



To analyse the profile of the persons and associations that participated in the course, quantify peer education activities and analyse their evolution.
MethodA quantitative study using an analysis of the course records from 2009 to 2018 was designed for this purpose inside mihsalud program designed to promote health amongst persons in vulnerable situations in the city of Valencia (Spain). It offers a yearly training-action course of community health workers (CHW) that is attended by persons who have been proposed by associations. The associations were defined according to their population (immigrant, local or intercultural) and the CHWs according to gender, country of birth, year of course, association and continuity after training. Means and confidence intervals were calculated at 95% and a bivariate analysis was conducted in order to compare the activities that took place in 2009 to 2013 with those of 2014 to 2018. The time trends were analysed by applying linear regression models that included the different years studied as the dependent variable.
Results201 CHW of 31 nationalities were trained, 81.6% (95% confidence interval [95% CI]: 75.5-86.7] were women. Eighty-two associations participated, 51.2% (95% CI: 39.9-62.4] worked with culturally diverse populations. Participation by associations (p=.017) and CHWs (p=.377) increased in a statistically significant manner over the years. After the course, 35.3% (95% CI: 28.7-42.4] of the CHWs continued to collaborate voluntarily in the associations.
ConclusionsThe results of the CHW training-action course improve over time given that a significant increase in participation by associations and women can be seen, along with a greater number of activities completed during the training. One effect of this is that CHWs are contracted or carry out voluntary activities in the associations.
Analizar el perfil de las personas y asociaciones que participaron en los cursos, cuantificar las actividades de educación entre iguales y analizar su evolución.
MétodoSe diseñó un estudio cuantitativo utilizando un análisis de los registros del curso de 2009 a 2018, dentro del programa mihsalud diseñado para promover la salud entre las personas en situación de vulnerabilidad en la ciudad de Valencia (España). Anualmente se ofrece un curso de formación-acción para agentes de salud de base comunitaria (ASBC), al que asisten personas propuestas por asociaciones. Las asociaciones se definieron según su población (inmigrantes, locales o interculturales) y los ASBC según el género, el país de nacimiento, el año de curso, la asociación y la continuidad después de la capacitación. Las medias y los intervalos de confianza se calcularon al 95% y se realizó un análisis bivariado para comparar las actividades que tuvieron lugar en 2009 a 2013 con las de 2014 a 2018. Las tendencias temporales se analizaron aplicando modelos de regresión lineal que incluyeron el estudio de diferentes años como la variable dependiente.
Resultados201 ASBC de 31 nacionalidades fueron entrenados, 81.6% (intervalo de confianza del 95% [IC 95%]: 75,5 a 86,7) eran mujeres. Participaron 82 asociaciones, el 51,2% (IC 95%: 39,9 a 62,4) trabajaron con poblaciones culturalmente diversas. La participación de asociaciones (p = 0,017) y ASBC (p = 0,377) aumentó de manera estadísticamente significativa a lo largo de los años. Después del curso, el 35,3% (IC 95%: 28,7 a 42,4] de los ASBC continuaron colaborando voluntariamente en las asociaciones.
ConclusionesLos resultados del curso de formación-acción de ASBC mejoran con el tiempo dado que se puede observar un aumento significativo en la participación de asociaciones y mujeres, junto con un mayor número de actividades completadas durante la capacitación. Un efecto de esto es que los ASBC son contratados o realizan actividades voluntarias en las asociaciones y también están involucrados en proyectos de salud.
Mihsalud (Mujeres, Infancia y Hombres construyendo salud [Women, Children and Men Building Health])1 is a public participation program promoted by the Public Health Centre of Valencia since 2007 in coordination and collaboration with healthcare services and the primary healthcare network, the Association of Cooperation Between Communities (ACOEC), the Town Hall and third sector organizations of the city. The aim of the program is to promote health amongst people living in contexts of higher vulnerability by mobilising the city's associations and local organizations. The program was recognised as a model of best practices by the Ministry of Health, Social Services and Equality in 2016 and by the Council of Universal Healthcare and Public Health of the Regional Government of Valencia in 2018.
