




To analyse historical sex differences in fetal mortality in Spain since 1900 and their association with biological, social, and contextual determinants between 1996 and 2019.
MethodWe conducted a population-based, retrospective observational study using official data from the Spanish National Statistics Institute. Fetal mortality rates and sex ratios were calculated and stratified by maternal age, gestational age, marital status, municipality size, maternal geographic origin, and ecological proxies of solar exposure. The analysis was strictly descriptive and ecological, without attempting causal inference.
ResultsA persistent excess of male fetal mortality was observed throughout the study period. In the first decades of the twentieth century, male rates exceeded female rates by approximately 30–40%. As fetal mortality declined, the sex differential progressively narrowed, reaching around 5–10% in recent decades. Sex inequality varied non-linearly across gestation and differed by maternal age, residential environment, and geographic origin. The sex ratio was lower for conceptions occurring in months with higher solar irradiation and in southern peninsular provinces and the Canary Islands.
ConclusionsSex inequality in fetal mortality in Spain is persistent yet modifiable, and is consistent with the interaction between male biological vulnerability and social and contextual determinants. Incorporating fetal sex is essential for understanding perinatal inequalities.
Analizar históricamente la desigualdad por sexo en la mortalidad fetal en España desde 1900 y su asociación con determinantes biológicos, sociales y contextuales entre 1996 y 2019.
MétodoEstudio observacional, retrospectivo y de base poblacional a partir de datos oficiales del Instituto Nacional de Estadística. Se calcularon las tasas de mortalidad fetal y las razones de masculinidad estratificadas por edad materna, edad gestacional, estado civil, tamaño del municipio, origen geográfico de la madre e indicadores ecológicos de exposición solar. El análisis fue estrictamente descriptivo y ecológico, sin intentar establecer inferencias causales.
ResultadosSe observa una sobremortalidad fetal masculina persistente durante todo el periodo analizado. En las primeras décadas del siglo xx, las tasas masculinas superaban a las femeninas en torno al 30-40%. Con el descenso de la mortalidad fetal, el diferencial por sexo se redujo progresivamente hasta situarse en décadas recientes en torno al 5-10%. La desigualdad por sexo varía de forma no lineal a lo largo de la gestación y presenta diferencias según la edad materna, el entorno residencial y el origen geográfico. La razón de masculinidad es menor en concepciones ocurridas en meses de mayor irradiación solar y en provincias del sur peninsular y Canarias.
ConclusionesLa desigualdad por sexo en la mortalidad fetal en España es persistente, pero modificable, y es coherente con la interacción de la vulnerabilidad biológica masculina y los determinantes sociales y contextuales. Incorporar el sexo fetal resulta clave para comprender las desigualdades perinatales.
Fetal mortality is a sensitive indicator of population health and health-care systems, as it reflects biological conditions of pregnancy and social, environmental, and care-related factors before birth. International evidence has shown that male fetuses have a higher risk of intrauterine death than female fetuses. A meta-analysis based on more than 30 million births in high-income countries documented excess of male fetal mortality across different definitions of fetal death and gestational periods.1
Several studies have examined the biological mechanisms underlying this inequality. They show that excess male fetal mortality concentrates in contexts of intrauterine stress and among fetuses with growth restriction.2 These findings point to greater biological vulnerability of the male fetus to adverse conditions during gestation, possibly related to sex-specific differences in fetal growth, placental function, and physiological adaptive capacity. However, fetal sex is usually treated only as a secondary variable and rarely analysed as a structuring axis of inequality.3
Despite robust international evidence, sex inequality in fetal mortality has received little systematic attention in Spain. Existing national research has examined socio-economic, migratory, and territorial inequalities in stillbirth and perinatal outcomes, without treating fetal sex as a central analytical axis.4–7 To our knowledge, no study has analysed trends in sex differences in fetal mortality at the national level or explored their stratification by social and contextual determinants. The only partial exception is Fuster et al.,8 who reported higher male fetal mortality among native and immigrant mothers for 2007–2012.
This gap is particularly relevant in a country such as Spain, which in recent decades has undergone profound demographic and social transformations that have been widely documented in recent national research.9
Against this background, the present study aims to analyse historical sex differences in fetal mortality in Spain, focusing on their social and biological determinants during 1996–2019.
