




To determine the impact that intersectoral policies and social participation, implemented worldwide, have had on the modification of the social determinants for health and on the reduction of social health inequities.
MethodA scoping review of the literature published in the period 2005-2015 was performed. The literature search was conducted on PubMed and Scielo databases. Two researchers reviewed each document. Data were analysed according to the intersectoral action and social participation variables and according to the theoretical frameworks of the Social Determinants Model of the Commission on Social Determinants of Health (CSDH) and the theoretical constructs of Social Capital (SC) and Life Course (LC).
ResultsOut of 45 documents likely to be selected for final review, all of them based on title and abstract, 20 documents were eventually picked out and analysed; most them (n = 8) were conducted in all Latin America and Latin America's countries. Twelve documents reported intersectoral action associated with social participation in partnership with different institutions. Regarding theoretical frameworks, most of studies (n = 8) used CSDH and SC. In relation to health outcomes, the studies showed mainly: increased access to health and education, follow-up of pregnant women, increasing in prenatal examinations, reduction in malnutrition/child mortality, reduction in extreme poverty/hunger; reduction in epidemics/tuberculosis, control of alcohol/drug consumption, promotion of health/mental as well as basic sanitation improvements.
ConclusionsIntersectoral and social participation experiences studied yielded positive outcomes regarding health status and quality of life in the communities in which such experiences were implemented.
Determinar el impacto que las políticas intersectoriales y la participación social, implementadas en todo el mundo, han tenido tanto en la modificación de los determinantes sociales de la salud como en la reducción de las desigualdades sociales en salud.
MétodoSe realizó una revisión exploratoria (periodo 2005-2015). La búsqueda bibliográfica se hizo en las bases de datos PubMed y Scielo. Cada artículo fue revisado por dos investigadores. Los datos fueron analizados según las variables de acción intersectorial y participación social, y de acuerdo con los marcos teóricos: modelo de determinantes sociales de la Comisión de Determinantes Sociales de la Salud (CDSS) y constructos teóricos de capital social (CS) y curso de la vida.
ResultadosDe los 45 documentos seleccionables para la revisión final, basándose en el título y el resumen, 20 fueron seleccionados y analizados; la mayoría (n = 8) realizados en América Latina. Doce artículos informaban sobre acciones intersectoriales en asociación con participación social en colaboración con diferentes instituciones. En cuanto a los marcos teóricos, la mayoría (n = 8) utilizaron CDSS y CS. En relación con los resultados de salud, los estudios mostraron principalmente: mayor acceso a la salud y educación, seguimiento de embarazadas, aumento en exámenes prenatales, reducción de la desnutrición/mortalidad infantil, reducción de la pobreza extrema/hambre, reducción de las epidemias/tuberculosis, control del consumo de alcohol/drogas, promoción de la salud/salud mental, y mejoras en el saneamiento básico.
ConclusionesLas experiencias intersectoriales y de participación social estudiadas arrojan resultados positivos en el estado de salud y calidad de vida de las comunidades en que fueron implementadas.
Around 10 years after the creation of the WHO Commission on Social Determinants of Health (CSDH-WHO), and after some progress in studies on reducing health inequities, particularly in Europe, high indices of vulnerability and social inequity continue in certain social groups. This situation produces differentiated access to material and symbolic resources that impact the health of people and populations.1
In Latin American and other poor countries, there are peripheral urban territories marked by poverty, low education levels, unemployment or informal income generation, violence, insertion, high rates of abuse of alcohol and other drugs, disruption of social networks of support, and geographical and political exclusion. Africa has even the highest morbidity burden compared to other regions, and it also has the lowest per capita expenditure on health.1 Studies show how the poverty present in many people affects all life and health from birth and throughout the life course reducing life expectancy and increasing the chances of premature death in the most inequitable countries. Focusing on poverty is essential to Global Commission on the Social Determinants of Health.2–5Exclusion from or difficult access to income, work, education, housing, transportation and mobility, culture, leisure, a sustainable environment and social support networks cause of health inequities in poor countries. There are groups of people that suffer health problems and deaths, which are unfair and avoidable. 6,7
Studies have emphasised the strong recommendation of the CSDH-WHO in the construction of intersectoral policies to address health inequities. Intersectoral Action for Health is an important component of the Global Strategy for Health for All by the Year 2000 and a component of the 2006 “Health in All Policies” (HiAP). A HiAP approach promotes “effective and systematic action for the improvement of population health, using genuinely all available measures in all policy fields”.8 Intersectoral actions should occur at superstructural levels and be based on agreements between areas of government, i.e. all other sectors (economic, labour and employment, education, transportation, housing, environment, etc.) should elect health promotion as a priority, through global action aimed at reducing social inequities.9–13
Strategies focused in intersectoral policies are indisputable from the viewpoint of its urgency and necessity, but it is insufficient when considering the growth of social problems in urban territories in medium and large cities worldwide, especially cities in poor or developing countries.14 Therefore, in addition to these strategies from the central government of a country, it is necessary to include civil society in order to execute actions to reduce social inequities that affect the levels of health of the population, especially in the poorest territories.15
Thus, a scoping review was conducted with the general objective of determining the impact that intersectoral policies and social participation, implemented worldwide, have had on the modification of the social determinants of health and on the reduction of social inequities in health.
It is worth noting that there are studies referring to HiAP, including evaluation studies of the policies implemented in several countries, mainly in Europe1,6,14. However, few studies have shown intersectoral policies and community participation. So, this review could inform future intersectoral policies including successful experiences with the participation of civil society.
