







Health reforms in Latin America and the Caribbean
More infoTo assess the level of development of palliative care in 13 countries participating in the iLIVE project, based on the World Health Organization's Conceptual Framework. The study includes an in-depth analysis of two comparative case studies: Spain and Argentina.
MethodA descriptive, cross-sectional, mixed-methods study was conducted using six dimensions and 14 macro-indicators. Key informants in each country provided data from official sources or expert knowledge. A comparative analysis was performed across countries, and a comparative case study approach was applied to Spain and Argentina, including health system profiles and indicator classification. Consensus on final data was reached through discussion groups.
ResultsEleven of thirteen countries provided complete or partial data. Most countries reached an advanced level of development, especially regarding the availability of essential medicines. Spain demonstrated higher integration and national policy development, while Argentina showed progress despite structural challenges. Twelve indicators lacked sufficient official data.
ConclusionsAlthough considerable progress has been made, disparities persist in key areas such as education, coordination, and equitable access. The World Health Organization framework proved useful for identifying development gaps and supporting evidence-based policymaking. Regular assessments are necessary to adapt strategies and ensure sustainable palliative care integration.
Evaluar el nivel de desarrollo de los cuidados paliativos en 13 países participantes en el proyecto iLIVE, basándose en el Marco Conceptual de la Organización Mundial de la Salud. El estudio incluye un análisis en profundidad de dos estudios comparativos de caso: España y Argentina.
MétodoSe realizó un estudio descriptivo, transversal y de métodos mixtos utilizando seis dimensiones y 14 macroindicadores. Informantes clave de cada país proporcionaron datos de fuentes oficiales o expertos. Se realizó un análisis comparativo entre países y se aplicó un enfoque de estudio de caso comparativo múltiple, incluyendo perfiles de sistemas sanitarios y clasificación de indicadores. El consenso sobre los datos finales se alcanzó mediante grupos de discusión.
ResultadosOnce de 13 países proporcionaron datos completos o parciales. La mayoría de los países alcanzaron un nivel avanzado de desarrollo, especialmente en la disponibilidad de medicamentos esenciales. España demostró una mayor integración y desarrollo de políticas nacionales, mientras que Argentina mostró avances a pesar de los retos estructurales. Doce indicadores carecían de datos oficiales suficientes.
ConclusionesAunque se han logrado avances considerables, persisten las disparidades en áreas como educación, coordinación y acceso equitativo. Es necesario realizar evaluaciones periódicas para adaptar las estrategias y garantizar una integración sostenible de los cuidados paliativos.
About 61 million people in the world need palliative care (PC).1 PC aims to improve quality of life of patients/families facing life-threatening illnesses. This care prevents and alleviates suffering by means of the early identification, evaluation and treatment of physical, psycho-social and spiritual problems.2 The development of PC must be recognized as a public health priority by governments.1,3 It is projected by 2060, due to an aging population and the increase in chronic illness 47% of global deaths will require PC.1
To assess PC services development,4 the World Health Organization (WHO) recently published a conceptual model with 14 indicators,4 covering six aspects: PC services, health policies, use of essential medications, training and enablement, empowerment of people and communities and research. Indicators are categorized as basic (evaluate development in any country) and strategic (for countries with early-stage PC development). The goal is to enable comprehensive evaluation, comparison and improvement of health systems. Next to measuring and evaluating, benchmarking is necessary. Benchmarking refers to comparing services with those of other more highly developed services or countries in order to carry out improvements in what is done and how it is done.5
In recent years, several documents have been published which analyse and compare the development of PC in different regions: Europe,6 Eastern Mediterranean,7 Latin American8 or Asia-Pacific region.9 World Atlas of Palliative Care was launched in 2020 at the international level.10
The present study is part of the iLive project, “Live well, die well”, which aimed at developing new evidence-based and sustainable interventions in order to alleviate symptoms and suffering which occur at the end of life of those patients in the advanced stages of illness and their families.11 This study aimed to describe development of PC in the participating countries. Analysis of development in these countries was based on the WHO framework.4 Furthermore, in-depth evaluation of the situation in Spain and Argentina was conducted to facilitate benchmarking and identify areas for improvement. The findings aim to guide public policy and support the work of policymakers.
MethodDesignThis study employed a descriptive, cross-sectional, mixed-methods design using a multiple case study approach.4 It was structured in two phases: 1) a comparative evaluation of palliative care development across 13 countries using the WHO Conceptual Framework with 14 macro-indicators; and 2) an in-depth analysis of two selected countries (Spain and Argentina), treated as comparative case studies. Participation in the second phase was voluntary; only Spain and Argentina agreed to join this stage of the study, which determined their inclusion. The data collection combined documentary review, expert consultation, and consensus-based validation, allowing for both quantitative and qualitative interpretation of the results.12
Participant selectionA total of 40 participants took part in the study, including key informants (palliative care researchers and professionals) from the iLIVE project (Argentina, Austria, Germany, Iceland, Netherlands, New Zealand, Norway, Slovenia, Spain, Switzerland and United Kingdom),13 and national stakeholders (representatives from health authorities and civil society organizations). Each country contributed 2–5 participants, reflecting voluntary participation and the availability of experts and stakeholders.
