




It has been established in the literature that workers within public organisations are intrinsically motivated. This paper is an empirical study of the healthcare sector using methods of qualitative analysis research, which aims to answer the following hypotheses: 1) doctors are intrinsically motivated; 2) economic incentives and control policies may undermine doctors’ intrinsic motivation; and 3) well-designed incentives may encourage doctors’ intrinsic motivation.
MethodWe conducted semi-structured interviews à-la-Bewley with 16 doctors from Navarre's Healthcare Service (Servicio Navarro de Salud-Osasunbidea), Spain. The questions were based on current theories of intrinsic motivation and incentives to test the hypotheses. Interviewees were allowed to respond openly without time constraints. Relevant information was selected, quantified and analysed by using the qualitative concepts of saturation and codification.
ResultsThe results seem to confirm the hypotheses. Evidence supporting hypotheses 1 and 2 was gathered from all interviewees, as well as indications of the validity of hypothesis 3 based on interviewees’ proposals of incentives.
ConclusionsThe conclusions could act as a guide to support the optimal design of incentive policies and schemes within health organisations when healthcare professionals are intrinsically motivated.
Ha sido establecido por la literatura que los trabajadores de las organizaciones públicas están intrínsecamente motivados. Este trabajo es un estudio empírico en el sector sanitario que utiliza métodos de investigación del análisis cualitativo, cuyo objetivo es tratar de dar respuesta a las siguientes hipótesis: 1) los médicos son agentes motivados intrínsecamente, 2) los incentivos económicos y las políticas de control pueden minar la motivación intrínseca de los médicos, y 3) los incentivos bien diseñados pueden impulsar la motivación intrínseca de los médicos.
MétodoRealizamos entrevistas semiestructuradas à-la-Bewley a 16 médicos del Servicio Navarro de Salud-Osasunbidea. Las preguntas fueron diseñadas siguiendo las teorías existentes sobre motivación intrínseca e incentivos, y con el objetivo de responder a las hipótesis planteadas. Los entrevistados tuvieron la oportunidad de contestar a las preguntas sin restricción de tiempo. La información relevante para el objetivo del estudio fue seleccionada, cuantificada y analizada siguiendo los conceptos cualitativos de codificación y saturación.
ResultadosLos resultados parecen confirmar las hipótesis formuladas. Todos los entrevistados aportaron evidencia indicando la validez de las hipótesis 1 y 2. También se obtuvieron diferentes propuestas de incentivos por parte de todos los entrevistados que indican la validez de la hipótesis 3.
ConclusionesLas conclusiones pueden ser una guía en el diseño de sistemas y políticas de incentivos óptimos en el seno de las organizaciones sanitarias cuando los profesionales médicos están intrínsecamente motivados.
In standard incentive theory, it is widely assumed that agents’ choices depend only on the monetary payments with which they are rewarded. This is known as the price effect, which for many decades, economic theorists have considered to be the only tool able to incentivize economic agents. This rationalization of the economic behaviour has been challenged in recent decades by behavioural economics (BE).1 An extensive number of academic works coming from BE have established that economic agents also make their decisions based on other non-monetary motivations such as social preferences, reciprocity, and ethical values. The existence of such non-monetary motivations may have lead decision makers and managers to predict economic agents’ behaviour poorly and to design poor incentive policies.
Intrinsic motivation has been one of the most studied non-monetary incentives within BE.2–4 BE has established that monetary rewards and intrinsic motivation interact sometimes as substitutes (when incentives adversely affect agents’ intrinsic motivation), and sometimes as complements (when incentives positively affect agents’ intrinsic motivation).3 BE calls the former the crowding-out effect and the latter the crowding-in effect. This interplay between monetary rewards and agents’ intrinsic motivation has also been studied within self determination theory (SDT).5–7 As seen within an SDT framework, individuals are intrinsically motivated because they gain enjoyment from the mere fact of doing an activity, or they get utility from the feelings of acting autonomously or are self-motivated rather than controlled by externally imposed rewards or contingencies.8–10 Large empirical studies within an SDT framework have also demonstrated that extrinsic rewards and contingencies may crowd out the intrinsic motivation.5,6 However less attention has been paid to the crowding-in effect despite there being empirical work showing its existence.3
A large body of literature addresses the topic of workers’ non-monetary motivations in the context of public and non-for-profit organisations.11–18 In the context of health organisations some papers analyse optimal incentives when doctors’ are intrinsically motivated or have altruistic preferences.18–21 To our knowledge, however, only one such study is empirical.19 This work focuses on finding empirical evidence about doctors’ intrinsic motivation and also about crowding-out and crowding-in effects. A number of papers have been concerned with establishing a framework for the intrinsic motivation of health-care professionals.18–21 Within this framework, we seek to test the following hypotheses: 1) doctors are intrinsically motivated agents, 2) financial incentives and control and command policies may crowd out doctors’ intrinsic motivation, and 3) well designed incentives may crowd in doctors’ intrinsic motivation.
