



We implemented and evaluated the Parenting Skills Program for families in Spain 1) to examine differences in parenting skills, social support, children's behaviours and parental stress pre, immediately post and six months post intervention and 2) to identify mechanisms by which the intervention is related to changes in the four outcomes examined.
MethodsQuasi-experimental study design with pre (T0), post (T1), a follow-up (T2) and no control group, complemented by a qualitative study was used. The outcome variables were social support, parenting skills, parental stress and children's behaviours. 216 parents completed pre and post questionnaire and 130 parents the follow-up questionnaire. 39 professionals and 34 parents participated in 17 interviews and 5 discussion groups.
ResultsCompared with T0, all four outcomes improved significantly at T1. 76% of the participants improved parenting skills and 61% social support. 56% reduced children's negative behaviours and 66% parental stress. All outcomes maintained this significant improvement at T2. Parents and professionals describe different changes in parents’ parenting skills, stress and social support after participation in the PSP, and in their children's behaviours. Some subcategories emerged after analysing parents’ and professionals’ discourses.
ConclusionsThis study describes positive parenting effects on participants of a parent-training program in Spain, which is a country where implementation and evaluation of these kind of interventions is an incipient issue.
Se introdujo y evaluó el Programa de Habilidades Parentales para familias a fin de: 1) examinar las diferencias en cuanto a habilidades parentales, apoyo social, comportamientos infantiles y estrés parental preintervención, inmediatamente después y 6 meses después de la intervención, y 2) identificar los mecanismos que explican los cambios generados por la intervención para las cuatro variables examinadas.
MétodoEstudio cuasiexperimental con pre (T0), post (T1) y seguimiento (T2), sin grupo control, complementado con un estudio cualitativo. Variables: apoyo social, habilidades parentales, estrés parental y comportamientos infantiles. Completaron el cuestionario pre y post 216 padres/madres, y 130 el de seguimiento. Treinta y nueve profesionales y 34 padres/madres participaron en 17 entrevistas y cinco grupos de discusión.
ResultadosComparado con T0, las cuatro variables mejoraron significativamente en T1. El 76% de los participantes mejoraron las habilidades parentales y el 61% el apoyo social. El 56% redujo los comportamientos infantiles negativos y el 66% el estrés parental. Las variables mantuvieron significativa la mejora en T2. Padres/madres y profesionales describieron cambios en las cuatro variables tras participar en el Programa de Habilidades Parentales. Surgieron subcategorías tras el análisis discursivo.
ConclusionesEste estudio describe efectos positivos en la parentalidad de los participantes en un programa de educación parental español, siendo este un país donde la introducción y la evaluación de este tipo de programas son incipientes.
Positive parenting is defined as ‘parental behaviour based on the best interest of the child that is nurturing, empowering, non-violent and provides recognition and guidance which involves setting of boundaries to enable the full development of the child’.1 There is evidence of a relationship between positive parenting and children's development in different socioeconomic contexts.2 Coercive parental behaviours have been related to children experiencing difficulties in self-regulation and aggressiveness, while warmth and effective parental communication have been associated with positive child development.3 Moreover, parenting effects go beyond childhood, having consequences in adolescence and adulthood. Insecure emotional attachment, lack of stimulation and failure to regulate problem behaviours during childhood are associated with children's negative development leading to mental problems in teenagers,4 as well as academic underachievement, engagement in risky, aggressive or criminal conduct during adolescence (violence, drug use, unsafe sexual relations).5
Parent-training programs aim to improve children and adolescents positive development by giving parents or primary caregivers knowledge about child development, and teaching them skills and self-efficacy for effective parenting (e.g., praise or appropriate discipline).6 They have shown positive effects on several health indicators such as reduction of risky health behaviours, reduction of unintended pregnancy, improvements on emotional child/adolescent regulation, stress and depression reductions or self-esteem increments.7,8
These interventions have been extensively used and evaluated primarily in Anglo-Saxon countries and in some Central European countries. However, parenting programs are an incipient issue in Southern European countries9 where, although implementation of such programs has increased in recent years, in most cases they lack standard implementation and any evaluation of the intervention.10
In order to overcome these limitations Southern European countries, and specifically in Spain, a group-based parent-training intervention [Parenting Skills Program for families (PSP)] was developed, implemented and preliminary evaluated in Barcelona.11,12 The objectives of this study were: 1) to compare parenting skills, social support, children's behaviours and parental stress before the parent-training intervention, immediately after it, and again after six-months, and 2) to identify the mechanisms by which the intervention is related to changes in the four outcomes examined.
