



To evaluate the incidence of risky consumption (RC) and heavy episodic drinking (HED) in the Cohort of Spanish university students at two-year follow-up and to identify predictors of these patterns of alcohol consumption and the association between these patterns and academic achievement.
MethodWe carried out a cohort study. Alcohol consumption was measured with the AUDIT. The following variables were collected by questionnaire: place of residence, parents' education, alcohol consumption in the family, age of onset of use, alcohol expectancies, and the academic achievement. We constructed logistic regression models using three dependent variables: RC, HED, and academic achievement.
ResultsThe response rate at two-year follow-up was 64.1%. The incidence of RC and HED at two-year follow-up were 24.92% and 4.01% respectively. The prevalence of RC rose from 37.1% to 54.6%. On the contrary, HED dropped from 12.2% to 8.7%. In relation to incidence of RC, being male (OR=2.77), medium (OR=1.59) or high expectancies (OR=2.24), and early age of onset of use (OR=2.26) constituted risk factors. In contrast, living with parents constituted a protective factor (OR=0.48). For HED, being male (OR=1.92) and high expectancies (OR=2.96) were risk factors. RC and HED were risk factors for low academic achievement.
ConclusionsHED is a pattern of alcohol consumption mainly associated with adolescence, while RC is associated with youth. Both patterns are predictors of academic achievement. Public Health strategies should focus on modifying expectancies and limit access to alcohol at young ages.
Determinar la incidencia del consumo de riesgo de alcohol (CR) y del consumo intensivo (CI) en una cohorte de estudiantes universitarios a los 2 años de seguimiento e identificar los factores de estas pautas de consumo de alcohol y su asociación con el redimiento académico.
MétodoSe ha realizado un estudio de cohortes. El consumo de alcohol se ha medido con el AUDIT. Las siguientes variables se han medido mediante cuestionario: lugar de residencia, educación parental, consumo de alcohol en la familia, edad de inicio de uso, expectativas sobre alcohol y rendimiento académico. Para el análisis de datos se han construido modelos de regresión logística con las tres variables dependientes consideradas: CR, CI y rendimiento académico.
ResultadosLa tasa de respuesta en el seguimiento se situó en el 64,1%. La incidencia de CR y CI a los 2 años fue del 24,92% y el 4,01%. La prevalencia de CR aumentó del 37,1% al 54,6%. Por el contrario, el CI disminuyó del 12,2% al 8,7%. Con relación a la incidencia de CR, el ser varón (OR=2,77), las medias (OR=1.59) y altas expectativas (OR=2.24), y la edad temprana de inicio de uso (OR=2,26) son factores de riesgo. Por el contrario, el vivir con los padres muestra un factor protector (OR=0,48). Para el CI, ser varón (OR=1,92) y las altas expectativas (OR=2,96) son también factores de riesgo. Ambos patrones de consumo constituyen factores de riesgo del bajo rendimiento académico.
ConclusionesEl CI es un patrón de consumo principalmente asociado con la adolescencia, mientras que el CR se asocia con la juventud. Ambos patrones son predictores del rendimiento académico. Las estrategias de salud pública deberían centrarse en la modificación de expectativas y en limitar el acceso al alcohol de los más jóvenes.
Psychological, physical and social damage have been associated to patterns of high alcohol consumption among adolescents, like risky consumption (RC), characterized by high consumption of alcohol, or heavy episodic drinking (HED), described as the consumption of high quantities of alcohol in a short period of time.1–5
There have been many alerts about the high prevalence of these drinking habits among adolescents6–8 and many risk factors have been identified as familiar background,9,10 age of onset,11,12 peer influence,13,14 and expectancies.11,15
On the other hand, these own patterns of alcohol consumption may consist in risk factors for some aspects, like academic attainment. RC and HED may interfere directly or indirectly on educational achievement by reducing the number of hours dedicated for studying, by affecting the motivation and school attitudes or even limiting neurocognitive abilities.16,17
As the adolescent development is related to multiple dimensions and the alcohol consumption patterns and its associated factors can be modified at different ages,18 it is desirable to know the trajectory of these drinking habits and their associated risk factors throughout the years.
Up to now, there is increasing longitudinal data about prevalence and risk factors of alcohol drinking among subjects that are in process of development and independence.19–23 Nonetheless, in Spain, such longitudinal studies are still scarce. In one-year follow-up study with high school students (13–20 years old), Fuentes-Almendras et al24 identified increment of drinking. Higher drinking frequency was related to older ages and to being male. In another two-year follow-up study, 15 years-old male outscored female on week alcohol consumption.25
Therefore, in an attempt to extend the data provided by a previous work of our group,11 the aim of this study is to evaluate the incidence of RC and HED in the Cohort of Spanish university students at two-year follow-up and to identify predictors of these patterns of alcohol consumption and the association between these patterns and academic achievement.