The contribution of this study is twofold:
- •
It is new empirical research on the topic of incentives and intrinsic motivation in the context of health organisations.
- •
It introduces qualitative analysis to the study of incentives for physicians in Spanish health organisations.
We performed in-depth semi-structured interviews á-la-Bewley to physicians at Servicio Navarro de Salud-Osasunbidea (SNS-O, Spain)22 (N=16). Interviews were undertaken over a sixteen-month period starting in February 2010. The questions addressed to the doctors in the interviews were designed in order to test the hypotheses formulated above. The questions open-ended and were grounded in SDT and BE theory.
Doctors were invited to participate through a formal invitation letter. The letter briefly informed them about the interview although no details about the research goals were given to avoid biasing doctors’ answers. The letter was sent together with a document stating that the results would remain anonymous. We asked doctors to talk openly and to give their candid opinions about the health organization for which they were working.
Providing enough time and comfortable place for the interview is very important in order to obtain high-quality data. We performed most of the interviews at the doctor's workplace, usually in their personal offices at a date and time of their convenience.
The duration of the interviews ranged from a minimum of 57minutes to a maximum of 1hour and 44minutes. All interviews were performed by authors (MB and JMC) and were recorded. We also took field notes, something considered relevant to improve the quality of data. The recorded audios were transcribed to a text document. Transcripts and notes allowed all the details of the interview to be registered.
We initially used random sampling of eight interviewees from a population of senior doctors, followed by emergent sampling.24 All interviewees were doctors working at SNS-O. For the following eight cases, we used emergent sampling making new sampling decisions as we gained more knowledge about the phenomena of interest. All but one of the interviewees were senior staff, highly qualified, in high responsibility positions, and with long tenure within the health care system. They were mostly men (fourteen out of sixteen) and from a wide range of services. All but three were working in hospitals. The remaining three were working or had worked in a publicly outsourced private health care organization or in public primary care centres.
Data gathering and analysisThe information was collated and coded.23 We used three main categories: 1) intrinsic motivation (IM), 2) crowding-out (CO), and 3) crowding-in (CI).
Each code grouped homogeneous statements —observations— which directly referred to the same category. Codes where necessary were subcoded.
Codes were of two types: deductive and inductive. Deductive codes are those which have been labelled on the basis of existing theories —BE and SDT— prior to interviews. Inductive codes are those which spontaneously emerge from respondents’ statements.
A descriptive analysis and some quantification were shown within each of the three main categories. We found the frequency of each code in respondents’ discourse, and linked it back to the respondents. For each category, we also explored interactions between codes. Statements were classified into positive or normative. Positive statements are those that describe an actual situation experienced by the respondent. Normative statements are those that describe respondents’ views about how things should be in health care organizations.
We defined 32 codes where all relevant statements were included (detailed code definitions and descriptions, considering their inductive an deductive nature, are available for interested readers in the Appendix online to this article). Statements and codes have been organized in spreadsheets.
A threshold on the informative value of codes was defined based on the concepts of saturation and hierarchy.23 A code is saturated when it emerges repeatedly in a sufficient number of interviews, and always in the same explanatory or causal direction. The hierarchy criterion is applied to those codes, subcodes and subsubcodes that do not achieve saturation but are nested into other higher level codes which are already saturated.
ResultsA total number of 642 statements concerning IM and crowding effects were drawn from the 16 interviews. The total number of statements is distributed as follows: 250 for IM, 214 for CO and 178 for CI. The following sections show the results separately by category.