MethodStudy design and data sourcesWe conducted an observational study of fetal mortality in Spain using official data from the Spanish National Statistics Institute (INE). For the period 1900–1974, we used aggregated series from the Movimiento Natural de la Población to examine long-term trends in fetal mortality by sex. The stratified analyses by maternal, social, and contextual determinants were based on individual-level microdata from the Boletín Estadístico de Parto y de Muertes Fetales Tardías for the period 1996–2019. The study period was truncated in 2019 in order to exclude the impact of the COVID-19 pandemic.
The analysis uses exhaustive national administrative records. Annual live births ranged from approximately 600,000 in the early twentieth century to around 400,000 in recent years, while late fetal deaths declined from roughly 20,000 to about 1300 per year.
Event definition and variablesThe fetal mortality rate (FMR) was defined as the number of fetal deaths divided by the total number of births (live births+fetal deaths). For 1997–2019, gestational age information was available in the microdata. Analyses stratified by gestational age and fetal sex were restricted to deaths from 20 completed weeks onwards, as fetal sex is not recorded before this threshold.
For earlier periods, gestational age was not reliably recorded. To construct a long-term historical series, all registered fetal deaths were included in the numerator of the FMR. Evidence from 1997–2019 shows that 84% of fetal deaths with known gestational age occurred after 27 weeks, suggesting that historically registered fetal deaths predominantly correspond to late gestational losses. Between 1900 and 1931, when stillbirths and very early neonatal deaths were not distinguished, an 80/20 proportional distribution was applied based on the observed breakdown for 1932–1960.
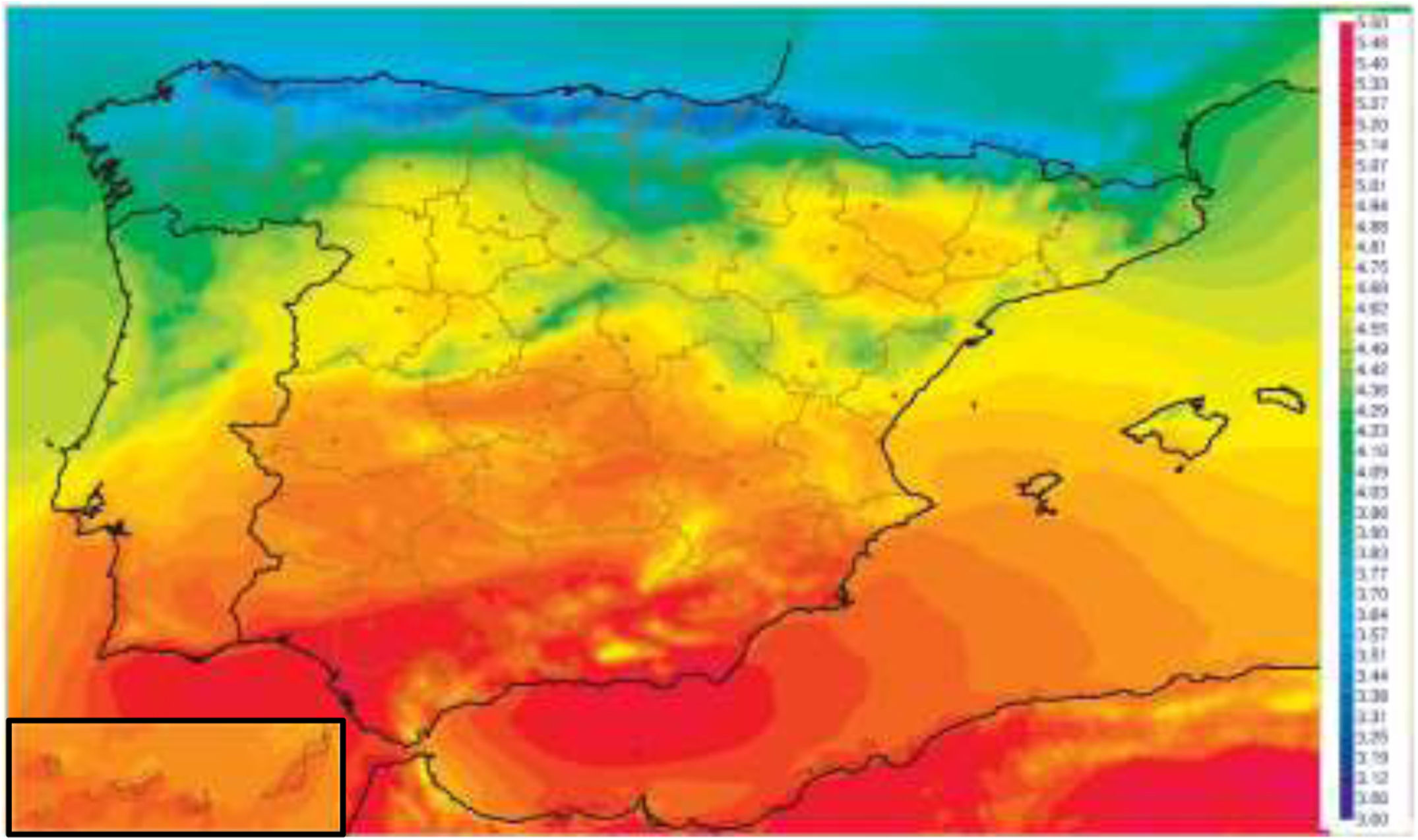
Covariates included gestational age, maternal age, marital status, size of municipality of residence, maternal geographic origin, and month preceding conception. Maternal and gestational age were included given their well-established association with fetal mortality and sex ratio variation.7 Solar exposure was used as a proxy for maternal vitamin D levels, in light of evidence linking vitamin D status to implantation, placental function, fetal survival, and potential sex ratio variation.10–12 It was operationalized through two ecological indicators: seasonality of conception and a North–South classification based on the latitudinal gradient of annual solar irradiation in mainland Spain. Provinces with systematically lower average irradiation (La Coruña, Lugo, Orense, Pontevedra, Asturias, Cantabria, Biscay, Guipúzcoa, and Álava) were grouped as “North”, and those with higher irradiation levels (Huelva, Seville, Cádiz, Málaga, Granada, Almería, Murcia, Alicante, Jaén, Córdoba, Santa Cruz de Tenerife, and Las Palmas) as “South”, according to official irradiation maps (Fig. 1). Rural–urban residence captured contextual differences in environment and healthcare, while marital status and nationality proxied social support and potential disparities in prenatal care.13,14