One of the lines of action of Mihsalud focuses on health literacy2 in the community, offering a yearly course of training-action of community health workers (CHW) to enable local leaders linked to associations to become involved in the program;3 nurses play a role as educators and coordinators to enable the program to extend to the community. The underlying rationale of the course is the potential for change brought about by peer to peer health education,4 based on the idea that if a person is concerned about his/her health, he/she will discuss this with peers, to seek support or advice, for whom the issues are also important. There is evidence to show that peer to peer based education programs have been effective in promoting health in a wide range of communities and environments5,6 and also favour community participation, which in turn reduce health inequalities.7
The purpose of this study is to describe and analyze the profile of the persons that have participated in the CHW training-action courses and of the associations that they belong to, and also to quantify the peer to peer education activities carried out over ten courses and analyze their progress over time.
MethodA cross-sectional descriptive study that analyzes the memoranda of the ten CHW training-action courses imparted from 2009 to 2018 has been carried out. The scope of the study was to direct stakeholders of the associations of the city of Valencia and the persons they proposed for training as CHWs.
To select CHWs, associations that participated in the program were asked to suggest a specific student profile and the associations and propose one or two persons with leadership and communications skills and with an interest in promoting health to transmit information to their peers. The organisations also offer the support required for them to complete the practical part of the course by enabling them to carry out peer to peer education activities on their premises.
The theoretical modules of the course are designed as participatory sessions with group dynamics based on meaningful learning.8 The sessions are combined with workshops that the students receive, through which they acquire the knowledge that they shall subsequently transfer in their own contexts when carrying out the practical module in their associations.
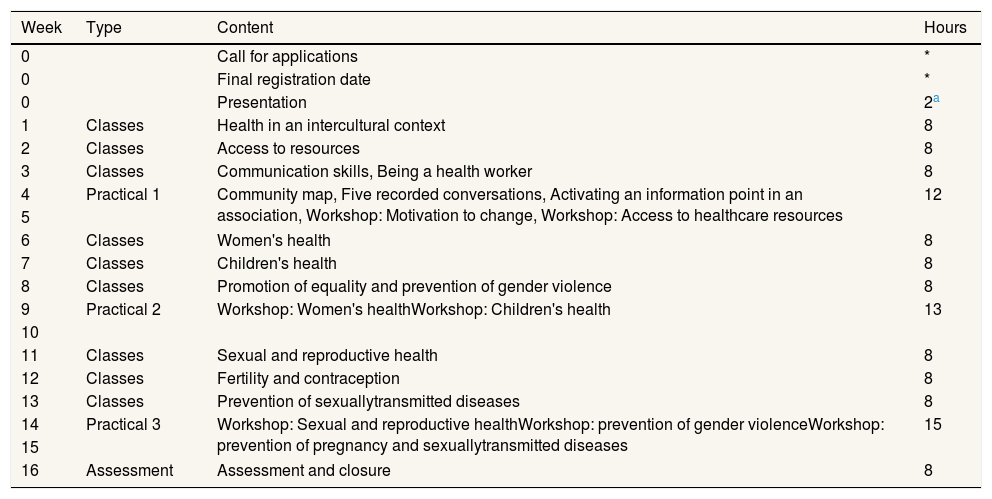
The training-action course lasts for 120hours over 12 weeks: 80 theoretical and 40 practical, given in two sessions of 4hours every week. The theoretical part is divided into three modules, and after each one there are 2 weeks to complete the practical part (Table 1).
Time distribution of the contents of the community health workers course.
| Week | Type | Content | Hours |
|---|---|---|---|
| 0 | Call for applications | * | |
| 0 | Final registration date | * | |
| 0 | Presentation | 2a | |
| 1 | Classes | Health in an intercultural context | 8 |
| 2 | Classes | Access to resources | 8 |
| 3 | Classes | Communication skills, Being a health worker | 8 |
| 4 | Practical 1 | Community map, Five recorded conversations, Activating an information point in an association, Workshop: Motivation to change, Workshop: Access to healthcare resources | 12 |
| 5 | |||
| 6 | Classes | Women's health | 8 |
| 7 | Classes | Children's health | 8 |
| 8 | Classes | Promotion of equality and prevention of gender violence | 8 |
| 9 | Practical 2 | Workshop: Women's healthWorkshop: Children's health | 13 |
| 10 | |||
| 11 | Classes | Sexual and reproductive health | 8 |
| 12 | Classes | Fertility and contraception | 8 |
| 13 | Classes | Prevention of sexuallytransmitted diseases | 8 |
| 14 | Practical 3 | Workshop: Sexual and reproductive healthWorkshop: prevention of gender violenceWorkshop: prevention of pregnancy and sexuallytransmitted diseases | 15 |
| 15 | |||
| 16 | Assessment | Assessment and closure | 8 |
The two hours of Presentation are not calculated as course time.