Intrinsic motivationAll interviewed physicians reported being intrinsically motivated. Doctors’ major explanations regarding IM were two: they enjoy or like the medical practice —Like/Enjoy— and they are vocational professionals —Vocation. We consider Like/Enjoy and Vocation the major explanations of IM because they emerge independently —they cannot be placed as subcodes of each other code.
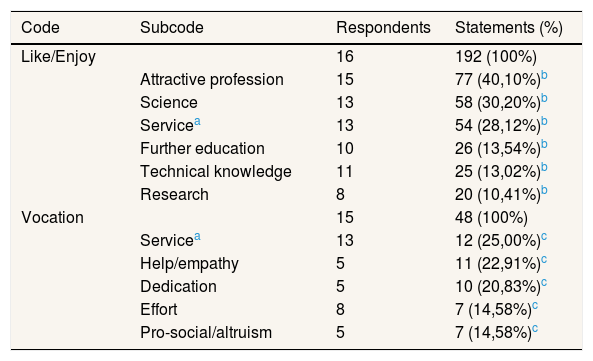
Table 1 shows the results, including relations between IM codes and subcodes. Column three shows the number of respondents who at least made one statement regarding the code or subcode displayed in the same row of the table. Column four shows the number of statements included in the code/subcode, and its percentage of appearance.
Codes of intrinsic motivation.
| Code | Subcode | Respondents | Statements (%) |
|---|---|---|---|
| Like/Enjoy | 16 | 192 (100%) | |
| Attractive profession | 15 | 77 (40,10%)b | |
| Science | 13 | 58 (30,20%)b | |
| Servicea | 13 | 54 (28,12%)b | |
| Further education | 10 | 26 (13,54%)b | |
| Technical knowledge | 11 | 25 (13,02%)b | |
| Research | 8 | 20 (10,41%)b | |
| Vocation | 15 | 48 (100%) | |
| Servicea | 13 | 12 (25,00%)c | |
| Help/empathy | 5 | 11 (22,91%)c | |
| Dedication | 5 | 10 (20,83%)c | |
| Effort | 8 | 7 (14,58%)c | |
| Pro-social/altruism | 5 | 7 (14,58%)c |
Service is classified as a subcode for both, Like/Enjoy and Vocation. This is because doctors refer to it as an important reason for both codes.
Numbers in subcodes add up more than the number in the code and percentages add up more than 100% because many statements of interviewees involve two or more subcodes. This is the case for Science and Technical Knowledge for instance.
Subcodes explaining vocation do not add up numbers above the Vocation's one nor a percentage above 100%. In this case, despite some statements were also included within two or more codes at the same time, we leave out some statements and codes which had a little incidence.
Appendix provides a detailed description of codes.
The main reasons for Like/Enjoy include Attractive Profession, Science, Service, Further Education, Technical Knowledge and Research. Most have to do with tasks featured by a technical or scientific component. We conclude that one of the main components of doctors’ intrinsic motivation is that medicine challenges their intellectual curiosity. They consider the medical profession to be a field where they can boost their scientific aspirations. For the case of Vocation, the main explanations were Service, Help/Empathy, Dedication, Effort and Pro-social/Altruism. In this case almost all reasons belonged to the “helping others” or the humanistic part of the medicine.
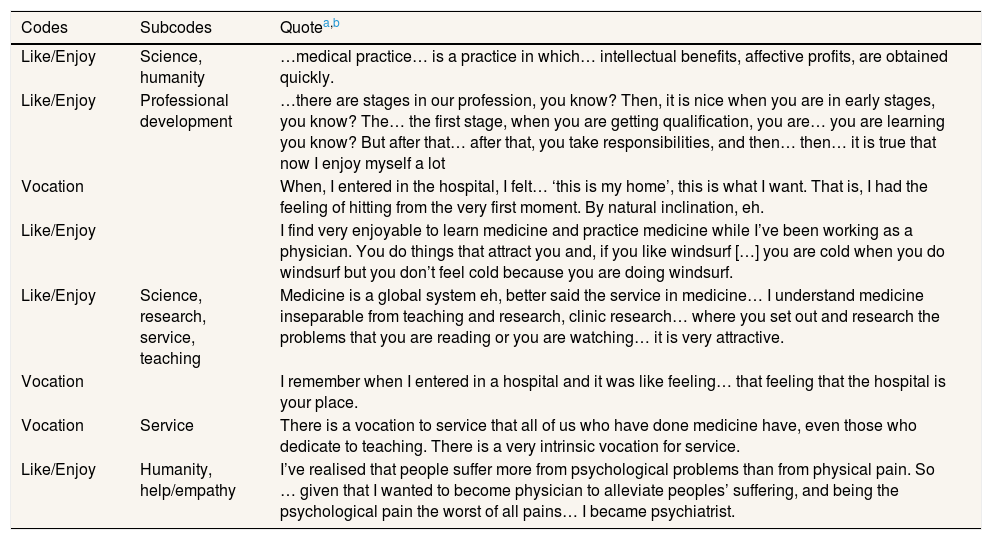
Table 2 shows a selection of representative statements relating IM jointly with the code, subcode and subsubcode to which they have been linked.
