



Socio-economical changes in Europe are leading to the rise of new issues regarding the labour market and health of young workers. Job insecurity is a widely studied phenomenon that involves an increasing number of young workers. We investigated its association with mental health and hazardous behaviours.
MethodIn this pilot study, 504 subjects aged between 18 and 40 were interviewed. STROBE guidelines were used. Socio-economic factors were evaluated. Adapted forms of validated scales were used to assess depression, anxiety disorder, alcohol and drug abuse and smoking habit. Univariate and multivariate analyses were performed.
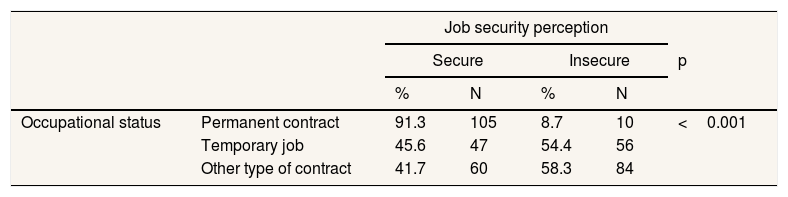
ResultsJob insecurity appeared to be partially connected with the type of employment. Most respondents with a permanent contract felt their situation was secure, while this proportion was reduced when referring to temporary jobs and other kinds of contract (p <0.001). Job security perception was associated with depression, anxiety, alcohol abuse and smoking habit (p <0.001).
ConclusionsJob security perception appears to be the most important predictive factor for the presence of depression and anxiety symptoms, alcohol consumption and smoking habit compared to other socio-economic factors under study.
Los cambios socioeconómicos en Europa están provocando el surgimiento de nuevas cuestiones sobre la salud de los trabajadores jóvenes. La inseguridad laboral es un fenómeno que involucra una cantidad creciente de trabajadores jóvenes. Nuestro estudio tiene como objetivo investigar la asociación entre inseguridad laboral y salud mental y comportamientos peligrosos.
MétodoEn este estudio piloto fueron entrevistados 504 sujetos con edades comprendidas entre 18 y 40 años. Se evaluaron los factores socioeconómicos. Se usaron formas adaptadas de escalas validadas para evaluar la depresión, la ansiedad, el abuso de alcohol y drogas, y el hábito de fumar. Se realizaron análisis univariados y multivariados.
ResultadosLa mayoría de los encuestados con contrato permanente consideró que su situación era segura, mientras que esta proporción se redujo al referirse a trabajos temporales y otros tipos de contrato (p <0,001). La percepción de la seguridad laboral se asoció con la depresión, la ansiedad, el abuso de alcohol y el hábito de fumar (p <0,001).
ConclusionesLa percepción de la seguridad laboral parece ser el factor predictivo más importante para la presencia de síntomas de depresión y ansiedad, el consumo de alcohol y el hábito de fumar, en comparación con otros factores socioeconómicos en estudio.
In the last decades, social and economical changes in Western Countries caused deep changes in the labour market. Particularly, unemployment and flexibility have grown, leading to the new concept of job insecurity.1 In particular, job insecurity is defined as “the discrepancy between the level of job security a person experiences and the level she might prefer”.2
Within the European Union (EU), the number of employed people is still lower than it used to be before the 2008 crisis by 2.2 million workers.3 Specifically, talking about the Italian situation, the occupational rate shows an overall fall of 2.3% in 2008, whereas the occupational rate among the youth population (15-34 years old) is still 16.5% below the EU average rate.3 Data describe a growth of short-term workers within the total employed population in the EU, increasing from 17.5% to 19.6%, between 2008 and 2015.3 Moreover, about 50% of short-term contracts last less than one year and only 20% of them last at least 12 months.3 This trend is more common among the young workers population. Among workers aged 20 to 24, the rate of short-term employees has risen from 19.4% to 45.6% among the men population and from 26.1% to 49.5% among women. We can also see an increase for men and women aged 25 to 29 and 30 to 34 years old.3
The role played by occupation as a health determinant is well known, but the need of a better comprehension of the job insecurity has also emerged. Many studies assessed the spatial and temporal work's flexibility impact on health. However, the evidence on this possible association is not consistent. A meta-analysis considering 27 studies4 has demonstrated the existence of an association between short-term jobs and poor mental health. This association seems to be stronger when the insecurity grows, and it changes according to gender and social background. There are also other studies which not only underline the associations between short-term contracts and poor psychological outcomes, but do also prove a causal connection between them.5–8 At the same time the literature present a variety of results9–11 that could be related to the variety of outcomes assessed in these papers. Other studies show how lower income,12 reduced access to benefits and poorer future perspectives13–15 or gender16 can affect the association. The results are not easily generalized, because each country has its own welfare system, providing different plans of assistance to its citizens. In light of this, it seems to be clear that job insecurity needs to be better assessed as a social determinant of health. Our research aimed to explore the job insecurity as a possible risk factor for poor mental health, alcohol and drugs abuse and smoking habit in the Southern Europe context. This pilot study was used to identify the key points and possibly relevant aspects that can help this assessment.