MethodsDesign, population and sampleA cohort study was carried out to evaluate the neurocognitive consequences of alcohol use. The study population was first year students (18 to 19 years old) at the University of Santiago de Compostela (Spain) (target n=2700).
Data collection proceduresInitial data collection was carried out by means of a questionnaire filled in by students in the classroom (October to February 2006). The subjects were analyzed two-year follow up again (October to February 2008).
Alcohol use was measured with the Galician validated version of the AUDIT.26,27 In this version, for a screening of RC, the cut-off value is 5 for men and 4 for women. Along with the AUDIT, we used another questionnaire that asked about the potential factors associated with alcohol use (educational level and alcohol use of parents, presence of alcohol related problems and age of onset of use). One of the items in this second questionnaire referred specifically to alcohol expectancies. In this question the students were required to rank 7 positive and 7 negative expectancies about the effects of alcohol. This question was generated using items from a questionnaire previously used with Spanish youths.28 This same questionnaire was used to ask about students' grades and several socio-demographic variables.
Definition of variables(1) Risky consumption (RC). Dichotomous variable generated from AUDIT score. A different cut-off value was established according to gender: >4 for women; and >5 for men. (2) Heavy episodic drinking (HED). Dichotomous variable generated from the third AUDIT question “How often do you have 6 or more alcoholic drinks per occasion?” which was coded as follows: never=0, less than once a month=0, once a month=0, once a week=1, daily or almost daily=1. The sensitivity and specificity of this question with this cut-off value are respectively 0.40 and 0.94.29 (3) Low academic achievement. Dichotomous variable generated from mean grades of students at two-year follow-up. A cut-off value was established at the 20th percentile. So, students included in the 20th percentile of the mean of their grades at two-year follow-up were classified as “low academic achievement”.
Several socio-demographic variables were considered such as gender, place of residence (at the parents' home/outside of the parents' home), and the maternal educational level (primary school/high school/university). Alcohol use in the subject’s family was included as mother’s alcohol use (doesn’t consume/consumes). Maternal educational level and mother’s alcohol use have been considered because of their greater variability. Four categories were defined for age of onset of use (after 16 years old, at 16, at 15, before the age of 15). Finally, taking the number of positive and negative expectancies into account, a score ranging from 0 to 14 was generated (0 being the maximum of negative expectancies and 14 the maximum of positive expectancies). The scores were divided up into terciles.
Statistical analysisWe constructed logistic regression models to estimate odds ratios (OR) using three dependent variables: RC, HED, and academic achievement. The models for RC and HED include socio-demographic data as independent variables. Finally, two models were constructed for academic achievement, one with RC as independent variable and another with HED.
All the subjects, even abstainers, were included in the models. Maximal models were generated including all theoretical independent variables. From these maximal models, final models were generated. Final models included all significant variables and also no significant variables when their exclusion changed the OR of other variables by more than 10%.
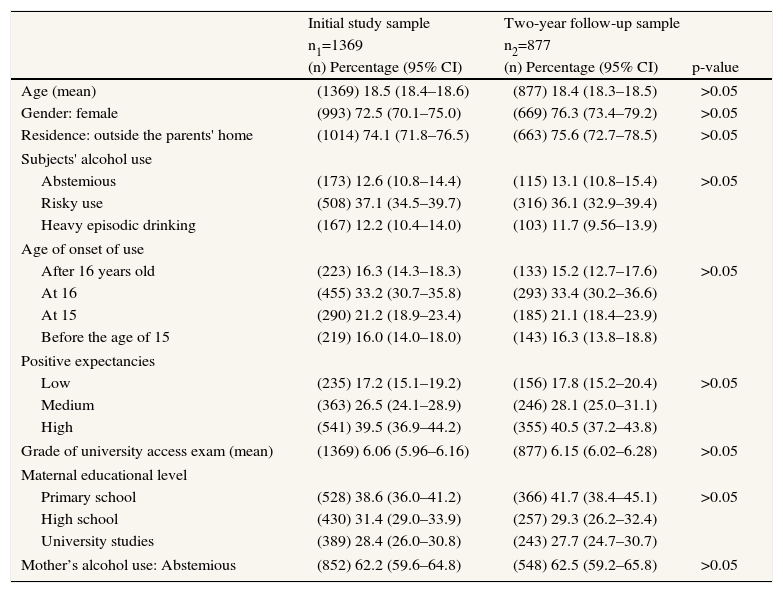
ResultsThe response rate at two-year follow-up was 64.1%. Table 1 shows the characteristics of total sample (n=1369) and the characteristics of two-year follow-up sample (n=877). The table does not show significant differences for any variable. The observed reduction in the follow-up sample might be explained by two motives of similar weight: dropping out of college; and absences from school or degree change.