MethodsDescription of the interventionIn the context of the community health strategy “Health in the Neighbourhoods”13 in Barcelona (Spain), parenting problems were identified as a community problem. After confirming that no parent-training interventions based on a theoretical framework had been previously used in the city, the Parenting Skills Program for families (PSP) was designed and implemented. PSP is based on the “Program Guide to Development of Emotional, Educational, and Parental Competencies”,14 which includes components associated with more effective parent training programs and, in addition, incorporates scientific recommendations.15 The program consists of 11 weekly sessions of 90minutes in which, following written guidelines, 10-14 parents with children 2-17 years old participate. Children only participate in two sessions. The program suggests some different strategies depending on the children's age, but the core components are the same. Parents are grouped according to their children age. The main contents of the program are development stages understanding; attention, respect, recognition and warmth needs; self-esteem and assertiveness; active listening and empathy; effective communication; problem-solving; negotiation and agreements; everyday family organization and boundaries and norms for children's behaviour regulation. The PSP was piloted between 2011 and 2013.11
Research designThis is a quasi-experimental study with measures before, immediately after the-intervention and after a follow-up of six months (T0, T1 and T2, respectively), with no control group. It combines quantitative and qualitative methods. The quantitative study aimed to identify the magnitude of changes from the baseline situation, immediately and six months later in the four outcomes examined. The objectives of the qualitative study were descriptive and explanatory. Specifically, the aim was to identify mechanisms related to changes in the four outcomes examined, increasing breadth of understanding of quantitative outcomes.
Sample and data collectionProfessionals involved in the intervention: 1) worked in social, health or educational services or in socio-educational associations related to family's issues; 2) received training on PSP; and 3) implemented the interventions in Catalonia, primarily in Barcelona. Parents selected to participate: 1) had children 2 to 12 years old; 2) spoke Catalan or Spanish; 3) had not participated in other parent-training program; and 4) were recruited by education, health or social services or socio-educational associations. Professionals used different types of recruitment strategies (poster, personal interviews, phone calls…).
Quantitative sub-studyA questionnaire with five sections was used in order to collect data from parents about: 1) parental stress, 2) social support, 3) parenting skills, 4) children's negative behaviours, and 5) sociodemographic profile. The four initial sections were based on previously validated scales in similar populations. The first section included the Spanish version of the Parental Stress Scale16 consisting of 12 items distributed in two subscales (baby's rewards [α=0.77] and stressors [α=0.76]) scored on a five point Likert scale (degrees of agreement/disagreement) (points scored between 1-5). Section two included the Duke-UNC Functional Social Support Questionnaire17 consisting of eight items grouped into two subscales (confident [α=0,92] and emotional [α=0,81] social support) scored with a five point Likert temporal scale (points scored between 1-5). Section three used a scale that included 19 items distributed into six dimensions of parental skills, scored using a four point Likert temporal scale (points scored between 0-3), which has previously been translated into Spanish and validated.18 Its subscales were: 1) children's understanding, 2) emotional self-regulation, 3) parenting self-esteem, 4) empathetic and assertive communication, 5) agreements, and 6) behavioural regulation (Cronbach alpha ranged between 0,69 for subscale 6 and 0,89 for subscale 4). The fourth section used the five-item problems behaviours subscale of the Strength and Difficulties Questionnaire (α=0,83)19 where items are scored on a three point Likert scale (points scored between 0-2). The fifth section collected sociodemographic data about sex, age, country of birth, marital status, educational level and employment status.
Twenty-two groups were carried out between 2013 and 2015, 257 parents started the intervention and 216 completed the questionnaire both at baseline and immediately after the intervention (84% retention rate), and 130 of these completed it six months after the intervention (51% retention rate).
Qualitative sub-studyThe qualitative study included 39 professionals and 34 parents, who participated in seventeen semi-structured interviews and five discussion groups. These instruments were used to collect information to describe the main effects of the PSP and the processes explaining these effects. They were conducted immediately after finishing the PSP sessions by an external researcher in an isolated, comfortable setting. Depending on the number of people, we used focus group scripts (for parents) and group or individual interview scripts (for professionals). Sessions duration were variable, depending on the number of participants (0.5-1.5hours). Scripts were prepared based on a literature review of the subject in which key elements to be examined were identified and were related to quantitative instruments. The questions sought to provide opportunities for participants to present their own experiences (parents) or parents’ experiences (professionals) in processes of participation in PSP. Scripts had seven questions piloted before starting the evaluation study. They were similar for professionals and parents, but worded differently. They focus on: a) the main effects of PSP; b) the mechanisms of changes associated to the four outcomes analysed; and c) the individual or social variables related to those effects.
