



Over the past thirty years the interest in and application of participatory research methods in public health research has grown considerably. A common theme in participatory research is that it breaks down the objectification of the people being studied and strives to involve those with whom the research is being conducted on more equal terms than is the case with traditional public health research. Participatory action research (PAR) “seeks to understand and improve the world by changing it. At its heart is collective, self-reflective enquiry that researchers and participant's undertake so they can understand and improve upon the practices in which they participate and the situation in which they find themselves”.1 In public health PAR is also frequently, and especially in the US, referred to as community-based participatory research (CBPR).2 PAR holds great, and as yet largely unrealised promise, to create greater mobilisation and community interest and action on health inequities and action on the social determinants of health.
OriginsThe use of PAR in public health comes from various traditions. Freire3 developed PAR in adult education in low income countries to support participatory adult learning. This research encouraged poor and deprived communities to examine and analyse the structural reasons for their oppression Freire developed the idea of praxis: “reflection and action on the world in order to transform it”.3 His work was aimed at radical change in societal power structures to empower people who had little power within the status quo. PAR also draw on Lewin's4 work in the 1940s which applied PAR to organisational change and was less transformation of the status quo than Freire. Like these two traditions of PAR the use of PAR in public health various in the extent to which it is transformative rather than adaptive.
Uses and methodsPAR has been applied to a wide range of issues in public health. These include community asset mapping, participatory evaluation of public health programs, community monitoring of health service quality, research documenting and advocating to remove threats to health including poor water and sanitation and environmental pollution and participatory health policy research. PAR can be used with community members, health service workers and policy makers. A systematic review indicated most health service PAR has been conducted in low and middle income countries.5 In high income countries it is often used as a method to empower groups who are excluded and hold little power including Roma peoples in Europe6 and Indigenous peoples in Canada and Australia.7 PAR is often not reported in the academic literature despite application to local projects.8
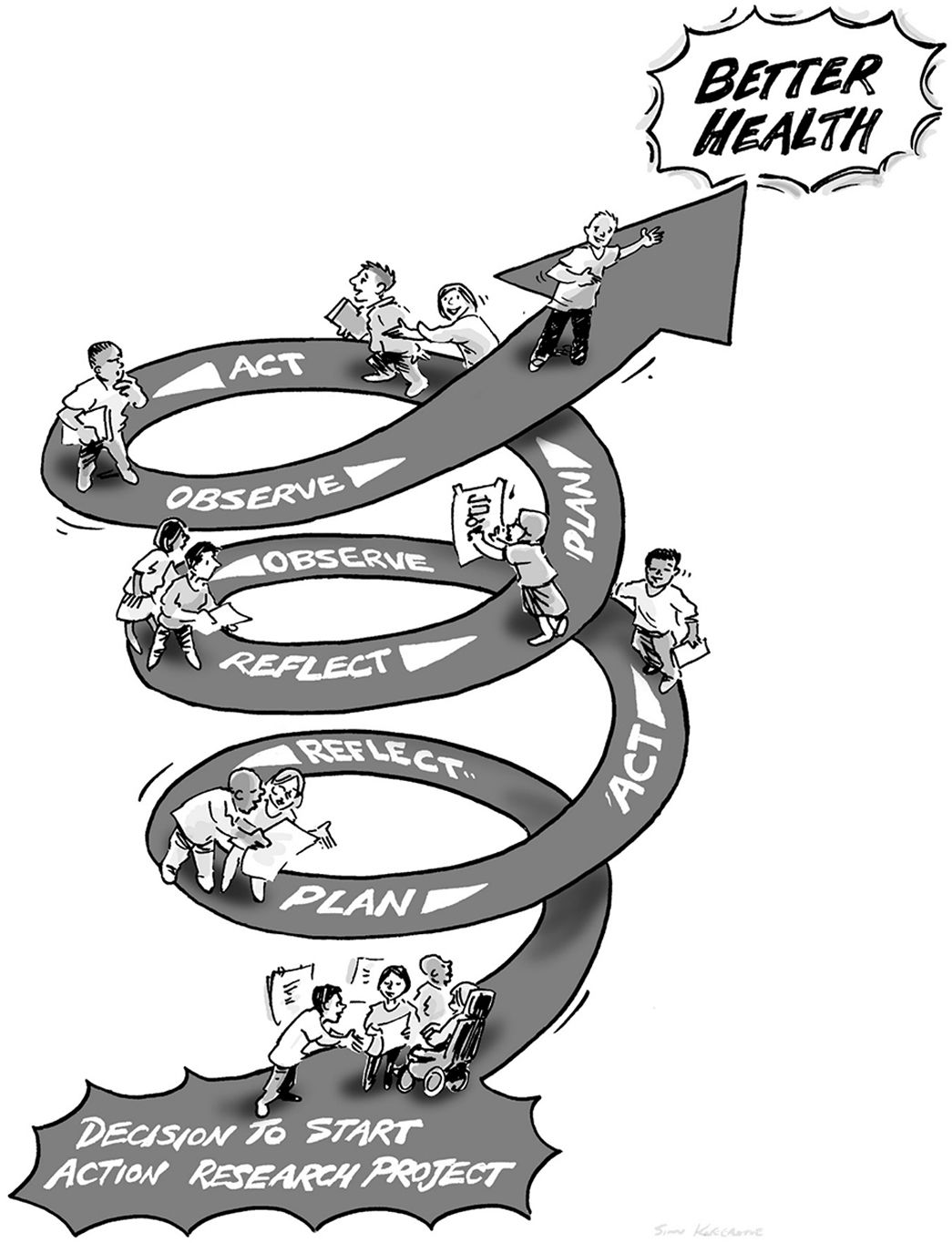
