



We assessed prevalence of suicidal ideation and plans among illicit drug users and their association with contextual factors, by gender.
MethodsCross-sectional study. In a sample of 511 illicit drug users recruited during spring 2012 in drug treatment and prevention facilities in Catalonia (Spain), the prevalence of suicidal ideation/plans in the last 12 months was assessed. Poisson regression was used to examine associations between suicidal ideation/plans and various factors (socio-demographic, psychological, illegal drug market activities and marginal income generation activities, which included any reported sex work, stealing, peddling, begging or borrowing on credit from a dealer).
ResultsThe average age was 37.9 years (standard deviation: 8.62); 76.3% were men. Suicidal ideation/plans were reported by 30.8% of men and 38.8% of women, with no significant differences by age or gender. Recent aggression (male prevalence ratio [PR]=2.2; female PR=1.4), psychological treatment (male PR=1.2; female PR=1.3) and illegal/marginal income generation activities (male PR=1.5; female PR=1.1) were associated with suicidal ideation/plans. Men who trafficked were more likely to have suicidal ideation/plans (PR=1.3), while prison history was positive for women (PR=1.8) and negative for men (PR=0.7).
ConclusionsPrevalence of suicidal ideation/plans was high among illicit drug users recruited from healthcare facilities. Besides psychological variables, participation in illegal market activities and crime ought to be considered in drug users’ suicidal prevention. Suicide risk needs to be evaluated in drug treatment facilities and psychological status and context contemplated.
Se evaluó la prevalencia de ideación y de planes suicidas entre los/las consumidores/as de drogas ilícitas y su asociación con factores contextuales, por sexo.
MétodosEstudio transversal. En una muestra de 511 consumidores/as de drogas ilícitas, reclutados/as durante la primavera de 2012 en centros de tratamiento y preventivos de Cataluña, se evaluó la presencia de ideación o plan suicida en los últimos 12 meses. Se utilizó una regresión de Poisson para examinar las asociaciones entre la ideación o el plan suicida y diversos factores (sociodemográficos, psicológicos, mercado de drogas y actividades marginales de generación de ingresos, considerándose trabajo sexual, robo, venta ambulante, mendicidad o endeudamiento con un traficante).
ResultadosLa edad media fue de 37,9 años (desviación estándar: 8,62). El 76,3% eran hombres. El 30,8% de los hombres y el 38,8% de las mujeres reportaron ideación o plan suicida, sin diferencias significativas por sexo y edad. La agresión reciente (razón de prevalencia [PR] hombres=2,2, PR mujeres=1,4), el tratamiento psicológico (PR hombres=1,2, PR mujeres=1,3) y las actividades ilegales o marginales de generación de ingresos (PR hombres=1,5, PR mujeres=1,1) se asociaron a la ideación o plan suicida. Los hombres que traficaban eran más propensos a tener ideación o plan suicida (PR=1,3), mientras que la prisión lo fue positivamente para las mujeres (RP=1,8) y negativamente para los hombres (PR=0,7).
DiscusiónLa prevalencia de ideación o plan suicida fue alta entre los/las consumidores/as de drogas ilícitas reclutados/as en centros sanitarios. El estado psicológico, la participación en actividades de mercado y el crimen deben considerarse especialmente para la prevención del suicidio. El riesgo de suicidio debe ser evaluado en los centros de tratamiento de drogas, contemplando el estado psicológico y el contexto.
