



Alcohol consumption is one of the main health and social problems in Ecuador. The aim of this study was to explore gender differences in the prevalence and psychosocial profile of problematic consumers among university students.
MethodWe surveyed 3,232 students by using the AUDIT and psychosocial scales. To discriminate the explanatory value of each variable, a CHAID segmentation analysis was used.
ResultsThe prevalence of alcohol consumption was 92.24% in men and 82.86% in women. In total, 49.73% of men and 23.80% of women reported problematic consumption. In men, the profile of problematic consumption was defined by higher scores in anxiety and depression, especially if they showed higher levels of psychological stress and lower life engagement. In women, problematic consumption showed a tendency towards psychological inflexibility, especially in those with lower life engagement.
ConclusionThere is a need to prioritise attention to alcohol consumption in university students and to design different interventions for men and women.
El consumo de alcohol constituye un problema de salud pública en Ecuador. El objetivo de este estudio es analizar la prevalencia y el perfil de consumo de alcohol en estudiantes universitarios.
MétodoSe encuestó a 3232 estudiantes a través del AUDIT y escalas psicosociales. Para discriminar el valor explicativo de estas sobre el consumo se utilizó un análisis CHAID.
ResultadosLa prevalencia total de consumo fue del 92,24% en los hombres y del 82,86% en las mujeres. En total, el 49,73% de los hombres y el 23,80% de las mujeres reportaron un consumo problemático. En los hombres, el perfil de consumo problemático se caracterizó por síntomas de ansiedad y depresión, especialmente si existía mayor nivel de estrés y menor compromiso vital. En las mujeres, el consumo problemático se caracterizó por mayor inflexibilidad psicológica y menor compromiso vital.
ConclusiónEl consumo de alcohol en estudiantes universitarios requiere atención y el diseño de intervenciones específicas según el sexo.
Alcohol is the most widely consumed psychoactive drug in the Western world.1 Among the main factors related to risky alcohol consumption, age,2 gender,3 and coping mechanisms4 have drawn special attention. However, the specific profile which discriminates problematic alcohol consumption −considered hazardous or harmful for your health or for psychosocial functioning according to WHO guidelines5− remains unclear.
The aim of this study is to explore gender differences in the prevalence and psychosocial profile of problematic consumers in university students.
MethodDesign and procedureA descriptive and cross-sectional study was done under the Helsinki Declaration ethical guidelines. Alcohol consumption and psychosocial variables were surveyed online using scales translated and/or adapted from the original versions to Ecuadorian Spanish. Once the participant logged in as a student at the university, a reminder to complete the survey was displayed for one month. A consent form preceded the survey explicitly guarantying anonymity and a brief results report was provided for their records in order to enhance commitment with forthright answers.
ParticipantsThe total sample consisted of 5,500 college students enrolled at a university in the south of Ecuador. The final sample was composed by 3,232 students who completed the survey (58.7% of the total enrollment). A total of 1,522 were men (average age of 21.62+3.51) and 1,710 women (average age of 20.85 +3.27).
Instruments- •
Alcohol Use Disorders Identification Test (AUDIT, Self-report version).5 This scale evaluates alcohol consumption. Scores range from 0 to 40. Higher scores indicate higher risk of problematic alcohol consumption.
- •
Type A Behavior Scale.6 It measures competitive drive, intense striving for achievement, hostility, aggressiveness, impatience and exaggerated sense of time urgency, associated with cardiovascular disorders and premature death. Scores range from 0 to 10. Higher scores indicate higher tendency towards personality type A.
- •
UCLA Loneliness Scale Revised-Short.7 It evaluates the subjective feeling of loneliness, lack of emotional support or significant relationships compared to the desired one. Scores range from 0 to 9. Higher scores indicate a greater degree of loneliness.
- •
Avoidance and Action Questionnaire (AAQ-7).8 It measures psychological flexibility/inflexibility. Scores range from 7 to 49. Higher scores indicate greater psychological inflexibility.