Characteristics of the subjects at initial study: initial study sample and two-year follow-up sample
| Initial study sample | Two-year follow-up sample | ||
| n1=1369 | n2=877 | ||
| (n) Percentage (95% CI) | (n) Percentage (95% CI) | p-value | |
| Age (mean) | (1369) 18.5 (18.4–18.6) | (877) 18.4 (18.3–18.5) | >0.05 |
| Gender: female | (993) 72.5 (70.1–75.0) | (669) 76.3 (73.4–79.2) | >0.05 |
| Residence: outside the parents' home | (1014) 74.1 (71.8–76.5) | (663) 75.6 (72.7–78.5) | >0.05 |
| Subjects' alcohol use | |||
| Abstemious | (173) 12.6 (10.8–14.4) | (115) 13.1 (10.8–15.4) | >0.05 |
| Risky use | (508) 37.1 (34.5–39.7) | (316) 36.1 (32.9–39.4) | |
| Heavy episodic drinking | (167) 12.2 (10.4–14.0) | (103) 11.7 (9.56–13.9) | |
| Age of onset of use | |||
| After 16 years old | (223) 16.3 (14.3–18.3) | (133) 15.2 (12.7–17.6) | >0.05 |
| At 16 | (455) 33.2 (30.7–35.8) | (293) 33.4 (30.2–36.6) | |
| At 15 | (290) 21.2 (18.9–23.4) | (185) 21.1 (18.4–23.9) | |
| Before the age of 15 | (219) 16.0 (14.0–18.0) | (143) 16.3 (13.8–18.8) | |
| Positive expectancies | |||
| Low | (235) 17.2 (15.1–19.2) | (156) 17.8 (15.2–20.4) | >0.05 |
| Medium | (363) 26.5 (24.1–28.9) | (246) 28.1 (25.0–31.1) | |
| High | (541) 39.5 (36.9–44.2) | (355) 40.5 (37.2–43.8) | |
| Grade of university access exam (mean) | (1369) 6.06 (5.96–6.16) | (877) 6.15 (6.02–6.28) | >0.05 |
| Maternal educational level | |||
| Primary school | (528) 38.6 (36.0–41.2) | (366) 41.7 (38.4–45.1) | >0.05 |
| High school | (430) 31.4 (29.0–33.9) | (257) 29.3 (26.2–32.4) | |
| University studies | (389) 28.4 (26.0–30.8) | (243) 27.7 (24.7–30.7) | |
| Mother’s alcohol use: Abstemious | (852) 62.2 (59.6–64.8) | (548) 62.5 (59.2–65.8) | >0.05 |
n: subjects; 95% CI: 95% confidence interval.
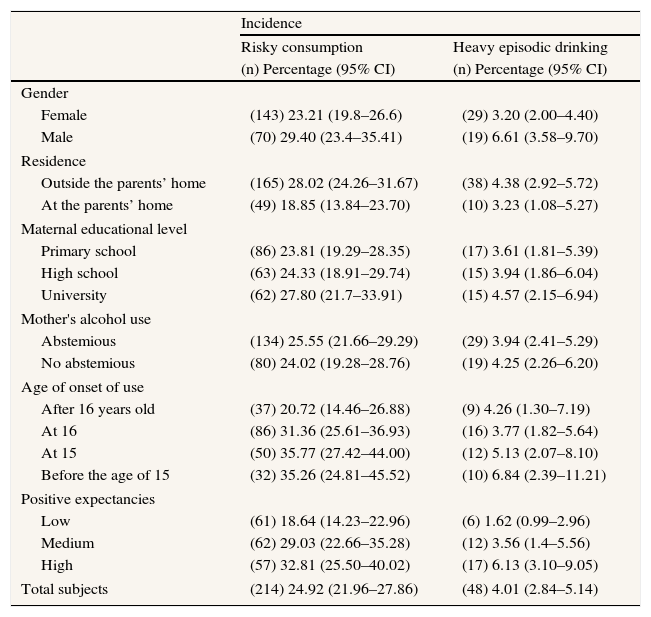
The incidence of RC and of HED at two-year follow-up were 24.92% (95% CI: 21.96–27.86) and 4.01% (95% CI: 2.84–5.41) respectively. The condition of being male, having a non-abstainer mother, besides of the early age of onset of use, and high positive expectancies are associated with the higher incidence rates of RC and HED (table 2).
