



To analyze the political agenda on diabetes in Spain under democracy by considering the frequency and content of initiatives in the Spanish parliament.
MethodsA systematic search of parliamentary interventions (1979-2010) reported on the Spanish Congress of Deputies’ web page was carried out using the key word “diabetes”. A descriptive study of the frequency of interventions was performed, followed by a content analysis, according to the priorities of the World Health Organization (WHO), the International Diabetes Federation and the Spanish Diabetes Federation. Other study variables were the year of presentation, legislature, type of initiative and whether a political decision was taken (yes/no).
ResultsThere were 59 interventions: 22% were related to the first international initiatives and 44.1% took place in the last two legislatures in response to the WHO's program Diabetes Action Now. A total of 32.2% of the initiatives addressed educational and social programs, while 23.7% addressed access to resources and health services. Most initiatives (74.6%) consisted of parliamentary questions to the government, which only required a response. Of the 15 initiatives requiring a decision to be taken, only eight were approved.
ConclusionsSpanish legislators aim to comply with international standards. Nevertheless, political decision-making has sometimes been slow. Importantly, most of the political responsibilities related to health have been transferred to the autonomous regions. The updated National Diabetes Strategy in Spain will need to strengthen public health policies according to established international priorities. Monitoring parliamentary interventions has proven to be a valid tool for evaluating patterns of political debate and decisions on diabetes.
Analizar la agenda política sobre diabetes en el periodo democrático español, considerando la frecuencia y el contenido de las iniciativas parlamentarias.
MétodosBúsqueda sistemática de las iniciativas parlamentarias (1979-2010) en la página web del Congreso de los Diputados, usando la palabra clave «diabetes». Estudio descriptivo de la frecuencia de las iniciativas, y análisis de contenido, según las prioridades de la Organización Mundial de la Salud (OMS), la Federación Internacional de Diabetes y la Federación Española de Diabetes. Otras variables: año de presentación, legislatura, tipo de iniciativa y decisión política (sí/no).
ResultadosHubo 59 iniciativas, el 22% relacionadas con las primeras internacionales y un 44,1% las dos últimas legislaturas como respuesta al programa Diabetes Action Now de la OMS. Un 32,2% estuvieron relacionadas con programas sociales y educativos, y un 23,7% con recursos y acceso a los servicios de salud. La mayoría (74,6%) fueron preguntas de control al gobierno, que sólo requieren respuesta y no aprobación/desaprobación. De las 15 iniciativas que requerían decisión, ocho fueron aprobadas.
ConclusionesLos legisladores españoles han tenido en cuenta los estándares internacionales. Sin embargo, la toma de decisiones a veces ha sido lenta, aunque es importante tener en cuenta que la mayoría de las responsabilidades políticas relacionadas con la salud están transferidas a las comunidades autónomas. Las estrategias nacionales sobre diabetes requieren fortalecer las políticas en salud pública considerando las prioridades internacionales sobre el tema. Monitorizar las iniciativas parlamentarias es una herramienta para evaluar el debate político y las decisiones tomadas sobre la diabetes.