- •
Life Engagement Test (ELT)t.9 It measures vital commitment or degree to which the person is engaged in activities that are meaningful to them. Scores range from 6 to 30. Higher scores indicate a greater value guided life (life engagement).
- •
Perceived Stress Scale (PSS-14).10 It evaluates the degree to which situations in a person's life are considered stressful, in terms of unpredictability, uncontrollability and overload. Scores range from 0 to 64. A higher score indicates a greater stress level.
- •
Patient Health Questionnaire of Depression and Anxiety (PHQ-4).11 It assess depression and anxiety associated with functional impairment and disability days. Scores range from 0 to 12. A higher score indicates a greater anxiety and depression level.
- •
Satisfaction Life Question (LSQ).12 “How satisfied are you with your life as a whole nowadays?”. Scores range from 0 to 10. A higher score indicates higher satisfaction.
Participants were divided into three groups based on the AUDIT's cut-offs: non-consumers (AUDIT=0); non-problematic alcohol consumption (AUDIT ≤16); problematic alcohol consumption −hazardous, harmful or dependent consumption− (AUDIT >16). Chi-squared test and ANOVA were conducted with an adjusted significance level of p 0.05 and 0.01.
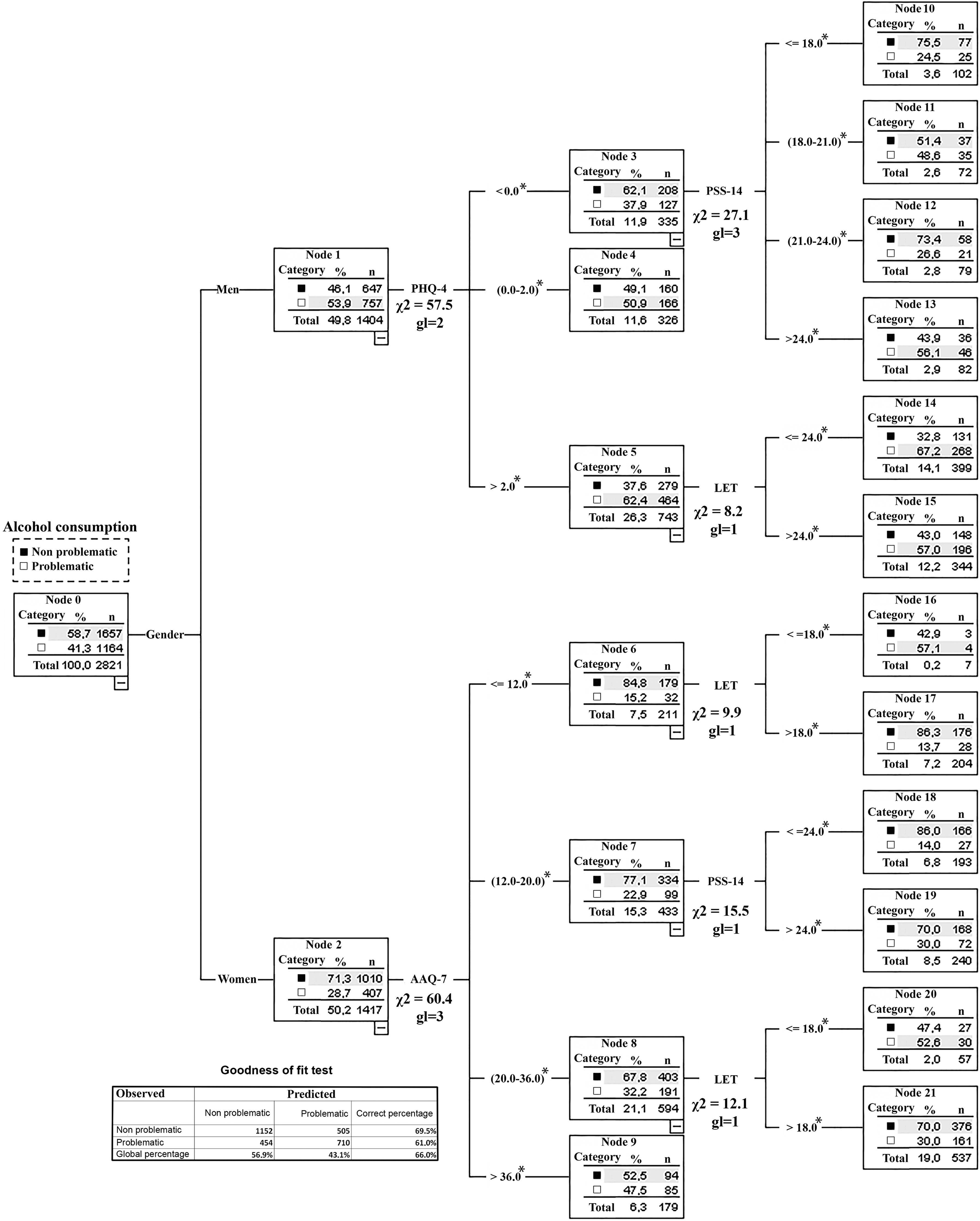
In order to establish the discriminatory power of each of the scales for non-problematic and problematic consumers, a CHAID (Chi-squared Automatic Interaction Detection) analysis was conducted. This test provides cut-offs for each scale defining the best-fit profile for both groups. All the statistical analysis were made using the statistical package SPSS (vs. 15.0).
ResultsPrevalence of alcohol consumption in men and womenA total of 12.7% (n=411) students did not consume alcohol, 7.7% among men and 17.1% among women; 51.3% (n=1,657) consumed moderately (non-problematic), 42.5% among men and 59.1% among women; and 36% (n=1,164) reported problematic consumption: 27.4% hazardous consumption, 4.7% harmful consumption and 3.9% dependent, based on AUDIT categories. In fact, 49.7% of men and 23.8% of women reported problematic alcohol consumption.
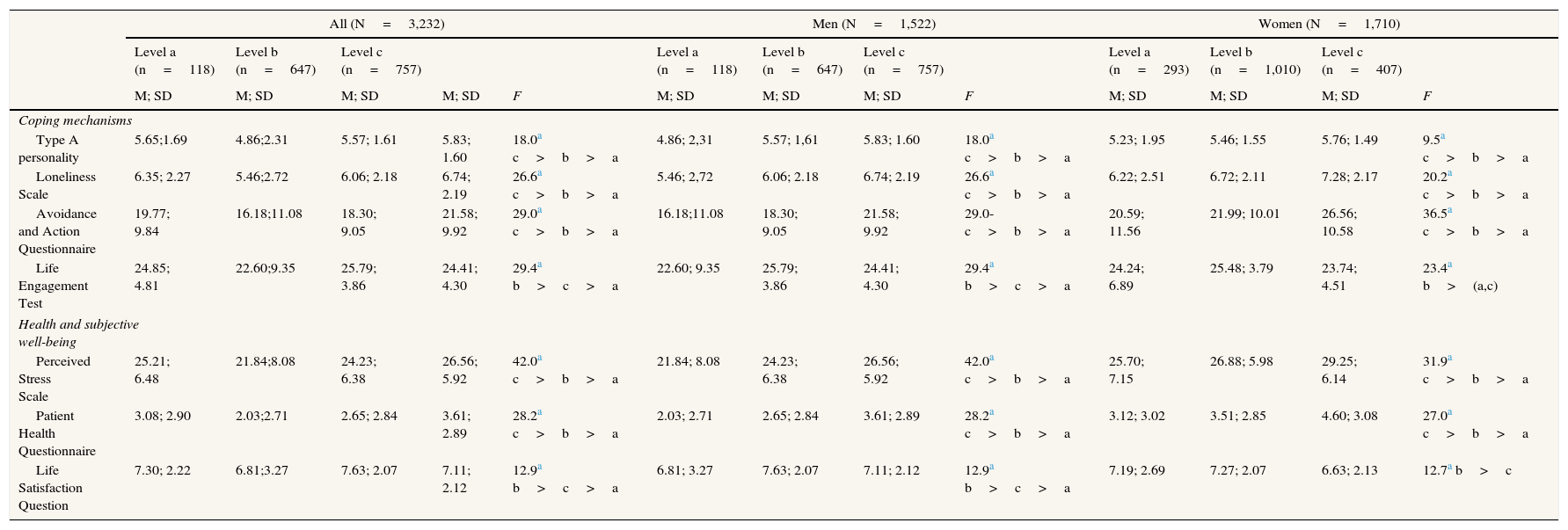
Table 1 shows the distinct profile of psychosocial variables for men and women with no alcohol consumption, non-problematic consumption, and problematic consumption.