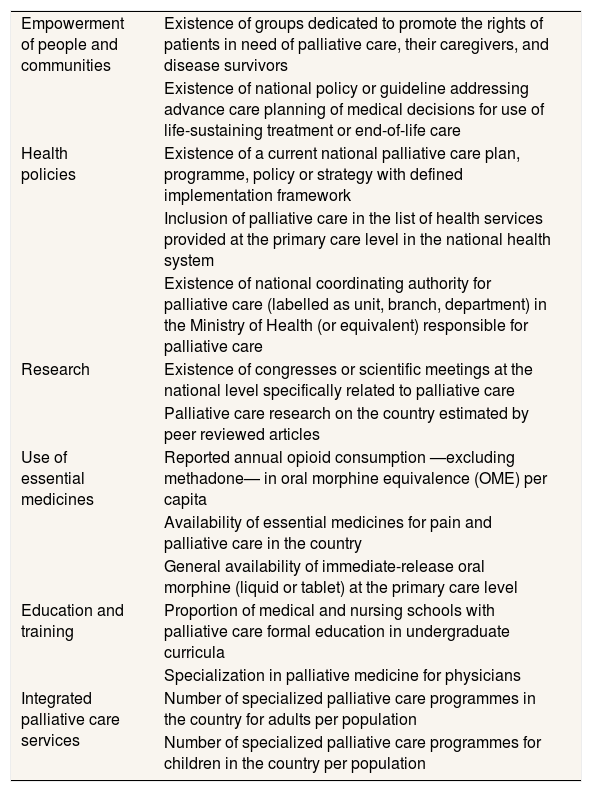
InstrumentsVariables which have been analysed correspond to the six aspects of development proposed by the WHO.4 These aspects contain the 14 macro-indicators described in Table 1.4
Conceptual framework of development in six aspects and 14 indicators of the World Health Organization.4
| Empowerment of people and communities | Existence of groups dedicated to promote the rights of patients in need of palliative care, their caregivers, and disease survivors |
| Existence of national policy or guideline addressing advance care planning of medical decisions for use of life-sustaining treatment or end-of-life care | |
| Health policies | Existence of a current national palliative care plan, programme, policy or strategy with defined implementation framework |
| Inclusion of palliative care in the list of health services provided at the primary care level in the national health system | |
| Existence of national coordinating authority for palliative care (labelled as unit, branch, department) in the Ministry of Health (or equivalent) responsible for palliative care | |
| Research | Existence of congresses or scientific meetings at the national level specifically related to palliative care |
| Palliative care research on the country estimated by peer reviewed articles | |
| Use of essential medicines | Reported annual opioid consumption —excluding methadone— in oral morphine equivalence (OME) per capita |
| Availability of essential medicines for pain and palliative care in the country | |
| General availability of immediate-release oral morphine (liquid or tablet) at the primary care level | |
| Education and training | Proportion of medical and nursing schools with palliative care formal education in undergraduate curricula |
| Specialization in palliative medicine for physicians | |
| Integrated palliative care services | Number of specialized palliative care programmes in the country for adults per population |
| Number of specialized palliative care programmes for children in the country per population |
The preparation of key informants and data collection were carried out in different stages:
Preliminary meeting: researchers (EV, PB, MM) formed a discussion group to present the method and theoretical framework to the key informants, and to reach an agreement on the data gathering process. Any questions that arose were also addressed during this session.
Data collection and analysis: data was collected using a template that included 14 WHO macro-indicators4 (Table 1). Official sources were consulted in each country (websites of ministries, legislation, PC guides, etc.) by key informants. In cases where the information came from unofficial sources or was based on the expert's own experience was considered present.
Consensus discussion group: Once all data was compiled, a structured discussion group was held with the key informants. Preliminary results were presented, and each indicator was reviewed in detail. Divergences were addressed through collaborative debate, and agreement was reached by majority consensus. This process validated the final classification of each indicator and ensured consistency, reliability, and contextual relevance of the information used in the final report.
Data analysisIndicators where no information was available after consulting key informants, the different Atlas of PC were consulted.
After compiling all the data, a discussion group involving key informants was convened to review the preliminary findings. During this session, each indicator was examined by country, and discrepancies or missing information were discussed. When divergent interpretations emerged, participants presented supporting evidence and reached agreement. It ensured the accuracy, consistency, and credibility of the data. Data collection and consensus-building took place between May 2023 and November 2024.