Mean global irradiance in 1983–2005 (kWh m-2 day-1). SIS (CM-SAF).
(Source: Sancho Ávila et al.17).
FMR was defined as the number of stillbirths divided by the total number of births (the sum of live births and stillbirths), expressed per thousand (‰). Sex inequality was assessed using the ratio between male and female FMR (male FMR / female FMR×100).
The sex FMR is a widely used indicator in population studies because it allows for the comparison of relative risks between male and female fetuses independently of overall mortality levels. However, it should be interpreted cautiously, as it may mask absolute differences and is sensitive to variations in registration practices and subgroup composition.
Analytical strategyThe analysis was strictly descriptive and exploratory. It is an ecological study that does not aim to establish causal relationships. Temporal trends in fetal mortality by sex were examined, and sex ratios were calculated stratified by different social and contextual determinants, without any intention of causal inference.
Although the analysis is based on population data, some variability may arise in subgroup analyses, particularly for smaller categories, which should be taken into account when interpreting the results.
Data qualitySpanish fetal mortality statistics may be affected by underreporting.15,16 The main sources of incomplete coverage appear to be administrative failures, delays in notification, or documentation inconsistencies rather than systematic selection mechanisms.
An important methodological consideration concerns the potential existence of sex-differential registration biases. In contrast to live births —historically declared by parents at the Civil Registry— the registration of late fetal deaths in Spain is initiated within the clinical setting. As documented by Juárez,15 when a fetal death occurs after six months of gestation, the event is certified through standardized medical documentation completed by the attending physician as part of routine clinical procedures.
Because the primary documentation is generated within the healthcare system and does not depend on parental initiative, there is no clear theoretical basis to expect systematic differences in registration by fetal sex. While incomplete coverage may affect absolute levels of fetal mortality, it is unlikely to substantially bias relative comparisons between male and female fetuses.
