



I want to draw attention to a central —and remediable— cause of social and material inequalities in health which, despite this status, is an «elephant in the room»: an issue that almost all are aware of but which is never addressed directly by those involved with health inequality and public policy. While it is commonplace to discuss the impact of gender inequality on women and girls1 and while it is also becoming commoner to discuss its impact on men and boys,2,3 something which is never discussed is its general impact on all public policy. However, there is a strong case to be made that one particular, patriarchal, form of masculinity is almost globally dominant, and that this dominance is reflected in unhealthy and antisocial patterns of socialisation which affect most if not all children and adults in Europe and in most societies worldwide. Furthermore, this socialisation has major and unacknowledged impacts on public policy-impacts which contribute importantly to much of the inequality and suffering experienced by humankind.
Concepts and definitionsFirst some concepts and definitions. Patriarchy is the systematic domination by men of women and of other men. Masculinities are the range of alternative ways (national, social, racial, sexual) in which male gender relations are expressed (for example, working class, Latin American and gay masculinities). Hegemonic masculinity is the form of masculinity which is culturally and politically dominant at a particular time and place. Health inequality refers to unfair or unjust differences in health determinants or outcomes within or between defined populations. Structural violence is suffering caused by public policies and institutions. Hegemony is a subtle and complex process whereby particular beliefs, values and ideologies are reinforced by those with political and cultural power such that they become perceived as both natural and inevitable, in the words of former UK prime minister Margaret Thatcher, speaking of market liberalism, «there is no alternative».
Hegemonic masculinity nowGiven what we know of the massive scale of global sociocultural variation it is extraordinary that, despite this diversity, a relatively specific form of gender relations has for many years remained globally dominant. I am referring to the variant of masculinity which is characterised by generally agreed «negative» attributes such as toughness, aggressiveness, excessive risk-taking, suppression of emotions; «positive» attributes such as strength, protectiveness, decisiveness, courage: and more contested attributes like individualism, competitiveness, rationality, and «practicality».
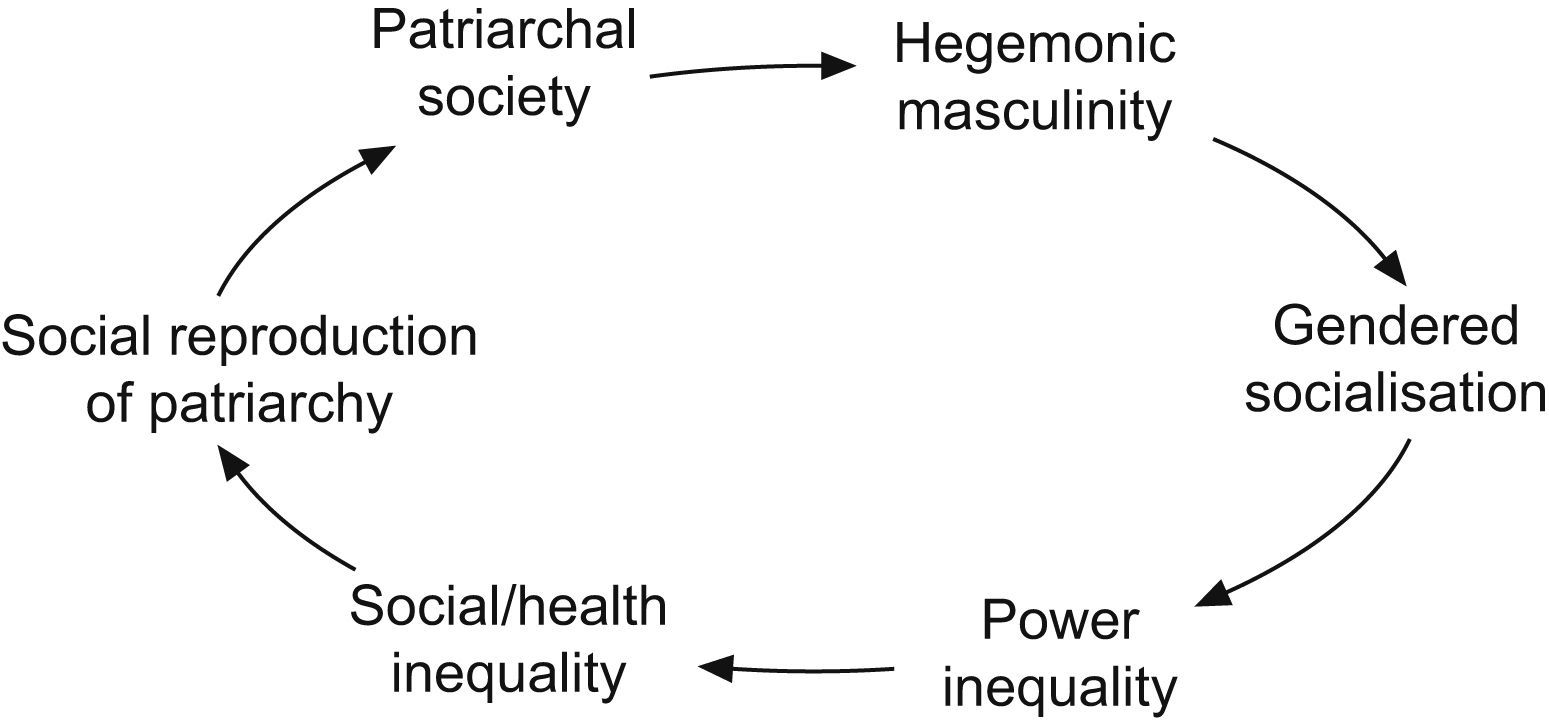
Perhaps the hegemonic dominance of this form of masculinity is not all that surprising if one considers its obvious overlaps with the equally dominant (neo)liberal economic relations of the free market. More worrying is the fact that worldwide acceptance of childhood socialisation into the above negative features of this hegemonic masculinity is what subsequently results in power inequalities between individuals, between social/racial/gender groups and between institutions —and in turn— in the individual and the structural violence through which power inequalities are expressed. Figure 1 is a highly simplified representation of how these social relations are produced and sustained. What I’m effectively saying is that patriarchal socialisation and hegemonic masculinity are unacknowledged, preventable causes of most health inequalities.
