



Over the past two decades, deaths from cardiovascular diseases (CVDs) have been declining in high-income countries, but have increased in low and middle-income countries.1,2 There is a lack of data across European countries in relation to CVD in migrants and minority ethnic groups.3,4 Spain is a common touristic destination for European Union citizens, but also for people from other continents, specially Latin America and Africa.5 As they come from different geographical areas and the reason to visit our country is different, we hypothesize that the profile of CVD is different too. To know these differences we conducted a retrospective study of foreign citizens admitted to Hospital General Universitario de Alicante from 2000 to 2012. Patients were divided in two groups:
- 1)
Foreign citizens from high-income countries (FCHICs): European Union, United States, Canada, Australia and New Zealand.
- 2)
Foreign citizens from low and middle-income countries (FCLMICs): Latin America, North Africa, Sub-Saharan Africa, Eastern Europe and Asia.
The following variables were collected: demographic characteristics, nationality and diagnosis at discharge. We used IBM SPSS© 21.0 version for statistical analysis.
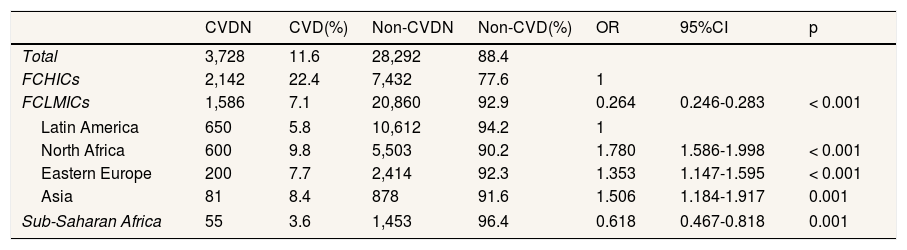
In the period 2000-2012, a total of 387,862 patients were admitted to the hospital, of whom 32,020 were foreign citizens, representing an 8.2% of admissions. Within this group of patients, 3,728 (11.6%) had a discharge final diagnosis of CVD. Table 1 shows admissions for CVD vs. non-CVD in foreign citizens from high-income countries and from low and middle-income countries and also among regions of low and middle-income countries. The percentage of women was higher in low and middle-income countries than in high-income countries (36% vs. 26.9%) (odds ratio: 1.53; 95% confidence interval: 1.33–1.76; p<0.001), being Latin American women the majority in this group. Foreign citizens from low and middle-income countries were younger than those from high-income countries (median age, 57.9 vs. 67.2; p<0.001). According to region of origin, patients from Sub-Saharan Africa were the youngest (median: 37.8 years). Prevalence of admission for CVD in low and middle-income countries was lower than in high-income countries (7.1% vs. 22.4%) (p<0.001). The most common diagnosis was coronary heart disease (37.3%), followed by vascular disease (25.9%), arrhythmia (13.7%), myocardiopathy and heart failure (7.9%), valvular heart disease (6.8%), hypertension (5.5%), pulmonary hypertension/pulmonary embolism (2.1%) and pericarditis (0.8%). Accordingly to country of origin, United Kingdom had the highest percentage of coronary heart disease (31.6%), Morocco and Algeria were the countries with more admissions because of valvular heart disease (17.1% and 8.3% respectively), the majority of cases of pericarditis came from Morocco (21.4%) and Ecuador (17.9%), and 17.7% cases of pulmonary hypertension and pulmonary embolism came from Argentina. In the group of high-income countries the prototype patient was a man in his sixties with coronary heart disease from an European high-income country, while in the group of low and middle-income countries the profile was a woman in her fifties with a long-term myocardiopahty or valvular heart disease, coming from a Latin American or North African country.
Cardiovascular and non-cardiovascular disease admissions of foreign citizens from high-income, low and middle-income countries admitted to Hospital General Universitario de Alicante from 2000 until 2012.
| CVDN | CVD(%) | Non-CVDN | Non-CVD(%) | OR | 95%CI | p | |
|---|---|---|---|---|---|---|---|
| Total | 3,728 | 11.6 | 28,292 | 88.4 | |||
| FCHICs | 2,142 | 22.4 | 7,432 | 77.6 | 1 | ||
| FCLMICs | 1,586 | 7.1 | 20,860 | 92.9 | 0.264 | 0.246-0.283 | < 0.001 |
| Latin America | 650 | 5.8 | 10,612 | 94.2 | 1 | ||
| North Africa | 600 | 9.8 | 5,503 | 90.2 | 1.780 | 1.586-1.998 | < 0.001 |
| Eastern Europe | 200 | 7.7 | 2,414 | 92.3 | 1.353 | 1.147-1.595 | < 0.001 |
| Asia | 81 | 8.4 | 878 | 91.6 | 1.506 | 1.184-1.917 | 0.001 |
| Sub-Saharan Africa | 55 | 3.6 | 1,453 | 96.4 | 0.618 | 0.467-0.818 | 0.001 |
CI: confidence interval; CVD: cardiovascular disease; FCHICs: foreign citizens from high-income countries; FCLMICs: foreign citizens from low and middle-income countries; OR: odds ratio.
The main limitation of the present study is that it is focused only in admitted patients, not including out-patient consultations or visits to the emergency room, so we have only analyzed the most severe cases that required hospital admission. Patients from low and middle-income countries are younger than patients from high income countries, leading to a lower number of admissions in this group because coronary heart disease but not for other CVDs (as valvular heart disease or pericarditis). Additionally, it is important to note that patients with severe CVDs have difficulties for travelling abroad, so we could have been seeing only the “tip of the iceberg”, those who arrived to our country. In the same way, some foreign citizens returned to their countries when they were recovered, limiting their follow-up.
In summary, we can conclude that the profile of CVDs in high-income countries and low and middle-income countries is different. Differences according to country of origin are discovered when a large group of people is analyzed.
Authorship contributionsThis manuscript has not been submitted to another journal and all authors have made substantial contributions to all of the following: 1) conception and design of the study, acquisition of data, analysis and interpretation of data, 2) drafting the article or revising it critically for important intellectual content, 3) final approval of the version to be submitted.
FundingNone.
Conflicts of interestThe authors declare that they have no competing interests.