Main characteristics of the subjects and incidence of risky consumption and incidence of heavy episodic drinking at two-year follow-up.
| Incidence | ||
| Risky consumption | Heavy episodic drinking | |
| (n) Percentage (95% CI) | (n) Percentage (95% CI) | |
| Gender | ||
| Female | (143) 23.21 (19.8–26.6) | (29) 3.20 (2.00–4.40) |
| Male | (70) 29.40 (23.4–35.41) | (19) 6.61 (3.58–9.70) |
| Residence | ||
| Outside the parents’ home | (165) 28.02 (24.26–31.67) | (38) 4.38 (2.92–5.72) |
| At the parents’ home | (49) 18.85 (13.84–23.70) | (10) 3.23 (1.08–5.27) |
| Maternal educational level | ||
| Primary school | (86) 23.81 (19.29–28.35) | (17) 3.61 (1.81–5.39) |
| High school | (63) 24.33 (18.91–29.74) | (15) 3.94 (1.86–6.04) |
| University | (62) 27.80 (21.7–33.91) | (15) 4.57 (2.15–6.94) |
| Mother's alcohol use | ||
| Abstemious | (134) 25.55 (21.66–29.29) | (29) 3.94 (2.41–5.29) |
| No abstemious | (80) 24.02 (19.28–28.76) | (19) 4.25 (2.26–6.20) |
| Age of onset of use | ||
| After 16 years old | (37) 20.72 (14.46–26.88) | (9) 4.26 (1.30–7.19) |
| At 16 | (86) 31.36 (25.61–36.93) | (16) 3.77 (1.82–5.64) |
| At 15 | (50) 35.77 (27.42–44.00) | (12) 5.13 (2.07–8.10) |
| Before the age of 15 | (32) 35.26 (24.81–45.52) | (10) 6.84 (2.39–11.21) |
| Positive expectancies | ||
| Low | (61) 18.64 (14.23–22.96) | (6) 1.62 (0.99–2.96) |
| Medium | (62) 29.03 (22.66–35.28) | (12) 3.56 (1.4–5.56) |
| High | (57) 32.81 (25.50–40.02) | (17) 6.13 (3.10–9.05) |
| Total subjects | (214) 24.92 (21.96–27.86) | (48) 4.01 (2.84–5.14) |
n: subjects; 95% CI: 95% confidence interval.
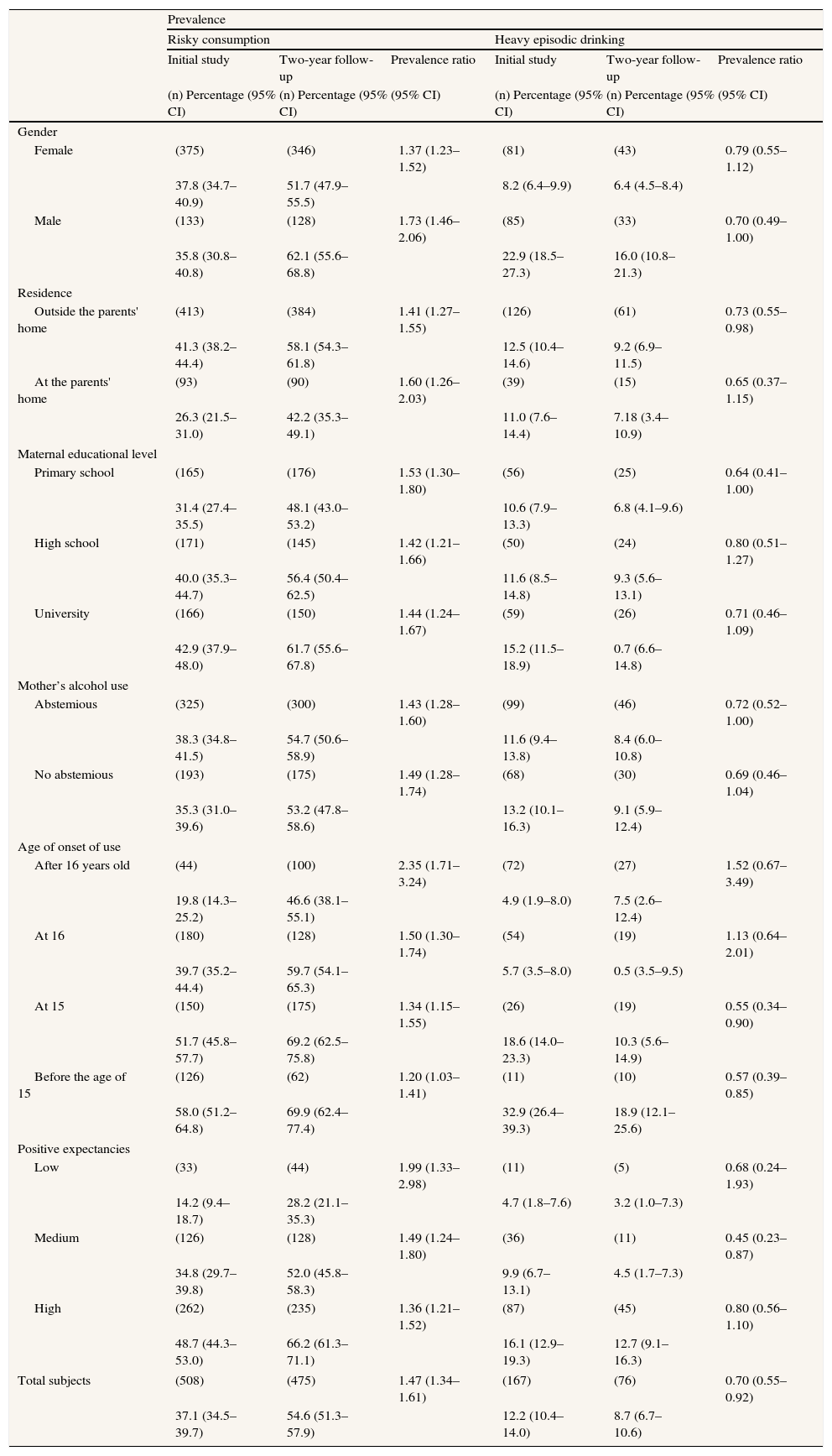
Table 3 shows the prevalences of alcohol consumption. The prevalence of RC shows significant changes, 37.1% vs. 54.6%, prevalence ratio=1.47 (95% CI: 1.34–1.61). On the contrary, the prevalence of HED drops from 12.2% to 8.7%, prevalence ratio=0.70 (95% CI: 0.55–0.92). In relation to abstemious variable, the prevalence at initial study and at two-year follow-up do not show significant differences.
Main characteristics of the subjects and prevalence of risky consumption and prevalence of heavy episodic drinking