Illustrative statements of intrinsic motivation.
| Codes | Subcodes | Quotea,b |
|---|---|---|
| Like/Enjoy | Science, humanity | …medical practice… is a practice in which… intellectual benefits, affective profits, are obtained quickly. |
| Like/Enjoy | Professional development | …there are stages in our profession, you know? Then, it is nice when you are in early stages, you know? The… the first stage, when you are getting qualification, you are… you are learning you know? But after that… after that, you take responsibilities, and then… then… it is true that now I enjoy myself a lot |
| Vocation | When, I entered in the hospital, I felt… ‘this is my home’, this is what I want. That is, I had the feeling of hitting from the very first moment. By natural inclination, eh. | |
| Like/Enjoy | I find very enjoyable to learn medicine and practice medicine while I’ve been working as a physician. You do things that attract you and, if you like windsurf […] you are cold when you do windsurf but you don’t feel cold because you are doing windsurf. | |
| Like/Enjoy | Science, research, service, teaching | Medicine is a global system eh, better said the service in medicine… I understand medicine inseparable from teaching and research, clinic research… where you set out and research the problems that you are reading or you are watching… it is very attractive. |
| Vocation | I remember when I entered in a hospital and it was like feeling… that feeling that the hospital is your place. | |
| Vocation | Service | There is a vocation to service that all of us who have done medicine have, even those who dedicate to teaching. There is a very intrinsic vocation for service. |
| Like/Enjoy | Humanity, help/empathy | I’ve realised that people suffer more from psychological problems than from physical pain. So … given that I wanted to become physician to alleviate peoples’ suffering, and being the psychological pain the worst of all pains… I became psychiatrist. |
Results show that doctors are intrinsically motivated professionals. Their intrinsic motivation is sourced in two dimensions featuring the medical practice: the scientific or technical dimension and the humanistic or pro-social dimension.
Crowding-outEvidence of the CO effect was also found. We codified 214 statements referring to CO incentives. The fact that money may hurt doctors’ intrinsic motivation was widely shared by all interviewees.
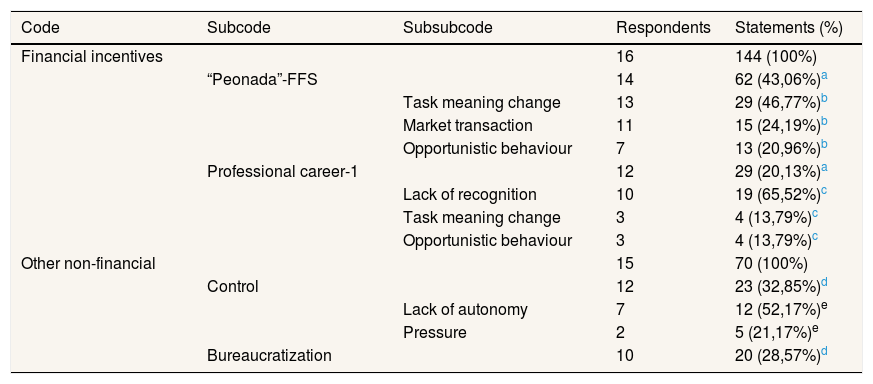
Table 3 shows the results and relevant codes explaining the CO. Columns one, two and three of the table show the code/subcode/subsubcode hierarchy. Column four shows the number of respondents who made at least one statement linked to the code or subcode in the same row. The number of statements and percentages are shown in column five.