MethodA scoping review is a review method characterised by researching the existing, relevant literature, which seeks to map and summarise a series of tests to convey the range and depth of a field supported in evidence-based practice. The scoping review method has six stages: 1) identifying the research question; 2) identifying relevant studies; 3) study selection; 4) charting the data; 5) collating, summarising and reporting the results; and 6) consultation with interested individuals to inform or validate study results (optional).16
The current review was carried out from October to December 2015 and in the following stages:
- 1.
Identifying the research question. The research question was identified as: “What policies or actions or strategies or programs, that include intersectoral actions and social participation focussing on the social determinants of health and reduction of social health inequities (SHI), which have been implemented worldwide, have shown modifications of these determinants and/or reduction of these inequities?”. In this work, intersectorality is understood as a policy and as a technical and administrative process that involves negotiation and the distribution of power, resources and capacities (technical and institutional) between different sectors. Intersectoral action is understood as not only the political intent of the government, but also managerial capacity, together with new institutional arrangements between different sectors of the administration to achieve results. Social participation is understood as organisational arrangements and practices that involve groups and organisations of civil society, particularly those that work with resource allocation for health needs.17
- 2.
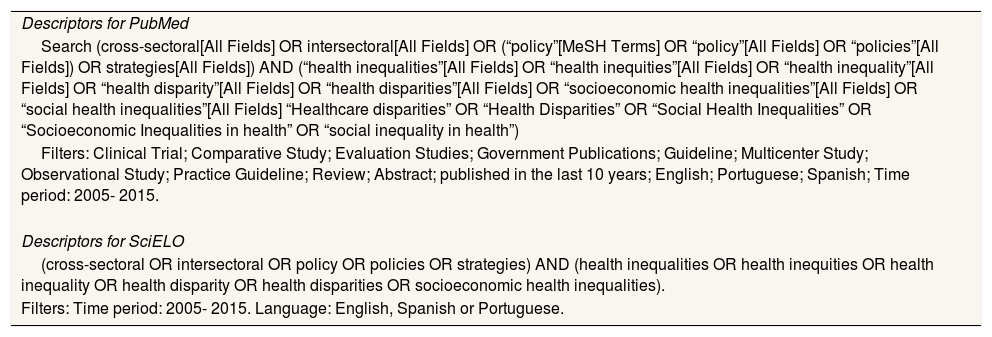
Identifying relevant studies. Databases were searched by pairs on PubMed and SciELO. The selection of these databases was due to the criterion of the search range, which allowed access to worldwide studies (PubMed) and Latin America (SciELO), thus recognising the importance of programmes and initiatives in Latin America on the SDH, through intersectoral strategies. The search period was from 2005 to 2015. This criterion was determined in line with the creation date of the CSDH-WHO in March 2005; this fact has been considered relevant for the development, by the countries, of policies and actions oriented to the modification of the social determinants of health as well as to the reduction of SHI. The search strategies applied to the databases are presented in Table 1.
Table 1.Database search strategy.
Descriptors for PubMed Search (cross-sectoral[All Fields] OR intersectoral[All Fields] OR (“policy”[MeSH Terms] OR “policy”[All Fields] OR “policies”[All Fields]) OR strategies[All Fields]) AND (“health inequalities”[All Fields] OR “health inequities”[All Fields] OR “health inequality”[All Fields] OR “health disparity”[All Fields] OR “health disparities”[All Fields] OR “socioeconomic health inequalities”[All Fields] OR “social health inequalities”[All Fields] “Healthcare disparities” OR “Health Disparities” OR “Social Health Inequalities” OR “Socioeconomic Inequalities in health” OR “social inequality in health”) Filters: Clinical Trial; Comparative Study; Evaluation Studies; Government Publications; Guideline; Multicenter Study; Observational Study; Practice Guideline; Review; Abstract; published in the last 10 years; English; Portuguese; Spanish; Time period: 2005- 2015. Descriptors for SciELO (cross-sectoral OR intersectoral OR policy OR policies OR strategies) AND (health inequalities OR health inequities OR health inequality OR health disparity OR health disparities OR socioeconomic health inequalities). Filters: Time period: 2005- 2015. Language: English, Spanish or Portuguese. - 3.
Study selection. The studies were selected according to an analysis of the title, followed by an analysis of the abstract and, finally, a thorough analysis of the content, conducted in two stages a full reading of documents by each reviewer on independent way and then by pair. Documents focused on the research question (intersectoral actions and social participation focussing on the social determinants of health and reduction of social health inequities) were included. Documents that did not show results in the modification of SDH and/or in the reduction of SHI were excluded.
- 4.
Charting the data. The documents selected were analysed as proposed by Andrade et al.17 for intersectoral action, as defined in Stage 1. In accordance with this conceptual framework, the following variables were defined:
- •
Intersectoral action (IA):
IA-A: Creation of ministries focused on specific problems; e.g. social development, urban development, gender equality, poverty reduction, among others. As well as intersectoral policy created by Decree of the federal government.
IA-B: Central government initiatives to address social emergencies, such as drug use, violence, etc., which combine the participation of local authorities and civil society organisations, associations and groups, as well as mobilisation and decision-making, providing more flexibility for governance.
- •
Social Participation (SP):
SP-A: social participation that integrates with the system of governance,
SP-B: ombudsmen and public defenders,
SP-C: corporate councils,
SP-D: associations of users of services in dialogue with governments.
- •
- 5.