The most important aspect of PAR is that it relies on a cycle of reflection, planning, acting, further observing and reflection, then new plans and action (Fig. 1). This reflexivity is central and is deeply relational in that the researchers and the other actors (community members or service or policy players) are engaging together in these processes. PAR can use a range of qualitative and quantitative methods. A PAR initiative conducted in the North West Amazonian region of Brazil9 working with a Indigenous community to address a sanitation problems detailed the application of the following methods showing the range that can be used: questionnaires, interviews, participant observation, talking maps, photo panels, geo-referencing of water and sanitation, copro-parasitological investigations of residents, study of composition and disposal of solid waste, analysis of soil samples, demands and petitions, community newspapers, and training workshops. The authors of this study noted the tension present in most PAR exercises of juggling methodological rigour with the perspectives of the community. Many authors (for example see collection in Wallerstein et al.) have noted this tension which goes to the heart of the question of knowledge and truth and objectivity and subjectivity. Public health research has traditionally drawn on a positivist tradition which assumes an objective and verifiable truth. In this view those who are the focus of research are viewed as passive subjects who are studied and reported on but not involved in the research at all. This tradition of public health research has been questioned both in terms of the extent to which can ever be objective and free of the bias of researchers and in terms of how it objectifies and de-powers groups of people. One of the strongest challenges to these traditional research approaches in public health has come from Indigenous peoples. They have reported being exploited by outside researchers who have often not understood cultural and community practices or valued Indigenous knowledges.10 PAR offers a promising framework within which to involve such groups in the conception, conduct and evaluation of research who have previously been the subject of research in but who feel they and their communities have benefited little.
Participatory action research and power
Despite the promise of PAR in public health as more experience has been gained theoretical, methodological and political questions have been raised about its application and contribution to improving health and health equity. Here I will address the issues concerning power as a central issue for public health researchers to consider because they are important to PAR which is seeking to redress inequities through action on social determinants.