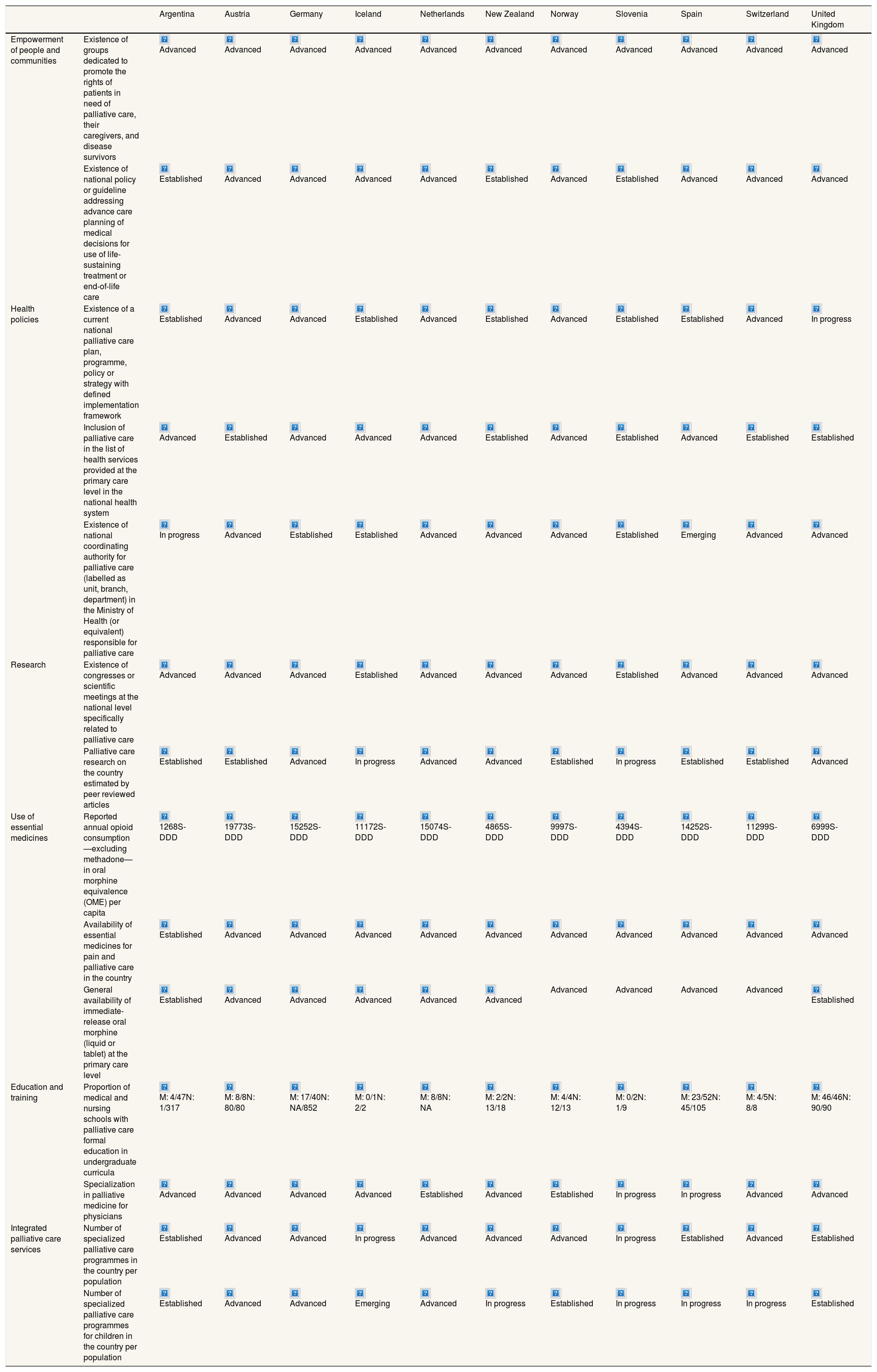
To classify countries a colour code was used: green (presence of evidence and availability of data), yellow (information, that is not supported by official sources) and red (absence of information) (Table 2).
Degree of official evidence of indicators by country.