Collating, summarising and reporting the results. This work used the SDH model of the CSDH-WHO1,10,11,18–20 as a conceptual and theoretical framework, as well as the theoretical constructs of social capital (SC)21,22 and the life course (LC).23,24
The SDH model is defined in two spheres: structural and intermediate determinants. Structural determinants are those linked to social stratification and include socioeconomic and political contexts and distribution of power and resources, as well as labour market, gender, ethnicity, social class and education level. Intermediate determinants include: a) material circumstances, such as housing, income level, working conditions or neighborhood; b) psychosocial circumstances, such as lack of social support, stressful situations (negative life events), poor control, etc.; c) behavioral and biological factors, such as life-threatening lifestyles; and d) the health system.1,10,11,18–20Social capital is a theoretical construct developed by Macinko and Starfield21, and Kawaschi et al.22, who took the concept social capital from contributions by thinkers like Robert Putnam, James Coleman and Pierre Bourdieu, and applied in the field of health and more specifically in the field of studies on social determinants of health. The social capital is defined as a specific form of social organisation in which a strong network of interpersonal relationships is based on reciprocity and social cooperation. This organisation produces a personal and collective development capital that determines development in all sectors: economic, cultural, political, social and health.21,22
The theoretical construct of life course understands that the socioeconomic inequities present in certain regions have a lifelong effect on people born and raised in these regions. Thus, life course epidemiology is defined as the study of long-term effects on health or disease risk of physical or social exposures during gestation, childhood, adolescence, young adulthood and later adult life.23,24
The documents were then compared according to the variables and theoretical frameworks and the results achieved in practice concerning the SDH and the reduction in health inequities in their regions. Likewise, we sought to analyse the implications of these studies for current research and our results.
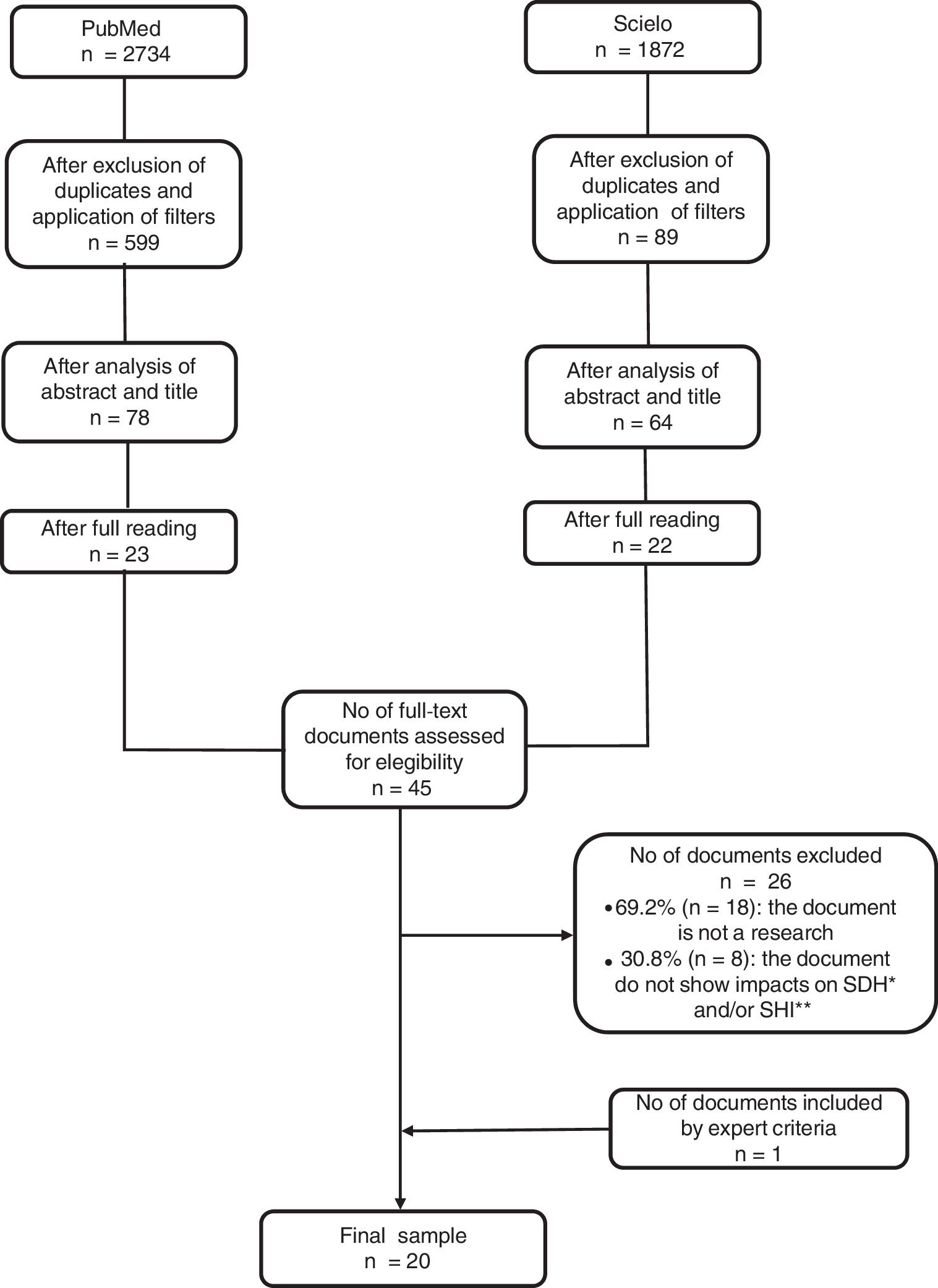
ResultsThe process described collected 2734 documents from the PubMed database and after excluding duplicates and applying filters referring to the design of the studies to be reviewed, 599 documents remained. Further selection based on titles and abstracts reduced this to 78 documents. After full reading, remained 23 documents to be reviewed. Regarding the SciELO database, 1872 documents were initially collected. After applying filters, excluding duplicates and analysing the titles, 89 documents remained. After reading the abstracts, 64 documents were selected, of which 22 were selected for review following in-depth reading. Therefore, 45 documents with the potential for final selection for review were selected. After re-reading and preliminary analysis of the results in pairs and independently, 26 documents were excluded for not being a research (n = 18, 69.2%), and not showing impacts on SDH and/or SHI (n = 8, 30.8%.) Thus, 19 documents were selected. However, one document was included by expert criteria, constituting the final sample of 20 (Fig. 1).