MethodThe team performed a cross-sectional pilot study in the city of Torino, Italy. STROBE guideline for observational studies was used for reporting.17 The participants (18-40 years old) were enrolled by using a convenience sample, recruited in public recreational areas, like concerts club and bars, between April and June 2016. The participants were informed about the study and signed the informed consent. Two researchers performed direct personal interviews. Each interview lasted around 20minutes. Different Italian translated evaluation scales were used to evaluate the presence of mental health problems, drug and alcohol abuse and tobacco addiction.
Sample size calculationThe sample size has been defined according to demographic data for population aged between 18 and 40 living in Torino.18 The total number of people who fits these characteristics is 224.767. Our sample size was calculated using both the expected frequency of 45.6% of young men with a temporary job and the expected frequency of 49.5% of young women with a temporary job.3 The sample size calculation gave us a result of 380 interviews to be performed according to the frequency of temporary job in men, and 386 interviews to be performed according to female ones. In order to be conservative, we planned to enrol 500 subjects. The sample size has been calculated using EpiInfo software.
Questionnaires and scalesThe questionnaire was composed of sixty multiple-choice questions. The first fifteen questions assessed socio-economic factors (gender, age, nationality, family status and structure, educational level, occupational status and perception and income level and perception). In particular, question 11 asked whether the subject perceived his own occupational status as very secure, quite secure, quite insecure or very insecure. During the analyses process this variable were recorded in “secure” for quite secure and very secure answers, and in “insecure” for very insecure and quite insecure answers. The other questions were used to screen and assess clinical health outcomes and substances consumption habits. The Italian translated versions of the following validated scales were used; the Patient Health Questionnaire-9 is a self-administered questionnaire used for screening purposes towards depression symptoms,19 according to DSM-IV cut-offs.20 To assess the anxiety symptoms the Generalized Anxiety Disorder-7 was used.21 The alcohol consumption was screened with the Alcohol Use Disorder Identification Test (AUDIT), developed by the WHO.22 The Drug Abuse Screening Test (DAST-10) was used to assess the presence and severity of drugs consumption/abuse.23 To screen nicotine addiction, the sample answered to the Fagerstrom Test for Nicotine Dependence.24 Questionnaires were administered after delivering information about privacy terms and conditions. Further information were provided when necessary. Finally, the questionnaires were completed ensuring the proper privacy, while the information was stored anonymously.