| Argentina | Austria | Germany | Iceland | Netherlands | New Zealand | Norway | Slovenia | Spain | Switzerland | United Kingdom | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Empowerment of people and communities | Existence of groups dedicated to promote the rights of patients in need of palliative care, their caregivers, and disease survivors | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced |
| Existence of national policy or guideline addressing advance care planning of medical decisions for use of life-sustaining treatment or end-of-life care | Established | Advanced | Advanced | Advanced | Advanced | Established | Advanced | Established | Advanced | Advanced | Advanced | |
| Health policies | Existence of a current national palliative care plan, programme, policy or strategy with defined implementation framework | Established | Advanced | Advanced | Established | Advanced | Established | Advanced | Established | Established | Advanced | In progress |
| Inclusion of palliative care in the list of health services provided at the primary care level in the national health system | Advanced | Established | Advanced | Advanced | Advanced | Established | Advanced | Established | Advanced | Established | Established | |
| Existence of national coordinating authority for palliative care (labelled as unit, branch, department) in the Ministry of Health (or equivalent) responsible for palliative care | In progress | Advanced | Established | Established | Advanced | Advanced | Advanced | Established | Emerging | Advanced | Advanced | |
| Research | Existence of congresses or scientific meetings at the national level specifically related to palliative care | Advanced | Advanced | Advanced | Established | Advanced | Advanced | Advanced | Established | Advanced | Advanced | Advanced |
| Palliative care research on the country estimated by peer reviewed articles | Established | Established | Advanced | In progress | Advanced | Advanced | Established | In progress | Established | Established | Advanced | |
| Use of essential medicines | Reported annual opioid consumption —excluding methadone— in oral morphine equivalence (OME) per capita | 1268S-DDD | 19773S-DDD | 15252S-DDD | 11172S-DDD | 15074S-DDD | 4865S-DDD | 9997S-DDD | 4394S-DDD | 14252S-DDD | 11299S-DDD | 6999S-DDD |
| Availability of essential medicines for pain and palliative care in the country | Established | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | |
| General availability of immediate-release oral morphine (liquid or tablet) at the primary care level | Established | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Advanced | Established | |
| Education and training | Proportion of medical and nursing schools with palliative care formal education in undergraduate curricula | M: 4/47N: 1/317 | M: 8/8N: 80/80 | M: 17/40N: NA/852 | M: 0/1N: 2/2 | M: 8/8N: NA | M: 2/2N: 13/18 | M: 4/4N: 12/13 | M: 0/2N: 1/9 | M: 23/52N: 45/105 | M: 4/5N: 8/8 | M: 46/46N: 90/90 |
| Specialization in palliative medicine for physicians | Advanced | Advanced | Advanced | Advanced | Established | Advanced | Established | In progress | In progress | Advanced | Advanced | |
| Integrated palliative care services | Number of specialized palliative care programmes in the country per population | Established | Advanced | Advanced | In progress | Advanced | Advanced | Advanced | In progress | Established | Advanced | Established |
| Number of specialized palliative care programmes for children in the country per population | Established | Advanced | Advanced | Emerging | Advanced | In progress | Established | In progress | In progress | In progress | Established |






















































































































































M: medical school; N: nursing school (the number indicated in indicator 11 considers the proportion of compulsory palliative care studies among the total number of schools of each specialty); NA: no data available; S-DDD: defined daily doses for statistical purposes, per million inhabitants per day.
To classify countries according to the availability of information from official or expert sources, a colour scheme was used in which green stands for evidence and availability of these data, and yellow means information, but it is not backed up by official sources or experts opinions, and red where there is no information about the aspect to be evaluated, or this criterion is not complied with.
Source: own elaboration based on WHO.4
The level of development of palliative care is also taken into account in a simplified way and is noted in the results as follows. Levels are: 1) no known hospice-PC activity; 2) capacity-building activity; 3a) isolated PC provision; 3b) generalized PC provision; 4a) countries where hospice-PC services are at a stage of preliminary integration into mainstream service provision; and 4b) countries where hospice-PC services are at a stage of advanced integration into mainstream service provision.14
To facilitate comparison of certain variables in the case study of Spain and Argentina, we include a description of the country's population, surface area, population density and development index as well as an overview of their political and social care systems.
A detailed summary of the development of palliative care in Spain and Argentina, respectively, based on the six dimensions and 14 macro-indicators of the WHO Conceptual Framework4 is presented in Tables S1 and S2 in Supplementary data. For each indicator, the level of development was classified using a four-level scale (from emerging to advanced), accompanied by a justification based on available evidence. This structured approach allows for a comprehensive and comparable assessment of national progress in palliative care implementation, while also identifying specific areas for improvement in each country.
ResultsComparison of countries involved in the iLIVE ProjectOut of the 13 participating countries, 11 (84.6%) completed required information. Despite repeated contact, two participating countries were unable to complete the full set of indicators due to internal limitations in data availability or informant engagement. Level of development in nine countries corresponds to level 4b (countries where PC services and hospices are found to be at a stage of advanced integration within the provision of general services). Slovenia, it is classified as 3b (generalized provision of PC). Argentina, it is classified as 4a (countries in which PC services and hospices are at the stage of preliminary integration within the provision of general services).10,14
A color-based infographic has been made in Table 2 to indicate whether the information is available. Green boxes (134/154) mean that information has been provided by experts through their experience or official documents, yellow (8/154) is that information is not from an official source or from experts and red (12/154) is that information could not be collected because was not available.