Concerning the year of publication, five studies were from 2015, four from 2014, two from 2013, two from 2012, two from 2011, one from 2010, two from 2009, one from 2008 and one from 2006. According to geographical distribution, two were in Europe context, two in Latin America context, one in Africa, one in Americas and three in Australia. Other were developed in specific countries: three of the studies were developed in Brazil, one in Cuba, one in Mexico, two in Canada, three in the United States and one in Venezuela. The range of studies involved regions or continents, such as Americas, Latin America, Europe and Australia as well as cities of a certain region or country, or the national contexts of certain countries. Other contexts included territorial communities (neighbourhoods and/or regions) or group communities (ethnic, gender) in a given state or city of a given country. Concerning the study design, there were six case studies, three review studies/documental analysis, six qualitative research studies (three ethnographic studies, two participatory action research studies and one qualitative evaluation study), three evaluation studies, one longitudinal ecological study and one randomised controlled trial (Table 2).
Scope, objective, design, intersectoral action and social participation, and outcomes from selected documents.
| Authors | Scope and objective | Study design | Intersectoral action and social participation according variablesa and theoretical frameworkb | Outcomes (modifications of social determinants and reduction of social health inequities) |
|---|---|---|---|---|
| Andrade et al.17 | Latin America: Brazil, Chile, Colombia, Cuba Objective: Analyze intersectoral public policies developed by the governments of the countries, as well as communities and civil society involved in the implementation of policies. | Case Study (four case studies) | Bolsa Família (Brazil): Variables: IA (B) Theoretical framework: CSDH (A) | Increased access to health and education services; Increase prenatal consultations from 49% to 61%; Increase immunization and reduction of child malnutrition; Decrease of infant mortality below 5 years; income increase for families living in extreme poverty and extension of the social and financial protection network |
| Chile Crece Contigo (Chile): Variables: IA (B) Theoretical framework: CSDH (A)+ LC | Positive effects on reducing child poverty and increasing access to educational and health opportunities. | |||
| De Cero a Siempre (Colombia): Variables: IA (B) + SP (A, C) Theoretical framework: CSDH (A) + LC | Child nutritional status and income generation for women have improved; Increase coverage of population aged up to and including 5 years, about 4 million children; Increasing the guarantee of rights to the integral attention of 2 - 9 million vulnerable children in the poorest populations; Improved nutritional status of children and women's employment. | |||
| Erradicación de Aedes aegypti (Cuba): Variables: IA (B) + SP (A, C) Theoretical framework: CSDH (B) | Reduction of dengue infections and improvement of environmental management for vector control. | |||
| Diba and D’Oliveira36 | Brazil Objective: To analyze the relationship of an experience in Theater and Community together with health teams dedicated to the promotion of health for young people in social vulnerability. | Ethnographic study | Project of theater for young people in social vulnerability from a Civil Society Organization of Public Interest that integrates the Art, Culture and Citizenship Program – Cultura Viva, of the Ministry of Culture of Brazil, implemented in 2004. Research shows that the culture sector strategy has impacts on health promotion for young people in the theater group Variable- SP (D) Theoretical framework - SC | According to the research referentials the results are in two axes: 1- True Friends Increase of social capital and strengthening of social support networks; Control of problematic use of alcohol and other drugs. 2- Dialog: Spatial listening to daily suffering and social support; Access to information and social protagonism and awareness of rights and duties; Social participation and community empowerment; Promotion of health. |
| Baum et al.25 | Australia To examine to what Adelaide Thinkers in Residence (ATiR) scheme contribute to the change in norms whereby promoting well-being and achieve the strategy “Health in All Policies” in Australia. | Mix method case study | The ATiR scheme was the initiative of Australian government between 2003-2013 addressed to developing new ideas and approaches to social problem solving in different social areas. The scheme involves different partners from government, non-government organizations, business, industry and community organizations. Variables: IA (A, B) and SP (A, B, C, D) Theoretical framework: CSDH (A, B), SC | ATiR program on HiAP promoted a series of innovations relevant to health, increasing prevention and promotions actions in health: focused on strategies for rehabilitating/reintegrating prisoners to reduce repeat offending and improve community safe; increased quality of life through design and city planning; increased system to assist homeless people; strategies for “age friendly” society where old people are safe, healthy and heave access to services; development health equity and integrate health concerns into the policy development process. |
| Eugenio et al.37 | Mexico Objective: To present the process and results of the three-year educational work with the community of El Molino, Jocotepec, Jalisco, Mexico in the reduction of health inequalities through intersectoral project with education | Participatory action research | Popular Education Process with the following steps: 1. knowledge of the community, 2. conformation of primary group, 3. social mobilization with integration of work commissions, 4. process growth with different modalities of participation. Variables: SP (A, B, D) Theoretical frameworks: CSDH (A, B) and SC | Acquisition of health information for healthy lifestyles; Creation of 5 community networks; Repair in 20% in the drainage system; Improvements in basic sanitation and housing conditions; Get access to schools; Admission of young people in higher education; Reforestation and creation of ecological park; Training of women's groups to reassess their social role and income-generating activities; Decrease in depression rates among women and decrease in gender violence; Significant decrease in rates of Hepatitis A, Conjunctivitis and dengue. |
| Farrington et al.26 | Europe - European City Network Objective: to analyze four behavioral risk factors (tobacco use, alcohol abuse, unhealthy diet and physical inactivity) by non-communicable diseases (NCDs) | Evaluation study | WHO Healthy Cities Network during its fifth phase (‘Phase V’: 2009-13) in modifying four lifestyles behavioral risk factors for NCDs, and specifically to confirm if evidence-based interventions were being implemented, and to assess the potential added value of Healthy Cities in prevention of NCDs Variables: IA (A, B) and SP (A, B, D) Theoretical frameworks: CSDH (A, B) and SC | Cities, where there were actions with community engagement, got results more successful and there were multiples examples of how attention had been paid to the social determinants of heath. Evidence showed that cities continue to be significant innovative forces within their countries; the mutual dependency of the national and local levels was highlighted. Interventions to promote physical activity have shifted focus from projects to be more integrated with other policy areas and based on intersectoral collaboration |