Statistical analysisThe statistical analysis was conducted with STATA MP13 software (Stata Corp., College Station, TX, 2013). A descriptive analysis was conducted. Frequencies and percentages of the categorical variables were reported. The sample was stratified for gender, perceived job security and occupational status, performing a univariate analysis. To assess predictors of depression, anxiety, alcohol consumption, illegal substances usage and smoking habit, a multivariate regression analysis was conducted using a stepwise forward approach throughout five different models of ordered logistic regression.25 The included independent variables were gender, age, nationality, familiar status, occupational status, job security perception, salary perception, presence of congenital pathologies and study title. The included independent variables were selected considering the main risk factors for poor mental health and risky behaviours pointed out by the scientific literature.5–13,16,26–35 Finally, the results were reported as Odds Ratios values with their related 95% confidence intervals and p-values. All the results were considered statistically significant when the p-value was below 0.05.
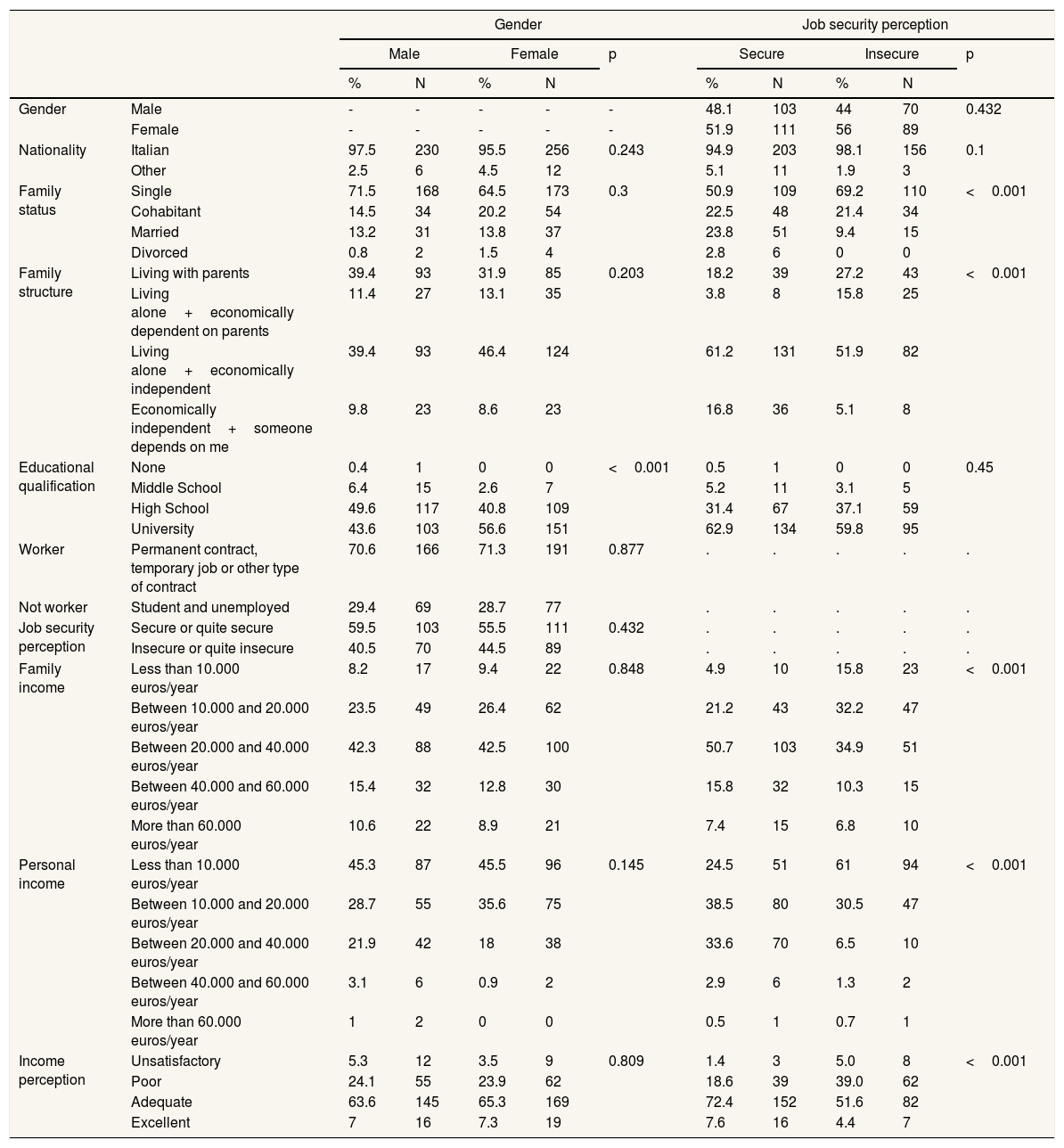
ResultsThe final sample size for the pilot study consisted of 504 subjects. In Table 1 the main demographic, occupational and social features of the sample are resumed stratified by gender and perception of job security. Data show how the workers who perceive their job situation as insecure are more often unmarried (69.2% vs. 50.9%; p <0.001). Speaking about family structure and economical independence, it is shown that insecure workers more often live with their parents than the secure workers do (27.2% vs. 18.2%; p <0.001) or do still rely economically on them, even when living on their own (15.8% vs. 3.8%; p <0.001). On the other hand, a larger proportion of secure workers lives on its own and is not only more frequently economically independent (61.2% vs. 51.9%; p <0.001), but it also appears to share more often part of its income with parents and/or relatives (16.8% vs. 5.1%; p <0.001). These differences may be partially explained with the difference in mean age. The mean age in the secure group is 30,05±5,23 years while in the insecure group is 28,01±4,56 years (p <0.001). While no statistically significant differences are shown between secure and insecure workers on the basis of their educational qualification, relevant differences appear to exist among the different kind of job contract in the sample. Analysing the association between familiar and individual annual income groups and the perception of job security or insecurity, Table 1 shows that both groups feel their situation as insecure. By assessing the association between the perception of personal income and job security, it emerged that workers who describe themselves secure are more likely to consider their income adequate (72.4% vs. 51.57%; p <0.001) or excellent (7,6% vs. 4.4%; p <0.001), while, on the other side, perceived job insecurity may lead to consider the income as unsatisfactory (5% vs. 1.4%; p <0.001) or poor (39% vs. 18.6%; p <0.001).
Socio-demographic data stratified by gender and job security perception.