Each year more than 800,000 people die by suicide worldwide,1 representing 15% of the 15,000 fatal injuries occurring daily. In some countries, suicide is among the leading causes of death among the young; in fact, amongst those aged 15-29 years it is the second cause after road traffic injuries.1 Although Spain has one of the lowest suicide death rates in Europe, a total of 3,158 deaths were attributed to suicides in 2010.2 Furthermore suicide data could be underestimated as deaths or injuries may not be clearly identified as intentional. Suicidal behavior occurs along a continuum progressing from negative thoughts or ideations, plans, non-fatal suicide, and finally fatal suicide. Prevalence of suicidal ideations, thoughts and plans are more difficult to estimate than fatal suicides. Non-fatal suicidal behaviors are several times more frequent than fatal suicides (10, or more times) and they are among the most powerful predictors of subsequent suicide deaths.3 Prevalence of suicidal behaviors differs by sex: pessimistic thoughts and ideations are more frequent among women and men carry out more fatal suicides, rates being reported to be three times higher than in females.4
Suicidal behavior is a multifaceted problem for which presence of mental disorders increases risk.5 A majority of suicidal victims (more than 90%), have a diagnosable chronic mental disorder. The most prevalent psychiatric disorders in suicide deaths among the general population were depression, mood disorders, schizophrenia, and substance abuse.6 Previous studies have reported its association with substance use: one study found a five-fold increase in risk of suicide among alcohol abusers compared to social drinkers.7 Use of other psychoactive substances like heroin, cocaine and sedatives has also been linked to fatal suicides.8 The consumption of more than two substances has been linked to greater likelihood of both fatal and non-fatal suicidal behavior.9
Additionally, several studies have shown traumatic experiences were associated with greater suicide risk, developing thoughts of suicide and to plan attempts.5,10 The context of illegal drug use favours exposure to traumatic events.11,12 In fact, in the conceptual framework to explain the relationship between drug use and violence, one of the models introduced by Goldstein refers to systemic crime derived from illicit drug distribution and use.13 Ilgen's study went beyond the Goldstein model showing that illicit drug users in treatment with prior violent behaviour were more likely to report suicide attempts.14
The purpose of this study was to assess, separately by sex, the prevalence of suicidal ideations and plans among illicit drug users recruited in drug treatment facilities and its association with drug-scene contextual factors, including recent violent trauma experience and crime involvement.
MethodStudy design and sampleCross-sectional study of illicit drug users recruited in treatment and prevention centers in Catalonia between April and June 2012. From the list of current public treatment facilities (2010), centers were selected to cover the whole territory. To this aim five geographical areas were considered; and sampling strategies adapted to contemplate each type of facility in a given area. As Outpatient Treatment Centers (OTC) are the main entrance door to treatment in Catalonia, they were prioritized. Finally 48 centers participated: 26 OTC, 12 Therapeutic Communities (ThC), and 10 Harm Reduction Facilities (HRF). The number of participants to be recruited was determined based on the centre's activity, over-sampling the smallest selected centres, especially HRF. In HRF quotas were applied for sex and country of birth. Ethical approval was granted by the IMIM (Hospital del Mar Medical Research Institute) ethics committee. Informed consent was obtained from participants prior to their involvement in the study; HRF clients were rewarded with 10€.
A total of 514 illicit drug users participated in the study (N approached=558; participation rate: 92.1%; reasons for rejecting were to be in a hurry, not interested, or unknown), answering an anonymized 78 item questionnaire, involving single or multiple-choice answers about socio-demographic aspects, substance use patterns, health services evaluation, crime, drug market activities, violence and suicide. The final sample for the present analyses consisted of 511 individuals for whom suicide information was available, as three men (0.6%) did not answer those questions.
VariablesThe presence of suicidal ideation/plan (IP) was assessed using two questions based on the Composite International Diagnostic Interview (CIDI)15 referring to the previous 12 months: Did you think about committing suicide? and Did you make a suicide plan? These were combined into a single variable, suicide IP, with categories ‘yes’, reflecting a positive answer to either of the two original questions, or ‘no’ to both.
Independent variables included in this study relate to socio-demographic aspects (nationality, municipality, level of education, employment and marital status); psychoactive substance use patterns (age at first illegal drug use, alcohol risk use, parenteral administration ever, opiate and cocaine use ever, recent illegal polydrug use), psychological treatment last 12 months, violent traumatic experience, illegal drug market activities (ever trafficked and income generation activities) and crime (prison ever). Alcohol risk use was assessed through the AUDIT-C referring to the last 12 months: men with a score of 4 or more and women with 3 or more were considered risk alcohol users.16 Recent illegal polydrug use was defined as the daily use of two or more illicit substances during the last 30 days of active use. Presence of any violent traumatic experience was assessed based on four questions referring to the last 12 months17: 1) How many times have you been attacked, kicked, burned etc. or injured by firearm, knife, stick, broken bottle?, 2) How many times have you received any physical aggression not involving any weapon?, 3) How many times have you been a victim of any sexual abuse? and 4) How many times have you been a victim of any psychological abuse? Answers to these questions were summarized as aggression, including any kind of violence received, either physical, whether involving a weapon or not, sexual or psychological. A variable was created reflecting income generating activities (IGA) or sources of funding for drug money, in which we distinguished between legal income generation activities (money obtained from family, partner, legal job, pension or street trade) and illegal and/or marginally legal ones (money obtained from sex work, stealing, peddling, begging, borrowing on credit from a dealer); “legal activities” was coded if no illegal and/or marginal activity was reported.