Differences in psychosocial variables depending on gender and the level of alcohol consumption.
| All (N=3,232) | Men (N=1,522) | Women (N=1,710) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Level a (n=118) | Level b (n=647) | Level c (n=757) | Level a (n=118) | Level b (n=647) | Level c (n=757) | Level a (n=293) | Level b (n=1,010) | Level c (n=407) | |||||
| M; SD | M; SD | M; SD | M; SD | F | M; SD | M; SD | M; SD | F | M; SD | M; SD | M; SD | F | |
| Coping mechanisms | |||||||||||||
| Type A personality | 5.65;1.69 | 4.86;2.31 | 5.57; 1.61 | 5.83; 1.60 | 18.0a c>b>a | 4.86; 2,31 | 5.57; 1,61 | 5.83; 1.60 | 18.0a c>b>a | 5.23; 1.95 | 5.46; 1.55 | 5.76; 1.49 | 9.5a c>b>a |
| Loneliness Scale | 6.35; 2.27 | 5.46;2.72 | 6.06; 2.18 | 6.74; 2.19 | 26.6a c>b>a | 5.46; 2,72 | 6.06; 2.18 | 6.74; 2.19 | 26.6a c>b>a | 6.22; 2.51 | 6.72; 2.11 | 7.28; 2.17 | 20.2a c>b>a |
| Avoidance and Action Questionnaire | 19.77; 9.84 | 16.18;11.08 | 18.30; 9.05 | 21.58; 9.92 | 29.0a c>b>a | 16.18;11.08 | 18.30; 9.05 | 21.58; 9.92 | 29.0- c>b>a | 20.59; 11.56 | 21.99; 10.01 | 26.56; 10.58 | 36.5a c>b>a |
| Life Engagement Test | 24.85; 4.81 | 22.60;9.35 | 25.79; 3.86 | 24.41; 4.30 | 29.4a b>c>a | 22.60; 9.35 | 25.79; 3.86 | 24.41; 4.30 | 29.4a b>c>a | 24.24; 6.89 | 25.48; 3.79 | 23.74; 4.51 | 23.4a b>(a,c) |
| Health and subjective well-being | |||||||||||||
| Perceived Stress Scale | 25.21; 6.48 | 21.84;8.08 | 24.23; 6.38 | 26.56; 5.92 | 42.0a c>b>a | 21.84; 8.08 | 24.23; 6.38 | 26.56; 5.92 | 42.0a c>b>a | 25.70; 7.15 | 26.88; 5.98 | 29.25; 6.14 | 31.9a c>b>a |
| Patient Health Questionnaire | 3.08; 2.90 | 2.03;2.71 | 2.65; 2.84 | 3.61; 2.89 | 28.2a c>b>a | 2.03; 2.71 | 2.65; 2.84 | 3.61; 2.89 | 28.2a c>b>a | 3.12; 3.02 | 3.51; 2.85 | 4.60; 3.08 | 27.0a c>b>a |
| Life Satisfaction Question | 7.30; 2.22 | 6.81;3.27 | 7.63; 2.07 | 7.11; 2.12 | 12.9a b>c>a | 6.81; 3.27 | 7.63; 2.07 | 7.11; 2.12 | 12.9a b>c>a | 7.19; 2.69 | 7.27; 2.07 | 6.63; 2.13 | 12.7a b>c |
M: median; SD: standard deviation.