| Gender | Job security perception | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | p | Secure | Insecure | p | ||||||
| % | N | % | N | % | N | % | N | ||||
| Gender | Male | - | - | - | - | - | 48.1 | 103 | 44 | 70 | 0.432 |
| Female | - | - | - | - | - | 51.9 | 111 | 56 | 89 | ||
| Nationality | Italian | 97.5 | 230 | 95.5 | 256 | 0.243 | 94.9 | 203 | 98.1 | 156 | 0.1 |
| Other | 2.5 | 6 | 4.5 | 12 | 5.1 | 11 | 1.9 | 3 | |||
| Family status | Single | 71.5 | 168 | 64.5 | 173 | 0.3 | 50.9 | 109 | 69.2 | 110 | <0.001 |
| Cohabitant | 14.5 | 34 | 20.2 | 54 | 22.5 | 48 | 21.4 | 34 | |||
| Married | 13.2 | 31 | 13.8 | 37 | 23.8 | 51 | 9.4 | 15 | |||
| Divorced | 0.8 | 2 | 1.5 | 4 | 2.8 | 6 | 0 | 0 | |||
| Family structure | Living with parents | 39.4 | 93 | 31.9 | 85 | 0.203 | 18.2 | 39 | 27.2 | 43 | <0.001 |
| Living alone+economically dependent on parents | 11.4 | 27 | 13.1 | 35 | 3.8 | 8 | 15.8 | 25 | |||
| Living alone+economically independent | 39.4 | 93 | 46.4 | 124 | 61.2 | 131 | 51.9 | 82 | |||
| Economically independent+someone depends on me | 9.8 | 23 | 8.6 | 23 | 16.8 | 36 | 5.1 | 8 | |||
| Educational qualification | None | 0.4 | 1 | 0 | 0 | <0.001 | 0.5 | 1 | 0 | 0 | 0.45 |
| Middle School | 6.4 | 15 | 2.6 | 7 | 5.2 | 11 | 3.1 | 5 | |||
| High School | 49.6 | 117 | 40.8 | 109 | 31.4 | 67 | 37.1 | 59 | |||
| University | 43.6 | 103 | 56.6 | 151 | 62.9 | 134 | 59.8 | 95 | |||
| Worker | Permanent contract, temporary job or other type of contract | 70.6 | 166 | 71.3 | 191 | 0.877 | . | . | . | . | . |
| Not worker | Student and unemployed | 29.4 | 69 | 28.7 | 77 | . | . | . | . | . | |
| Job security perception | Secure or quite secure | 59.5 | 103 | 55.5 | 111 | 0.432 | . | . | . | . | . |
| Insecure or quite insecure | 40.5 | 70 | 44.5 | 89 | . | . | . | . | . | ||
| Family income | Less than 10.000 euros/year | 8.2 | 17 | 9.4 | 22 | 0.848 | 4.9 | 10 | 15.8 | 23 | <0.001 |
| Between 10.000 and 20.000 euros/year | 23.5 | 49 | 26.4 | 62 | 21.2 | 43 | 32.2 | 47 | |||
| Between 20.000 and 40.000 euros/year | 42.3 | 88 | 42.5 | 100 | 50.7 | 103 | 34.9 | 51 | |||
| Between 40.000 and 60.000 euros/year | 15.4 | 32 | 12.8 | 30 | 15.8 | 32 | 10.3 | 15 | |||
| More than 60.000 euros/year | 10.6 | 22 | 8.9 | 21 | 7.4 | 15 | 6.8 | 10 | |||
| Personal income | Less than 10.000 euros/year | 45.3 | 87 | 45.5 | 96 | 0.145 | 24.5 | 51 | 61 | 94 | <0.001 |
| Between 10.000 and 20.000 euros/year | 28.7 | 55 | 35.6 | 75 | 38.5 | 80 | 30.5 | 47 | |||
| Between 20.000 and 40.000 euros/year | 21.9 | 42 | 18 | 38 | 33.6 | 70 | 6.5 | 10 | |||
| Between 40.000 and 60.000 euros/year | 3.1 | 6 | 0.9 | 2 | 2.9 | 6 | 1.3 | 2 | |||
| More than 60.000 euros/year | 1 | 2 | 0 | 0 | 0.5 | 1 | 0.7 | 1 | |||
| Income perception | Unsatisfactory | 5.3 | 12 | 3.5 | 9 | 0.809 | 1.4 | 3 | 5.0 | 8 | <0.001 |
| Poor | 24.1 | 55 | 23.9 | 62 | 18.6 | 39 | 39.0 | 62 | |||
| Adequate | 63.6 | 145 | 65.3 | 169 | 72.4 | 152 | 51.6 | 82 | |||
| Excellent | 7 | 16 | 7.3 | 19 | 7.6 | 16 | 4.4 | 7 | |||
Table 2 describes how the large majority of those who have a permanent contract feel their situation as secure, while this proportion is reduced by about its half when referring to temporary jobs and other kinds of contract (p <0.001).