Power concerns theory because of the question of whose world view dominates in the research. For example, Indigenous researchers have called for decolonised research practices which challenge the powerless position Indigenous peoples are ascribed by many dominant cultures. If PAR is viewed simply as a mean for researchers to gain greater co-operation in their research and does not involve a sharing of power and control then the empowering potential of the research is reduced. Lazarus et al.11 note that it is important for PAR to “honour both academic and community-bedded or indigenous knowledges in order to realign the power dynamics”. If PAR is to empowering for communities it needs to value (rather than pay lip service) to lay knowledge.12 This acceptance of different knowledges requires researchers to relinquish their position as the sole “experts” and accommodate their paradigms of thinking to those of others.
Power also concerns method and the extent to which the processes of designing and conducting the research are truly participatory. On the basis of a systematic review of article on participatory research in health George et al.5 concludes that only a very small proportion of the studies were fully participatory and that there were “significant shortfalls in the participatory intent of most articles” and that “few articles discussed power or control in developing and implementing their participatory interventions with communities”. In a rare article the dilemmas of being a community researcher in a PAR study of health and poverty in ethnically mixed areas of east London were examined. While community researchers reported gaining some personal empowerment they found a conflict between their role as researcher and community member and found it difficult to practice reflexivity pointing to the need for increased institutional support for community researchers. Similar difficulties in applying PAR with Roma people in Sweden were found whereby the Roma participants were distrustful of existing civic institutions because of a history of discrimination and resultant powerlessness.13 More attention is required to examining, negotiating and challenging power in the process of conducting PAR. Jagosh et al., 14 based on a realist review of PAR research, note the importance of process in PAR and how it can lead to capacity building, self-empowerment and infrastructure development. They also note that conflict in PAR processes is healthy and that the processes, if working well, will also feature resistance, negotiation in order to build the necessary consensus and trust to conduct research and take action on its basis. PAR is the only method available to public health researchers that will uncover power dynamics and give voice to groups who are excluded by the social and economic processes of the dominant society such as Roma, people with disabilities and Indigenous peoples.
Finally, the politics of PAR need greater consideration. PAR has been promoted in public health as a mean of taking action to reduce health inequities. Public health research has long been criticised for focusing too much on understanding problems and not enough on solving them.15 Kemmis and McTaggart16 maintains that a crucial feature of PAR is its ability to open “communicative space” between participants. They see that in this space critical perspectives are developed and then, informed by cycles of reflection and observation, action can be tested in terms of its ability to bring about change. Inevitably, when PAR is used to research actions designed to reduce inequities engagement in political processes is required to bring about change. Public health researchers may be reluctant to be involved in such action. Yet if they are committed to participatory approaches for change then evidence indicates that long-term engagement in the issue and with community, service or policy partnerships will be required.17 Yet funding bodies and Universities practices rarely encourage such long term engagement. Time-limited projects and academic publications are more valued than achieving social and economic change. One solution is for researchers to become activist-researchers and engage in longer term struggles as members of social movements such as the People's Health Movement (www.phmovement.org) or ALAMES (www.alames.org). Political science is clear that policy change rarely reflects evidence alone. At its best PAR can use evidence to influence political process and change power balances in order to bring about policy change for health equity.18 This is most likely to happen when the limitation of evidence is accepted by the PAR participants and the need for political engagement accepted.19
Freudenberg and Tsui19 note that the local focus of many PAR initiatives is a considerable constraint to participants addressing the structural causes of health inequities. They note many of these may not be transparent in local settings and are often rooted in corporate power and national economic arrangements. It is for this reason that Freire3 focused much of his PAR work on encouraging people to understand and unpack the root cause of their oppression and powerlessness. The implications of this is that PAR seeking to challenge existing political power structures will benefit from Freire consciousness raising as part of the process so that local health concerns are linked with their structural causes rather than seen as the product of individual behaviour. PAR is the only empirical method available to public health that will allows such wide-ranging assessments of complex realities and policy and political engagement. As such it is vital that public health researchers embrace PAR and use it to increase the empowerment and social change potential of their research.
Authorship contributionsThe author is entirely responsible for conceiving and writing the editorial.
FundingNone.
Conflicts of interestNone.