Statistical analysesSuicidal IP subjects’ characteristics were analyzed separately by sex. Basic descriptive analyses were done to characterize the study sample; chi-square and t-tests were used for comparisons. Poisson regression models with robust variance were used to identify factors associated with suicidal IP, via prevalence ratios (PR), absence of suicidal IP being the reference category. Correlated observations according to the type of recruitment center (HRF, OTC, or ThC) were taken into account through the generalized estimating equation procedure. Variables with p values less than 0.20 in the previous bivariate analyses were included in the regressions and progressively withdrawn in a backward procedure. Psychoactive substance use variables were not included in the model as subjects were under different treatment experiences and drugs would refer to different time periods. The separate models for males and females were adjusted by age and socio-demographic variables that had been found relevant in either males or females (municipality, level of education, employment status, and marital status). When in a given variable there were more than 15 missing answers, a new category was created in order to avoid losing these cases from the analysis. Potential confounders and interactions were tested. Statistical significance was set at p <0.05. All analyses were performed using SPSS version 18.
ResultsDescription of the sampleThe sample included 390 men (76.3%) and 121 women, their average age was 37.9 years overall (SD: 8.62; range: 18-71), 38.0 years (SD: 8.48) for men and 37.6 years for women (SD: 9.02). More than half of the participants came from OTC (61.8%) while HRF and ThC accounted for approximately 19.0% each. The majority of participants were Spaniards (91.0%) and half of them residents in Barcelona city and its conurbations (54.0%). Over half of both men and women were unemployed or had never worked (60.1%). The percentage of men who started illegal drug use when aged 12 years or under was 15.5% and for women it was 7.4% (p <0.05). The majority of participants had been cocaine users (93.2%), while 36.8% had used opiates and 43.5% had used parenteral route ever. Around one third of subjects were illegal polydrug users. More women reported having received psychological treatment (40.5% vs 26.6% for men, p <0.01) and no sex differences were found in recent aggressions (55.7% and 50.1% for men, p <0.31). Regarding illegal drug market activities, more men declared having ever trafficked (52.8% vs 41.3% of women, p <0.05), and having engaged in marginal IGA (84.5% of men vs 74.4% of women, p <0.05). The proportions of subjects ever sentenced to prison were 44.2% and 29.0% for men and women, respectively (p <0.01).
Suicidal ideation and planSuicidal IP was present in 30.8% of men (95% confidence interval [95%CI]: 26%-35%) and 38.8% of women (95%CI: 30%-47%), the proportion overall being 32.7% (95%CI: 28%-36%). Although higher presence of both ideation and plans was found for women, no statistically significant differences were observed. Plans were less frequent than ideation, 52.0% of people with an ideation reported plans; only two persons reported just plans; no gender differences were observed in this distribution.
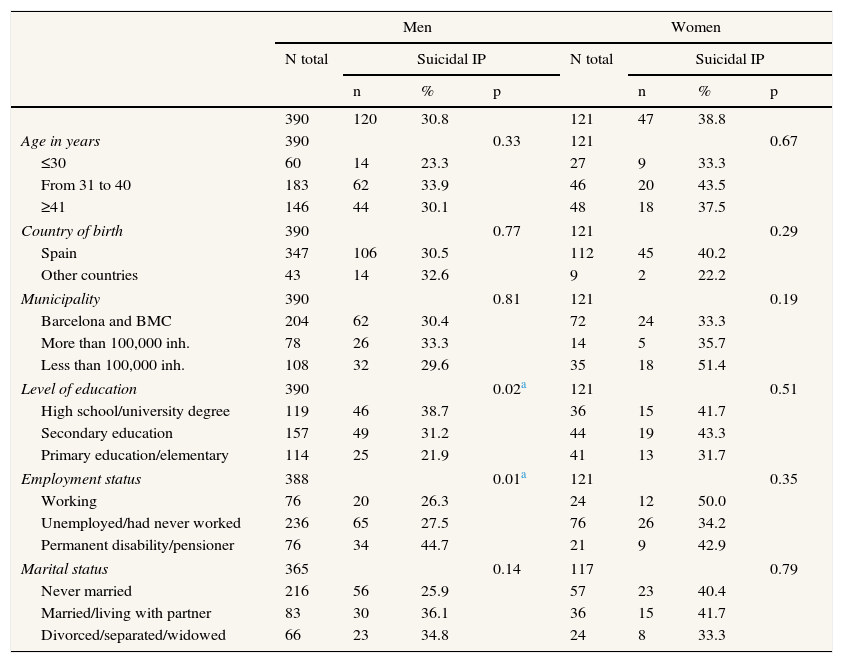
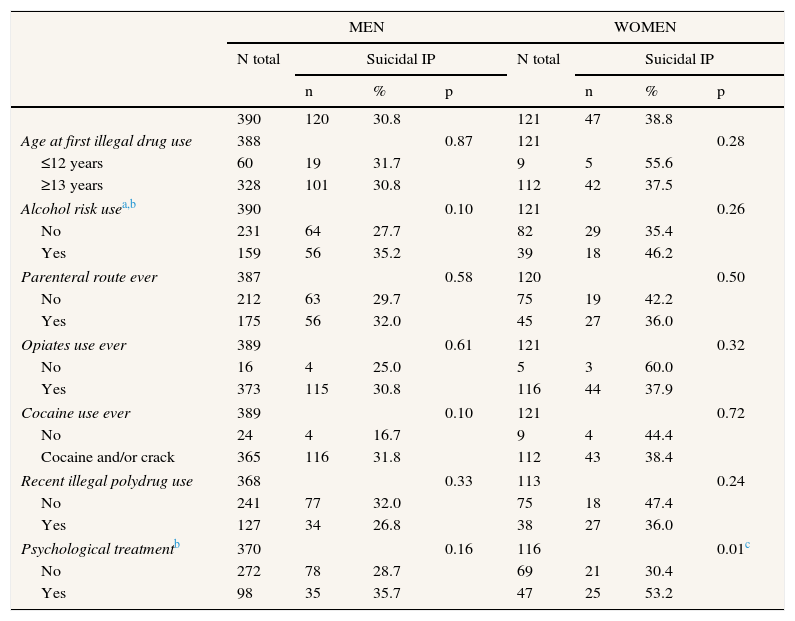
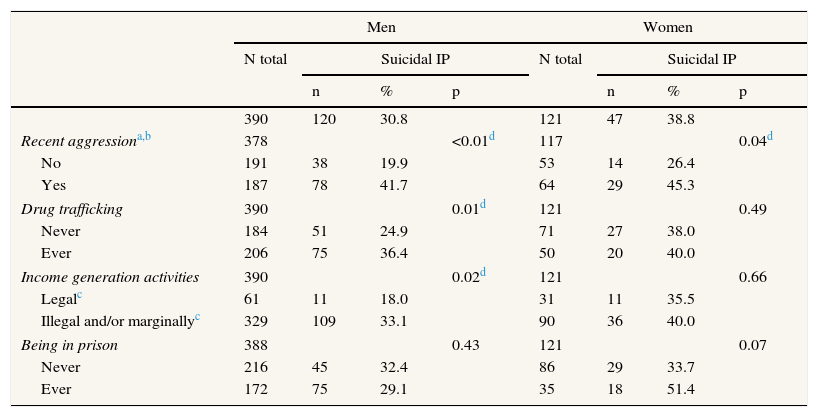
No significant differences for suicidal IP were found in the age distribution or in other sociodemographic variables in either men or women, except for level of education and employment status in men (Table 1). None of the drug use patterns analyzed showed increased risk of suicidal IP (Table 2). However, the prevalence of women reporting suicidal IP was higher among those who had been in psychological treatment in the last 12 months. The prevalence of suicidal IP was higher among both men and women reporting recent aggression (Table 3). In relation to involvement in the illegal drug market, suicidal IP was significantly more common for men who trafficked (36.5%), and those who declared marginal IGA (33.1%). Although more than half of the women with a prison history presented suicidal IP (51.4%), the association was marginally not significant.