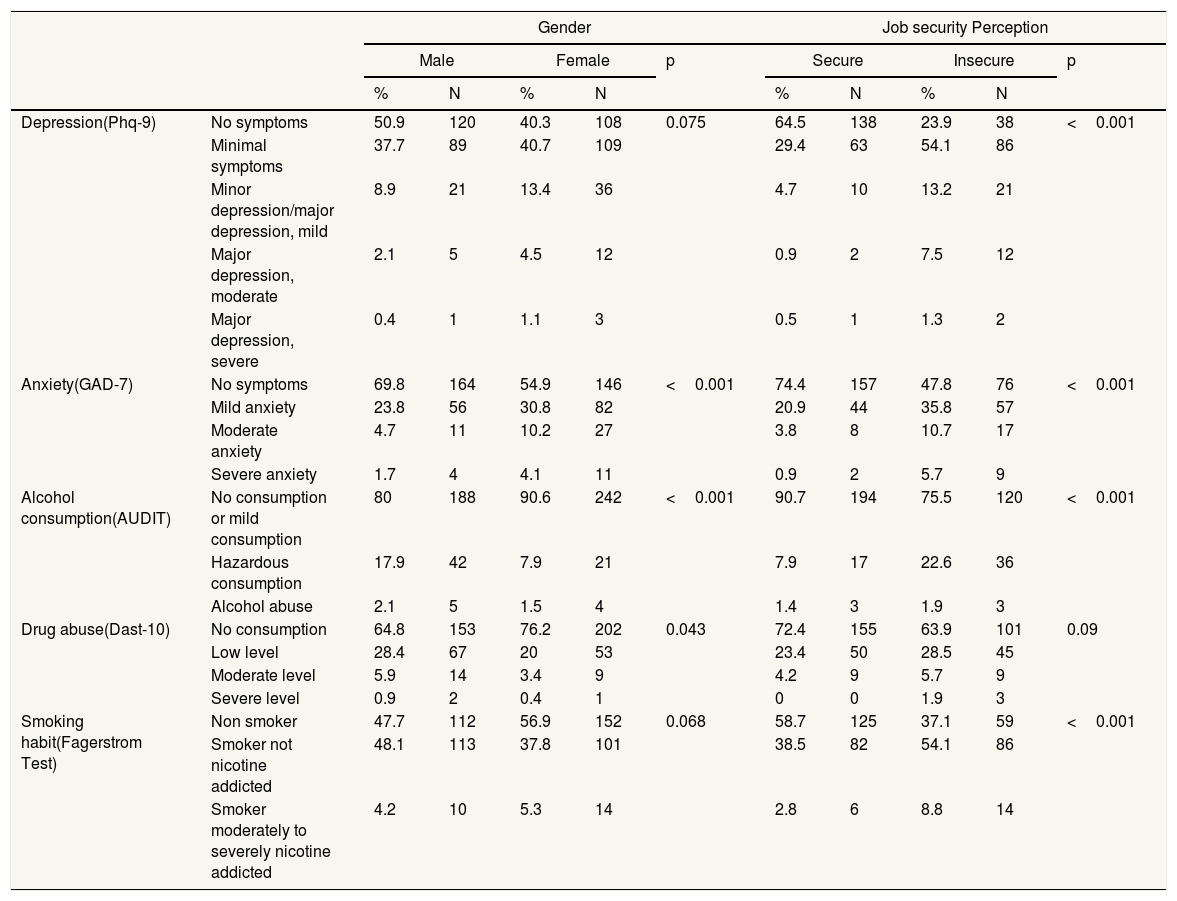
Table 3 shows the main differences regarding mental problems’ and substances consumption's prevalence between the male and the female population. A statistically significant higher proportion of anxiety disturbance is recorded in the female population (30.8% show mild anxiety, 10.2% moderate anxiety and 4.1% severe generalized anxiety disorder, versus 23.8%, 4.7% and 1.7% respectively for the male population; p <0.001). On the other side, the male population appears to be statistically significant more related towards hazardous alcohol consumption (17.9% vs. 7.9%; p <0.001). The same statistically significant results are shown for drugs abuse (p=0.043).
Mental health and hazardous habits outcome stratified by gender and job security perception.
| Gender | Job security Perception | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | p | Secure | Insecure | p | ||||||
| % | N | % | N | % | N | % | N | ||||
| Depression(Phq-9) | No symptoms | 50.9 | 120 | 40.3 | 108 | 0.075 | 64.5 | 138 | 23.9 | 38 | <0.001 |
| Minimal symptoms | 37.7 | 89 | 40.7 | 109 | 29.4 | 63 | 54.1 | 86 | |||
| Minor depression/major depression, mild | 8.9 | 21 | 13.4 | 36 | 4.7 | 10 | 13.2 | 21 | |||
| Major depression, moderate | 2.1 | 5 | 4.5 | 12 | 0.9 | 2 | 7.5 | 12 | |||
| Major depression, severe | 0.4 | 1 | 1.1 | 3 | 0.5 | 1 | 1.3 | 2 | |||
| Anxiety(GAD-7) | No symptoms | 69.8 | 164 | 54.9 | 146 | <0.001 | 74.4 | 157 | 47.8 | 76 | <0.001 |
| Mild anxiety | 23.8 | 56 | 30.8 | 82 | 20.9 | 44 | 35.8 | 57 | |||
| Moderate anxiety | 4.7 | 11 | 10.2 | 27 | 3.8 | 8 | 10.7 | 17 | |||
| Severe anxiety | 1.7 | 4 | 4.1 | 11 | 0.9 | 2 | 5.7 | 9 | |||
| Alcohol consumption(AUDIT) | No consumption or mild consumption | 80 | 188 | 90.6 | 242 | <0.001 | 90.7 | 194 | 75.5 | 120 | <0.001 |
| Hazardous consumption | 17.9 | 42 | 7.9 | 21 | 7.9 | 17 | 22.6 | 36 | |||
| Alcohol abuse | 2.1 | 5 | 1.5 | 4 | 1.4 | 3 | 1.9 | 3 | |||
| Drug abuse(Dast-10) | No consumption | 64.8 | 153 | 76.2 | 202 | 0.043 | 72.4 | 155 | 63.9 | 101 | 0.09 |
| Low level | 28.4 | 67 | 20 | 53 | 23.4 | 50 | 28.5 | 45 | |||
| Moderate level | 5.9 | 14 | 3.4 | 9 | 4.2 | 9 | 5.7 | 9 | |||
| Severe level | 0.9 | 2 | 0.4 | 1 | 0 | 0 | 1.9 | 3 | |||
| Smoking habit(Fagerstrom Test) | Non smoker | 47.7 | 112 | 56.9 | 152 | 0.068 | 58.7 | 125 | 37.1 | 59 | <0.001 |