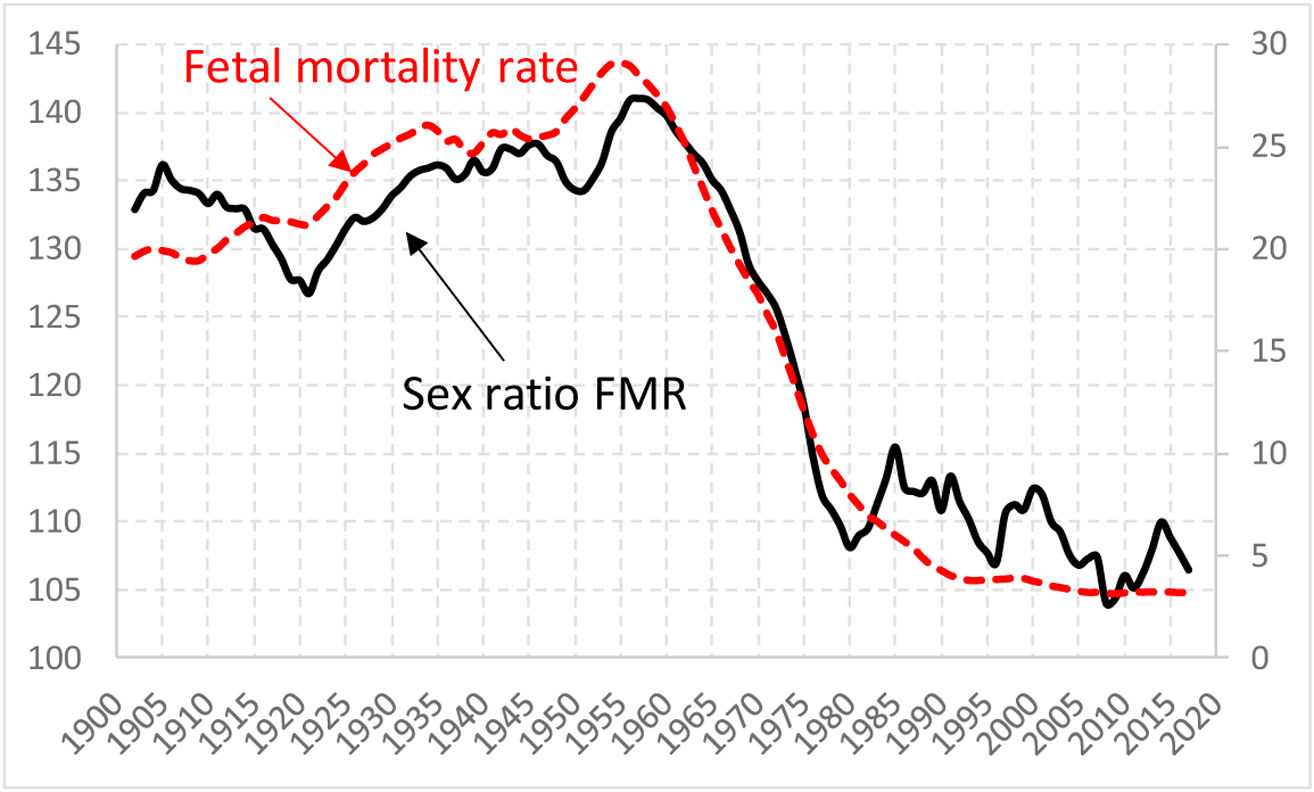
ResultsTemporal trendsFigure 2 shows the temporal evolution of the FMR by sex and the sex ratio in Spain. Throughout the entire study period, a persistent excess of male fetal mortality is observed. In the first decades of the twentieth century, when fetal mortality levels were high, male rates exceeded female rates by approximately 30–40%.

With the decline in the FMR from the mid-twentieth century onwards, the sex differential progressively narrowed. The sex ratio gradually approached the value of 100 (sex equality); however, in the most recent decades, excess male mortality, although much more moderate, remains at around 5–10%.