| Prevalence | ||||||
| Risky consumption | Heavy episodic drinking | |||||
| Initial study | Two-year follow-up | Prevalence ratio | Initial study | Two-year follow-up | Prevalence ratio | |
| (n) Percentage (95% CI) | (n) Percentage (95% CI) | (95% CI) | (n) Percentage (95% CI) | (n) Percentage (95% CI) | (95% CI) | |
| Gender | ||||||
| Female | (375) | (346) | 1.37 (1.23–1.52) | (81) | (43) | 0.79 (0.55–1.12) |
| 37.8 (34.7–40.9) | 51.7 (47.9–55.5) | 8.2 (6.4–9.9) | 6.4 (4.5–8.4) | |||
| Male | (133) | (128) | 1.73 (1.46–2.06) | (85) | (33) | 0.70 (0.49–1.00) |
| 35.8 (30.8–40.8) | 62.1 (55.6–68.8) | 22.9 (18.5–27.3) | 16.0 (10.8–21.3) | |||
| Residence | ||||||
| Outside the parents' home | (413) | (384) | 1.41 (1.27–1.55) | (126) | (61) | 0.73 (0.55–0.98) |
| 41.3 (38.2–44.4) | 58.1 (54.3–61.8) | 12.5 (10.4–14.6) | 9.2 (6.9–11.5) | |||
| At the parents' home | (93) | (90) | 1.60 (1.26–2.03) | (39) | (15) | 0.65 (0.37–1.15) |
| 26.3 (21.5–31.0) | 42.2 (35.3–49.1) | 11.0 (7.6–14.4) | 7.18 (3.4–10.9) | |||
| Maternal educational level | ||||||
| Primary school | (165) | (176) | 1.53 (1.30–1.80) | (56) | (25) | 0.64 (0.41–1.00) |
| 31.4 (27.4–35.5) | 48.1 (43.0–53.2) | 10.6 (7.9–13.3) | 6.8 (4.1–9.6) | |||
| High school | (171) | (145) | 1.42 (1.21–1.66) | (50) | (24) | 0.80 (0.51–1.27) |
| 40.0 (35.3–44.7) | 56.4 (50.4–62.5) | 11.6 (8.5–14.8) | 9.3 (5.6–13.1) | |||
| University | (166) | (150) | 1.44 (1.24–1.67) | (59) | (26) | 0.71 (0.46–1.09) |
| 42.9 (37.9–48.0) | 61.7 (55.6–67.8) | 15.2 (11.5–18.9) | 0.7 (6.6–14.8) | |||
| Mother’s alcohol use | ||||||
| Abstemious | (325) | (300) | 1.43 (1.28–1.60) | (99) | (46) | 0.72 (0.52–1.00) |
| 38.3 (34.8–41.5) | 54.7 (50.6–58.9) | 11.6 (9.4–13.8) | 8.4 (6.0–10.8) | |||
| No abstemious | (193) | (175) | 1.49 (1.28–1.74) | (68) | (30) | 0.69 (0.46–1.04) |
| 35.3 (31.0–39.6) | 53.2 (47.8–58.6) | 13.2 (10.1–16.3) | 9.1 (5.9–12.4) | |||
| Age of onset of use | ||||||
| After 16 years old | (44) | (100) | 2.35 (1.71–3.24) | (72) | (27) | 1.52 (0.67–3.49) |
| 19.8 (14.3–25.2) | 46.6 (38.1–55.1) | 4.9 (1.9–8.0) | 7.5 (2.6–12.4) | |||