Codes of crowding-out.
| Code | Subcode | Subsubcode | Respondents | Statements (%) |
|---|---|---|---|---|
| Financial incentives | 16 | 144 (100%) | ||
| “Peonada”-FFS | 14 | 62 (43,06%)a | ||
| Task meaning change | 13 | 29 (46,77%)b | ||
| Market transaction | 11 | 15 (24,19%)b | ||
| Opportunistic behaviour | 7 | 13 (20,96%)b | ||
| Professional career-1 | 12 | 29 (20,13%)a | ||
| Lack of recognition | 10 | 19 (65,52%)c | ||
| Task meaning change | 3 | 4 (13,79%)c | ||
| Opportunistic behaviour | 3 | 4 (13,79%)c | ||
| Other non-financial | 15 | 70 (100%) | ||
| Control | 12 | 23 (32,85%)d | ||
| Lack of autonomy | 7 | 12 (52,17%)e | ||
| Pressure | 2 | 5 (21,17%)e | ||
| Bureaucratization | 10 | 20 (28,57%)d |
All statements regarding CO were classified into two major codes: Financial Incentives and Other Non-Financial. Peonada-FFS, and Professional Career-1 are subcodes of Financial Incentives. Interviewees colloquially call “Peonada” to a Fee-For-Service (FFS) payment for working out-of-hours aimed to reduce waiting lists. The main reasons through which Peonada-FFS causes CO are captured in subcodes Task Meaning Change, Market Transaction and Opportunistic Behaviour. This means that the introduction of the FFS scheme may have caused:
- •
A change in the perception of the medical work from a vocational activity to a means for seeking extra remuneration or money (task meaning change).
- •
Doctors to start seeing the provision of health services as market interactions governed by market rules (market transaction).
- •
Doctors to behave strategically aimed at maximising their earnings (opportunistic behaviour).
Lack of Recognition, Task Meaning Change and Opportunistic Behaviour subcodes capture the main explanations of the CO nature of the Professional Career-1. The current professional career is hurting doctors’ IM because it recognizes neither the effort nor the quality of their work. This is an important result, since the so called professional career is the genuine incentive scheme in the SNS-O.
Within the non-financial causes of CO we consider two codes: Control and Bureaucratization. Statements under Control point out that doctors perceive as controlling some managerial decisions taken in the SNS-O health organizations. Doctors reported that this hurts their IM because they feel their autonomy is constrained. We group these Control statements within the subsubcode Lack of Autonomy.
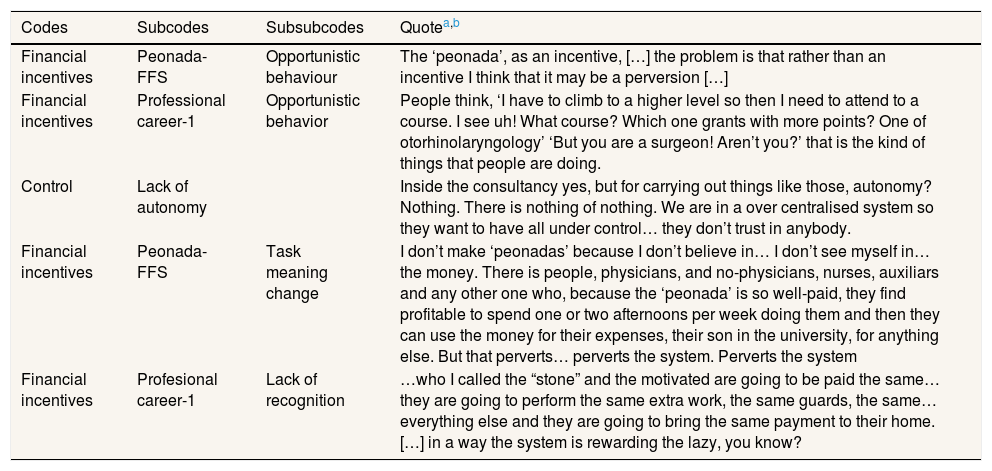
Finally, the last reason for CO reported by doctors is the Bureaucratization of the medical profession. This highlights the CO effect caused by lack of competitive stimulus, and lack of professional incentives in the context of public health organisations in the SNS-O. A selection of the most illustrative statements showing evidence of CO is shown in Table 4.