We analysed information from 12 secondary documents with facilitators notes about the program effects. The parents who participate in the qualitative study were a subsample of those included in the quantitative sub-study. Some of them deny their participation in the qualitative sub-study because they did not have time to attend the focus groups or interviews or because they did not want to share their experiences verbally with an external researcher. Data collection ended when data saturation was reached.
Variables and data analysisQuantitative and qualitative data were collected and analysed separately and they were triangulated at the discussion phase.
Quantitative sub-studySociodemographic variables were sex (woman vs. man), age (<30 years old, 30-35 years old, 36-40 years old or>40 years old), origin (born in Spain vs born in other country), marital status (married or cohabiting vs non-cohabiting), educational level (no studies or primary studies, secondary studies or university studies finished) and employment status (unemployed, homemakers, employed or others). Four outcomes were examined: parenting skills, parental stress, social support and children's negative behaviours. For parenting skill variables, results were examined for each dimension separately. Regarding the scales, pre-, immediate-post and 6-month post-intervention item scores for each variable were summed and medians calculated. The bivariate association between sociodemographic and outcome variables were tested with the chi square test. Differences between T0, T1 and T2 were analysed. The percentage of parents that showed any improvement between baseline and immediately after the intervention, and between baseline and six months after the intervention were calculated for the four outcomes. Since the Kolgomorov-Smirnov test confirmed a non-normal distribution of data, medians were compared through the non-parametric Friedman test, carried out with SPSS.20.
Qualitative sub-studyThe qualitative information was audio recorded and then transcribed. After that, a content analysis performed by an external researcher using a system of categories previously created by one researcher and checked by the other two, based on the quantitative sub-study and on theoretical considerations. The categories were: 1) general effects, 2) positive factors, 3) barriers, 4) parenting skills effects, 5) children's behaviour effects, 6) parental stress effects, 7) social support effects, 8) outcome variables relationships, 9) personal determinants of change, and 10) contextual determinants of change. These categories were the same for each of the informants’ transcriptions. The first step of the analysis was textual, selecting quotes from transcripts of the interviews and discussion groups. The second step was conceptual in order to identify emergent subcategories and the interrelations between them. These were defined when the data had reached saturation. For the qualitative analysis, the Atlas.ti 6.2 program was used. Some quotes were selected and organized according to the emergent subcategories in order to show the main effects of the PSP as well as the processes that could explain them.
Ethical considerationsEthical considerations were taken into account in the study. Participants received a document where the research process was explained and granted their authorization by signing an informed consent. Two datasets were created, one with personal information and a code assigned to each participant, and another without personal information and with the code and the different variables. Participants were informed about the study during the implementation of the qualitative study. The research procedure adhered to the Barcelona Public Health Agency and University of Barcelona protocols of ethical considerations for good research practices of the ethical committee of each institution. It followed all legal requirements.
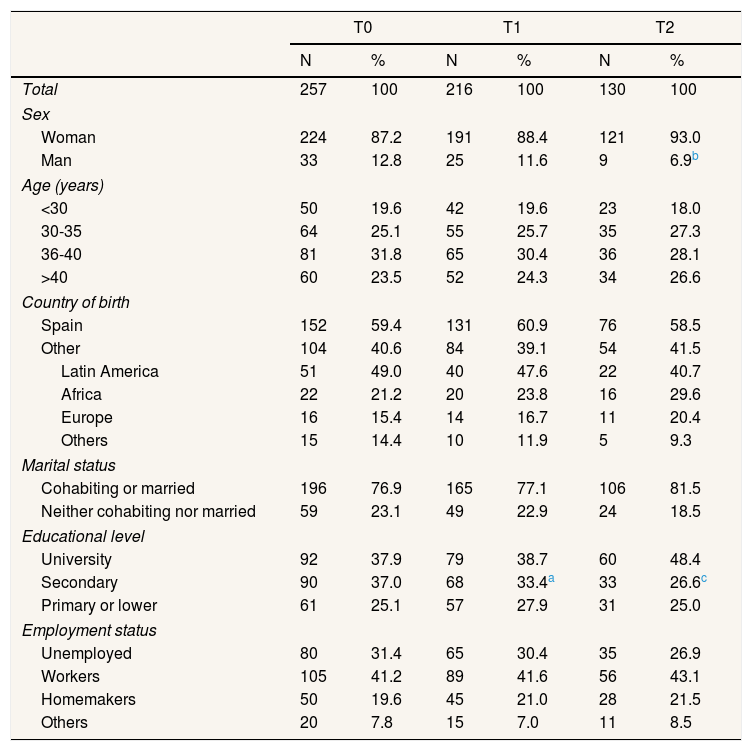
ResultsDescription of the sampleData came from 22 groups of 10-14 parents with a child 2-12 years old. Most parents were married or cohabiting, almost one third were 36-40 years old; 40% were immigrants, mostly from Latin-American countries; one quarter had primary studies or less and 31% were unemployed. The main reasons for not finalizing the intervention were work-related factors (e.g. change in work schedule or finding a job), family reasons (having a new child or caring for a dependant relative) and change of house. Difficulties to contact participants after six months (because they changed mobile phone number, they didn’t answer to phone call or they move to another city) were the main reason for losses to follow-up and most of them where men and people with secondary educational level. Statistically significant differences between participants in the pre-intervention and in the immediate post-intervention were observed for educational level with people with secondary studies being more likely to drop out. When participants who started the intervention were compared with those followed up at six months, the same pattern for educational level was found and additionally the proportion of men at the follow-up significantly decreased (Table 1). Most participants had one child (between 34%) or two children (between 43%), most of whom were aged between 3 and 5 years; 50% were girls. Professionals (n=39) were 95% women and 51% were community nurses. All of them implemented PSP and had previous experience as facilitators of family groups.