Minimizing the gap between scientific knowledge of diabetes and applying such knowledge to modify individual risk behavior and social patterns concerning diabetes continues to pose a challenge to public health at the beginning of the 21st century, since achieving these goals depends on measures that must be implemented through decision-making.1
In addition to the disabilities resulting from its complications, diabetes causes considerable economic costs in secondary and tertiary healthcare in poorer countries, while it mainly affects the most disadvantaged population groups in richer countries.2,3 In Spain, the Di@bet.es Study found that the overall, age- and sex-adjusted prevalence of diabetes mellitus was 13.8% (95% confidence interval [95%CI]: 12.8%-14.7%), of which about half had unknown diabetes: 6.0% (95%CI: 5.4%-6.7%).4
A worldwide increase in the prevalence of diabetes has highlighted the importance of calls from various international institutions, such as the World Health Organization (WHO) and other bodies concerned with diabetes, for the need to create or update diabetes prevention programs and healthcare and to improve the quality of life of affected individuals.5–8 This task requires a determined effort as regards governmental policies and investment, in addition to efforts by health professionals. Thus, political decisions could exert an influence through direct courses of action, such as assigning resources to strengthen prevention and care strategies within the health services, and indirect action, such as public awareness campaigns to promote a healthy diet, as well as policies designed to encourage physical activity.In the case of the European Union, a report by the European Federation of Nurses on Diabetes/International Federation of Diabetes-Europe (2008) indicated that healthcare for people with diabetes remains far from ideal.9 Only half of the member states have national diabetes plans and, furthermore, most of the countries that do have such a plan have yet to implement it fully.10 In Spain, the National Diabetes Plan was approved in 1991, but was judged insufficient by those in the scientific community and the health system.11,12 Rising diabetes figures show that the plan failed, as most of the actions envisaged were never implemented effectively. As a result, the Spanish national health system approved a Diabetes Strategy in 2006.6 In addition, some autonomous regions in Spain also have their own respective diabetes healthcare plans13–15 or diabetes is included within the general healthcare plan.16–20 These documents detail the epidemic magnitude of the disease and the implications for public health in Spain and the Spanish regions, as well as the needs of the population and courses of action to control the disease.13–20The Cortes Generales (Congress and Senate) constitute one of the main sources of information for identifying health-related priorities in the political agenda and discerning whether these coincide with the specific needs of patients with diabetes. This source is one of the approaches used in political epidemiology studies, which focus on how institutions derived from political power can affect health.21 Proposals concerning the scope of public healthcare are made by parliamentary groups, which wield legislative power, approve budgets and monitor governmental actions.22 This methodology has already been used on previous occasions to analyze other important public health issues.23–26
A decade after the Spanish transition to democracy, the Saint Vincent Declaration was signed,6 provoking political debate within and beyond the Spanish parliament. The present study aimed to analyze the political agenda concerning diabetes in democratic Spain (1979-2010) as reflected in the frequency and discourse of Spanish parliamentary debates on the subject.
MethodsWe conducted a systematic search of the Congress of Deputies’ database (available at: http://www.congreso.es), for 1979-2010. This database contains information on parliamentary interventions and the daily proceedings of Deputies and Senate sessions.27 The search strategy included the use of the keyword “diabetes” in free text format. We classified the data collected according to Spanish Congress Regulations27,28 and classified the initiatives into the following categories: 1) legislative initiatives; 2) policy-oriented initiatives (non-legislative proposals); 3) government accountability initiatives (parliamentary questions to the government, interpellations and requests for information).
The content of initiatives was analyzed and the initiatives were classified in accordance with the conclusions of the Second National Congress of the Spanish Diabetes Federation in 200628 and the observations made by the WHO in its Diabetes Action Now program.29 The issues studied were the following: 1) social programs: strategies involving educational, health promotion and disease prevention programs; 2) access to resources and healthcare services: determinants, barriers and conditioning factors affecting the profile of use and access to primary and specialist healthcare services for patients with diabetes; 3) multisectoral and national diabetes plans and strategies; 4) calls for clinical and epidemiological research into the causes, symptoms and consequences of diabetes; 5) promotion/prevention strategies for childhood; 6) economic issues related to budgets and funding of diabetes programs; 7) foot care in diabetes.
SPSS software enabled us to perform a sweep of the text content of initiatives on diabetes. We carried out a descriptive study of the frequencies of these issues. To conduct an internal validation of the content of the initiatives as measurement tools and to ensure a common meaning, the research team produced operative definitions for each thematic issue. Subsequently, we calculated the level of inter-observer agreement (authors AA and JCR) by means of the concordance index and obtained a high level of agreement (82%).
We also analyzed issues identified in the initiatives according to: 1) year of presentation and legislature; 2) the parliamentary group promoting the intervention: Partido Socialista Obrero Español (PSOE, Spanish Socialist Workers’ Party), Partido Popular (PP, Popular Party), Convergència i Unió (CIU, Convergence and Union), Grupo Parlamentario Mixto (Mixed Group) and Izquierda Unida (IU, United Left), others; 3) the parliamentary group in government at the time of the intervention: PSOE/PP; 4) the decisions made on policy initiatives: approved/not approved; and 5) where the initiative was debated (in Special Commissions or in parliament). Legislative and non-legislative proposals need approval while the government accountability initiatives (parliamentary questions to the government, interpellations and requests for information) need only a government reply (with or without debate).