Illustrative statements of cowding-out.
| Codes | Subcodes | Subsubcodes | Quotea,b |
|---|---|---|---|
| Financial incentives | Peonada-FFS | Opportunistic behaviour | The ‘peonada’, as an incentive, […] the problem is that rather than an incentive I think that it may be a perversion […] |
| Financial incentives | Professional career-1 | Opportunistic behavior | People think, ‘I have to climb to a higher level so then I need to attend to a course. I see uh! What course? Which one grants with more points? One of otorhinolaryngology’ ‘But you are a surgeon! Aren’t you?’ that is the kind of things that people are doing. |
| Control | Lack of autonomy | Inside the consultancy yes, but for carrying out things like those, autonomy? Nothing. There is nothing of nothing. We are in a over centralised system so they want to have all under control… they don’t trust in anybody. | |
| Financial incentives | Peonada-FFS | Task meaning change | I don’t make ‘peonadas’ because I don’t believe in… I don’t see myself in… the money. There is people, physicians, and no-physicians, nurses, auxiliars and any other one who, because the ‘peonada’ is so well-paid, they find profitable to spend one or two afternoons per week doing them and then they can use the money for their expenses, their son in the university, for anything else. But that perverts… perverts the system. Perverts the system |
| Financial incentives | Profesional career-1 | Lack of recognition | …who I called the “stone” and the motivated are going to be paid the same… they are going to perform the same extra work, the same guards, the same… everything else and they are going to bring the same payment to their home. […] in a way the system is rewarding the lazy, you know? |
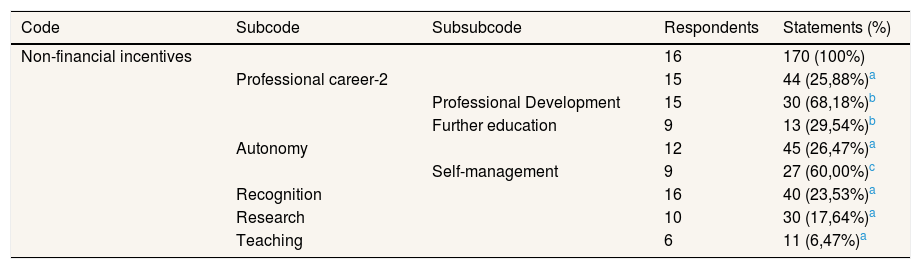
Respondents made 178 statements related to the crowding-in category. A fact that saturates rapidly is that non-financial incentives are the main ones to cause CI. Only a few experiences of crowding-in were explained in the course of interviews. However a lot of proposals and ideas of CI incentives were suggested by the interviewees.
Table 5 shows the codes explaining evidence for CI. Column four shows the number of respondents who at least made one statement linked to the code/subcode/subsubcode in the same row. Column five shows the number of statements and percentage of response in brackets. The main code explaining this category is Non-Financial Incentives which includes both, statements referring to proposals and to experiences. Statements referring to Non-Financial Incentives were classified into five main subcodes: Professional Career-2, Autonomy, Recognition, Research and Teaching.
Codes of crowding-in.
| Code | Subcode | Subsubcode | Respondents | Statements (%) |
|---|---|---|---|---|
| Non-financial incentives | 16 | 170 (100%) | ||
| Professional career-2 | 15 | 44 (25,88%)a | ||
| Professional Development | 15 | 30 (68,18%)b | ||
| Further education | 9 | 13 (29,54%)b | ||
| Autonomy | 12 | 45 (26,47%)a | ||
| Self-management | 9 | 27 (60,00%)c | ||
| Recognition | 16 | 40 (23,53%)a | ||
| Research | 10 | 30 (17,64%)a | ||
| Teaching | 6 | 11 (6,47%)a |
A first insight is that the most appropriate incentives for CI are those that promote the professional development of doctors such as professional career, opportunities for research and teaching. As evidence of the importance of setting an effective professional career scheme, doctors said that a new professional career scheme based on Professional Development and Further Education was needed. Other CI actions like providing more autonomy for managing their own work and recognition of the achievements of their work in terms of quality, merit or excellence based criteria, were also reported. Doctors wished for more autonomy to manage and organize their own work: Self-management.