Last 12 months suicidal ideation/plan among men and women using illegal drugs according to socio-demographic variables. Catalonia, Spain (2012).
| Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| N total | Suicidal IP | N total | Suicidal IP | |||||
| n | % | p | n | % | p | |||
| 390 | 120 | 30.8 | 121 | 47 | 38.8 | |||
| Age in years | 390 | 0.33 | 121 | 0.67 | ||||
| ≤30 | 60 | 14 | 23.3 | 27 | 9 | 33.3 | ||
| From 31 to 40 | 183 | 62 | 33.9 | 46 | 20 | 43.5 | ||
| ≥41 | 146 | 44 | 30.1 | 48 | 18 | 37.5 | ||
| Country of birth | 390 | 0.77 | 121 | 0.29 | ||||
| Spain | 347 | 106 | 30.5 | 112 | 45 | 40.2 | ||
| Other countries | 43 | 14 | 32.6 | 9 | 2 | 22.2 | ||
| Municipality | 390 | 0.81 | 121 | 0.19 | ||||
| Barcelona and BMC | 204 | 62 | 30.4 | 72 | 24 | 33.3 | ||
| More than 100,000 inh. | 78 | 26 | 33.3 | 14 | 5 | 35.7 | ||
| Less than 100,000 inh. | 108 | 32 | 29.6 | 35 | 18 | 51.4 | ||
| Level of education | 390 | 0.02a | 121 | 0.51 | ||||
| High school/university degree | 119 | 46 | 38.7 | 36 | 15 | 41.7 | ||
| Secondary education | 157 | 49 | 31.2 | 44 | 19 | 43.3 | ||
| Primary education/elementary | 114 | 25 | 21.9 | 41 | 13 | 31.7 | ||
| Employment status | 388 | 0.01a | 121 | 0.35 | ||||
| Working | 76 | 20 | 26.3 | 24 | 12 | 50.0 | ||
| Unemployed/had never worked | 236 | 65 | 27.5 | 76 | 26 | 34.2 | ||
| Permanent disability/pensioner | 76 | 34 | 44.7 | 21 | 9 | 42.9 | ||
| Marital status | 365 | 0.14 | 117 | 0.79 | ||||
| Never married | 216 | 56 | 25.9 | 57 | 23 | 40.4 | ||
| Married/living with partner | 83 | 30 | 36.1 | 36 | 15 | 41.7 | ||
| Divorced/separated/widowed | 66 | 23 | 34.8 | 24 | 8 | 33.3 | ||
BMC: Barcelona Metropolitan Conurbation; IP: ideation/plan.
Last 12 months suicidal ideation/plan among men and women using illegal drugs according to psychoactive substance use patterns. Catalonia, Spain (2012).
| MEN | WOMEN | |||||||
|---|---|---|---|---|---|---|---|---|
| N total | Suicidal IP | N total | Suicidal IP | |||||
| n | % | p | n | % | p | |||
| 390 | 120 | 30.8 | 121 | 47 | 38.8 | |||
| Age at first illegal drug use | 388 | 0.87 | 121 | 0.28 | ||||
| ≤12 years | 60 | 19 | 31.7 | 9 | 5 | 55.6 | ||
| ≥13 years | 328 | 101 | 30.8 | 112 | 42 | 37.5 | ||
| Alcohol risk usea,b | 390 | 0.10 | 121 | 0.26 | ||||
| No | 231 | 64 | 27.7 | 82 | 29 | 35.4 | ||
| Yes | 159 | 56 | 35.2 | 39 | 18 | 46.2 | ||
| Parenteral route ever | 387 | 0.58 | 120 | 0.50 | ||||
| No | 212 | 63 | 29.7 | 75 | 19 | 42.2 | ||
| Yes | 175 | 56 | 32.0 | 45 | 27 | 36.0 | ||
| Opiates use ever | 389 | 0.61 | 121 | 0.32 | ||||
| No | 16 | 4 | 25.0 | 5 | 3 | 60.0 | ||
| Yes | 373 | 115 | 30.8 | 116 | 44 | 37.9 | ||
| Cocaine use ever | 389 | 0.10 | 121 | 0.72 | ||||
| No | 24 | 4 | 16.7 | 9 | 4 | 44.4 | ||
| Cocaine and/or crack | 365 | 116 | 31.8 | 112 | 43 | 38.4 | ||
| Recent illegal polydrug use | 368 | 0.33 | 113 | 0.24 | ||||
| No | 241 | 77 | 32.0 | 75 | 18 | 47.4 | ||
| Yes | 127 | 34 | 26.8 | 38 | 27 | 36.0 | ||
| Psychological treatmentb | 370 | 0.16 | 116 | 0.01c | ||||
| No | 272 | 78 | 28.7 | 69 | 21 | 30.4 | ||
| Yes | 98 | 35 | 35.7 | 47 | 25 | 53.2 | ||
IP: ideation/plan.