| Smoker not nicotine addicted | 48.1 | 113 | 37.8 | 101 | 38.5 | 82 | 54.1 | 86 | |||
| Smoker moderately to severely nicotine addicted | 4.2 | 10 | 5.3 | 14 | 2.8 | 6 | 8.8 | 14 | |||
The perceived job security among the workers interviewed in this study seems to be also related to mental disturbances and substances use and/or abuse: secure workers showed less depression symptoms than insecure workers (p <0.001) as reported in Table 3. The same pattern is noticeable for the presence of anxiety-related symptoms (p <0.001). For what it concerns alcohol consumption and tobacco addiction, we can still find a preponderance among insecure workers rather than secure (p <0.001).
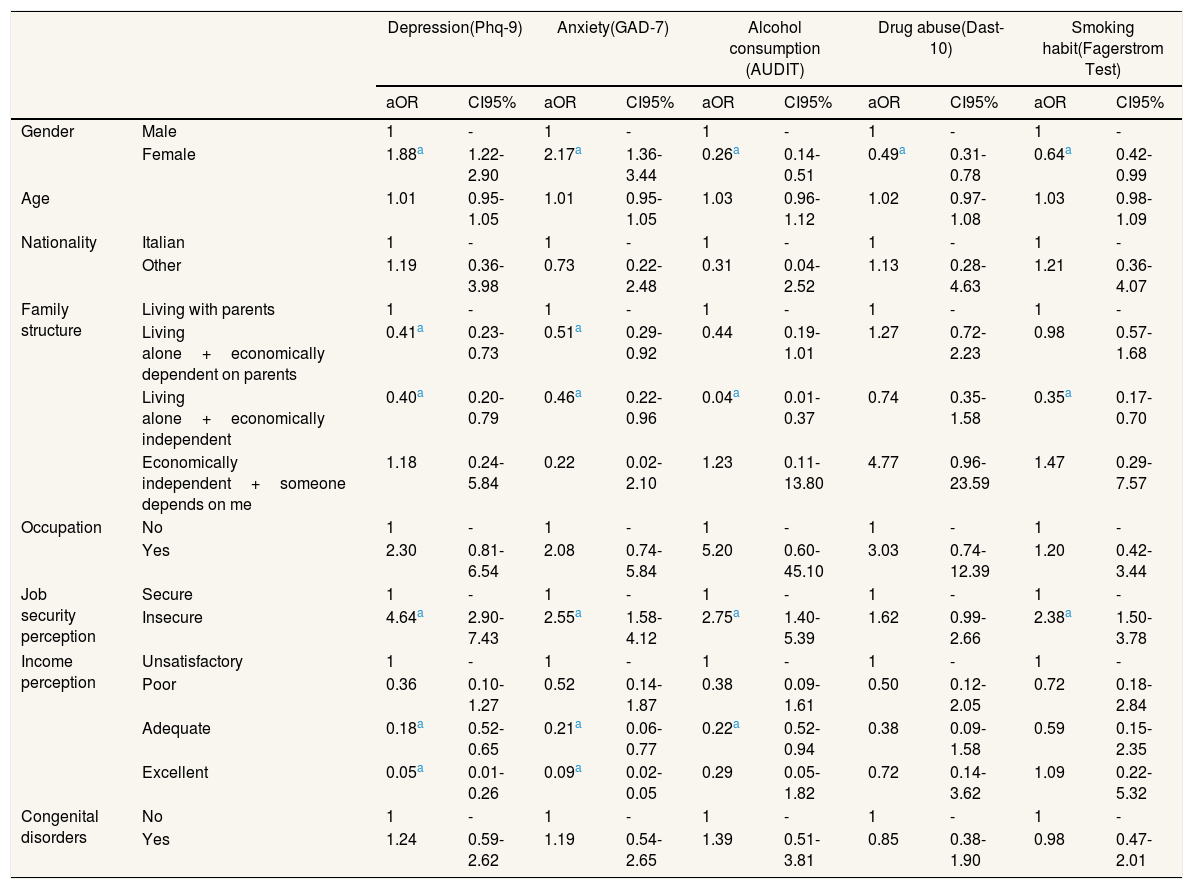
Multivariate analysisTable 4 identifies, through an ordered logistic regression, the presence of potential predictors related to the clinical outcomes assessed. Firstly, it is noticeable how the female gender appears to be a predictor of depression (odds ratio [OR]: 1.88; 95% confidence interval [95%CI]: 1.22-2.90; p=0.004). Referring to family status, apparently those who live alone, both economically dependent and independent, appear to be protected from developing depressive symptoms (OR: 0.41; 95%CI: 0.23-0.73; p=0.002 for dependents who live alone; OR: 0.40; 95%CI: 0.20-0.79; p=0.008 for independents living alone). Another important positive predictor of depressive disturbances is the perception of job insecurity (OR: 4.64; 95%CI: 2.90-7.43; p <0.001), while the presence of an adequate (OR: 0.18; 95%CI: 0.05-0.65; p=0.009) or of a high income (OR: 0.05; 95%CI: 0.01-0.26; p <0.001) may be a strong negative factors towards the development of depressive symptoms. Coherently, the analyses show that the same predictors which intervene in depressive outcomes are present for anxiety outcomes (female gender OR: 2.17; 95%CI: 1.36-3.44, p=0.001; living alone but relying economically on parents OR: 0.51; 95%CI: 0.29-0.92; p=0.04; to be economically independent OR: 0.46; 95%CI: 0.22-0.96; p=0.04). The perception of job insecurity is again a potential positive predictor for anxiety (OR: 2.55; 95%CI: 1.58-4.12; p <0.001). Presence of an adequate income seems to be a negative predictor for anxiety (OR: 0.21; 95%CI: 0.06-0.77; p=0.02), just as the presence of a high income (OR: 0.09; 95%CI: 0.02-0.51; p=0.006).