Iceland, Switzerland and United Kingdom are the only countries where all the information could be collected, while Slovenia has the most indicators in red (four). On the other hand, New Zealand is the country with the most indicators in yellow (four).
Below each color infographic, the level of development of each of the indicators is shown according to the recently published European Atlas6 or, in the case of New Zealand, the information has been extracted from the Atlas of Palliative Care in the Asia Pacific Region.9 In the case of indicators 8 and 11, no gradient is shown, only quantitative data.
In some cases, the key informants could not find the indicator data requested or could not access any official document indicating it, since data collection ended in 2024 and these Atlases have been published in 2025.
Case studies: Spain and ArgentinaSubsequently, the 11 countries that participated in the first phase of the study were informed that a new phase would be undertaken to conduct a more in-depth analysis of the indicators within each country. Only Spain and Argentina (18.2% of the participants) agreed to take part in this phase.
- 1)
Spain: description of National Health System
Spain is a country divided into 17 autonomous communities and two autonomous cities. Due to the organisation of its territory in 1986, the National Health System was set up within the General Health Law in which the model of the health system is decentralised in response to the new territorial organisation of the State, under Article 8 of the Constitution. During 80s and 90s, a process of decentralisation of the health service took place with the transfer to the Autonomous Communities of competences referring to matters of health.15
Throughout these same decades, the introduction and development of PC began as the result of personal initiatives.16 On many occasions this was promoted by the support of the Asociación Española Contra el Cáncer or Orden Hospitalaria de San Juan de Dios.17 Towards the end of 90s, Ministry of Health and Consumption began to consider the possibility of offering PC within the Health Service and to this end, it was necessary to update both its structures and health planning. Finally, this took shape in December 2000 with the approval of a document in the plenary session of Interterritorial Congress of National Health Service where were included the guidelines for the Development of a National Plan for Palliative Care. Aim of this document was to plan a model of integrated and interdisciplinary attention which would respond to PC needs of the Spanish population.18
The decentralization process began in the 80s and 90s, with the transfer of health competencies to autonomous communities completed in 2002, except for Ceuta and Melilla, which remain under the National Institute of Health Administration (INGESA). Different communities developed their own PC plans and strategies, leading to uneven growth and a lack of a unified measurement or evaluation system. This hampers regional development analysis and the availability of official resources.
- 2)
Argentina: description of National Health System
Argentina's healthcare system is fragmented into public, private, and social insurance subsectors. The public sector offers free or affordable services, while social insurance is mandatory for workers, funded by employers and employees. Private insurance, or ‘prepay’, provides subscription-based services. Programs like “Programa Sumar” and “Incluir Salud” aim to improve access, but cultural and geographic differences hinder timely care, especially in poorer provinces. The variability in care quality across regions reflects the system's fragmentation.
Economic crisis has decreased government funding for healthcare, potentially reducing coverage and quality of health services. This could result in cuts in essential programs and investment in health infrastructure. Strategies and policies are needed to guarantee the stability and equity of the system during difficult times.19
Argentina has been recognized by the Pan American Health Organisation (PAHO)20 for its efforts to improve health system's quality through the’Quality Improvement Plan’. However, equity of access remains a problem, especially for rural or less developed populations and vulnerable minorities.
Key quality indicators in health system include population data, access and coverage resources, morbidity and mortality, maternal and child health, and quality of care. Other indicators used to monitor the Millennium Development Goals are also essential for evaluating and improving health system in Argentina.
PC has significantly developed over the past decades, starting with individual initiatives in the mid-1980s. By 2000, standards for PC organization and delivery were established through Resolution 934/2001 by the National Ministry of Health. These standards were incorporated into the National Quality Assurance Program, and the categorization of services began. In 2016, they were updated under new “Guidelines” with expert input. That same year, a National Palliative Care Program for cancer patients was launched. In 2022, the National Palliative Care Law (Ley 27.678) was enacted, with partial regulation still pending.