Source: adapted from López et al.3
The CHWs have to do the following in the practice periods: draw up a community map, create an information point, hold health conversations based on “motivational messages” and deliver peer to peer education workshops.8 The teaching team is multi-disciplinary and consists of 16 healthcare and non-healthcare professionals: 7 primary care professionals (nursing, paediatrics, midwifes, etc.), 5 public health professionals (medicine, nursing), 2 CHWs, 1 psychologist and 1 actress. The idea is that at the end of the course the persons trained as CHWs can act as health promoters and so enable associations to include health in their agendas as a participatory process and to become involved in community projects.9
Variables studiedA data base was prepared on a spreadsheet used to include the variables: gender, country of birth, year of training and association.
The type of population that the activities were designed for was taken into account and was divided accordingly, thus classifying the associations as: local, immigrant and intercultural community (if designed for communities with two or more cultures). To study the continuity and role of the CHW after training, follow-ups were conducted using telephone conversations, records of attendance at program community forums and visits by program technicians to the associations. The follow-ups enabled the role they had within each association to be identified: if they continued to be linked to them or not after the course and if they participated in community health projects. Finally, the peer to peer education activities conducted in the associations in the practice periods of the 10 training-action courses were collected.
Analysis of the dataA descriptive analysis of the sample was carried out in which the quantitative variables were described as averages with their corresponding 95% confidence intervals (95% CI). The qualitative variables were expressed as absolute and relative frequencies, likewise with their 95% CI. A bivariate analysis was also carried out using classical statistical methods, relating the means of the quantitative variables with the Student's t test to compare them in two different time periods: from 2009 to 2013 and from 2014 to 2018. The time trends were analysed by applying linear regression models, using the different years studied as the dependent variable. The confidence levels for the proportions were determined using a macro designed for SPSS called ICIP v. 2001 designed by Doménech.10 An alpha level of under 0.05 of statistical significance was adopted in all cases. The IBM SPSS Statisticsv.20 program was used for the statistical analysis of the variables.
Ethical considerationsThe study was submitted to the Ethical Committee of the Foundation for Biomedical and Healthcare Research of the Regional Government of Valencia, which considered that “given the characteristics of the study and the regulations in force at the time of its preparation, no approval is required” by said committee.