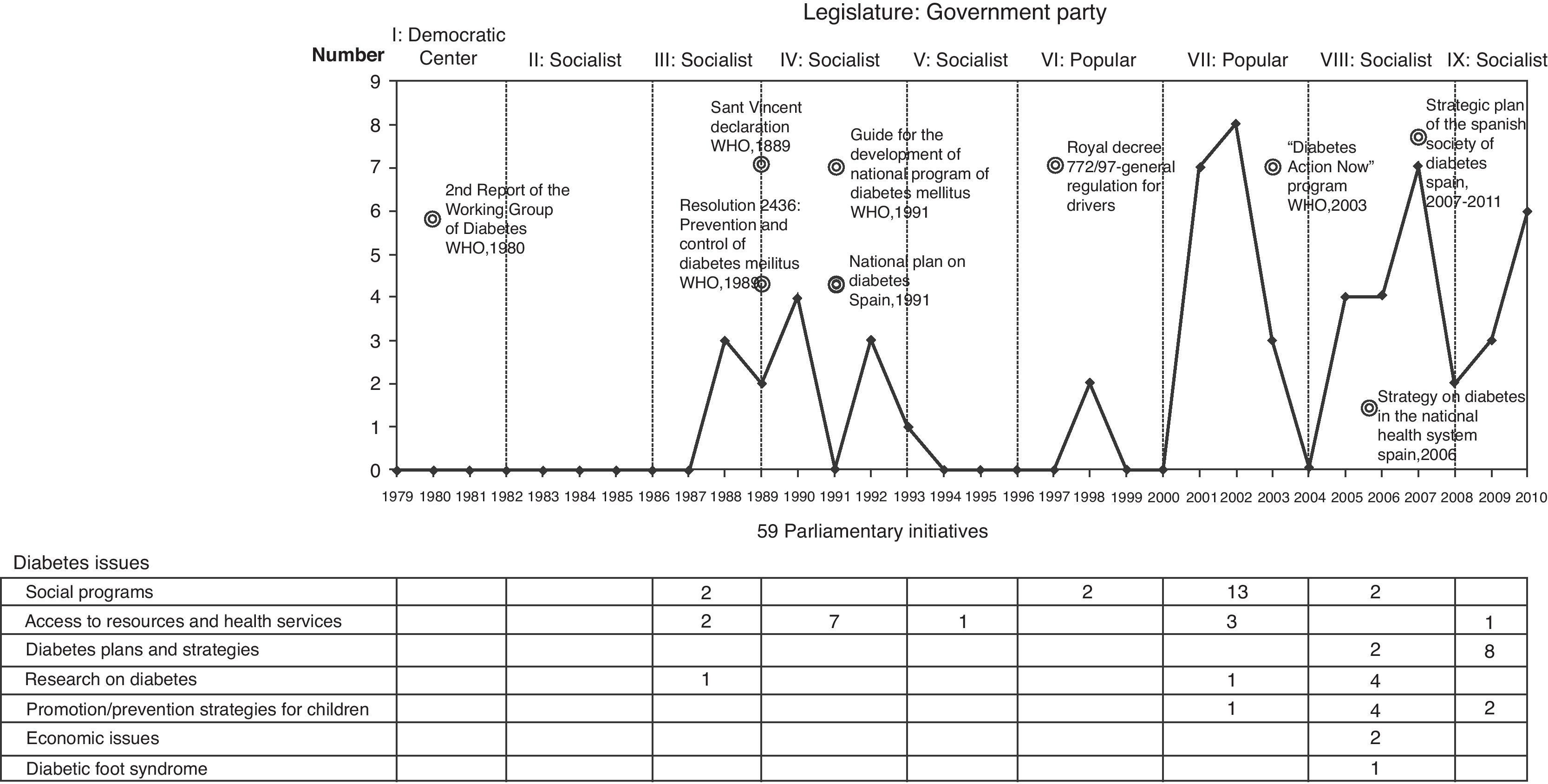
ResultsThe history of diabetes in the parliamentary agenda is shown in figure 1. The first two of the 59 parliamentary initiatives were questions to the Socialist government during the third legislature (1988). Specifically, the Popular Party asked questions about “Discrimination against people with diabetes in employment contracts” and “The number of people diagnosed with diabetes and in treatment in Spain”. Out of these 59 initiatives, 43 (72.8%) were presented during the 7th, 8th and 9th legislatures (2001, 2002 and 2007). A total of 74.6% (n = 44) of initiatives consisted to questions to the government, interpellations and requests for information and the remaining 15 corresponded to non-legislative proposals. Of the latter, 53.3% (n = 8) were approved, with or without modifications.