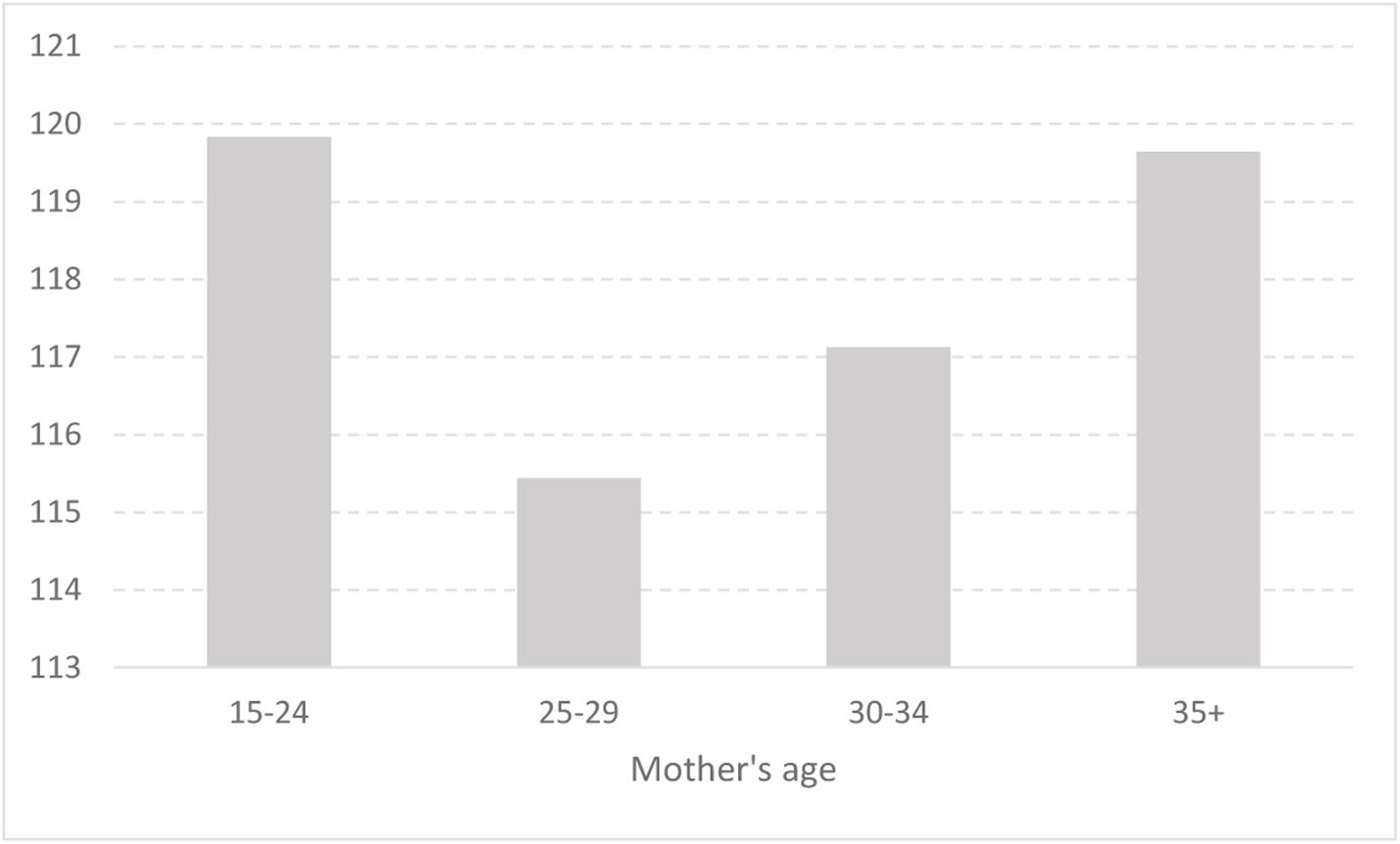
Maternal ageFigure 3 shows the sex ratio of fetal deaths by maternal age (1975–2019). Clear differences in excess male fetal mortality are observed according to maternal age.

From the 25–29 age group onwards, the sex ratio increases, reaching its highest values among mothers aged 35 years or older. Overall, the results indicate that sex inequality in fetal mortality varies by maternal age, with the most pronounced differentials concentrated at the extremes of the female reproductive period.
Gestational ageFigure 4 shows the sex ratio of fetal deaths by gestational age for the period 1997–2019. The analysis is restricted to fetal deaths from 20 weeks of gestation onwards, as information on fetal sex is not available prior to this threshold.

The sex RFM varies markedly by gestational age. The highest values are observed at 20–24 weeks of gestation, where the sex ratio exceeds 130%. This is followed by a notable decline in the 25–27 week interval, and then a moderate increase in subsequent weeks.