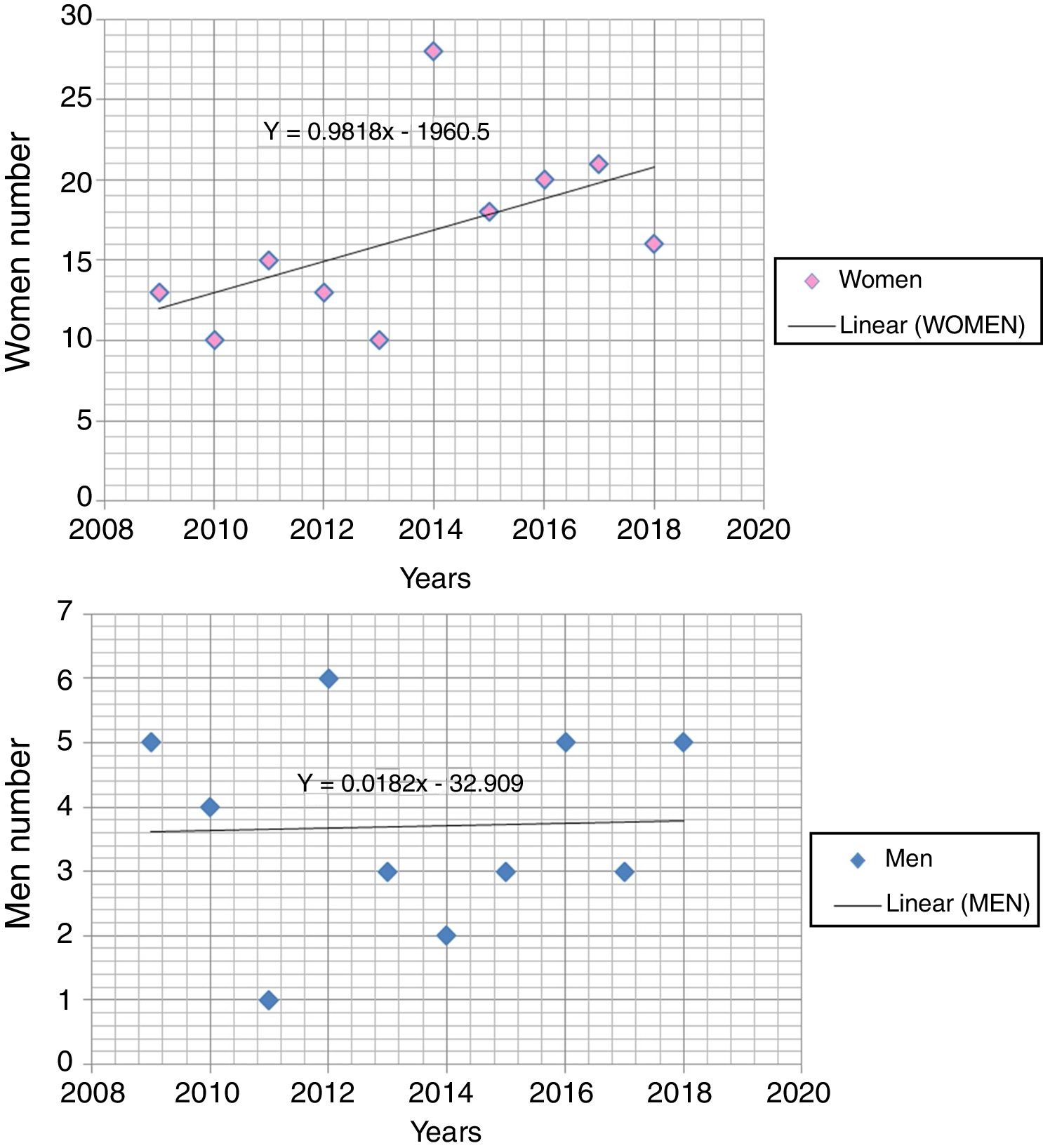
Results201 CHWs were trained in the last 10 years of the period under study. Most of them were women, 164, or 81.6% (95% CI: 75.5-86.7) against 37 men, or 18.4% (95% CI: 13.3-24.5). The number of trained CHWs showed an upward trend over the years (Fig. 1), more notable amongst women than men, although there is no statistical significance by gender (p=0.377). The number of women increased from 12 in the first course to 16 in the most recent one.

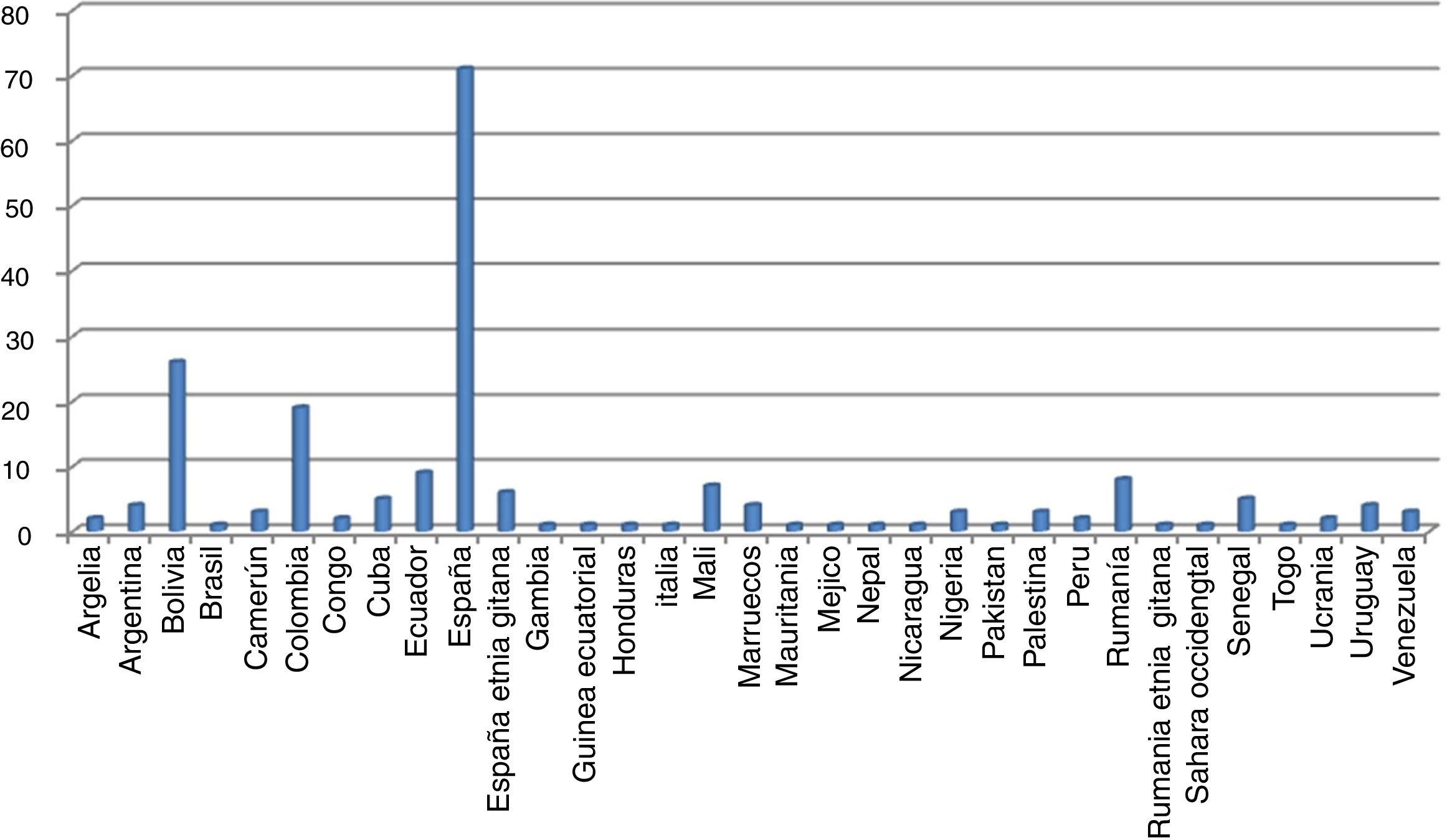
The trained CHWs came from 31 countries (Fig. 2), although 71, or 35%, were from Spain (95% CI: 28.7-42.4) and 6, or 3%, Spanish of the Roma ethnic group (95% CI: 1.1-6.4]. 26, or 12.9% (95% CI: 8.6-18.4) were from Bolivia and 12, or 9.5% (95% CI: 5.8-14.4) from Colombia.

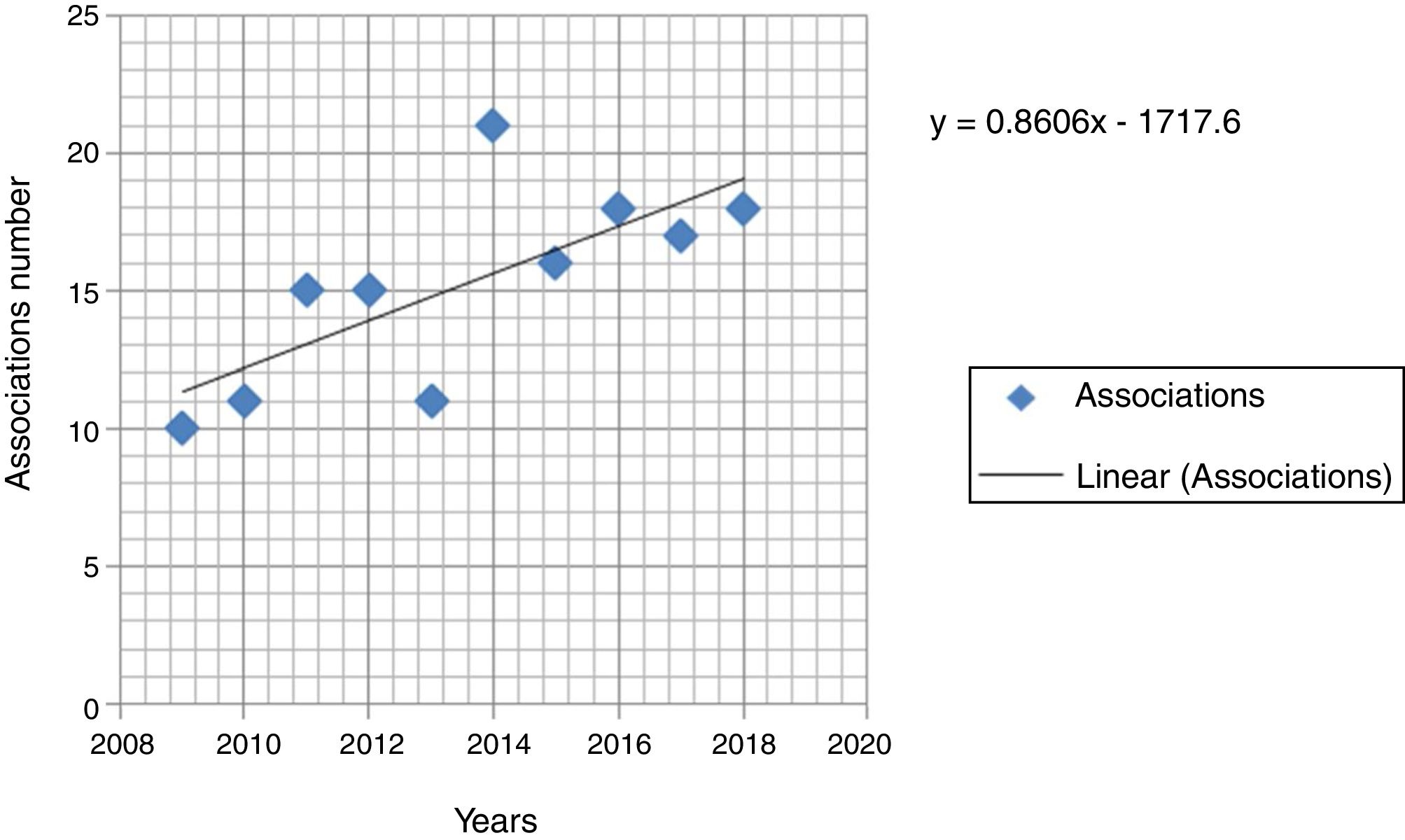
82 associations or organisations were involved in the 10 courses. 42 of them, or 51.2% (95% CI: 39.9-62.4) worked with culturally diverse communities; 24, or 29.3% (95% CI: 19.7-40.4) worked with immigrant populations; 15, or 18.3% (95% CI: 10.6-28.4) with the local population; and 1.2% (95% CI: 0.3-6.6) was a foundation that worked with the Roma community. The trend in the number of associations involved over time shows an increase and is statistically significant (p=0,017), as can be seen in (Fig. 3).There are associations interested in sending several participants but only a maximum of two people per association are allowed every year.