Last 12 months suicidal ideation/plan among men and women using illegal drugs according to recent aggression and illegal activities. Catalonia, Spain (2012).
| Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| N total | Suicidal IP | N total | Suicidal IP | |||||
| n | % | p | n | % | p | |||
| 390 | 120 | 30.8 | 121 | 47 | 38.8 | |||
| Recent aggressiona,b | 378 | <0.01d | 117 | 0.04d | ||||
| No | 191 | 38 | 19.9 | 53 | 14 | 26.4 | ||
| Yes | 187 | 78 | 41.7 | 64 | 29 | 45.3 | ||
| Drug trafficking | 390 | 0.01d | 121 | 0.49 | ||||
| Never | 184 | 51 | 24.9 | 71 | 27 | 38.0 | ||
| Ever | 206 | 75 | 36.4 | 50 | 20 | 40.0 | ||
| Income generation activities | 390 | 0.02d | 121 | 0.66 | ||||
| Legalc | 61 | 11 | 18.0 | 31 | 11 | 35.5 | ||
| Illegal and/or marginallyc | 329 | 109 | 33.1 | 90 | 36 | 40.0 | ||
| Being in prison | 388 | 0.43 | 121 | 0.07 | ||||
| Never | 216 | 45 | 32.4 | 86 | 29 | 33.7 | ||
| Ever | 172 | 75 | 29.1 | 35 | 18 | 51.4 | ||
IP: ideation/plan.
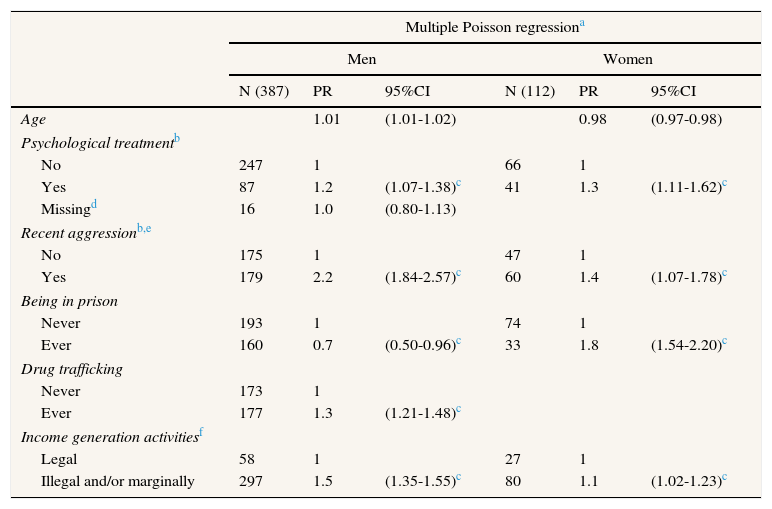
Results of the multiple Poisson regression analyses are shown in Table 4. The model for men showed that individuals who had received psychological treatment (PR=1.2), suffered recent aggression (PR=2.2), had been involved in drug trafficking (PR=1.3), and those who reported marginal IGA (PR=1.5) were more likely to have suicidal IP; while, having been in prison was protective (PR=0.7). For women, the variables associated with higher probability of suicidal IP were psychological treatment (PR=1.3), recent aggression (PR=1.4), having been in prison (PR=1.8) and marginal IGA (PR=1.1).
Multiple Poisson regression models exploring factors associated with last 12 months suicidal ideation/plan in men and women using illegal drugs. Catalonia, Spain (2012).
| Multiple Poisson regressiona | ||||||
|---|---|---|---|---|---|---|
| Men | Women | |||||
| N (387) | PR | 95%CI | N (112) | PR | 95%CI | |
| Age | 1.01 | (1.01-1.02) | 0.98 | (0.97-0.98) | ||
| Psychological treatmentb | ||||||
| No | 247 | 1 | 66 | 1 | ||
| Yes | 87 | 1.2 | (1.07-1.38)c | 41 | 1.3 | (1.11-1.62)c |
| Missingd | 16 | 1.0 | (0.80-1.13) | |||
| Recent aggressionb,e | ||||||
| No | 175 | 1 | 47 | 1 | ||
| Yes | 179 | 2.2 | (1.84-2.57)c | 60 | 1.4 | (1.07-1.78)c |
| Being in prison | ||||||
| Never | 193 | 1 | 74 | 1 | ||
| Ever | 160 | 0.7 | (0.50-0.96)c | 33 | 1.8 | (1.54-2.20)c |
| Drug trafficking | ||||||
| Never | 173 | 1 | ||||
| Ever | 177 | 1.3 | (1.21-1.48)c | |||
| Income generation activitiesf | ||||||
| Legal | 58 | 1 | 27 | 1 | ||
| Illegal and/or marginally | 297 | 1.5 | (1.35-1.55)c | 80 | 1.1 | (1.02-1.23)c |
CI: confidence interval; PR: prevalence ratio.