From 34–36 weeks onwards, a progressive reduction in the sex ratio is observed. This decline continues at more advanced gestational ages, and from week 39 onwards the sex ratio falls below 1, indicating that in the final stage of pregnancy the proportion of fetal deaths is higher among female than among male fetuses. Overall, these results demonstrate that sex inequality in fetal mortality changes substantially across gestation.
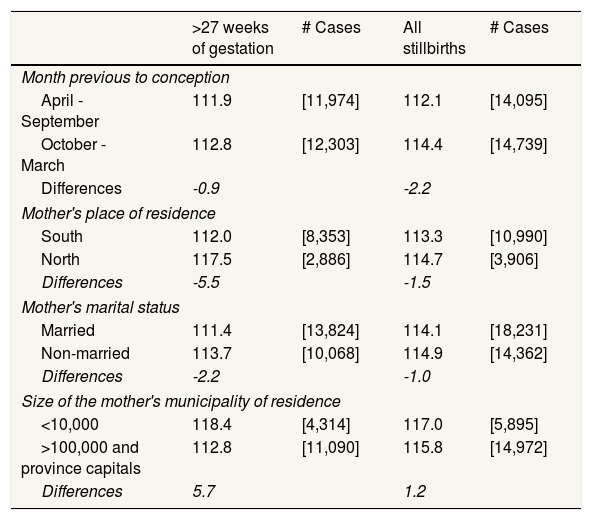
Solar exposureTable 1 presents the sex ratio of fetal deaths by the month preceding conception and by maternal area of residence, used as indirect indicators of solar exposure. The sex ratio is lower when conception occurs between April and September compared with October–March.
Sex ratio of fetal deaths by selected determinants (Spain, 1997–2019).
| >27 weeks of gestation | # Cases | All stillbirths | # Cases | |
|---|---|---|---|---|
| Month previous to conception | ||||
| April - September | 111.9 | [11,974] | 112.1 | [14,095] |
| October - March | 112.8 | [12,303] | 114.4 | [14,739] |
| Differences | -0.9 | -2.2 | ||
| Mother's place of residence | ||||
| South | 112.0 | [8,353] | 113.3 | [10,990] |
| North | 117.5 | [2,886] | 114.7 | [3,906] |
| Differences | -5.5 | -1.5 | ||
| Mother's marital status | ||||
| Married | 111.4 | [13,824] | 114.1 | [18,231] |
| Non-married | 113.7 | [10,068] | 114.9 | [14,362] |
| Differences | -2.2 | -1.0 | ||
| Size of the mother's municipality of residence | ||||
| <10,000 | 118.4 | [4,314] | 117.0 | [5,895] |
| >100,000 and province capitals | 112.8 | [11,090] | 115.8 | [14,972] |
| Differences | 5.7 | 1.2 | ||
Source: INE and author's own calculations.
Similarly, provinces in southern peninsular Spain and the Canary Islands show a lower sex ratio than that observed in northern provinces, consistent with the territorial gradient in solar irradiation (Fig. 1). Overall, the results indicate differences in the sex ratio associated with both the seasonality of conception and the geographic location of maternal residence.
Maternal marital statusAccording to Table 1, the sex ratio is slightly higher among non-married mothers compared with married mothers.
Differences between rural and urban areasThe results shown in Table 1 indicate that the sex ratio is higher in smaller municipalities (<10,000 inhabitants) than in larger ones (>100,000 inhabitants and provincial capitals).
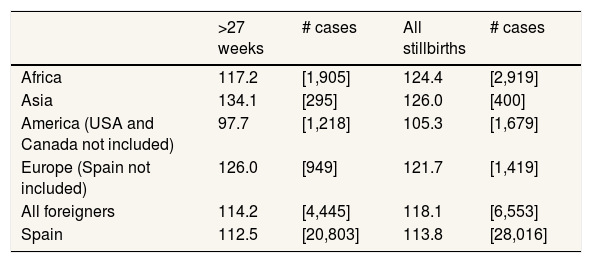
Maternal geographic originTable 2 presents the sex ratio of fetal deaths by maternal geographic origin for the period 1996–2019. The results reveal notable differences. Mothers of Spanish nationality show a relatively low sex ratio, lower than that observed in most groups of foreign-born mothers. In particular, the highest values are found among mothers from Asia and from Europe (excluding Spain). Mothers originating from Africa also exhibit a higher sex ratio than Spanish mothers. By contrast, those from Ibero-America display the lowest values among all groups analysed, even lower than those observed for Spanish mothers.