General description of the parents participating in the different phases of the intervention.
| T0 | T1 | T2 | ||||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Total | 257 | 100 | 216 | 100 | 130 | 100 |
| Sex | ||||||
| Woman | 224 | 87.2 | 191 | 88.4 | 121 | 93.0 |
| Man | 33 | 12.8 | 25 | 11.6 | 9 | 6.9b |
| Age (years) | ||||||
| <30 | 50 | 19.6 | 42 | 19.6 | 23 | 18.0 |
| 30-35 | 64 | 25.1 | 55 | 25.7 | 35 | 27.3 |
| 36-40 | 81 | 31.8 | 65 | 30.4 | 36 | 28.1 |
| >40 | 60 | 23.5 | 52 | 24.3 | 34 | 26.6 |
| Country of birth | ||||||
| Spain | 152 | 59.4 | 131 | 60.9 | 76 | 58.5 |
| Other | 104 | 40.6 | 84 | 39.1 | 54 | 41.5 |
| Latin America | 51 | 49.0 | 40 | 47.6 | 22 | 40.7 |
| Africa | 22 | 21.2 | 20 | 23.8 | 16 | 29.6 |
| Europe | 16 | 15.4 | 14 | 16.7 | 11 | 20.4 |
| Others | 15 | 14.4 | 10 | 11.9 | 5 | 9.3 |
| Marital status | ||||||
| Cohabiting or married | 196 | 76.9 | 165 | 77.1 | 106 | 81.5 |
| Neither cohabiting nor married | 59 | 23.1 | 49 | 22.9 | 24 | 18.5 |
| Educational level | ||||||
| University | 92 | 37.9 | 79 | 38.7 | 60 | 48.4 |
| Secondary | 90 | 37.0 | 68 | 33.4a | 33 | 26.6c |
| Primary or lower | 61 | 25.1 | 57 | 27.9 | 31 | 25.0 |
| Employment status | ||||||
| Unemployed | 80 | 31.4 | 65 | 30.4 | 35 | 26.9 |
| Workers | 105 | 41.2 | 89 | 41.6 | 56 | 43.1 |
| Homemakers | 50 | 19.6 | 45 | 21.0 | 28 | 21.5 |
| Others | 20 | 7.8 | 15 | 7.0 | 11 | 8.5 |
T0: baseline; T1: immediately after the intervention; T2: 6 months after the intervention.
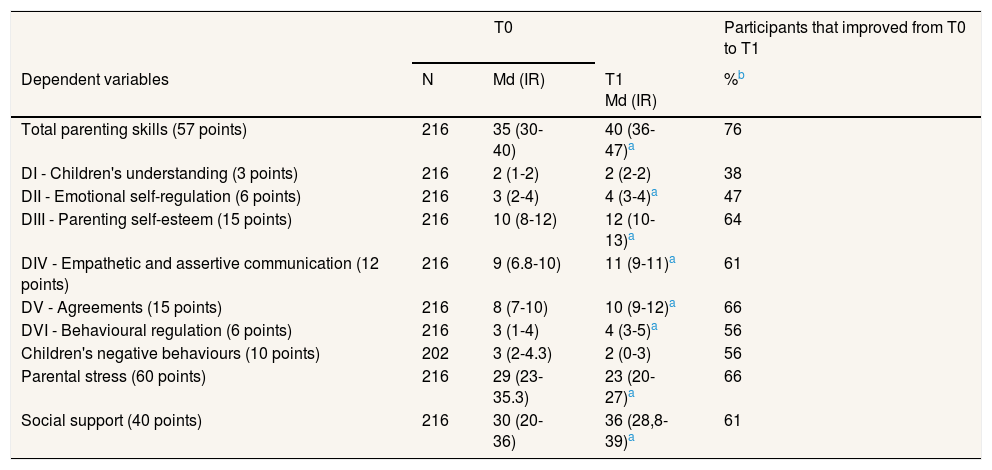
Table 2 presents medians of the evolution of the 216 participants who completed the intervention. Compared with T0, all outcomes significantly improved at T1. Specifically, 76% of the participants improved their parenting skills, 56% reduced children's negative behaviours, 66% decreased parental stress and 61% reported increased social support.