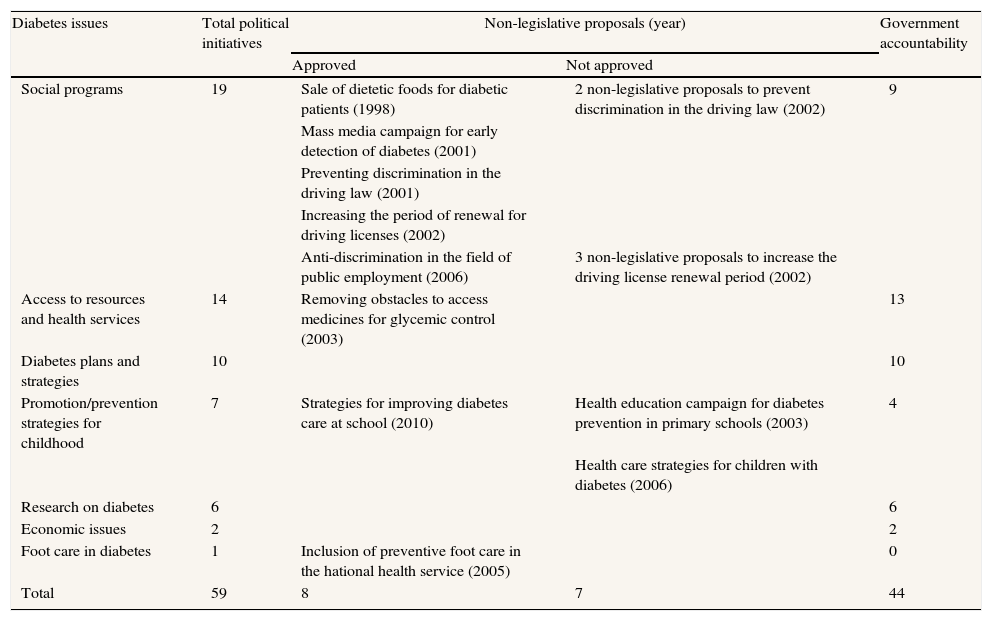
The issues addressed in the political agenda were mostly of a social and educational nature (32.2%, n = 19). Of these 19 initiatives, 10 were non-legislative proposals, of which five were approved. The second most debated issue was that of access to resources and healthcare services (23.7%, n = 14). Of these 14 initiatives, only one was a non-legislative proposal and was approved. Issues receiving less attention included seven initiatives about promotion/prevention strategies aimed at children, three were non-legislative proposals, and only one was approved in 2010. A further 10.2% (six initiatives-parliamentary questions to government) addressed research on diabetes. Economic issues were the subject of two parliamentary questions to government, and on one occasion foot care in diabetes was debated in connection with a non-legislative proposal, which was approved (table 1).
Diabetes agenda of the Spanish parliament, 1979-2010: priority issuesa
| Diabetes issues | Total political initiatives | Non-legislative proposals (year) | Government accountability | |
| Approved | Not approved | |||
| Social programs | 19 | Sale of dietetic foods for diabetic patients (1998) | 2 non-legislative proposals to prevent discrimination in the driving law (2002) | 9 |
| Mass media campaign for early detection of diabetes (2001) | ||||
| Preventing discrimination in the driving law (2001) | ||||
| Increasing the period of renewal for driving licenses (2002) | ||||
| Anti-discrimination in the field of public employment (2006) | 3 non-legislative proposals to increase the driving license renewal period (2002) | |||
| Access to resources and health services | 14 | Removing obstacles to access medicines for glycemic control (2003) | 13 | |
| Diabetes plans and strategies | 10 | 10 | ||
| Promotion/prevention strategies for childhood | 7 | Strategies for improving diabetes care at school (2010) | Health education campaign for diabetes prevention in primary schools (2003) | 4 |
| Health care strategies for children with diabetes (2006) | ||||
| Research on diabetes | 6 | 6 | ||
| Economic issues | 2 | 2 | ||
| Foot care in diabetes | 1 | Inclusion of preventive foot care in the hational health service (2005) | 0 | |