The situation regarding 102 CHWs, or 50.7% (95% CI: 43.6-57.9) and whether they stayed on at the associations after the course is unknown. This lack of knowledge gives a downward trend over time that is clearly significant (p<0.0001). As for the CHWs that continued to be linked to the associations, 71 carried on participating on a voluntary basis, which figures as 35.3% (95% CI: 28.7-42.4) and presents an upward and clearly significant trend throughout time (p <0.0001). On the other hand, 18 CHWs, or 9.0% (95% CI: 5.4-13.8), continued to be linked to the associations under contracts and also showed an upward and significant trend throughout time (p <0.007); and finally, 10, or 5.0%, were technicians of the associations (95% CI: 2.4-9.0) who continued as such after the course.
The total number of persons who were receiving training as CHWs carried out activities in which 7383 persons from the associative network of Valencia directly participated, which means that each CHW interacted with an average of 37.6 persons via said activities (peer to peer interactions).
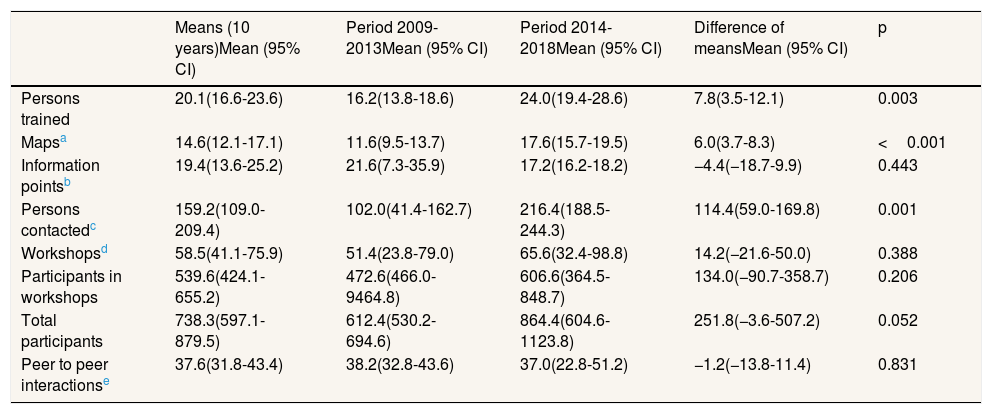
Table 2 shows the averages of the persons trained and the number of peer to peer education activities carried out during the practical sessions of the training-action course, divided into two time periods (2009-2013 and 2014-2018) and the calculation of the difference between the averages.