Comparison of scores before and immediately after the intervention.
| T0 | Participants that improved from T0 to T1 | |||
|---|---|---|---|---|
| Dependent variables | N | Md (IR) | T1 Md (IR) | %b |
| Total parenting skills (57 points) | 216 | 35 (30-40) | 40 (36-47)a | 76 |
| DI - Children's understanding (3 points) | 216 | 2 (1-2) | 2 (2-2) | 38 |
| DII - Emotional self-regulation (6 points) | 216 | 3 (2-4) | 4 (3-4)a | 47 |
| DIII - Parenting self-esteem (15 points) | 216 | 10 (8-12) | 12 (10-13)a | 64 |
| DIV - Empathetic and assertive communication (12 points) | 216 | 9 (6.8-10) | 11 (9-11)a | 61 |
| DV - Agreements (15 points) | 216 | 8 (7-10) | 10 (9-12)a | 66 |
| DVI - Behavioural regulation (6 points) | 216 | 3 (1-4) | 4 (3-5)a | 56 |
| Children's negative behaviours (10 points) | 202 | 3 (2-4.3) | 2 (0-3) | 56 |
| Parental stress (60 points) | 216 | 29 (23-35.3) | 23 (20-27)a | 66 |
| Social support (40 points) | 216 | 30 (20-36) | 36 (28,8-39)a | 61 |
IR: interquartile range; Md: median; N: participants.
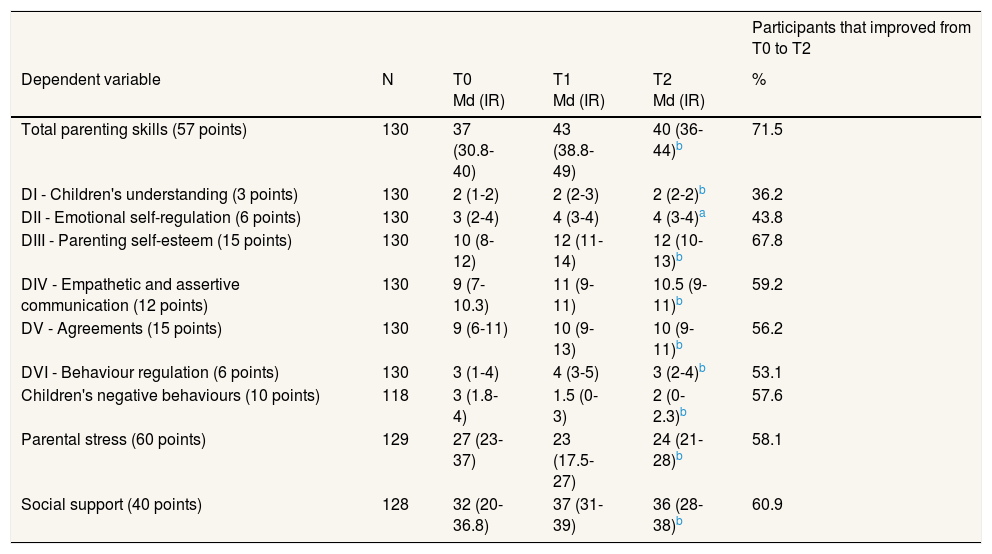
Table 3 presents the results of the follow-up six months after the intervention. All the outcomes significantly improved and the magnitude of the percentages of improvement was similar to that seen at T1 for most outcomes.