Ordered multivariate analysis (including gender, age, nationality, family structure, educational qualification, occupation, job security perception, income perception and congenital disorder).
| Depression(Phq-9) | Anxiety(GAD-7) | Alcohol consumption (AUDIT) | Drug abuse(Dast-10) | Smoking habit(Fagerstrom Test) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| aOR | CI95% | aOR | CI95% | aOR | CI95% | aOR | CI95% | aOR | CI95% | ||
| Gender | Male | 1 | - | 1 | - | 1 | - | 1 | - | 1 | - |
| Female | 1.88a | 1.22-2.90 | 2.17a | 1.36-3.44 | 0.26a | 0.14-0.51 | 0.49a | 0.31-0.78 | 0.64a | 0.42-0.99 | |
| Age | 1.01 | 0.95-1.05 | 1.01 | 0.95-1.05 | 1.03 | 0.96-1.12 | 1.02 | 0.97-1.08 | 1.03 | 0.98-1.09 | |
| Nationality | Italian | 1 | - | 1 | - | 1 | - | 1 | - | 1 | - |
| Other | 1.19 | 0.36-3.98 | 0.73 | 0.22-2.48 | 0.31 | 0.04-2.52 | 1.13 | 0.28-4.63 | 1.21 | 0.36-4.07 | |
| Family structure | Living with parents | 1 | - | 1 | - | 1 | - | 1 | - | 1 | - |
| Living alone+economically dependent on parents | 0.41a | 0.23-0.73 | 0.51a | 0.29-0.92 | 0.44 | 0.19-1.01 | 1.27 | 0.72-2.23 | 0.98 | 0.57-1.68 | |
| Living alone+economically independent | 0.40a | 0.20-0.79 | 0.46a | 0.22-0.96 | 0.04a | 0.01-0.37 | 0.74 | 0.35-1.58 | 0.35a | 0.17-0.70 | |
| Economically independent+someone depends on me | 1.18 | 0.24-5.84 | 0.22 | 0.02-2.10 | 1.23 | 0.11-13.80 | 4.77 | 0.96-23.59 | 1.47 | 0.29-7.57 | |
| Occupation | No | 1 | - | 1 | - | 1 | - | 1 | - | 1 | - |
| Yes | 2.30 | 0.81-6.54 | 2.08 | 0.74-5.84 | 5.20 | 0.60-45.10 | 3.03 | 0.74-12.39 | 1.20 | 0.42-3.44 | |
| Job security perception | Secure | 1 | - | 1 | - | 1 | - | 1 | - | 1 | - |
| Insecure | 4.64a | 2.90-7.43 | 2.55a | 1.58-4.12 | 2.75a | 1.40-5.39 | 1.62 | 0.99-2.66 | 2.38a | 1.50-3.78 | |
| Income perception | Unsatisfactory | 1 | - | 1 | - | 1 | - | 1 | - | 1 | - |
| Poor | 0.36 | 0.10-1.27 | 0.52 | 0.14-1.87 | 0.38 | 0.09-1.61 | 0.50 | 0.12-2.05 | 0.72 | 0.18-2.84 | |
| Adequate | 0.18a | 0.52-0.65 | 0.21a | 0.06-0.77 | 0.22a | 0.52-0.94 | 0.38 | 0.09-1.58 | 0.59 | 0.15-2.35 | |
| Excellent | 0.05a | 0.01-0.26 | 0.09a | 0.02-0.05 | 0.29 | 0.05-1.82 | 0.72 | 0.14-3.62 | 1.09 | 0.22-5.32 | |
| Congenital disorders | No | 1 | - | 1 | - | 1 | - | 1 | - | 1 | - |
| Yes | 1.24 | 0.59-2.62 | 1.19 | 0.54-2.65 | 1.39 | 0.51-3.81 | 0.85 | 0.38-1.90 | 0.98 | 0.47-2.01 | |
aOR: adjusted odds ratio; 95%CI: 95% confidence interval.