Evolution of the peer to peer education activities carried out in the practical sessions of the community health worker training course.
| Means (10 years)Mean (95% CI) | Period 2009-2013Mean (95% CI) | Period 2014-2018Mean (95% CI) | Difference of meansMean (95% CI) | p | |
|---|---|---|---|---|---|
| Persons trained | 20.1(16.6-23.6) | 16.2(13.8-18.6) | 24.0(19.4-28.6) | 7.8(3.5-12.1) | 0.003 |
| Mapsa | 14.6(12.1-17.1) | 11.6(9.5-13.7) | 17.6(15.7-19.5) | 6.0(3.7-8.3) | <0.001 |
| Information pointsb | 19.4(13.6-25.2) | 21.6(7.3-35.9) | 17.2(16.2-18.2) | −4.4(−18.7-9.9) | 0.443 |
| Persons contactedc | 159.2(109.0-209.4) | 102.0(41.4-162.7) | 216.4(188.5-244.3) | 114.4(59.0-169.8) | 0.001 |
| Workshopsd | 58.5(41.1-75.9) | 51.4(23.8-79.0) | 65.6(32.4-98.8) | 14.2(−21.6-50.0) | 0.388 |
| Participants in workshops | 539.6(424.1-655.2) | 472.6(466.0-9464.8) | 606.6(364.5-848.7) | 134.0(−90.7-358.7) | 0.206 |
| Total participants | 738.3(597.1-879.5) | 612.4(530.2-694.6) | 864.4(604.6-1123.8) | 251.8(−3.6-507.2) | 0.052 |
| Peer to peer interactionse | 37.6(31.8-43.4) | 38.2(32.8-43.6) | 37.0(22.8-51.2) | −1.2(−13.8-11.4) | 0.831 |
Maps are prepared of the territory where the association is located that delineate the local health resources and assets and significant meeting spaces for communities in vulnerable situations.
Information points in the association and in other significant locations are established using posters and information leaflets about the program and access to health services in the area.
Informal conversations are held in significant spaces or information points through which messages about health and access to health services and programs are transmitted.
Statistically significant differences were found in the averages of persons trained, maps prepared and persons contacted via conversations, with a larger number of these variables being identified in the second period of the courses (2014-2018). Likewise, larger averages in the number of workshops and their participants and in the total average of participants were found in the second period, although no significant differences could be seen.
DiscussionThe profile of the person trained as a CHW in the Mihsalud program is that of a woman, of 35 years of age, born in Spain, Bolivia or Colombia; who accesses the training-action course proposed by an intercultural association.