| Total | 59 | 8 | 7 | 44 |
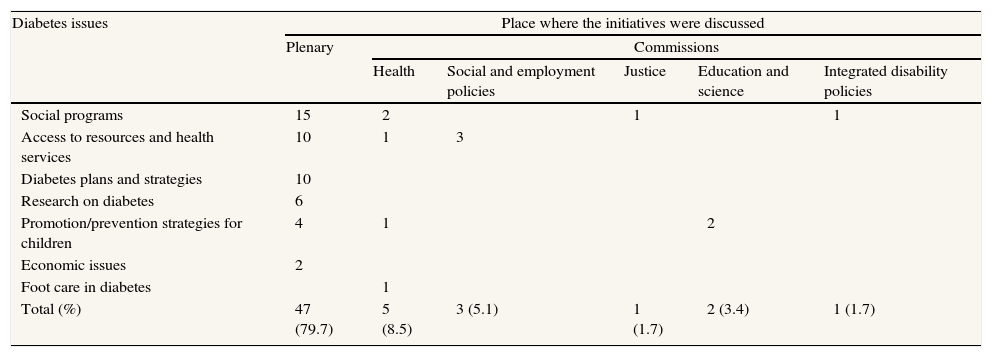
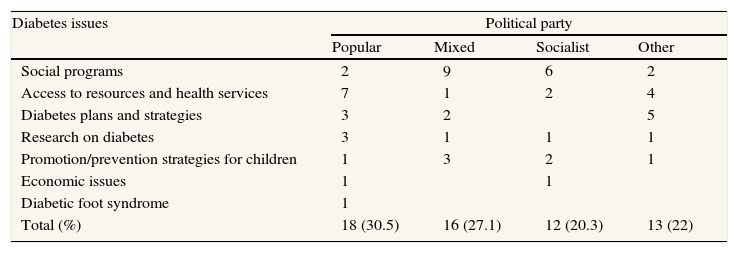
Tables 2 and 3 show diabetes priorities according to the political party that promoted parliamentary initiatives and the Organ of Congress that debated these issues. A total of 79.7% (n = 47) were discussed in plenary and 8.5% (n = 5) in the Commission for Health. Of these initiatives, 30.5% (n = 18) were promoted by the Popular Party, 27.1% (n = 16) by the Mixed Group and 20.3% (n = 12) by the Spanish Socialist Workers’ Party.
Priorities related to diabetes according to the organ of Congress that debated the initiatives (1979-2010)
| Diabetes issues | Place where the initiatives were discussed | |||||
| Plenary | Commissions | |||||
| Health | Social and employment policies | Justice | Education and science | Integrated disability policies | ||
| Social programs | 15 | 2 | 1 | 1 | ||
| Access to resources and health services | 10 | 1 | 3 | |||
| Diabetes plans and strategies | 10 | |||||
| Research on diabetes | 6 | |||||
| Promotion/prevention strategies for children | 4 | 1 | 2 | |||
| Economic issues | 2 | |||||
| Foot care in diabetes | 1 | |||||
| Total (%) | 47 (79.7) | 5 (8.5) | 3 (5.1) | 1 (1.7) | 2 (3.4) | 1 (1.7) |
Priorities related to diabetes according to the political party that promoted the parliamentary interventions (1979-2010)
| Diabetes issues | Political party | |||
| Popular | Mixed | Socialist | Other | |
| Social programs | 2 | 9 | 6 | 2 |
| Access to resources and health services | 7 | 1 | 2 | 4 |
| Diabetes plans and strategies | 3 | 2 | 5 | |
| Research on diabetes | 3 | 1 | 1 | 1 |
| Promotion/prevention strategies for children | 1 | 3 | 2 | 1 |
| Economic issues | 1 | 1 | ||
| Diabetic foot syndrome | 1 | |||
| Total (%) | 18 (30.5) | 16 (27.1) | 12 (20.3) | 13 (22) |
It was during the 6th legislature (1996-2000) that the first non-legislative proposal, proposed by the Socialist party, was approved, under the Popular Party government. This was a non-legislative proposal made in 1998, drawn up by the Commission for Health and Consumers, concerning “sale of dietetic products for people with diabetes”.