Female gender is also shown as a statistically significant potential negative predictor in reference to alcohol consumption (OR: 0.26; 95%CI: 0.14-0.51; p <0.001), just as economical independence (OR: 0.04; 95%CI: 0.01-0.37; p=0.004) and the presence of an adequate salary (OR: 0.22; 95%CI: 0.5-0.94; p=0.04). On the opposite side, the perception of job insecurity appears to be a positive predictor for alcohol use or abuse (OR: 2.75; 95%CI: 1.40-5.39; p=0.003). Female gender also appears to be a negative predictor towards drugs abuse (OR: 0.49; 95%CI: 0.31-0.78; p=0.003).
Referring to smoking habit and tobacco addiction, the female gender is again a statistically significant potential negative predictor (OR: 0.64; 95%CI: 0.42-0.99; p=0.04), together with economical independence (OR: 0.35; 95%CI: 0.17-0.70; p=0.003). The perception of job insecurity is instead a potential positive predictor for smoking habit (OR: 2.38; 95%CI: 1.50-3.78; p <0.001).
DiscussionThe association between unemployment and mental disturbances in the young population has been widely investigated, especially during the last decade, since the worldwide financial crisis started to display its influence on society. The increase of mental illnesses’ incidence among the unemployed young population appears to be a common trend in all European countries.26 Other studies conducted in Southern Europe countries have not only confirmed this trend, but have also pointed out a major association between unemployment and mood disorders, particularly with depression and anxiety.27–29 Moreover, similar results were found in other non-European countries, suggesting a possible important role of the crisis in the influence of labour market changes and on related health issues across the world.30,31 According to our preliminary results, the perception of job insecurity appears to be related not only to mental disturbances, but also to hazardous behaviours. These findings are confirmed in literature.32,33 In particular, one study found no significant differences between unemployed and subjects with an insecure work status according to the association with mental illnesses and substances abuse.34
Furthermore, this pilot study shows that an adequate or excellent income is a protective factor of depressive/anxious symptoms and alcohol intake, differing from one other study.35
In conclusion, the analysis of the existence of associations within labour market and mental health issues may lead to controversial conclusions. Because of this, it is important to study and consider all the main aspects that could intervene and influence specific outcomes. It is necessary to perform other specific longitudinal studies and to develop a strong advocacy of labour's policy making, coherent with the special needs of this specific portion of young workers.
Moreover, it is important to underline both points of strength and weakness of the study. First of all, few similar studies have been conducted to analyse the young worker's situation after the 2008 financial crisis. All the included studies collected data from different countries, thus making them difficult to compare among each other, since each country has its own welfare system. Moreover, a set of different validated scales was used to strengthen the assessment of the outcomes. On the other hand, the way the sample was selected, and the pilot study design may have led to selection biases and it cannot be considered as fully representative of the population of Italian young workers; at the same time, cross-sectional studies cannot give strong evidence of causal connections among the different variables. Another potential limitation of this and other studies that touch sensitive topics is the risk of underreporting of some important data about mental health problems or substances abuse. Since these topics have been assessed with questionnaires, the interviewed subjects may have omitted some information about their real condition.
This pilot study conducted in a single Italian city provided important information about how to perform more specific multicentre studies with larger sample sizes. These studies could explore this issue in southern Europe, in order to point out potential differences with other economical systems, based on stronger evidence.
Ethical standardsThe authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1964 and its later amendments.
After 2008 economic crisis the labor market changed. Job insecurity increased among young worker. Few studies assessed the possible association with the increased job instability and poor mental health. In particular, lower income and gender seem to affect this association. But this condition could differ substantially from different areas in the world.
What does this study add to the literature?This pilot study try to outline this association among more than 500 young Italian worker. Furthermore, the study assess the possible association between job insecurity and drug use, smoking and drinking habit. Job security perception appears to be the most important predictive factor for the outcome assessed, affecting not only mental health but alcohol consumption and smoking habit.
Carlos Álvarez-Dardet.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsAll the authors substantially contributed in the conception and design of the work, data collection, analysis and/or interpretation of the data. They gave their contribution in writing the article or gave an important intellectual contribution. They all approved the final version of the paper. Furthermore, each of them agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
FundingNone.
Conflict of interestNone.