Level a: no alcohol consumption; level b: non-problematic alcohol consumption; level c: problematic alcohol consumption.
Problematic consumption among men increases as the score in the PHQ-4 increases as well. Among those who scored 0 points in the PHQ-4 (n=335), problematic consumption was 37.9% (n=127) of the subjects. Among those who scored between 1 and 2 points, it was 50.9% (n=166). Finally, 62.4% (n=464) of those who scored more than 2 points (n=743) showed problematic consumption.
On the other hand, among those who scored 0 in the PHQ-4, the highest percentage of men with problematic consumption (56.1%; n=46) were the ones with more than 24 points (n=82) in the Perceived Stress Scale (PSS). Moreover, among the ones who scored more than 2 points in the PHQ-4 (n=743) and had a lower vital commitment (under 24), the consumption risk was higher (67.2%; n=268) than among those with higher vital commitment (57.0%; n=196).
Profile of problematic alcohol consumption in womenIn women (n=1,417), the percentage of problematic consumption increases as the score in psychological inflexibility (AAQ) also increases. Among those with 11 points or less (n=211), problematic consumption is 15.2% (n=32), while among those with more than 36 points (n=179), problematic consumption is 47.5% (n=85).
Lower vital commitment (less than 18 points) was associated with a greater proportion of problematic consumption among those who scored in the 20-36 interval in the AAQ, 52,6% (n=30) of the subjects. Meanwhile, women who scored in the 12-20 interval (AAQ) had a higher percentage of alcohol consumption when the score in the PSS exceeded 24 points (Fig. 1).
Discussion
At least one in three students reported problematic consumption and the rate found in men doubles that of women. This gender difference was higher than in other countries, maybe due to sociocultural gender roles differences.13 Interventions in Ecuadorian university students are encouraged in order to prevent the personal and social costs that problematic alcohol consumptions entails.1–3 Problematic alcohol consumption among men was characterized by a higher psychological stress,14 ineffective coping mechanisms focus on avoid aversive thoughts–psychological inflexibility15–, anxious Type A personality, and loneliness.4
Reduce problematic alcohol consumption in men requires promote strategies based on stress reduction and management, social support and value based action like in 12-step programs.
In women, problematic alcohol consumption was strongly associated with psychological inflexibility or ineffective coping mechanism to deal with life circumstances. Women will also benefit from interventions aim to promote the ability to distance oneself from aversive thoughts and emotions, without avoiding the here and now.
Preventive and treatment interventions would be justified both in women and men in Ecuadorian university population. Baseline seems especially severe in men although different cut-offs may be necessary when establishing the problematic consumption level in both sexes.
Given the cross sectional nature of the study, generalization of findings must be viewed with caution. Future research should complete these data with more universities in the country and data collection methods.
A growing number of research highlights the importance of psychosocial variables in alcohol consumption. However, designing and implementing interventions for the prevention of alcohol consumption according to gender is an issue that is being discussed.
What does this study add to the literature?The results of this study support the need to create gender differentiated programs. Problematic alcohol consumption in men was associated with higher stress levels, anxiety and depression symptoms, and lower vital commitment. In women, associated with a tendency of avoiding emotions or aversive thoughts, especially among those with lower vital commitment.
Napoleón Pérez-Farinós.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsP. Ruisoto has contributed to the project conception, design and data collection, as well as writing the article. R. Cacho has contributed to the writing and critical review with important intellectual contributions. J.J. López-Goñi has led the result analysis and interpretation, writing the article, critical review and approval of the final version for publishing. S. Vaca and M. Jiménez have contributed to the project conception and data collection.
FundingThis study was fully funded as a selected Program of Research and Innovation by the Universidad Técnica Particular of Loja (Ecuador).
Conflict of interestNone.
The authors wish to thank the National Secretariat of Higher Education, Science, Technology and Innovation (SENESCYT) of the Republic of Ecuador for their support through the Prometeo Project