Sex ratio of fetal deaths by maternal geographic origin (Spain, 1996–2019).
| >27 weeks | # cases | All stillbirths | # cases | |
|---|---|---|---|---|
| Africa | 117.2 | [1,905] | 124.4 | [2,919] |
| Asia | 134.1 | [295] | 126.0 | [400] |
| America (USA and Canada not included) | 97.7 | [1,218] | 105.3 | [1,679] |
| Europe (Spain not included) | 126.0 | [949] | 121.7 | [1,419] |
| All foreigners | 114.2 | [4,445] | 118.1 | [6,553] |
| Spain | 112.5 | [20,803] | 113.8 | [28,016] |
Source: INE and author's own calculations.
Our results confirm the persistence of excess male fetal mortality in Spain, in line with both the international1–3 and national4–6 literature. This disadvantage has been linked to greater biological fragility of the male fetus when exposed to adverse conditions during gestation, a phenomenon that has led to the coinage of the term “frail males”. The biomedical literature suggests that this male disadvantage is exacerbated in unfavourable gestational contexts and is associated with sex-specific differences in fetal growth, placental function, and physiological adaptation.2
A central finding of our study is that the magnitude of this male vulnerability appears to depend on the overall health-care context: we observe that higher levels of overall fetal mortality tend to be associated with greater relative inequality between sexes. This pattern is consistent with the hypothesis that improvements in obstetric care may disproportionately benefit the most fragile fetuses (in this case, males), thereby reducing their excess mortality. Consequently, sex inequality in fetal mortality may be interpreted as a sensitive indicator of the level of health-system development in the perinatal domain.
Gestational ageThe analysis by gestational age shows that sex inequality follows a clearly non-linear pattern, thereby refuting the notion of a uniform male disadvantage throughout gestation. This finding is consistent with previous studies documenting an attenuation or even a reversal of the differential at more advanced gestational ages.1,18 One plausible explanation relates to differential intrauterine selection processes: greater early loss among the most fragile male fetuses may result in the survival of a more positively selected male group at later stages of gestation.18,19 In late pregnancy, fetal deaths are more likely to be associated with obstetric causes less closely linked to intrinsic male biological fragility, which may explain the reduction or reversal of the sex differential. Our findings support the notion that sex inequality in fetal mortality exhibits a dynamic pattern across gestation, rather than a uniform one. However, the non-linear pattern across gestation suggests that mechanisms beyond intrauterine selection —such as obstetric decision-making at advanced gestational ages or differences in registration practices— may also contribute to the attenuation or reversal of the male excess.
Social determinants, maternal stress, and residential environmentIn the literature, maternal psychosocial factors emerge as a third relevant axis for understanding differential survival by sex. Numerous studies have linked maternal stress —both acute and chronic— to an increased risk of pregnancy loss, particularly among male fetuses.20–22 Evidence indicates that episodes of collective stress (such as terrorist attacks, economic recessions, armed conflicts, and pandemics) are associated with increases in spontaneous abortions and reductions in the proportion of male births. Other studies have reported similar associations linking fetal losses to work-related stress, economic insecurity, or situations of deprivation.23,24
Within this framework, our findings regarding maternal marital status are consistent with the literature: we observe a slightly higher sex ratio of fetal mortality among non-married women, suggesting a relatively greater loss of male fetuses in this group. However, because marital status is an imperfect proxy for social support —particularly in contemporary contexts where a substantial proportion of women have children within non-marital unions— the observed difference likely underestimates the true impact of the absence of partner support during pregnancy. If information on cohabitation or partnership status were available, the underlying differences might be even more pronounced. Our results suggest that family-related psychosocial factors may contribute, together with male biological vulnerability, to sex inequality in fetal mortality.
In addition, the maternal residential environment appears to play a moderating role in this phenomenon. The literature suggests that certain adverse environmental factors, such as air pollution, act as biological stressors that have been associated with an increased risk of fetal death and may disproportionately affect male fetuses.13,14,25,26 Accordingly, one might expect higher excess male fetal mortality in urban environments, where higher levels of pollution and psychosocial stress tend to concentrate.