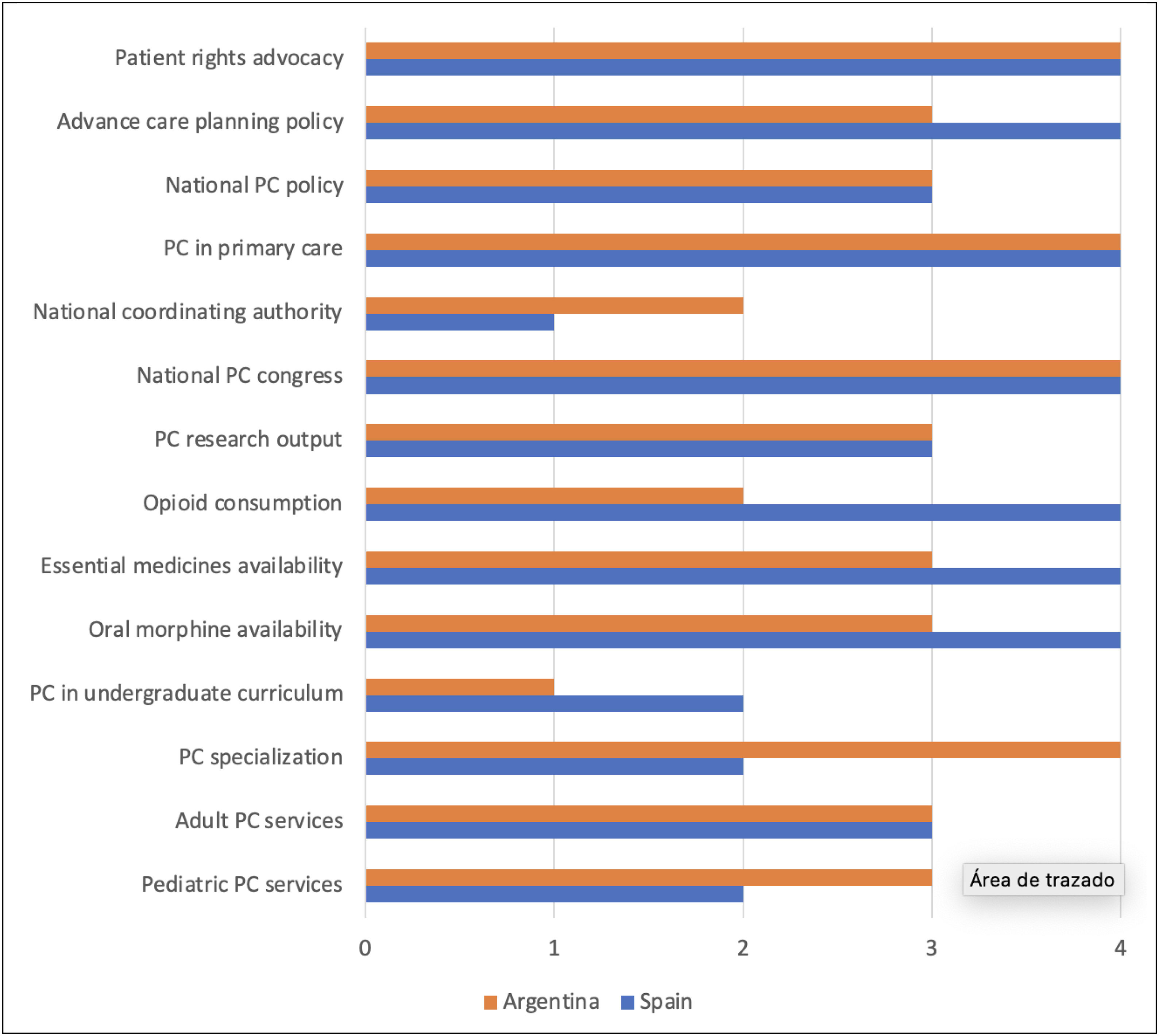
Comparative analysis of case studiesDevelopment of PC in Spain according to Baur et al.14 and Connor10 is level 4b (PC services and hospices are at a stage of advanced integration within the provision of general services).
Argentina ranks favorably in the Latin American region regarding quality and access to care, 21 but there is still room for improvement, particularly in equity of access and consistency in quality of care across the country. Currently development of PC in Argentina according to Baur et al.14 and Connor10 is level 4a (countries in which PC services and hospices are in a preliminary stage of integration within the provision of general service
Figure 1 presents a comparative visual summary of the level of palliative care development in Spain and Argentina across the 14 WHO macro-indicators. Each bar represents the degree of development attained by each country, ranging from level 1 (emerging) to level 4 (advanced). This “graph” highlights similarities and contrasts. This figure complements the narrative comparison and facilitates a clearer identification of strengths and gaps between both countries.
Discussion
This study evaluated the development of PC in 11 iLIVE countries using the WHO conceptual framework, with a focus on Spain and Argentina as contrasting case studies. The integration of quantitative indicators with contextual health system profiles allowed for an in-depth understanding of progress, persistent gaps, and structural determinants influencing PC integration. Building on these results, the discussion explores the implications of cross-country differences, the role of decentralization and governance, and the strategies needed to strengthen equitable and sustainable PC services.
Analysis of PC development in countries participating in study reveals that most of countries are at the highest level of PC development. In-depth evaluation of case studies in Spain and Argentina allowed for a comparison of two countries with cultural similarities but structural differences in health-care systems. International benchmarking provided a valuable opportunity for exploration and applied research.
Of the 14 indicators assessed, 12 presented at least some degree of data unavailability or unfulfilled criteria in one or more countries, highlighting that, despite significant progress, challenges remain in improving sources and quality of information. Access to essential medication, especially opioids, continues to be challenge in many countries.1 In Argentina, while the availability of opioids has improved in urban areas, significant difficulties persist in rural areas. This issue is a global challenge. Strategies such as strengthening the medication supply chain and providing appropriate training for health care professionals are crucial to improving access to medication.1 On the other hand, only two indicators —availability of national palliative care congresses and existence of patient advocacy groups— were reported consistently across all 11 countries. These were the only indicators with no missing or unconfirmed data in any country.