The content of the training-action and peer to peer education activities of the Mihsalud follows the model of “bridging roles” according to the classification of South et al.5 The main role of the persons trained as CHWs in this case is to act as a bridge between associations (and their communities) and the health services, especially when their peers are experiencing a situation of inequality due to a lack of information about access to and functioning of services and programs. The results obtained about the predominance of women trained as community health workers and the activities conducted are similar to those presented by Ramos-Martín et al., 11 although the community used as a basis for the study are residents of a clearly defined district and do not come from an associative context, at the same time, the effects in terms of improved health and a transformed reality are evident.12
The diversity of countries of origin and cultures has made it possible to generate spaces for intercultural mediation and encounters in each course, leading to positive experiences in terms of coexistence and joint work on health.13–15 Likewise, the program's model of participation meant an opportunity to share facilitating tools for participation amongst associations.16,17
The profile of the association that takes on CHWs after the course is that of an intercultural entity that integrates peer to peer education as a voluntary or remunerated activity. Participation by both associations and women increased throughout the courses. This may be due to the direct involvement of representatives of associations in the design of the Mihsalud program, which has take shape over the years and is known and positively valued by associations9 and by the people trained in them, such as CHWs, as much as other similar interventions;18 and the fact that the course design has seen improvements in terms of content and methodology after the assessments conducted at the end of each year. Likewise, the number of associations that take on persons trained as CHWs in health projects has increased, which could suggest that the course provides the needed skills and knowledge which are currently missing from within the third sector. Some organisations have also maintained links with CHWs in the form of volunteering activities19 while others have made use of the course to enable its professionals to acquire skills as CHWs to promote community health projects. Such results highlight the importance of associations to promote health in especially vulnerable collectives as proposed by Asweto et al.6 because of their potential for reaching out to groups of persons and for their inclusion in the health system via such training-action courses; and as stated in the study by Chiu20 in which ethnic minorities are included in cancer prevention programs. Both studies use the same strategy of the Mihsalud program, peer to peer education,3,4 to bring about the involvement of associations in setting up projects in conjunction and in coordination with the health services. Such an alliance for co-production21,22 between associations and public health services is aligned with the recommendations of the NICE guide to encourage community participation in health and reduce inequalities.7
The total of the activities in the practical periods of the course show the enormous potential for replication provided by peer to peer education,7 which converts the training-action period into part of an intervention geared towards the third sector, although the number and intensity of such activities after the course is unknown. The study has detected that many associations do not include community health workers after the training course, although data were missing regarding follow-ups with almost half of the trained CHWs. This lack of continuity was also detected in previous assessments and it is believed that the cause is a lack of resources and structure in most organisations. To respond to this situation, a guide designed for organisations such as the ones in this study was drawn up9 to facilitate and reinforce greater involvement in the program23,24 and lines of financing were created by the regional government (DGCV: 8285/02.05.2018), designed to prepare projects amongst communities in vulnerable situations.
The limitations of this study are as follows. The reasons why the CHWs are not linked to the associations after the course are unknown; there are collectives such as people of African origin who are poorly represented in the associative sphere and should therefore be encouraged to access these training-action courses, even when they are not part of formal associations; it would be necessary to introduce information on the 7383 people involved in the community by CHWs to evaluate the impact of the program on the community network and, finally, the specificity of the intervention in the context of the city of Valencia may make it difficult to transfer the programme for implementation into other contexts without a prior analysis of the local context, needs and stakeholders to involve.
ConclusionsThe profile of the person trained as a CHW in the Mihsalud program is that of a woman, of 35 years of age, born in Spain, Bolivia or Colombia. The profile of the association that takes on CHWs after the course is that of an intercultural entity. The time trend showed an increase in participation by associations that send CHWs for training, in which women are the predominant gender, thus resulting in an increase in the health promotion activities.
After the course, 35.3% of the CHWs continued to collaborate voluntarily in the associations.
Evaluation studies have been carried out on the Mihsalud program, which sets out to promote health in vulnerable populations and which has had satisfactory results. However, the training-action courses carried out, the number of agents, community health workers, the characteristics of the associations that trained them and that participate in the program with training and coordination of nursing staff are unknown factors.
What does this study add to the literature?This study contributes by showing that coordination between nurses and associations and community health workers increases people's participation; it also contributes by providing greater knowledge about the profiles of agents and associations, and their subsequent interventions in the community.
Carlos Álvarez-Dardet.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsAll the authors substantially contributed to the concept and design, and the collection, analysis and interpretation of the data. They drew up the draft and critically reviewed the intellectual content. They then gave their approval for publication of the version.
This study was prepared as part of the Doctoral Program in Clinical and Community Nursing of the University of Valencia. The article forms part of the compendium of articles for the doctoral thesis by P. López Sánchez.
FundingThis study forms part of a research project that received the Joan Baptista Peset Award of the Town Hall of Valencia granted by the Instituto Médico Valenciano in 2016.
Conflicts of interestsNone.
Our thanks to the Instituto Médico Valenciano, the town hall of Valencia, all the health associations and community health workers that contributed to the training-action courses, the Escuela Valenciana de Estudios para la Salud (EVES), and to the teaching team of collaborating healthcare professionals. In particular, our thanks to the management of the Public Health Centre of Valencia, without their commitment this research article would not have been possible.