| At 16 | (180) | (128) | 1.50 (1.30–1.74) | (54) | (19) | 1.13 (0.64–2.01) |
| 39.7 (35.2–44.4) | 59.7 (54.1–65.3) | 5.7 (3.5–8.0) | 0.5 (3.5–9.5) | |||
| At 15 | (150) | (175) | 1.34 (1.15–1.55) | (26) | (19) | 0.55 (0.34–0.90) |
| 51.7 (45.8–57.7) | 69.2 (62.5–75.8) | 18.6 (14.0–23.3) | 10.3 (5.6–14.9) | |||
| Before the age of 15 | (126) | (62) | 1.20 (1.03–1.41) | (11) | (10) | 0.57 (0.39–0.85) |
| 58.0 (51.2–64.8) | 69.9 (62.4–77.4) | 32.9 (26.4–39.3) | 18.9 (12.1–25.6) | |||
| Positive expectancies | ||||||
| Low | (33) | (44) | 1.99 (1.33–2.98) | (11) | (5) | 0.68 (0.24–1.93) |
| 14.2 (9.4–18.7) | 28.2 (21.1–35.3) | 4.7 (1.8–7.6) | 3.2 (1.0–7.3) | |||
| Medium | (126) | (128) | 1.49 (1.24–1.80) | (36) | (11) | 0.45 (0.23–0.87) |
| 34.8 (29.7–39.8) | 52.0 (45.8–58.3) | 9.9 (6.7–13.1) | 4.5 (1.7–7.3) | |||
| High | (262) | (235) | 1.36 (1.21–1.52) | (87) | (45) | 0.80 (0.56–1.10) |
| 48.7 (44.3–53.0) | 66.2 (61.3–71.1) | 16.1 (12.9–19.3) | 12.7 (9.1–16.3) | |||
| Total subjects | (508) | (475) | 1.47 (1.34–1.61) | (167) | (76) | 0.70 (0.55–0.92) |
| 37.1 (34.5–39.7) | 54.6 (51.3–57.9) | 12.2 (10.4–14.0) | 8.7 (6.7–10.6) | |||
n: subjects; 95% CI: 95% confidence interval.
The prevalence rates of RC at two-year follow-up are significantly higher than at initial study for all categories of subjects (table 3). The prevalence of RC present higher increase among the categories of subjects with lower prevalence at initial study (table 3). On the contrary, the prevalence of HED at two-year follow-up is significantly lower than at initial-study (table 3).
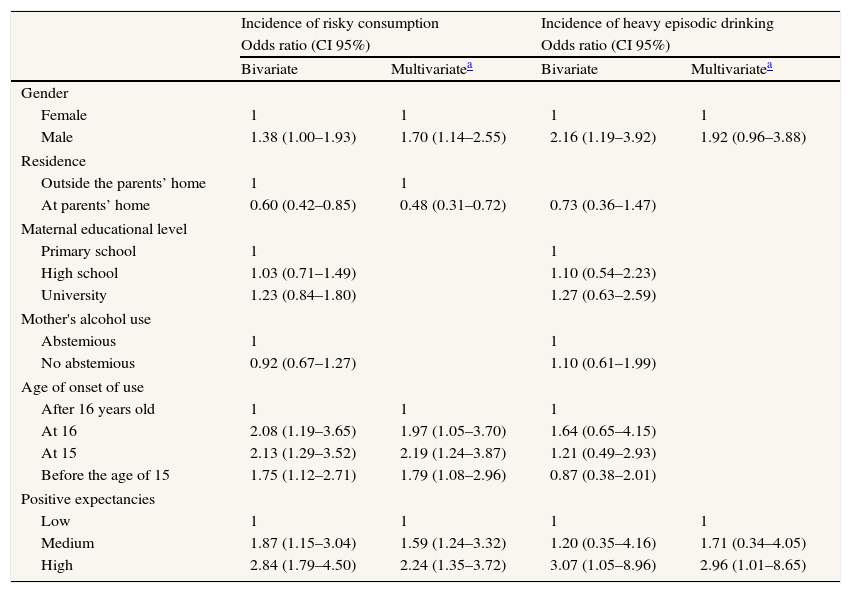
In relation to incidence of RC (table 4), the multivariate model shows that being male, high and medium positive expectancies, and age of onset of use at 15 years, all constitute risk factors for incidence of RC. On the contrary, living with parents shows a protective effect on RC. Table 4 also shows that being male and having high positive expectancies are risk factors for incidence of HED. Finally, table 5 shows the influence of RC and HED on academic achievement. Both patterns are risk factors of low academic achievement.