| Alia et al.38 | United States of America Objective: Describe the experience The Right Choice, Fresh Start (RCFS) Farmers ‘Market and analyze social networks in a context of a farmers’ market for healthy food sales within rural communities of Afro-descendent Americans in social vulnerability Of South Carolina – USA. The strategy involved local actors such as: farmers and consumers, researchers and students from the University of South Carolina, and health agencies | Ethnographic study | The Right Choice, Fresh Start (RCFS) Farmers’ Market – The RCFS market is a multi-vendor, produce-only Variables: SP (B, C, D) Theoretical framework: SC and CSDH (A, B) | Activating interest and social participation through the social capital increase; Economic and Financial Exchange had the potential to benefit customers by decreasing financial barriers to purchasing healthy foods; Educational exchanges could have educational benefits for children and adults - encouragement of healthier food styles; Resource sharing like goods, information, or services |
| Anaf et al.27 | Australia To examine intersectoral action for heath (IAH) in primary health care (PHC) in six cities of Australia | Case study | Good practice from participating sites (partners and service users) concerning collaborations with sectors other than health that addressed one or more social determinants Variables: IA (A, B) e SP (A, C, D) Theoretical framework: CSDH (A, B) SC and LC | Backgrounds and skills of collaborators enable to carry out IAH in PHC. Positive outcomes: Achieving a floor price on alcohol, Increased community engagement, Linking vulnerable people back into the community through a community based choir, less demand for medical attention, etc. Time and financial constraints are the main limitations to perform IAH |
| Nascimento et al.41 | Brazil Objective: To analyze how 105 Brazilian municipalities that adhered to the WHO Agenda 21 obtained impacts on living conditions and health | Longitudinal ecological study | Actions framed Agenda 21 and ‘Healthy Cities’ and aimed at social determinants of health and, among these, actions developed through intersectorality and others focused on the health sector Variables: IA (A, B) Theoretical framework: CSDH (A, B) and LC | Impacts of the agendas were detected for reduction of hunger and increase of universal access to education: ‘percentage of children under one year with protein/caloric undernourishment’ (interaction effect: p = 0.02) and ‘Age-grade distortion in the 8th grade of fundamental education’ (interaction effect: p <0.001); The coefficient of Tuberculosis prevalence, diminished from 32 to 0.6%; The percentage of the population served with piped water increased; The percentage of lady town councilors presented a significant increase; The proportional mortality of children under the age of one diminished |
| Pons-Vigués et al.39 | Europe - European cities Objective: to seek and analyze studies that focus on policies aimed at reducing health inequities. | Scoping review | Studies that have reported policies aimed at reducing health inequalities developed in communities, based on local governance of cities in Europe Variables: SP (A, B) Theoretical framework: CSDH (A, B) | Increase actions to promote health and oral health; Enhanced physical activities; decrease of cardiovascular risk factors; Improvements in economic access; renovation of physical areas in neighborhoods; Increase the number of day care centers providing care to high-quality children; Increasing access to healthy food; Prevention of HIV transmission between baby and baby; Countries that presented intersectoral actions showed success in policies to reduce health inequalities |
| García-Ramírez and Vélez-Álvarez28 | Latina America OPAS Objective: to identify government documents and studies and from 22 Latin American countries dealing with public policies on the Social Determinants of Health and emphasize the context of eight countries (Argentina, Brazil, Bolivia, Chile, Colombia, Costa Rica, Mexico and Venezuela) | Review study of literature and documentary | Programs addressed to the social determinants of health developed from governmental determinations of the corresponding countries, involving interministerial actions and community action: Community Doctors Program and Healthy Communities and Municipalities Program, Indigenous Safeguard Program, zero Malnutrition, Family Health Strategy, Together Network, Psychosocial Care Program, Barrio Adentro Mission, Milagro Mission and Robinson Mission Variables: IA (A, B) and SP (A, C, D) Theoretical framework: CSDH (A, B) and SC, LC | Strong social participation and empowerment of indigenous communities; Increase in health coverage and social inclusion; Increased access to health; Decrease of child malnutrition rates; Increase of social protection.; Increased access to services, barriers to gender, ethnicity; Improved socioeconomic conditions; Reduction of extreme poverty; Increased access to education and health |
| Prasad et al.29 | Americas: Guarulhos (Brazil), Toronto (Canada), Bogotá and Medellin (Colombia) Objective: to determinate utility of Urban Health Equity Assessment and Response Tool (Urban Heart) in supporting government efforts to improve health equity using the social determinants of health (SDH) approach | Evaluation study | Urban Health Equity Assessment and Response Tool (Urban HEART) guides users through a process of identifying health inequities and critical social determinants of health, to develop a plan of action to tackle those inequities Variable: IA (A, B), SP (A, C, D) Theoretical framework: CSDH (A, B) | In three cities, local governments spearheaded the process, while in Toronto, academia initiated and led the process. All cities used Urban HEART as a platform to engage multiple stakeholders. While Bogotá and Medellín prioritized among existing interventions, Guarulhos adopted new interventions focused on deprived districts. Actions were taken on intermediate determinants, e.g., health systems access, and structural SDH, e.g., unemployment and human rights |
| Clavier et al.30 | Canada – Quebec Objective: to evaluate the local implementation of a intersectoral procedural public health addressed to create healthy environments for vulnerable families in Quebec, Canada | Qualitative multiple case study | SIPPE-HE (Integrated Perinatal and Early Childhood Services for Families Living in Vulnerable Situations- Health Environment) program provides communities organizations to act on the social determinants of health of vulnerable families through intersectoral health actions, involving government, primary health care services, social services and community Variables: IA (A, B), SP (A, C, D) Theoretical framework: CSDH (A, B) and SC, LC | A few initiatives reached beyond the health and social services sector (8.9%). Membership and mandates of the local groups responsible for program implementation also showed little intersectorality The majority of all projects (74.5%) were focused on increasing access to local services for young parents and their families, services during pregnancy and after the birth, stimulation of child development, creation of social networks for families to connect them with community resources in their neighborhood, and projects to increase food security |
