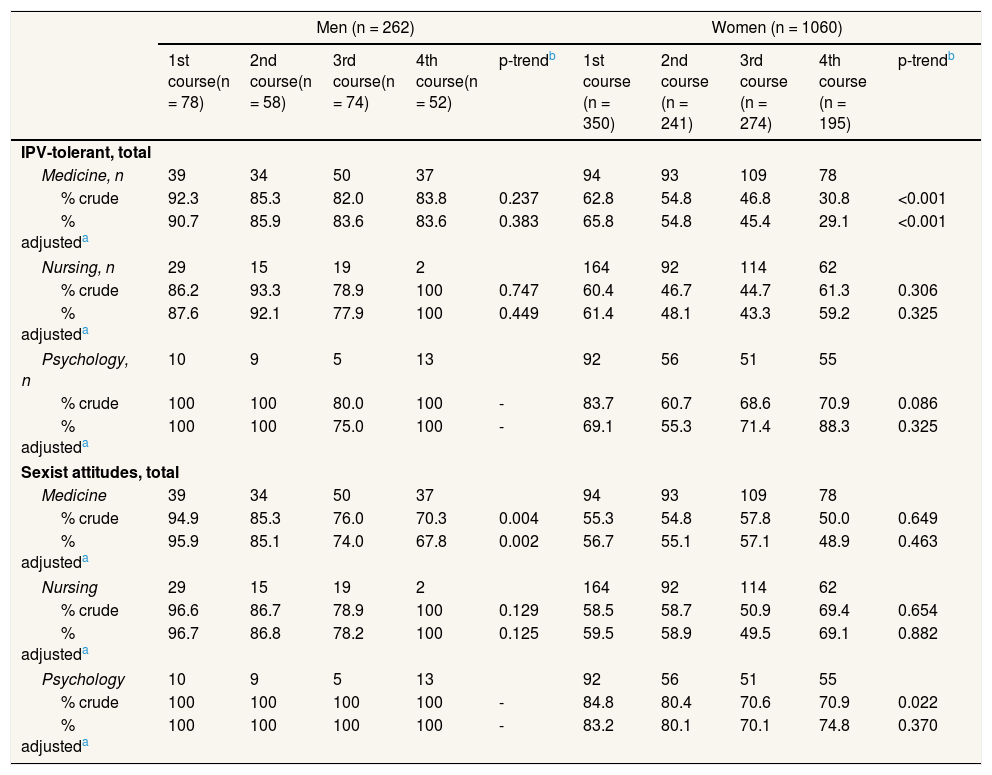
Table 2 shows the proportion of IPV-tolerant students and students with sexist attitudes according to sex, academic course, and degree. Compared to students of the first courses, only female medical students of higher courses showed less total IPV-tolerance. Likewise, the percentage of sexist attitudes was significantly lower among male medical students of higher courses. Similar results were obtained when repeating the analyses modeling IPV-tolerance and sexism as quantitative variables (see Table III of the online Appendix).
Estimated proportion of students tolerant to intimate partner violence and with sexist attitudes using a zero-tolerance criterion according to sex, degree and academic course.
| Men (n = 262) | Women (n = 1060) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1st course(n = 78) | 2nd course(n = 58) | 3rd course(n = 74) | 4th course(n = 52) | p-trendb | 1st course (n = 350) | 2nd course (n = 241) | 3rd course (n = 274) | 4th course (n = 195) | p-trendb | |
| IPV-tolerant, total | ||||||||||
| Medicine, n | 39 | 34 | 50 | 37 | 94 | 93 | 109 | 78 | ||
| % crude | 92.3 | 85.3 | 82.0 | 83.8 | 0.237 | 62.8 | 54.8 | 46.8 | 30.8 | <0.001 |
| % adjusteda | 90.7 | 85.9 | 83.6 | 83.6 | 0.383 | 65.8 | 54.8 | 45.4 | 29.1 | <0.001 |
| Nursing, n | 29 | 15 | 19 | 2 | 164 | 92 | 114 | 62 | ||
| % crude | 86.2 | 93.3 | 78.9 | 100 | 0.747 | 60.4 | 46.7 | 44.7 | 61.3 | 0.306 |
| % adjusteda | 87.6 | 92.1 | 77.9 | 100 | 0.449 | 61.4 | 48.1 | 43.3 | 59.2 | 0.325 |
| Psychology, n | 10 | 9 | 5 | 13 | 92 | 56 | 51 | 55 | ||
| % crude | 100 | 100 | 80.0 | 100 | - | 83.7 | 60.7 | 68.6 | 70.9 | 0.086 |
| % adjusteda | 100 | 100 | 75.0 | 100 | - | 69.1 | 55.3 | 71.4 | 88.3 | 0.325 |
| Sexist attitudes, total | ||||||||||
| Medicine | 39 | 34 | 50 | 37 | 94 | 93 | 109 | 78 | ||
| % crude | 94.9 | 85.3 | 76.0 | 70.3 | 0.004 | 55.3 | 54.8 | 57.8 | 50.0 | 0.649 |
| % adjusteda | 95.9 | 85.1 | 74.0 | 67.8 | 0.002 | 56.7 | 55.1 | 57.1 | 48.9 | 0.463 |
| Nursing | 29 | 15 | 19 | 2 | 164 | 92 | 114 | 62 | ||
| % crude | 96.6 | 86.7 | 78.9 | 100 | 0.129 | 58.5 | 58.7 | 50.9 | 69.4 | 0.654 |
| % adjusteda | 96.7 | 86.8 | 78.2 | 100 | 0.125 | 59.5 | 58.9 | 49.5 | 69.1 | 0.882 |
| Psychology | 10 | 9 | 5 | 13 | 92 | 56 | 51 | 55 | ||
| % crude | 100 | 100 | 100 | 100 | - | 84.8 | 80.4 | 70.6 | 70.9 | 0.022 |
| % adjusteda | 100 | 100 | 100 | 100 | - | 83.2 | 80.1 | 70.1 | 74.8 | 0.370 |
IPV: intimate partner violence.