However, our results reveal the opposite pattern: the sex ratio of fetal deaths is higher in small municipalities than in large cities and provincial capitals. One plausible interpretation is that the negative effects associated with pollution and urban stress may be offset by the advantages of urban areas in terms of access to specialised obstetric care. In cities, greater availability of advanced health-care resources may improve the survival of the most fragile fetuses, thereby reducing excess male mortality. This argument is consistent with evidence highlighting the central role of the quality of perinatal care in reducing fetal mortality.3,27,28 Nevertheless, these interpretations should be treated with caution, given the descriptive nature of our analysis and the lack of individual-level data on environmental exposures or health-care utilisation.
Maternal origin and solar irradiationMaternal geographic origin is associated both with overall levels of fetal mortality4–7 and with the magnitude of sex inequality. The study by Fuster et al.8 showed higher FMR among foreign women compared to native women, confirming this pattern of origin-based differences in Spain, although it did not explicitly analyse the role of fetal sex.
Our study extends this perspective by showing that maternal origin is also associated with differences in the sex ratio of fetal mortality, indicating that sex differences are intertwined with social and migratory inequalities. From a psychosocial standpoint, immigrant women are often exposed to higher levels of chronic stress resulting from labour precariousness, legal insecurity, and the absence of family support networks —factors that may intensify the selective loss of male fetuses.
Our findings should also be interpreted in light of the “healthy immigrant paradox”, a well-documented phenomenon whereby immigrant populations often exhibit better health outcomes than native populations despite facing socio-economic disadvantages.29 However, our results reveal a heterogeneous pattern by maternal geographic origin. While mothers from Ibero-America display relatively lower fetal mortality ratios, this pattern is not observed among mothers from Asia, Europe (excluding Spain), or Africa. Therefore, the healthy immigrant paradox may partially account for the favorable outcomes observed in the Ibero-American group, but it does not provide a uniform explanation across all groups analysed.
However, the heterogeneity observed across origin groups suggests the possible involvement of mechanisms beyond the psychosocial component. Maternal vitamin D status has been proposed as a potentially relevant biological factor, as higher levels have been associated with improved pregnancy outcomes and lower fetal mortality.10–12 Given the greater vulnerability of male embryos in early development, these effects could differentially benefit male survival.
This interpretation should be treated with caution. In our study, solar exposure is measured through ecological proxies, and the observed patterns —lower excess male fetal mortality in periods and regions with higher solar irradiation— are compatible with, but do not demonstrate, a modulatory role of vitamin D.
Differences in vitamin D deficiency across populations may also contribute to the higher excess male mortality observed in some groups, although this remains speculative.30 By contrast, the lower sex ratio among Ibero-American mothers’ points to the likely coexistence of multiple social and biological factors. These findings should be considered exploratory and highlight the need for studies incorporating individual-level data and biomarkers.
Availability of databases and material for replicationThis study is based exclusively on official statistics produced by the Spanish National Statistics Institute (INE). The aggregated historical series (Movimiento Natural de la Población) and the individual-level microdata on births and late fetal deaths (Boletín Estadístico de Parto y de Muertes Fetales Tardías) are publicly available on the INE website (www.ine.es<http://www.ine.es). No new data were generated in this study.
International literature shows higher fetal mortality among males, attributed to their greater biological vulnerability; however, in Spain fetal sex has rarely been analysed as a specific axis of inequality.
What does this study add to the literature?This study provides the first comprehensive analysis in Spain of sex inequality in fetal mortality as a central focus, showing how it is modulated by gestational age, social context, and the territorial environment.
What are the implications of the results?The findings highlight the need to systematically incorporate fetal sex into analyses of perinatal inequalities and into the design of maternal and child health policies and strategies.
Alberto Lana.
Transparency declarationThe author guarantees the accuracy, transparency, and integrity of the data and information contained in this study, and affirms that no relevant information has been omitted.
Authorship contributionsJ.J. Sánchez Barricarte conceived the study, conducted the analysis, and wrote the manuscript.
FundingThis work was funded by the project PHS-2024/PH-HUM-414 of the Community of Madrid (Spain).
Conflicts of interestNone.