| Lawless et al.43 | South Australia Objetive: to evaluate the impacts associated with programs: Water Sustainability HLA (Health Lens Analysis), Regional Migrant Settlement HLA and Digital Technology HLA | Qualitative evaluation study | Water Sustainability HLA was focused on the potential health impacts associated with increasing use of alternative water sources Regional Migrant Settlement HLA examined the interplay among the social, economic and health factors affecting migrant settlement Digital Technology HLA aimed to support increased use of digital technology by low socio-economic status groups in ways that promote positive health outcomes. Variables: IA (B) Theoretical framework: CSDH (A) | Increased understanding by policy-makers of the impact of their work on population health and health equity. Positive changes in policy direction because of a HLA, promoting and incorporating policy-relevant research. Greater understanding and stronger partnerships between health and other sectors. A favorable disposition toward employing HLA in future work |
| Baril et al.31 | Boston, USA Objective: To describe Boston Public Health Commission's health equity framework addressed to eliminate of racial and ethnic health inequities and the social determinants of health | Evaluation study | Intersectoral actions among Boston Public Health Commission, The New England partnership for health and community developed a theoretical framework for practices addressed to SDH Variables: IA (A, B), SP (A, B, C, D) Theoretical framework: CSDH (A, B) and SC | It was developed a health equity agenda for confronting racism, promoting actions that improved social capital, education, transportation, employment, food access, housing, environmental exposure, access to health services, socioeconomic status and public safety |
| Mendel et al.40 | United States of America Objective: to evaluates one of a number of community engagement strategies employed in the Community Partners in Care (CPIC) and describe the unique goals and features of a community engagement kickoff conference as used in CPIC. Los Angeles – United States of America | Randomized controlled trial (RCT) | Describe and assess the effectiveness of a kickoff community engagement conference used during the initial stage of the Community Partners in Care (CPIC) trial as a large-group, event based intervention for activating individuals and agencies in a communitywide effort to improve access and quality for depression care Variables: SP (C, D) Theoretical framework: SC | Stimulating a dialog sense of collective efficacy, and opportunities for learning and networking to address depression and depression care in the community; Activating interest and participation for implementing evidence-based quality improvement programs for depression across diverse community agencies; Introducing evidence-based toolkits and collaborative care models to potential participants in both intervention conditions and other community members |
| Muñoz42 | Venezuela Objective: To identify actions off health system, as well as own health system actions, directed at reduction of social determinants of health in Venezuela | Documental analysis | The following actions were analyzed: 1) Intersectoral actions focused on the structural SDH (Misiones Educativas, Misión Madres del Barrio, Misión Habitar, etc.) 2) Intersectoral actions focused on the Intermediates SDH (Misión Ciencia, Misión Árbol, Misión Alimentación, etc.) 3) Health System actions to reverse the effects of intermediates SDH (Misión Barrio Adentro, Misión Sonrisa, etc,) Variables: IA (A, B) SP (A, D) Theoretical framework: CSDH (A, B) | The results were: Some social and health improvements are observed but the challenges are immense. Identifying areas that need to be better focused (traffic accidents, violence, environment, workers’ health). Bureaucracy and corruption are obstacles to the success of intersectoral actions |
| Díaz et al.32 | Cuba Objective: To present the intersectoral strategy to control of dengue transmission, production of equity and healthy ecosystems in Cotorro – Cuba, between 2003 and 2006 | Participatory action research | A management group was formed, composed of representatives of the community, sectors and decision makers. The members were trained in the theory and method of participatory action research and ecology approach, and five workshops were held to coordinate the proposed actions. Variables: IA (B) and SP (A, C, D) Theoretical frameworks: CSDH (B) and SC | Control of vector proliferation and dengue transmission; Control of environmental risks for the proliferation of vectors; Reduction of 85% of outbreaks in houses to 29%; Reduction of 16% from unhealthy yards to 1%; Reduction of the tanks that served as reservoir for the mosquito from 68% to 8%; {Ut1}-In relation to the proliferation of A. aegypti neighborhood community groups found 188 outbreaks in outlying areas and 478 indoors. There were 452 foci resolution (68%) |
| Lal and Mercier33 | Canada – Vancouver Objective: To examine a partnership formed among public health sector and local community to create a social enterprise for persons with mental illness | Case study | Stakeholders representing organizations from several sectors of the community partnered to develop work opportunities for a population that is disadvantaged and persons with mental illness. Variables: IA (B), SP (A, C, D) Theoretical framework: CSDH (A, B), SC | Inclusion in the labor market and employment (horticulture activities) of persons at social disadvantage and persons with mental disorders (30% of these jobs would be reserved for this population); stimulation of healthy lifestyle; social integration in the community. But authors report strong challenges too represented role ambiguities into the team and differences in objectives and priorities; Stigma does local media go against the project |
| Manandhar et al.34 | Africa – Zambia Objective: To evaluate actions for maternal survival in Zambia - Africa | Qualitative research (participatory ethnographic evaluation) | “Intersectoral Interest Group Meetings” and “Dissemination and Discussion Events” with participation of Government departments, civil society, the indigenous health system, academia, technical provider associations, and media, advocacy and human rights organizations Variable: IA (B), SP (A, B, C, D) Theoretical framework: CSDH (A, B), SC | Government staff at central level faced with disease-focused interventions rather than underlying contextual social determinants of health. A weak culture of health sector intersectoral engagement with civil society and other sectors contributed to less successful actions. Final dissemination and discussion events incorporated material to stimulate wider discussion and make recommendations to promote intersectoral exchanges in researches and actions to improve Zambia's Health System. The intersectoral process provided the Zambia's health professionals with new insights into the socio-cultural and gender contexts to improve the health contexts and provide information about lived reality for women and girls in the area |
| Wimmer and Figueiredo35 | Brazil Objective: To analyze two intersectoral action in the Family Health Program context in Rio de Janeiro (Brazil) | Case study | Two intersectoral action in the Family Health Program context in Rio de Janeiro (Brazil): Maré favela complex and Curicica community. Intersectoral action among Family Health Program, Social Work sector and local non-governmental organizations Variable: IA (B), SP (A, B, C, D) Theoretical framework: CSDH (A, B), SC | Improvements in the coexistence of the family nucleus. Community integration. Creation of local activities focused on education and culture. Creation of leisure spaces. Organization of the community to fight for the rights and solubility of local problems through effective governmental actions |
LC: life course; SC: social capital.