Slovenia was the only participant country in level 3,14 and maybe this explains why have less information available and should be studied in depth in future research. This could be due to the disparity in the development in PC services between Eastern and Western Europe.22 This imbalance underscores the need for region-specific strategies that address local challenges and promote equitable and sustainable development of PC services.23
In the case of decentralised countries, such as Germany or Spain, may be an impediment to the existence of a national authority to coordinate PC services. Decentralisation allows for greater adaptability to local needs, but may also lead to considerable variability in the quality and availability of services.24 As a result, national policies need to be implemented with effective coordination between regions in order to mitigate these limitations and ensure equitable access in all areas of the country. In federal countries like Argentina, inequities regarding differences in budget allocations are added to the bureaucratic barriers that exist in each province, for example concerning opioid prescription, amongst others.25
The way to measure development of PC services has been evolving. Before the only criterion to be considered was the consumption of morphine measured qualitatively by experts in each country.26,27
Later on, WHO used a public health model to devise a series of indicators in the dimensions of appropriate policies, use of medications, education, and the appropriate provision of services.28 However, in 2021 WHO4 published a conceptual model updating the one previously28 and widening the dimensions to six. An approach based on indicators helps to identify areas in need of improvement and facilitates decision making by those politicians who are responsible.29
Decision-makers can greatly benefit from PC development data derived from indicators, helping to set health priorities, identify policy gaps, allocate resources, and strengthen activities. Measurement supports service quality improvement, awareness, resource mobilization, transparency, and the promotion of universal health coverage. Further international comparisons should be made for benchmarking.30
It is essential that countries’ PC programmes and health policies are registered in order to enable a comparative evaluation of the productivity and impact of PC services so that they can be better appreciated, as is the case in United Kingdom31 or Sweden.32 In general, access to big data can provide information on the productivity and work of PC within health care services and on where efforts need to be focused in order to carry out changes that will improve the care of patients and their family.33
Indicators assess global development levels, but distinguishing between more developed countries is challenging. Therefore, considering other criteria, such as interdisciplinary team integration and training in fields like psychology and social work, would be beneficial. Additionally, community involvement and volunteers are crucial for achieving social change that leads to political decisions.
Political actors should be aware that it is more effective to follow a community-based approach within PC services, given that they improve the well-being and quality of life of both patients and relatives during their illness and in bereavement.34 The index of death literacy35 is an example of the importance of community participation, as this tool can provide the politicians responsible with strategies to improve end of life care through the efficient and efficacious use of resources.36
This study faces several limitations, including difficulty in finding official sources and the variable quality of data provided by clinics and researchers. Given that this is a new conceptual framework, the changes over time in methods of measuring have complicated historical comparisons, affecting the consistency and traceability of results.
ConclusionsThis study provides a comparative evaluation of PC services in 11 countries, focusing on Spain and Argentina. While most required information was obtained, some areas still need improvement, helping identify country-specific issues. These findings can guide future public policy and PC development strategies.
The study emphasizes the need for periodic evaluations using standardized frameworks, like the WHO's, to monitor progress and adapt strategies. It also highlights the importance of ongoing work to integrate PC into health systems, tailoring strategies to local contexts and learning from international experiences.
Availability of databases and material for replicationData made available upon request by contacting the corresponding author.
Palliative care is essential to improving the quality of life for patients with life-threatening illnesses, yet access remains uneven globally. The World Health Organization has developed a conceptual framework with 14 indicators to assess the development of palliative care across different countries.
What does this study add to the literature?This study evaluates palliative care development across 11 countries participating in the iLIVE project, with an in-depth focus on Spain and Argentina. Using World Health Organization indicators. Spain shows a higher level of integration (level 4b), whereas Argentina remains in a preliminary stage of integration (level 4a). The study highlights the impact of political decentralization on care coordination and the challenges of data availability for policy evaluation.
What are the implications of the results?Findings emphasize the need for continuous assessment and benchmarking of palliative care services to drive improvements. Governments should strengthen national coordination, ensure equitable access to essential medications, and integrate palliative care into primary healthcare. In decentralized systems, enhanced coordination between regional authorities is crucial. Expanding formal education and interdisciplinary training in palliative care can further improve service quality and accessibility.
Jorge Marcos Marcos.
Transparency declarationThe corresponding author, on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionE. Víbora-Martín and V.A. Tripodoro have gathered all the information needed for this article and have contacted all the countries involved in the project. E. Víbora-Martín, V.A. Tripodoro and P. Barnestein-Fonseca have been responsible for the writing of this article. All authors have contributed to the review of the drafts that were used to submit this project and secure the grant. All authors have read and approved the final version of the manuscript.