Table IV of the online Appendix shows the proportion of students with IPV-tolerance and sexist attitudes according to sex and academic course, in the whole sample. Male students of higher courses had less tolerance toward sexual violence and fewer occupational sexist attitudes. In the case of female students, tolerance to all forms of IPV (except for humiliation) and occupational sexist attitudes were significantly lower among students of higher courses.
DiscussionAccording to the results of this study, the prevalence of IPV-tolerance and sexism was significantly higher in psychology students than in medicine or nursing students. When analyzing students’ differences between consecutive academic courses, IPV-tolerance was lower in female medical students of higher courses, and sexist attitudes were lower in male medical students of higher courses, suggesting that some aspects of future doctors’ training may address violence more than in other degrees. These sex differences deserve further consideration. In any case, it should be considered that the overall high prevalence of IPV-tolerance and sexism observed among students of health sciences could be due to the very sensitive zero-tolerance criterion employed (cut-off point: presence of tolerance towards a single IPV behavior and presence of a single sexist attitude), which may have increased false positives.
The fact that both male and female students of the psychology degree were more IPV-tolerant than the other health science students included in our study, even after adjusting for age and perception of abuse, deserves a profound reflection. Interestingly, in a recent study requested four groups of people to rate a series of simulated cases of self-inflicted violence, and psychology students committed errors similar to those of the group of volunteers.24 In another study, the acceptance by police officers and psychology students of some sexist stereotypes that emerge in cases of rape were compared.25 The results revealed that the students were more tolerant than the police officers toward myths like “she asked for it” and “he did not mean to”. Perhaps during psychology studies, the excess of theoretical and practical exposure to information and examples of dysfunctional behaviors and situations desensitizes students, increasing their tolerance. This is similar to medical and nursing students’ progressive loss of empathy towards physical disease during their studies.26 This explanation has also been supported in another observation derived from our results: the differences between the degrees in total tolerance in the first course are very small when compared with the differences that emerge in the fourth year. This suggests that advancing in psychology studies may contribute to the students’ acceptance of IPV; or at least, studying psychology may not foster IPV-rejection, unlike the other degrees. Another possible explanation for this finding is that psychology students were also notably more sexist than the other health science students. It seems clear that the less gender equity there is, the more IPV-tolerance and perpetration will exist.27,28 This same consideration may explain sex differences in IPV-tolerance, as male students were both more sexist and more IPV-tolerant than female students. Accordingly, sexist attitudes could be a first step in the pathway toward IPV-tolerance. In any case, beyond the possible explanations for these findings and considering the fatal implications of graduate psychologists with some IPV-tolerance or sexist attitudes, the design of suitable curricular tools to fight against IPV-tolerance and sexism are urgently needed. Previously, future research should confirm our findings and explore in greater depth the reasons we have hypothesized.
Differences in gender-role attitudes between psychology, medicine, and nursing students can also be analyzed similarly. In this case, the differences are very marked in the first course, indicating that psychology, medicine, and nursing students probably have different conceptions of gender equity already before starting their studies. In general, sexist attitudes were particularly manifest in the occupational sphere. This agrees with results of other authors who have warned that sexist occupational attitudes can be the most firmly rooted in society.23,29
Notwithstanding the cross-sectional nature of the study design, which urges caution in the interpretations, our results concerning the overall evolution of IPV-tolerance and sexism according to the academic course revealed interesting sex differences. On the one hand, there was a significant trend towards less IPV-tolerance in women over academic courses, but not in men. On the other hand, there was a significant decrease of sexism in men, but not in women. These findings suggest that changes in sexist attitudes come first, and only then does the teachable moment to produce changes in IPV-tolerance emerge. Given that women began university studies with more egalitarian attitudes than men, the progression throughout academic courses could produce improvements in IPV-tolerance. If this hypothesis is true, men would fail to find their teachable moment to reduce IPV-tolerance until postgraduate training or during clinical practice, which is probably too late.