Variables:
IA, Intersectoral Action:
-Creation of ministries focused on specific problems, e.g., Social Development, Urban Development, Gender Equality, Poverty Reduction, among others, and intersectoral policy created by decree of the federal government.
-Central government initiatives to address social emergencies such as, violence, etc., which combine the participation of local authorities and civil society organizations, associations and groups to decision-making.
SP, Social Participation:
A.→Social participation that integrates the governance system.
B.→Ombudsmen and Public Defenders.
C.→Corporate councils.
D.→Associations of users of health services in regular dialogues with governments.
Theoretical frameworks:
CSDH, Commission on Social Determinants of Health Model:
A.→Structural determinants: socioeconomic and political contexts and distribution of power and resources, labour market, gender, ethnicity, social class and education level.
B.→Intermediate determinants: housing, income level, working conditions or neighborhood; lack of social support, stressful situations, poor control, etc.; life-threatening lifestyles; health system.
According to analysis of intersectoral action and social participation, the studies indicated the creation of ministries and mergers between health departments and other sectors of public administration, including social assistance, education, environment, with a view to reducing health inequities and intersectoral policy created by decree of the federal government (IA category A). Government programmes focused on emergency issues like hunger, epidemics, infant mortality and malnutrition, and diseases (IA category B) were also identified. The analysis also indicated that intersectoral actions were conducted in combination with strong community participation (SP categories A, B, C and D).
According to the variables, 12 documents reported intersectoral action associated with social participation SP, in any of their categories.17,25–35Four documents reported local community-based social participation actions in partnership with different institutions.35–38 Three documents referred exclusively to intersectoral action conducted only by central government policies, without community participation39,42,43 (Table 2).
Regarding their theoretical frameworks, eight documents reported on intersectoral actions and social participation pertaining to CSDH and SC.25,26,30–35 Three documents showed the actions taken were included in all three (CSDH, SC, LC).17,27,28 Two documents showed actions inserted within SC.36,40 One included the CSDH and LC.41 And five only included references to the CSDH29,38,39,42,43 (Table 2).
In relation to the reduction in SHI, studies showed numerous improvements, including: increased access to health and education; follow-up of pregnant women and increase in prenatal examinations; reduction in malnutrition and child mortality; reduction in extreme poverty and hunger; a reduction in epidemics;17,28,30,32,35–38,41 reduction in infectious diseases, such as tuberculosis;39,41 control of problematic use of alcohol and other drugs;36,37 promotion of health and mental health and improvements in health care and mental health;36,37,40,43 environmental improvements and basic sanitation in vulnerable regions;37 creation of healthy habits among populations and social groups;38 increasing in social capital; increasing in social protection and access to healthcare for vulnerable population, reduction of violence and creation of safer areas.25,27,28,32,37,41
Other works revealed: increasing in health promotion actions and physical activities;24 decreasing in cardiovascular risk factors; renovation of physical areas in neighbourhoods to facilitate access to services; increasing in the number of day care centres providing high-quality care to children; increasing in access to healthy food; prevention of HIV transmission between mother and child and reducing noncommunicable diseases; installation of central heating systems to increase health status and quality of life in vulnerable neighbourhoods.28,30,31,35,37,39,41
Other authors showed up socioeconomic improvements, increasing in access to education and other social services, accessing to healthy food, decreasing in barriers to gender, reduction of extreme poverty and employment generation.28,33,34,37,41,43
Finally, other studies tackled SDH such as creation of agendas for confronting racism, promoting actions that improved social capital, education, transportation, employment, food access, housing, environmental exposure and access to healthcare services.30,42,43
DiscussionReflecting on our research question, the results of the review showed that the intersectoral and social participation experiences studied yielded positive outcomes regarding health status and quality of life in the communities, countries or regions in which such experiences were implemented.