A high prevalence of suicidal IP was observed among illicit drug users recruited in drug treatment facilities. Prevalence among women, although slightly higher didn’t differ statistically from that among men. Recent aggression, psychological treatment and previous illegal/marginal income generation activities were positively associated with suicidal IP for both men and women, while involvement in trafficking only among men and prison history was positively associated with suicidal IP among women and negatively among men.
Some limitations need to be considered when interpreting these results. First, this study provided evidence about the presence of ideations and plans during the previous 12 months, however it did not evaluate the frequency and intensity of them, or the presence of any non-fatal suicide attempt. Second, recruitment was done among illicit drug users in health centers, thus results can at most be representative of drug users in healthcare facilities. Third, being based on self-reported data, the results could be influenced by subjects tending to give answers considered “desirable”. In any case, if there was an under declaration of suicidal IP, reported prevalence would be an underestimate. Fourth, although the study sample is considerable, we cannot exclude a lack of statistical power, which would preclude finding some significant results; this would be especially important regarding a gender analysis perspective. In fact, it was not possible to analyze in depth the association of different forms of aggression with suicide behaviors due to small figures for some of them (e.g. sexual aggression). Fifth, not having assessed presence of mental disorders in our sample is a further limitation; although psychological treatment with the same reference period as suicidal IP was assessed and could be considered as a proxy of mental disorders it might also indicate a previous non-fatal suicide problem. Finally, being a cross-sectional design, we cannot draw conclusions about the directionality of the associations.
The study included analyses of suicide IP prevalence separately by sex, as factors associated with suicidal behaviors could differ for men and women. However, we haven’t been able to go deeper with a gender perspective as the study design didn’t consider all necessary aspects to this aim, like selective recruitment to achieve a larger sample of women or to better care for gender addressing questions (e.g. violence). Nevertheless, we can contribute to the gender debate by showing controversial results in men and women, like the differential outcome in subjects with a prison history or participation in drug trafficking. Also of note is the different direction for age, as in men the likelihood of suicidal IP increased with age, while for women it decreased.
Due to sample characteristics, substances used by subjects in the study were not considered in the multivariate analyses (e.g. 93% cocaine users may preclude finding an association with this substance). Furthermore, the sample included drug users in treatment, thus some of them might not be consuming in the period considered for assessing suicide (last 12 months) due to being in therapeutic communities or in substitution treatment. Besides, although alcohol was included in the analysis as its reporting was referring to the same period of time, it was not associated with suicidal IP. This lack of association in our study contrasts with other findings18 and might be related to the fact that study subjects, being illegal drug users, may have higher suicidal risk for this than for their alcohol risk use. Actually, in the above cited revision of cohort studies,18 subjects dependent on illicit drugs had a higher risk of suicide than subjects with alcohol dependence when compared to the general population.
The 32.7% prevalence of suicidal IP in illicit drug users from drug treatment facilities was noticeably higher than in the general population. In an Italian general population study the prevalence of ideations was 3% and plans 0.7%.19 Similarly, in a USA general population study, 3.7% of subjects had serious thoughts of suicide (ideation) and 1% suicidal plans.20 Reported prevalences of suicidal ideation or plans among illicit drug users vary, and this might be related to recruitment site or substance used. In a sample of users with any substance use disorder, taken from the general population, 23.4% reported suicidal ideation and 7.9% plans,21 slightly lower than in the present study. Cocaine and heroin users recruited in the community showed a prevalence of 27% of suicidal ideations;22 while subjects who had used psychotropic drugs recruited from treatment facilities, reported a lifetime prevalence of planned suicide with ideation of about 41%.23 As in our case, no sex differences in suicidal ideations were found in the study by Havens et al.22 while Darke and Ross24 found sex differences among patients in methadone treatment, females reporting more suicide attempts than males.