Comparison of scores before, immediately after the intervention and six months later.
| Participants that improved from T0 to T2 | |||||
|---|---|---|---|---|---|
| Dependent variable | N | T0 Md (IR) | T1 Md (IR) | T2 Md (IR) | % |
| Total parenting skills (57 points) | 130 | 37 (30.8-40) | 43 (38.8-49) | 40 (36-44)b | 71.5 |
| DI - Children's understanding (3 points) | 130 | 2 (1-2) | 2 (2-3) | 2 (2-2)b | 36.2 |
| DII - Emotional self-regulation (6 points) | 130 | 3 (2-4) | 4 (3-4) | 4 (3-4)a | 43.8 |
| DIII - Parenting self-esteem (15 points) | 130 | 10 (8-12) | 12 (11-14) | 12 (10-13)b | 67.8 |
| DIV - Empathetic and assertive communication (12 points) | 130 | 9 (7-10.3) | 11 (9-11) | 10.5 (9-11)b | 59.2 |
| DV - Agreements (15 points) | 130 | 9 (6-11) | 10 (9-13) | 10 (9-11)b | 56.2 |
| DVI - Behaviour regulation (6 points) | 130 | 3 (1-4) | 4 (3-5) | 3 (2-4)b | 53.1 |
| Children's negative behaviours (10 points) | 118 | 3 (1.8-4) | 1.5 (0-3) | 2 (0-2.3)b | 57.6 |
| Parental stress (60 points) | 129 | 27 (23-37) | 23 (17.5-27) | 24 (21-28)b | 58.1 |
| Social support (40 points) | 128 | 32 (20-36.8) | 37 (31-39) | 36 (28-38)b | 60.9 |
IR: interquartile range; Md: median; N: participants.
Friedman test:.
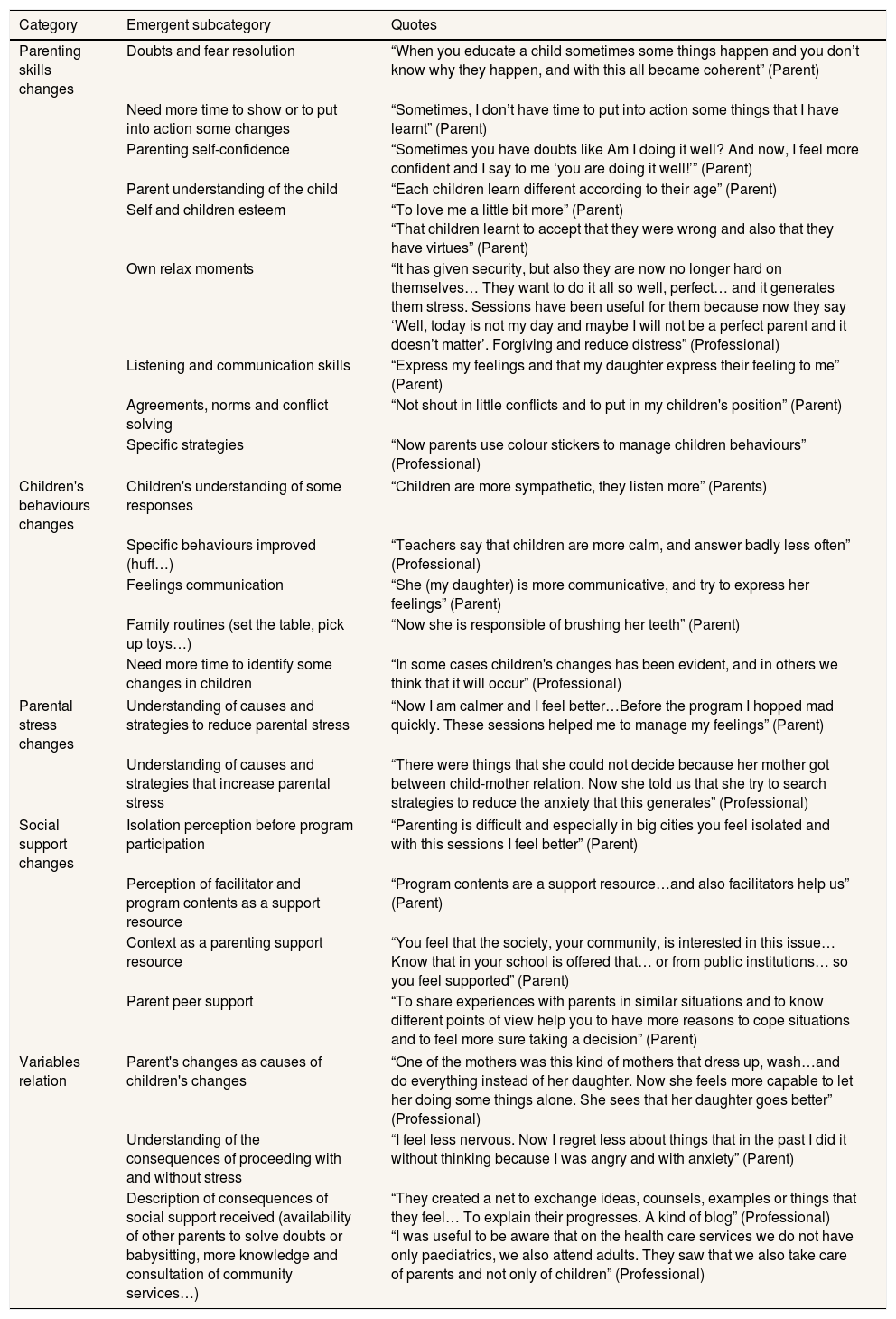
Parents and professionals described different types of changes in parents’ parenting skills, stress and social support and in the children's behaviours after the participation in the PSP. Table 4 shows emergent subcategories resulting from parents and professionals’ discourses. These allow us to identify the main changes for each outcome. Different quotes are included to illustrate each main effect of participation in the PSP.