During the 7th legislature, also under the Popular Party government, the Cortes Generales passed four non-legislative proposals. Two were presented by the Socialist party, as a result of the work of the Commission for Health and Consumers: the proposal of 2001 dealt with “The implementation of an information campaign to facilitate early detection of diabetes” whilst that of 2003 was related to “The elimination of bureaucratic obstacles to access to medication and glycemic control measures in people with chronic diabetes”, this latter being the only non-legislative proposal to address the issue of access to resources and healthcare services. Importantly, in the context of this concern for patients, a question was put to the government during the same legislature concerning “Acceptance shown by patients with diabetes as regards changes in the concentration contained in insulin phials and syringes”.
One of the most debated issues in Parliament during the 7th legislature was that of modifications to the General Regulation for Drivers. Proposed by the Mixed Parliamentary Group on the basis of the work of the Commission for Justice and the Interior, the non-legislative proposal on “The elimination of discriminatory treatment suffered by people with diabetes as regards the General Regulation for Drivers” was approved in 2001. Subsequently, the five non-legislative proposals debated in the plenary in 2002 on this subject were not approved. Nevertheless, one last non-legislative proposal proposed by various parliamentary groups, specifically addressed “An extension of the compulsory driving license renewal period for people with diabetes” and, following debate in plenary, was approved in 2002.
During the 8th legislature, governed by the Socialist Party, two non-legislative proposals were passed, one presented by the Popular Party and the other by the government's own party. The first proposal, drawn up by the Commission for Health and Consumers and passed in 2005, concerned “The inclusion in the list of services provided by the National Health Service of preventive foot care for people with diabetes mellitus”. The second, passed in 2006 and drawn up by the Working Commission for Integrated Disability Policies focused on “Preventing diabetes from being a cause for exclusion from access to public employment”.
The first two non-legislative proposals aimed at children during the 7th and 8th legislatures were not approved. In 2003, based on work by the Commission for Health and Consumers, the Socialist party presented an initiative aimed at introducing an “Information campaign in schools on diabetes mellitus” which was not approved, and in 2006, the proposal presented by the Popular Party in the plenary on “Healthcare for children with diabetes” was not passed either. However, in 2010 (9th legislature), based on work by the Commission for Education and Science, the Socialist party presented a non-legislative proposal to “Improve the specific nutrition of diabetic and allergic children at school”, which was approved.
Six questions on clinical and epidemiological research were presented to the government. Three of these were requests for information about the magnitude and causes of diabetes in Spain and, in particular, about the causes and consequences in specific groups, such as women. These questions were presented in the 3rd, 7th and 8th legislatures, respectively. Three questions were put during the 8th legislature on government plans for the creation of centers of reference for the study of diabetes and the creation of diabetes-specific networks.
DiscussionMonitoring parliamentary initiatives has proven to be a valid and widely used tool for evaluating patterns of political debate.22,25 Our findings indicate that diabetes has been on the Spanish parliamentary agenda since the end of the 1980s. As international programs and recommendations emerged, initiatives in the Cortes Generales increased. For example, support was given to educational and social programs on diabetes, initiatives aimed at the employment rights, transportation and nutritional needs of the population with diabetes, and initiatives on the availability of resources and access to healthcare services for people with diabetes.
Policy-makers carry out their work within the context of a wide range of problems and demands for resources, which must be addressed. It may be for this reason that the number of interventions in Spanish parliament has been relatively low (n = 59), even though diabetes is a prevalent disease with a high social cost, both of which are powerful motives for political action. This is particularly true when compared with the frequency of initiatives on other public health problems, such as the 569 initiatives on gender violence debated between 1979 and 2004,24 or the 299 initiatives on abortion.26 However, questions on abortion or on violence also involve other issues concerning justice, safety, etc., which should be taken into account when making this comparison. Diabetes is more present on the parliamentary agenda than obesity, for example, a serious public health problem which only elicited 20 interventions between 1979 and 2007.25
The increasing frequency of debate on diabetes has coincided with an increase in the prevalence of the disease both in Spain and elsewhere.2,4,8 The trend toward an increase in initiatives after 2002 is related to the announcement of strategies in Spain such as the national health system's diabetes strategy in 20066 and the Spanish Diabetes Society's Strategic Plan for 2007-2011.30 Spanish legislators aim to comply with international standards. Most initiatives on diabetes were related to monitoring government actions.