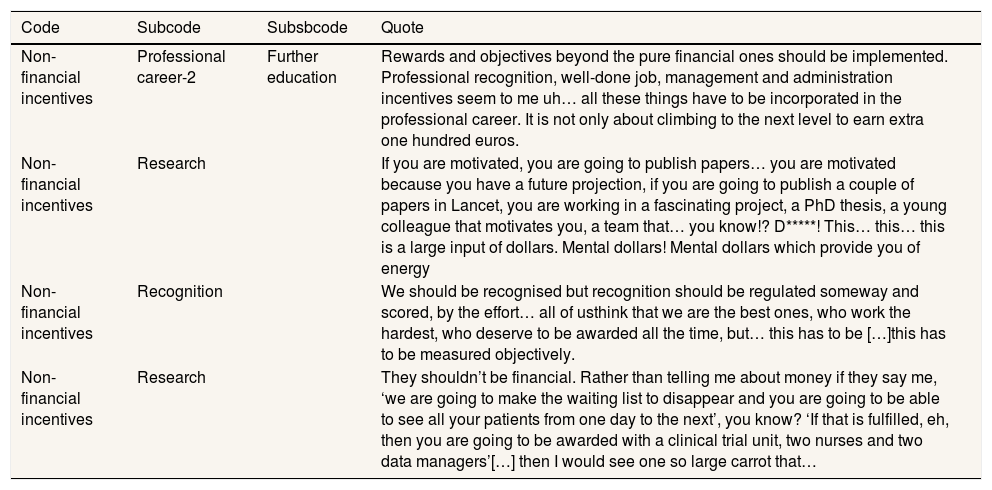
Table 6 shows quotes illustrating the request for a renewed professional career, more autonomy and other non-financial incentives.
Illustrative statements of crowding-in.
| Code | Subcode | Subsbcode | Quote |
|---|---|---|---|
| Non-financial incentives | Professional career-2 | Further education | Rewards and objectives beyond the pure financial ones should be implemented. Professional recognition, well-done job, management and administration incentives seem to me uh… all these things have to be incorporated in the professional career. It is not only about climbing to the next level to earn extra one hundred euros. |
| Non-financial incentives | Research | If you are motivated, you are going to publish papers… you are motivated because you have a future projection, if you are going to publish a couple of papers in Lancet, you are working in a fascinating project, a PhD thesis, a young colleague that motivates you, a team that… you know!? D*****! This… this… this is a large input of dollars. Mental dollars! Mental dollars which provide you of energy | |
| Non-financial incentives | Recognition | We should be recognised but recognition should be regulated someway and scored, by the effort… all of usthink that we are the best ones, who work the hardest, who deserve to be awarded all the time, but… this has to be […]this has to be measured objectively. | |
| Non-financial incentives | Research | They shouldn’t be financial. Rather than telling me about money if they say me, ‘we are going to make the waiting list to disappear and you are going to be able to see all your patients from one day to the next’, you know? ‘If that is fulfilled, eh, then you are going to be awarded with a clinical trial unit, two nurses and two data managers’[…] then I would see one so large carrot that… |
aEvery statement shown in the table comes from a different respondent and have been selected in order to serve as a guide of the codification process to the reader.
bOriginal respondents’ statements are in Spanish. Translations of those are displayed in the table. The reader can find the original statements in the electronic version of this paper.
Appendix provides a detailed description of codes.
In order to provide more consistency to the analysis performed in the CI section, we classify doctors’ statements into normative and positive. Then, for the CI statements we calculate the probability of being positive P(p), or being normative P(n), obtaining the following values: P(p) = 0.34 and P(n) = 0.66.
DiscussionTo the extent of our knowledge this paper is a pioneering study in the use of Qualitative Analysis methods in the research of incentives and doctors’ intrinsic motivation in health care in Spain. It reports on the empirical leg of a wider research on intrinsic motivation in health care organisations coming from BE and SDT.
Qualitative methods are the best approach to elicit the vision and opinions from workers related to attitudes towards work and incentives. However, they are subject to several sources of bias in the design of the study, the questions and the interviewers and interviewees. To overcome potential interviewers’ biases, interviews were performed by two researchers (MB and JC), one with a good deal of knowledge of the health care system and the other more expert in the use of qualitative methods. We realised that physicians are, in general, very science sensitive and familiar with the scientific method so the fact that they feel that they are participating in a research discipline incentivise them to be rigorous. This was confirmed in recordings, transcriptions and data afterwards.