Qualitative findings summary.
| Category | Emergent subcategory | Quotes |
|---|---|---|
| Parenting skills changes | Doubts and fear resolution | “When you educate a child sometimes some things happen and you don’t know why they happen, and with this all became coherent” (Parent) |
| Need more time to show or to put into action some changes | “Sometimes, I don’t have time to put into action some things that I have learnt” (Parent) | |
| Parenting self-confidence | “Sometimes you have doubts like Am I doing it well? And now, I feel more confident and I say to me ‘you are doing it well!’” (Parent) | |
| Parent understanding of the child | “Each children learn different according to their age” (Parent) | |
| Self and children esteem | “To love me a little bit more” (Parent) “That children learnt to accept that they were wrong and also that they have virtues” (Parent) | |
| Own relax moments | “It has given security, but also they are now no longer hard on themselves… They want to do it all so well, perfect… and it generates them stress. Sessions have been useful for them because now they say ‘Well, today is not my day and maybe I will not be a perfect parent and it doesn’t matter’. Forgiving and reduce distress” (Professional) | |
| Listening and communication skills | “Express my feelings and that my daughter express their feeling to me” (Parent) | |
| Agreements, norms and conflict solving | “Not shout in little conflicts and to put in my children's position” (Parent) | |
| Specific strategies | “Now parents use colour stickers to manage children behaviours” (Professional) | |
| Children's behaviours changes | Children's understanding of some responses | “Children are more sympathetic, they listen more” (Parents) |
| Specific behaviours improved (huff…) | “Teachers say that children are more calm, and answer badly less often” (Professional) | |
| Feelings communication | “She (my daughter) is more communicative, and try to express her feelings” (Parent) | |
| Family routines (set the table, pick up toys…) | “Now she is responsible of brushing her teeth” (Parent) | |
| Need more time to identify some changes in children | “In some cases children's changes has been evident, and in others we think that it will occur” (Professional) | |
| Parental stress changes | Understanding of causes and strategies to reduce parental stress | “Now I am calmer and I feel better…Before the program I hopped mad quickly. These sessions helped me to manage my feelings” (Parent) |
| Understanding of causes and strategies that increase parental stress | “There were things that she could not decide because her mother got between child-mother relation. Now she told us that she try to search strategies to reduce the anxiety that this generates” (Professional) | |
| Social support changes | Isolation perception before program participation | “Parenting is difficult and especially in big cities you feel isolated and with this sessions I feel better” (Parent) |
| Perception of facilitator and program contents as a support resource | “Program contents are a support resource…and also facilitators help us” (Parent) | |
| Context as a parenting support resource | “You feel that the society, your community, is interested in this issue… Know that in your school is offered that… or from public institutions… so you feel supported” (Parent) | |
| Parent peer support | “To share experiences with parents in similar situations and to know different points of view help you to have more reasons to cope situations and to feel more sure taking a decision” (Parent) | |
| Variables relation | Parent's changes as causes of children's changes | “One of the mothers was this kind of mothers that dress up, wash…and do everything instead of her daughter. Now she feels more capable to let her doing some things alone. She sees that her daughter goes better” (Professional) |
| Understanding of the consequences of proceeding with and without stress | “I feel less nervous. Now I regret less about things that in the past I did it without thinking because I was angry and with anxiety” (Parent) | |
| Description of consequences of social support received (availability of other parents to solve doubts or babysitting, more knowledge and consultation of community services…) | “They created a net to exchange ideas, counsels, examples or things that they feel… To explain their progresses. A kind of blog” (Professional) “I was useful to be aware that on the health care services we do not have only paediatrics, we also attend adults. They saw that we also take care of parents and not only of children” (Professional) | |
As far as we know, this is the first study in Spain where a parent-training program shows a positive impact in four outcomes both immediately after the intervention and six months later, and the qualitative mechanisms that specified that changes. The challenge in these situations should be to avoid returning to prior patterns of behaviour.20 This study is considered a success in this respect because improvements remained significant at the follow-up six months later.