According to the variables of this research, there is a prevalence of studies on intersectoral actions developed together with community participation (nongovernmental social organizations and civil society), which add up to 12 documents from the 20 analyzed.17,25–35 This recommendation is particularly emphasized in some of the reviewed studies17,37–40 and also by studies that do not address specific intersectoral actions but underline the need for intersectoral strategies to be necessarily accompanied by social participation (local decision-makers and community membership).6,44–46 It is interesting to note that four studies36–40 presented territorial intersectoral strategies in areas in neighbourhoods, which did not originate from central government policies, but were the result of the local community organization and stakeholders. These studies based their analysis on the argument that strong cohesion and production of a social capital, in addition to economic improvements, is very important for reducing social inequities in certain areas, especially when problems involve violence, poverty and security.20,40,47,48
Although intersectorality is denoted as essential to obtain good results from the policies implemented, the studies indicate that important administrative and managerial difficulties need to be overcome. The problems highlighted concern difficulties in surmounting a prevailing sectoral logic that makes cooperation, distribution of responsibilities and operational actions unfeasible. Moreover, difficulties related to governments promoting the decentralisation of power and deliberative capacity to intersectoral forums and obstacles to civil society organising itself in a cohesive manner to claim its rights to increased political power, are important factors.17,26,45,49
Andrade et al.17 presented as a complication in the implementation of intersectoral projects, the fact of the technical unpreparedness of managers. The need to create a cooperative culture in management and administrative relationships, together with technical training for intersectoral management, is fundamental.
According to our theoretical framework, eight documents reported on intersectoral actions and social participation using as theoretical reference of the SDH model of the CSDH-WHO associated with the social capital. 25,26,30–35 This data can be interpreted by associating the result referring to the variables, that is, the studies strongly emphasized the need to develop intersectoral actions associated with social participation and the importance of besides the economic social determinants also to strengthen the social bonds of the community involved in the project.
According to reduction in social health inequities, studies reviewed showed improvements in the following main areas: increased access to health services, increase in prenatal examinations, reduction in malnutrition and child mortality, prevention and reduction communicable and noncommunicable diseases, reduction in epidemics, prevention on HIV transmission, decrease in cardiovascular risk factors, increase access to healthy food. Positive results were also presented: increasing in access to education, transportation, housing, healthy environment, reduction of violence and creation of safer areas, reduction of poverty, socioeconomics improvements, decreased barriers to gender, employment, increase of social capital, etc.17,26–42 So according to the studies the overall results were positive and many advances in relation to the social determinants of health can be observed.50,51
Although advances can be verified in many countries, social inequities are still predominant factors marking health inequities and obstacles to the establishment of equity.17,28,34,36,42 In poor countries, policies that address the social determinants of health and the reduction of inequities are fragmented and show discontinuity in their implementation, management and inspection. Local governments show important differences in the pace and demarcation of priorities with which policies are implemented, creating gaps between regions in the same country.52,53 Concerning Latin American countries, there are problems related to strong cultural, ethnic and gender issues, and poverty which need to be addressed in order to implement intersectoral projects aimed at producing health equity.2,17
Although studies show that important SDH policies in Europe have been successfully implemented there are significant disparities between Eastern and Western Europe. Eastern European countries present health problems and inequities in health access that are as severe as the world's poorest countries.4,6,26,52 Similar to Eastern Europe, other studies reiterate that Iberian countries have high rates of health inequities.13,18,45,52–54It is interesting to note that all the documents initially collected had titles containing the central theme of the social determinants of health, social inequities and mentioned or recommended intersectorality as a coping strategy. However, only 20 documents focused directly on policies, strategies and/or actions that concretely applied intersectoral programmes focused on the social determinants of health and were combined with social participation. This observation is reinforced by the work of Pons-Vigués et al.39, which emphasizes the current tendency of an increase in academic-scientific productions on this subject, while countries still face enormous difficulties in achieving intersectoral experiences. This is due to the strong impregnation of the anachronistic logics of state and governance management, fragmented and cemented in sectorial interests, as well as the highly centralised manifestation of political power in national governments, without the necessary decentralisation of power to local governments and civil society. These observations were also mentioned by other studies.55,56
Results from the intersectoral experiences reported in the studies reviewed herein show significant advances in reducing health inequities, increasing access to services and improving the quality of life for the groups and populations involved.
Future studies are required to deepen new diagnoses on the subjects researched and to strengthen the strategies that aim to transform the forms of global governance in various localities across the planet towards social equity and health.
One limitation of this research is the range of studies reviewed; expansion of the search strategies in other databases is important so that studies in other regions of the planet can be analysed. The revised documents are predominantly derived from research developed in countries of the Western world. In addition, the literature evaluating or describing the impact of intersectoral actions on health is limited, something that has been observed by other review studies.15,51
This paper was an important initial step towards a deeper study of the theme investigated. In line with the WHO's objectives of eradicating global poverty by 2050, aimed at global health equity, global multi-sectoral, intersectoral and transnational cooperation actions will be increasingly needed. Therefore, studies like this and additional evidence are needed to show that intersectoral policies and/or combined with social participation can have an impact on the social determinants of health and on reducing social and health inequities.
The studies showed significant health outcomes and advanced in reduction social inequities. On the other hand, they also showed that enormous obstacles stand in the way of equity, participation and the expansion of democratic management objectives. Social mobilization is needed in the search for empowerment in the implementation of equitable social policies and more democratic and more participatory forms of governance, together with greater technical capacity in the exercise of intersectoral management.
Editor in chargeClara Bermúdez-Tamayo.
Authorship contributionsR.C. Fiorati developed the research, data collection and analysis and elaborated the manuscript. P. Serrano Gallardo guided the study, developed the research, data collection and analysis and elaborated the manuscript. J. Segura del Pozo, M. Ramasco Gutiérrez and R. Alexandre Arcêncio participated in the analysis of the data, reviewed the successive manuscripts and the final version.
FundingThis work was supported by the São Paulo Research Foundation (FAPESP), Brazil, under grant no. 2015/00746-8.
Conflicts of interestNone.