Qualitative research performed in this work is subject to the traditional criticism attributed to this method: people do not know their own motives so that what they say about them should not be taken seriously.25 However, the point for any interview-based qualitative analysis is that, what agents involved in a particular phenomenon say about their own motives is a kind of evidence that is informative about the true nature of this phenomenon.
The sample may be constrained not only in quantitative terms (N=16) but also in qualitative terms —interviewees are mainly seniors and men. We do not believe that this is a strong limitation. Interviewees were key informants who know their organisations, their staff, and relationships with management and policy decision makers fairly well. They also provided some vision of motivational changes visible in new generations and about gender-based crowding-out/in incentives. But, even though a lot of interesting suggestions and statements along these lines were made, we cannot be sufficiently certain about them to draw conclusions and we propose further research along these lines.
All proposals for policy changes of this work are based on opinions and not on confirmed results in real behaviour. Therefore, all policy implications discussed must be taken just as a suggestion, even though it comes from key informants of the sector and highly recognized stakeholders.
Results support hypotheses 1 (intrinsic motivation) and 2 (crowding-out) and suggest the validity of hypothesis 3 (crowding-in). Results also support our previous theoretical findings which conclude that in the long run, investing in workers’ intrinsic motivation is more efficient than using monetary incentives.26
Our results are consistent with those obtained in the economic literature and psychology. Doctors’ reporting that they like and enjoy medical practice confirms that they are intrinsically motivated professionals, a result in line with the classical definition of IM.8 Moreover, financial incentives (FFS and PC-1) lead to a change in the perceived nature of the medical practice, which is in accordance to one of the well-established results from BE.3,4 Finally, control and the perceived lack of autonomy reported by doctors as a cause of CO is consistent with results from SDT.6–9
Normative statements occur twice as frequently as positive statements (P(p) = 0.34 and P(n) = 0.66). This result suggests that physicians currently perceive a need for change toward a more motivating incentive schemes, managerial policies and organizational issues. There is much more work to do in the field than what is currently done in the SNS-O. We do not present normative/positive analyses for CO because asking about what should be done to design CO incentives makes no sense.
Our results about doctors’ intrinsic motivation and possible crowding-out and crowding-in effects do not suggest that only intrinsic motivation matters. We tried to throw some light on how monetary payments and rewards should be combined with other non-financial incentives in order to incentivize doctors for performance, quality of service supply and career development, when the intrinsic motivation plays a role.
This work is a step forward in the optimal design of incentive schemes and policies which crowd in doctors’ intrinsic motivation. Some proposals for changes and incentives made by doctors emerge from the analysis. Health care policy should consider focusing on: 1) facilities to engage in scientific and research activities: clinical trials, technical assistance, conferences attendance and so on; 2) activities involving professional development: further education stays in centres or institutions of excellence, teaching and the like; 3) more autonomy to organize own work, to self-manage and to set and agree objectives jointly with colleagues and with the management; 4) recognition at the workplace: the need for a renewed professional career designed with clear criteria to reward professional excellence. Given our findings, we recommend the development of further studies in this context that might help to future design, implementation and evaluation of new and innovative systems of incentives in health care organisations. Incentives in health care in Spain are narrowly focused on financial rewards and this research should serve as a first step to cast doubt on whether that should be the only strategy.
Editor in chargeClara Bermúdez-Tamayo.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
FundingThis project received financial support from the Spanish Ministry of Science and Innovation for (Project ECO2009-12836).
As far as our knowledge reaches, this is a pioneering work using qualitative methods to study the design and performance of incentives in health organisations. It is also the first qualitative study of incentives in health using the behavioural economics approach.
What does this study add to the literature?This work confirms that physicians of Servicio Navarro de Salud-Osasunbidea are intrinsically motivated professionals, monetary incentives and control policies hurt physicians intrinsic motivation, and non-financial incentives, where they are well designed, have the potential to foster physicians’ intrinsic motivation.
M. Berdud and J.M. Cabasés designed the study. Both authors designed and performed the interviews. M. Berdud carried out the qualitative analysis and wrote the first draft of the manuscript. J. Nieto worked on the interpretation of results. All authors contributed to and have approved the final manuscript.
Conflicts of interestNone.
First, we would like to thank to the physicians that were interviewed for their time, kindness and patience to participate in the study. Thanks also to the Spanish Ministry of Science and Innovation for financial support of this project.