Influence of characteristics of subject and their family background on incidence of risky consumption and incidence of heavy episodic drinking at two-year follow-up.
| Incidence of risky consumption | Incidence of heavy episodic drinking | |||
| Odds ratio (CI 95%) | Odds ratio (CI 95%) | |||
| Bivariate | Multivariatea | Bivariate | Multivariatea | |
| Gender | ||||
| Female | 1 | 1 | 1 | 1 |
| Male | 1.38 (1.00–1.93) | 1.70 (1.14–2.55) | 2.16 (1.19–3.92) | 1.92 (0.96–3.88) |
| Residence | ||||
| Outside the parents’ home | 1 | 1 | ||
| At parents’ home | 0.60 (0.42–0.85) | 0.48 (0.31–0.72) | 0.73 (0.36–1.47) | |
| Maternal educational level | ||||
| Primary school | 1 | 1 | ||
| High school | 1.03 (0.71–1.49) | 1.10 (0.54–2.23) | ||
| University | 1.23 (0.84–1.80) | 1.27 (0.63–2.59) | ||
| Mother's alcohol use | ||||
| Abstemious | 1 | 1 | ||
| No abstemious | 0.92 (0.67–1.27) | 1.10 (0.61–1.99) | ||
| Age of onset of use | ||||
| After 16 years old | 1 | 1 | 1 | |
| At 16 | 2.08 (1.19–3.65) | 1.97 (1.05–3.70) | 1.64 (0.65–4.15) | |
| At 15 | 2.13 (1.29–3.52) | 2.19 (1.24–3.87) | 1.21 (0.49–2.93) | |
| Before the age of 15 | 1.75 (1.12–2.71) | 1.79 (1.08–2.96) | 0.87 (0.38–2.01) | |
| Positive expectancies | ||||
| Low | 1 | 1 | 1 | 1 |
| Medium | 1.87 (1.15–3.04) | 1.59 (1.24–3.32) | 1.20 (0.35–4.16) | 1.71 (0.34–4.05) |
| High | 2.84 (1.79–4.50) | 2.24 (1.35–3.72) | 3.07 (1.05–8.96) | 2.96 (1.01–8.65) |
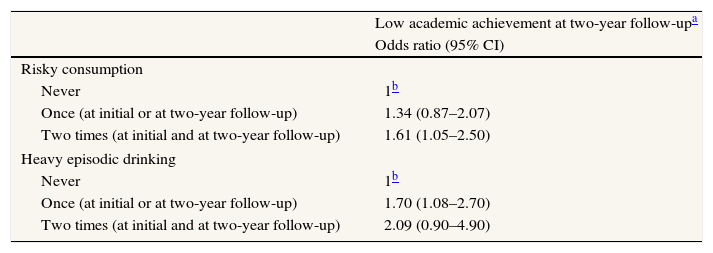
Influence of risky consumption and heavy episodic drinking on academic achievement
| Low academic achievement at two-year follow-upa | |
| Odds ratio (95% CI) | |
| Risky consumption | |
| Never | 1b |
| Once (at initial or at two-year follow-up) | 1.34 (0.87–2.07) |
| Two times (at initial and at two-year follow-up) | 1.61 (1.05–2.50) |
| Heavy episodic drinking | |
| Never | 1b |
| Once (at initial or at two-year follow-up) | 1.70 (1.08–2.70) |
| Two times (at initial and at two-year follow-up) | 2.09 (0.90–4.90) |
One out of four subjects that did not present RC at initial study does show it at two-year follow-up. Up to our knowledge, this proportion is among the higher ever cited in literature (Schulenberg et al18 have reported about 20%). In our study, the condition of being male, having a non-abstainer mother, and the early age of onset of use and high positive expectancies are associated with the higher rates, near 50%. Further study more, the higher incidences of onset of RC occur among categories of subjects that presented higher prevalence at initial study. This contributes for the expansion of prevalence of RC at two-year follow-up.