Our study is consistent with others reporting that parent-training programs have positive short-term quantitative effects,21 however there are fewer mixed and follow-up studies evaluating effects in parental psychosocial health22 or on children's behaviours.7 In addition, many of these evaluation studies only explore one outcome, but few simultaneously explore more than one.8 In Spain this gap is more evident because the vast majority focus only on parenting skills23 and there is a lack of programs showing effects on children and on parental stress. This study contributes to fill this gap with similar evidence as that reported by studies in other countries.
The reduction observed in children's negative behaviours, such as aggressiveness or defiance, but also the increase in children's positive behaviours, was consistent with studies from other countries (immediately and six months after the intervention).24 Children's improvement in their ability to express feelings and communicate with their environment, understand parents demands or improve some habits (sleeping, hygiene or others)25 have been previously reported. Previous studies also show that changes in children should be understood as a consequence of changes in parenting.26
Studies carried out in other countries have reported stress reduction immediately after intervention22 and six months later.24 Some of the mechanisms consistent with our study were that parents learned to understand children's behaviours and what is expected of them according to their needs.27 In addition, they incorporated strategies to manage their anxiety and learned how to keep calm.28 Furthermore, they perceived that other parents felt similar concerns of self-demand,29 and that also helped them to reduce stress.
Finally, findings about the effects of parent-training programs in social support are contradictory. Although some metanalyses30 concluded that social support effects were not significant, they also suggested that quantitative instruments were not designed to collect data about specific social support associated via qualitative studies with effects of parent-training programs (for example, peer support). However, other studies are consistent with our findings.31 Qualitative findings provided answers to these divergences and shown that parents felt isolated in parenting.28 Yet, after participating in a parent-training program this situation changed and parents identified the program content and the facilitator strategies as a source of social support for improving their parenting skills.32 In other studies parent peer support was identified as a main social support, not only during program implementation, but also afterwards.31
LimitationsThis study has several limitations. The response rate immediately after the intervention (84%) was higher than in some previous studies7 and similar to other studies that have been highlighted as successful because of their high participation.33 However, the higher dropout rate at the six-month follow-up was a limitation. Almost half of the sample was lost to follow-up after six months, again similar to other studies.34 The causes of this dropout were the difficulties to contact or meet with families 6 months later of the intervention (telephone number or living place changes, or they did not answer phone calls). In the future, specific recruitment strategies should be implemented in order to reduce the dropout in this phase of data collection (i.e. incentives or reminder content session). This was an important limitation and the follow-up results should be viewed with caution, because the trend observed in post-intervention results is less robust because of the sample reduction.
Another limitation was that a randomized control trial design with a control group was not used. Therefore, the quantitative outcomes identified should be viewed with caution and considered as an association and not a direct effect caused by the intervention. Although randomized control trial is the most recommended design for effectiveness evaluation, some authors35 consider that the evaluations with no control group should be accepted when an intervention is well developed, meets generally accepted standards, and qualitative methods show the involved mechanisms. Therefore, our qualitative findings helped to reduce this limitation, and contributed to confirm effects caused by PSP.
ConclusionsThe quantitative and qualitative findings show that parents PSP participants not only improved in aspects directly related to the intervention (parenting skills) but also in others related to the formation of positive parenting and family wellbeing (social support, parental stress, and children's behaviour). In addition, these positive effects with respect to the four indicators were maintained after six months without returning to pre-intervention values. Therefore, PSP seems to be an effective intervention to promote positive parenting and family wellbeing.
Editor in chargeCarlos Álvarez-Dardet.
The evaluation of parent-training programs is an incipient issue in Southern European countries. Moreover, most previous studies have only assessed results immediately after the end of the intervention, whereas this study also includes the results after six months of follow-up.
What does this study add to the literature?This parent-training program is effective for improving parenting skills, children behaviours, parental stress and social support immediately and six-months after participation. Quantitative and qualitative findings are described.
The corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsAll authors designed the study. N. Vázquez and L. Artazcoz analyzed data quantitative data and N. Vázquez, analyzed qualitative data and M.C. Molina and P. Ramos supported her. All authors contributed reviewing the literature, editing all versions of the paper and providing relevant contributions. All authors approved the final version.
FundingThis study has been developed as part of a PhD project financed and the PhD student was contract with a grant from the Government of Catalonia (FI_DGR_2013). None of the authors of this paper has a competing interest, financial or otherwise, in any of the programs or interventions included in this review.
Conflicts of interestsNone.