The first initiative on diabetes in the Cortes Generales of Spain occurred in 1988, and consisted of a parliamentary question to the government about employment discrimination against people with diabetes. Although the seriousness and morbidity of hypoglycemia, which can occur in the workplace among people being treated with insulin for diabetes, should not restrict their employment possibilities,31 people with diabetes do perceive discrimination.32 Specifically, a relationship has been reported between discrimination events in the workplace and the frequency of episodes of hypoglycemia.32 The same would appear to be the case with the complications of chronic diabetes. Furthermore, an association has been observed between the act of informing a potential employer of diabetes during a job interview and an increase in employment discrimination.32 According to European legislation, not contracting an individual because of a potential drop in productivity due to diabetes is considered discrimination. Discrimination on the basis of health is a source of social exclusion and of economic costs which must be met by social security systems. In the European Union, traditional social security laws are being supplemented by strong anti-discriminatory measures concerning occupation and employment. It is probably for this reason that, years after the first question was posed to the government about employment discrimination and following various related initiatives, one of these initiates was approved in Spain in 2006 to prevent diabetes from being a cause for exclusion from access to public employment.
The results of previous and recent research on the relationship between driving and diabetes have been contradictory. Some researchers have observed a slight increase in the risk of accidents among drivers with diabetes, others a greater risk among specific subgroups, whilst still others have observed no increase in risk.33 Nevertheless, the European Union directive 91/439 establishes that people on insulin for diabetes cannot drive trucks, heavy goods vehicles or buses, with the exception, in special cases, of small trucks.34 This directive is applied differently by the different European Union member states35. In Spain, various parliamentary groups joined forces at the beginning of the first decade of the 21st century to propose changes to Royal Decree 772/97 on transport in order to address the discrimination experienced by people with diabetes as a result of being obliged to renew their driving licenses every 6 or 12 months according to the course of their disease.36
Diabetes is not distributed randomly among the population. The groups most at risk for this disease are those living in conditions of poverty and material deprivation.37 Equally, control of the disease is not equal for all members of the population. Gender, socioeconomic level and ethnic group are all associated with the disease, reflecting the uneven effectiveness of health resources and care.37 Consequently, parliamentary initiatives on access to resources and healthcare services are of particular importance. The 2006 Spanish Diabetes Strategy requires multidisciplinary political decision-making in order to direct economic and political resources toward some of the international priorities that remain unaddressed.
Interpretation of these results should take into account the study's limitations. Forty-four of the initiatives focused on government accountability initiatives and did not need political approval (only a government response), hampering deeper content analysis of some aspects, since we could not follow up the government responses and other political debates.
The political debate on diabetes in Spain does not end in the Cortes Generales since the political action related to health is also carried out in the 17 autonomous parliaments of the autonomous regions in Spain. Most of these autonomous regions have plans for diabetes prevention and control, either specific or integrated in strategies on non-communicable diseases. Thus, this study should be complemented by an analysis of these plans and strategies and the parliamentary debates in the autonomous regions. Future research should also include a thematic content analysis of the treatment of diabetes in the media.
Recent legislatures have demonstrated political interest in research and the creation of diabetes research centers, as well as in epidemiological monitoring, within a context of global trends in this disease and its risk factors and in related diseases such as obesity. Such a scenario calls for the generation of more and better scientific knowledge of diabetes, taking a more integrated approach such as that proposed by the WHO Commission on Social Determinants of Health.38 The aim of such an approach is to develop integrated courses of action, by identifying and providing information on groups at risk and establishing effective coordination between healthcare and scientific knowledge to develop more efficient prevention strategies.
Parliament is one of the main sources of information when identifying health-related priorities on the political agenda and discerning whether these coincide with the specific needs of patients with diabetes.
What does this paper add to the literature?Monitoring parliamentary initiatives is a valid and widely used tool for evaluating patterns of political debate and decisions on diabetes, as shown by political epidemiology studies. Our findings indicate that diabetes has been on the Spanish parliamentary agenda since the end of the 1980s. However, there is evidence of slow political decision-making because the first parliamentary initiative was not approved until 2006 and most of the debates on diabetes are government accountability initiatives and do not need to be approved.
All the authors contributed to data analysis and drafting of the manuscript and approved the final version submitted to the journal.
FundingNone.
Conflict of de interestsNone.