The analysis of the evolution of the prevalence of IPV-tolerance and sexist attitudes in each degree suggests that only medicine students underwent a consistent and positive change throughout their studies, male students in sexist attitudes and female students in IPV-tolerance. It is difficult to offer a tentative hypothesis to explain this phenomenon because, in all three degrees, IPV is addressed at some point, and professors seem to be sufficiently committed to this formation.20,30 In addition, the psychology degree has the most curricular content about violence, but if we were seeking a student sensitized toward suffering, we would probably choose a nursing student. So, how is the medicine degree different? Perhaps medicine students are urged very early on to become participants in the unavoidable responsibility they will acquire to identify and treat cases of IPV, and this makes them more sensitive to the problem. There are numerous studies and experiences suggesting that any training in IPV is satisfactory for medicine students, especially if it is transversal and addresses real cases.31,32 Therefore, perhaps a greater effort should be made in nursing and psychology degrees, seeking higher student commitment towards IPV, emphasizing that they will be partly responsible for dealing with IPV and banishing some stereotypical ideas that contribute to IPV-tolerance and sexism.33
Our study has several limitations. The main one involves the cross-sectional nature of the data, which prevents us from analyzing with a high degree of validity the association between a certain academic course and changes in IPV-tolerance and sexist attitudes. Thereby, in order to appropriately test this hypothesis, we recommend conducting longitudinal research with a large cohort of students. A second limitation was our convenience sample, which does not allow the generalization of results. However, the aim was not to study the prevalence of IPV-tolerance and sexism, but their association across some health science degrees and over academic courses. In addition, although groups of students were quite comparable according to degree, some strata had few participants, and there was also a high disparity in the number of students from each university. Another limitation regarding the sample was having obtained a response rate below 50%, mainly due to a percentage of students who do not attend classes regularly. Moreover, students who attend regularly may differ from the others in academic variables. A third limitation was that our study did not include a sample of students from the social work degree, although social workers are acknowledged as essential health professionals to deal with IPV and as the best trained to provide an appropriate response.17,34 A fourth limitation was that the DVQ-R did not account for some current important forms of IPV, like cyber-abuse.35 Another limitation involved the small number of sociodemographic or academic variables and variables related to students’ history of personal and family violence, as they could have conditioned the results. Although the associations we found are maintained when adjusting for the available variables, perhaps other uncontrolled variables are responsible for part of the association, particularly the students’ social and educational environment, which may be different in the three degrees.
In conclusion, the level of IPV-tolerance and sexism among the students of medicine, nursing, and psychology was high, especially in male students. Compared to medicine and nursing degrees, the frequency of students’ tolerance towards IPV and sexist attitudes was significantly higher in the psychology degree. Only medicine students underwent a hypothetical positive trend throughout their studies, female students in IPV-tolerance and male students in sexist attitudes. Designing university curricula that seek the development of egalitarian gender-role attitudes is urgently needed, with special focus on male students, as a first step in the pathway toward decreasing IPV-tolerance. Longitudinal studies are needed that follow up a group of young people from the beginning to the end of their university studies, as well as qualitative studies that examine the quantity and quality of training about violence offered by the universities and received by the students.
Health professionals play a central role in identifying and addressing intimate partner violence. University education should form professionals in order to be less tolerant towards intimate partner violence and to promote egalitarian gender attitudes.
What does this study add to the literature?Tolerance towards intimate partner violence and sexist attitudes were high among students of health sciences in Spain, especially in male students and in the degree of psychology. Throughout academic courses, tolerance towards intimate partner violence and sexist attitudes only improved in medicine female and male students, respectively. These indicators did not significantly change among psychology and nursing students.
Miguel Ángel Negrín Hernández.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsF.J. Rodríguez-Díaz and A. Lana designed the study. V. García-Díaz and A. Fernández-Feito collected the data. A. Fernández-Feito and C. Bringas-Molleda performed the statistical analyses. V. García-Díaz and A. Lana drafted the first version of the manuscript. Lastly, all authors contributed to the critical revision of the paper and approved the final manuscript for publication. All authors have agreed to be accountable for all aspects of the study.
FundingThe study was supported by grants from the Ministerio de Sanidad, Servicios Sociales e Igualdad of Spain (Project SUBINMU012/009) and from the Universidad de Oviedo/Consejería de Educación, Cultura y Deporte del Principado de Asturias (Project UO-15- INVES-32).
Conflicts of interestNone.