Structural violence
Structural violence is a concept originally used in peace studies.4 It differs from interpersonal violence in that it refers to oppression and suffering caused by structural relations, such as the civil, social and economic relations of public policy. Its abstract nature should in no way detract from its importantce. In my view structural violence is a key concept for public health: it provides a common conceptual framework for events as diverse as what Engels called the «social murder» of the poor which resulted from exploitative and oppressive 19th century living and working conditions, the widespread suffering caused by the aggressive economic and trade policies of the World Bank and the World Trade Organisation,5 the avoidable damage caused by unaffordable drugs or health care, and the terrible results of wars, genocide, racism, and poverty.
An interesting example of the worldwide relationship between hegemonic masculinity and structural violence is in a paper by Caprioli and Boyer from the international relations literature.6 They found that «States that are characterized by higher levels of gender equality (as shown by higher proportions of women in national parliaments) use lower levels of violence during international crises than those with lower levels of gender equality». Such findings have important implications for how we manage our societies, not least, for how we manage the health inequalities resulting from the many varieties of structural violence.
What is to be done?While it is tempting to view the globally endemic problems of patriarchy and hegemonic masculinity in a resigned and fatalistic way, it is also important to acknowledge that they are —at least in principle— preventable. The previous Swedish government's Education Ministry established a Delegation on Gender Equality in Preschool which looked at the ways in which, from the very beginning of education and socialisation, children in preschool education face systematically gendered policies and practices, and which made recommendations to change this situation (unfortunately the report is not available in English). This provides a small example of how such issues can legitimately begin to be addressed through public policy. Given the nature of the global institutions whose practices help to sustain patriarchy —such as many of the world's major religions— I would not pretend that the task will be an easy one. Nonetheless, there is much to be said for adopting a public health perspective on these issues. If we can generate evidence and debate around the notion that patriarchy is a «preventable disease»,7 this is a valid and a potentially useful way forward. Another helpful approach would be to build public pressure for a global commission on masculinities.
The fact that virtually no one is currently acknowledging, let alone addressing this issue makes it no less important as a key global cause of mortality, morbidity and inequality. Discussion and action are long overdue.