We would like to thank the key informants from each country for their time, commitment, and contributions, as well as the local teams from the iLIVE project for facilitating access to national data.
Simon Allan1, Pilar Barnestein-Fonseca2,3, Mark Boughey4, Andri Christen5, Nora Lüthi5, Martina Egloff5, Steffen Eychmüller5, Sofia C Zambrano5,6, Gustavo G De Simone7, Eline E C M Elsten8,9, Eric C T Geijteman8,9, Iris Pot9, Carin C D van der Rijt9, Carl Johan Fürst10,11, Birgit H Rasmussen10, Maria E C Schelin10,11, Christel Hedman10-12, Gabriel Goldraij13, Svandis Iris Halfdanardottir14, Valgerdur Sigurdardottir14, Tanja Hoppe15, Melanie Joshi15, Julia Strupp15, Raymond Voltz15-18, Maria Luisa Martín-Roselló2,19, Silvi Montilla20, Verónica I Veloso20, Vilma Tripodoro7,20, Katrin Ruth Sigurdardottir21,22, Hugo M van der Kuy23, Lia van Zuylen24, Berivan Yildiz8, Agnes van der Heide8, Misa Bakan25, Michael Berger26, John Ellershaw27, Claudia Fischer26, Anne Goossensen28, Dagny Faksvåg Haugen21,29, Rosemary Hughes27, Grethe Skorpen Iversen21, Hana Kodba-Ceh25, Ida J Korfage8, Urska Lunder25, Stephen Mason27, Tamsin McGlinchey27, Beth Morris27, Inmaculada Ruiz Torreras2, Judit Simon26, Ruthmarijke Smeding27, Kjersti Solvåg21, Eva Vibora Martin2.
1Arohanui Hospice, Palmerston North, New Zealand.
2CUDECA Institute for Training and Research in Palliative Care, CUDECA Hospice Foundation, Malaga, Spain.
3Group C08: Pharma Economy: Clinical and Economic Evaluation of Medication and Palliative Care, Ibima Institute, Malaga, Spain.
4Department of Palliative Care, St Vincent's Hospital Melbourne, Fitzroy, Victoria, Australia.
5University Center for Palliative Care, Inselspital University Hospital Bern, University of Bern, Bern, Switzerland.
6Institute for Social and Preventive Medicine (ISPM), University of Bern, Bern, Switzerland.
7Research Network RED-InPal, Institute Pallium Latinoamérica, Buenos Aires, Argentina.
8Department of Public Health, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands.
9Department of Medical Oncology, Erasmus MC Cancer Institute, Erasmus MC University Medical Center Rotterdam, Rotterdam, The Netherlands.
10Institute for Palliative Care at Lund University and Region Skåne, Lund University, Lund, Sweden.
11Division of Oncology and Pathology, Department of Clinical Sciences, Lund University, Lund, Sweden.
12Research Department, Stiftelsen Stockholms Sjukhem, Stockholm, Sweden.
13Internal Medicine/Palliative Care Program, Hospital Privado Universitario de Córdoba, Cordoba, Argentina.
14Palliative Care Unit, Landspitali—National University Hospital, Reykjavik, Iceland.
15Department of Palliative Medicine, Faculty of Medicine and University Hospital, University of Cologne, Cologne, Germany.
16Center for Integrated Oncology Aachen Bonn Cologne Dusseldorf (CIO ABCD), Faculty of Medicine and University Hospital, University of Cologne, Cologne, Germany.
17Clinical Trials Center (ZKS), Faculty of Medicine and University Hospital, University of Cologne, Cologne, Germany.
18Center for Health Services Research (ZVFK), Faculty of Medicine and University Hospital, Cologne, Germany.
19Group CA15: Palliative Care, IBIMA Institute, Malaga, Spain.
20Institute of Medical Research A. Lanari, University of Buenos Aires, Buenos Aires, Argentina.
21Regional Centre of Excellence for Palliative Care, Western Norway, Haukeland University Hospital, Bergen, Norway.
22Specialist Palliative Care Team, Department of Anaesthesia and Surgical Services, Haukeland University Hospital, Bergen, Norway.
23Department of Clinical Pharmacy, Erasmus MC, University Medical Center, Rotterdam, The Netherlands.
24Department of Medical Oncology, Amsterdam University Medical Center, Amsterdam, The Netherlands.
25Research Department, University Clinic of Respiratory and Allergic Diseases Golnik, Golnik, Slovenia.
26Department of Health Economics, Center for Public Health, Medical University of Vienna, Wien, Austria.
27Palliative Care Unit, Institute of Life Course and Medical Sciences, University of Liverpool, Liverpool, UK.
28Informal Care and Care Ethics, University of Humanistic Studies, Utrecht, The Netherlands.
29Department of Clinical Medicine K1, University of Bergen, Bergen, Norway.