The prevalence of RC at two-year follow-up is also higher than at initial study, while prevalence of HED is lower than at initial study. These results suggest that HED is associated with adolescents and RC with young subjects. According to Jackson et al.30 and to Windle et al.31 adolescents' HED reaches its peak around 20 years-old and then tends to stabilize or decrease. Another longitudinal study has reported diminished relative risk for binge drinking over time for 12- to 20-year-old males.23
The prevalence of RC at two-year follow-up shows average increases of 50% on all variables, except for variables “age of onset of use” and “positive expectancies”, that show increases of 100% (table 3). These results are consistent with different studies.12,32
The prevalence of HED shows more marked decreases among categories of subjects with higher prevalence at initial study, except for the variable “positive expectancies”. Furthermore, among subjects with higher positive expectancies, the HED prevalence diminishes only 20%, opposite to the decrease of 30% showed by all subjects (table 3). Once more, the results of this work underline the role of positive expectancies in establishing and maintaining different patterns of alcohol consumption.
Both, socio-demographic characteristics and alcohol expectancies are associated with incidence of RC and with incidence of HED.
In relation to gender, at two-year follow up, opposite to initial study results, “being male” becomes a risk factor for incidence of RC, despite of the lower cut-off point used for RC in females. In line with these results, a work with Turkish college students has informed that alcohol use was predicted by being male33 and another Swedish study informed that being male has been related to frequent high alcohol consumption.34
Living with their parents is a protective factor for incidence of RC. However, this protective effect is lower at two-year follow-up (OR=0.48) than at initial study (OR=0.39).11 In contrast, this variable does not show an effect on incidence of HED.
The association found between the maternal educational level and the incidence of RC at two-year follow-up is similar as at initial study.11 It indicates that higher maternal educational level is still a risk factor for RC at early adulthood.
The observed association between early age of onset of alcohol use and incidence of RC or incidence of HED could be explained by tolerance generated by alcohol use. Other possible explanation for this association could be that the parents who “permit” alcohol use at an earlier age are also more likely to be more permissive with excessive consumption.9,10
The relationship between positive expectancies and alcohol consumption is similar to the one found at initial study. These results are consistent with those described in several studies, even though they have used different measurement scales for expectancies.
Finally, our results show that RC and HED are associated with low academic achievement. Inconsistent with these results, teacher-rated poor academic ability has been considered a predictor of adolescent HED among both women (OR=1.17, p<0.05) and men (OR=1.22, p<0.001).17 However, other study observed association between adolescent high HED and usual grades in school among men (OR=0.510, p<0.01) but not among women (OR=0.828, p>0.05).31
This lower achievement could be attributed to the confusion introduced by less academic effort of subjects who present these patterns of consumption. However, the fact that the models have been adjusted for grade of university access exam suggests absence of this confusion. Further, neuropsychological and psychophysiological evaluation of the subjects at two-year follow-up will facilitate the identification of the extension at which this lower academic achievement can be attributed to the neurocognitive consequences of alcohol consumption.
There are two possible limitations in our study: (1) Selection bias, because of the loss of subjects in the follow-up. However, the absence of significant differences between the initial sample and the follow-up sample (table 1) suggests absence of this bias. (2) Given that the question about expectancies is not specifically validated, expectancies may have not been correctly measured.
Our results show that HED in Spain is a pattern of alcohol consumption mainly associated with adolescence, while RC is associated with youth. Both patterns are predictors of academic achievement. Public Health strategies should focus on modifying expectancies and limit access to alcohol at young ages.
FundingThis research was supported by Consellería de Innovación e Industria, Xunta de Galicia, grant number PGIDIT05CS021103PR and INCITE08XIB211015PR, by Plan Nacional sobre Drogas, Ministerio de Salud y Consumo, Spain, grant number 2005/PN014, and by Ministerio de Ciencia e Innovación, Spain, grant number EDU2008-03440.
The authors N. Mota and A. Crego hold a predoctoral scholarship from Consellería de Innovación e Industria, Xunta de Galicia, and from Ministerio de Educación, Spain (grant number AP2006-03871), respectively.
Author contributionsF. Cadaveira, M. Corral, F. Caamaño-Isorna and S. Rodríguez Holguín have designed the study. A. Crego, M. Parada, N. Mota and R. Álvarez-Gil have collected data. F. Caamaño-Isorna and R. Álvarez-Gil have analysed and interpreted data. R. Álvarez-Gil and N. Mota have written the article. F. Caamaño-Isorna has approved the final version for publication.
Conflict of interestNo conflicts of interest.