As in previous studies men in the sample were more active in illegal drug market activities than women.25,26 Additionally, men engaging in drug trafficking were more likely to have suicidal IP, which was not the case for women. Even though a considerable number of women reported drug trafficking, and in a context of illegal drug consumption drug trafficking and illegal/marginal IGA are closely related, only being involved in marginal IGA was independently associated with suicidal IP for both sexes. In contrast, having been in prison was positively associated with suicidal IP only in women, while for men it was the opposite. This finding among women would be in accordance with the fact that prisoners have higher rates of suicidal behaviors than the general population,26 and that women recently released from prison were 36 times more likely to die by suicide within one year of their release.27
Violent aggressive events usually become a traumatic experience28 because the physical and psychological impact of violence to the victim can be devastating.29 Several studies have shown that drug use-related violence was highly prevalent among drug users.20,30 Crime and violence are frequent in an illegal drug market environment, and they have been associated with suicidal behavior among substance users.14 Accordingly, in our study, having suffered recent violent traumatic experiences as a result of physical, psychological and/or sexual aggression, in the same period as suicidal IP, was identified as a clear risk factor for suicidal IP proneness for both sexes. Other studies which have assessed similar traumatic experiences over different periods, such as childhood or lifetime, reported similar results globally, also among drug users in treatment.23 Also Rossow and Lauritzen31 reported an elevated prevalence of suicidal behavior and ideation among drug addicts (42% in the previous month), which increased with the number of areas of childhood adversities.
Suicidal IP prevalence among illicit drug users in drug treatment facilities in our study is within the range of prevalences found among subjects with mental disorders. O’Neill et al.21 found a prevalence of suicidal ideations in subjects with mood disorders of 30.2% while for anxiety it was 25.6%. Even though effectiveness of suicide preventive interventions is difficult to assess due to the complexity of the phenomenon32,33 its higher prevalence among patients with psychiatric disorders is well accepted.34 Accordingly, clinical depression guidelines recommend assessing suicide risk in patients with depression.35 However, although clinical guidelines for suicide identify alcohol consumption and consumption of some other drugs as risk factors, in general, they don’t address treatment or specific programs for drug users. In fact, some of these guidelines do not include any substance use disorder, or even alcohol on their screening list. In our understanding, protocols should include assessing suicide risk in drug users to provide adequate treatment. Thus, this would not only be a matter of mental health centers but also of drug treatment centers.
The study provides evidence that the prevalence of suicidal IP among illicit drug users is high, especially among both men and women reporting recent violent traumatic experiences, being involved in marginal income generation activities and having been in psychological treatment. It also suggests the need, independently of the illegal substance taken, for suicide risk to be assessed in drug treatment centers in order to detect and prevent suicidal behaviors. Subjects with previous involvement in illegal drug market activities and crime deserve special attention. Effective suicide prevention strategies should be addressed to illicit drug users in treatment.
Suicide is a great contributor to morbidity and mortality of drug users. Mental disorders, history of trauma, previous suicide attempt and stressful events are factors associated to it. There are knowledge gaps on associations of suicide behaviors with drug-scene contextual factors, drug market and crime.
What does this study add to the literature?One third of illicit drug users reported suicidal ideation and/or plans, without sex differences. Recent aggression and marginal income generation activities were associated with them. Suicide risk behavior ought to be assessed in drug treatment facilities in order to detect it and allow implementation of effective suicide prevention strategies.
María Teresa Ruiz Cantero.
Authorship contributionsAll authors participated in the study design and revised and improved successive versions of the manuscript. E. Arribas-Ibar conducted the statistical analysis, interpreted the results and wrote the first draft of the manuscript. A. Domingo-Salvany contributed to the statistical analysis, interpretation of results and manuscript writing. A. Sanchez-Niubò contributed to the statistical analysis and interpretation of results. M.T. Brugal reviewed the literature and contributed to interpretation of results. J.M. Suelves reviewed the literature and contributed to interpretation of results. All authors have approved the manuscript final version.
FundingFunding for this study was provided by Spanish Government Grant: Instituto de Salud Carlos III -FIS PI11/01358. Further financial support was provided by the Agència de Gestió d’Ajuts Universitaris i de Recerca (AGAUR 2009 SGR 718) and FIS-Redes de investigación cooperativa RD12/0028/0018 and RD16/0017/0013. The EU project JUST/2010/DPIP/AG/1410 also contributed to survey implementation. FIS, AGAUR and EU-JUST grants had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication. EAI was involved in the European Science Foundation research network programme ‘REFLEXION’-09-RNP-049.
Conflicts of interestThe authors declare they have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Our thanks to the participants, the collaborating centers and their professionals. We also are grateful to Dave Macfarlane for editing and English revision.











